
Abstract
Cough-suppression physiotherapy is a novel self-help therapy for chronic cough. We evaluated the effectiveness of cough physiotherapy in a pilot prospective observational study. We assessed cough-specific health-related quality of life (HRQOL) with the Leicester Cough Questionnaire (LCQ) and subjectively reported cough frequency and sleep disturbance in 23 patients with chronic cough refractory to medical therapy, before and after outpatient-based cough-suppression physiotherapy. Cough-suppression physiotherapy consisted of education, counselling, cough control, breathing retraining, and vocal hygiene. There was a significant improvement in cough-specific HRQOL after cough physiotherapy; mean (standard error of mean [SEM]) LCQ total score before 12.4 (0.9) versus after 15.1 (0.9); 95% confidence interval of difference −4.1 to −1.3; p < 0.001. The improvement in cough-specific HRQOL was greater than the LCQ minimal clinically important difference of 1.3. A significant improvement was seen in all LCQ domains: physical (p = 0.001), psychological (p < 0.001) and social (p < 0.04). There was a significant reduction in cough frequency scores (p = 0.002) and sleep disturbance scores (p = 0.02). Our findings suggest cough-suppression physiotherapy may lead to a clinically significant improvement in cough-specific HRQOL in patients with chronic cough.
Introduction
Chronic cough is one of the commonest reasons for referral to respiratory outpatient clinics. 1-3 Asthma, gastroesophageal reflux disease (GERD) and rhinitis (also known as upper airway cough syndrome) are the most frequently reported causes. 4 In up to 40% of patients, the cough is refractory to therapy directed at the most common causes of chronic cough. 5 These patients suffer considerable physical and psychological morbidity and have impaired quality of life. 6 Vomiting, incontinence, blackouts, sleep deprivation, depression, relationship difficulties and absence from work are frequent. 3 Antitussive drug therapy such as over-the-counter medications for chronic cough are ineffective and side effects such as sedation are common. 7 There is a pressing need to develop novel therapeutic approaches. Self-help interventions are often recommended to patients with chronic cough. These include avoiding triggers, encouraging vocal hydration, cough suppression and breaking the cycle of cough exacerbating upper airway irritation. 8,9 We set out to test the hypothesis that an outpatient-based cough-suppression physiotherapy program that encourages self-help intervention for patients with refractory chronic cough leads to an improvement in cough-specific health-related quality of life (HRQOL) in a pilot prospective observational study.
Methods
Patients
Consecutive patients with chronic cough attending a specialist adult cough clinic were recruited. Chronic cough was defined as a cough lasting more than 8 weeks in duration. All patients were assessed using a standardised diagnostic protocol. 10 A diagnosis was established if the patients had a suggestive history and/or investigations and a clinical response to specific therapy. Patients with refractory chronic cough had: (1) idiopathic chronic cough (all had negative investigations and treatment trials for asthma, upper airway cough syndrome and GERD) or (2) cough due to asthma, upper airway cough syndrome or GERD refractory to intensive therapy (oral corticosteroids, omeprazole 40 mg twice daily for 3 months, antimotility drugs, self-help measures to minimise GERD, nasal corticosteroids, decongestants and antihistamines). Exclusion criteria were (1) current smokers, (2) recent upper respiratory tract infection (<4 weeks), (3) use of angiotensin-converting enzyme inhibitor medication, (4) significant change in cough severity in the preceding 4 weeks, (5) abnormal chest X ray and (6) abnormal lung function tests.
Leicester Cough Questionnaire
Health status, the primary outcome measure, was assessed with the Leicester Cough Questionnaire (LCQ). 6 This is a 19-item, self-completed, cough-specific HRQOL questionnaire. It has been extensively validated and shown to be both reproducible and responsive. The questionnaire utilises a 7-point Likert-type response scale. There are three domains physical, psychological and social. A higher score indicates a better quality of life. Overall scoring ranges from 3 to 21. The minimal important difference (MID) for the LCQ total score is 1.3. 11
Cough frequency and sleep disturbance
Cough frequency and sleep disturbance resulting from cough was determined by the following questions:
Cough frequency: In the last 2 weeks, how many times a day have you had coughing bouts?
Sleep disturbance: In the last 2 weeks, has your cough disturbed your sleep?
Patients were asked to respond on a 7-point Likert-type scale.
Protocol
The cough-suppression physiotherapy programme was developed following a multidisciplinary review of interventions thought to be potentially useful in suppressing cough. This involved a review of the literature and critical review of the interventions. The team included physiotherapists, clinicians, pharmacists and patients. All patients attending clinic with refractory chronic cough were referred for outpatient cough physiotherapy. Cough-suppression physiotherapy components were prescribed on an individual basis according to the assessment. For example, nasal breathing exercises were prescribed only to those identified as mouth breathers on initial assessment. There were up to 3 sessions of cough-suppression physiotherapy available per patient, administered at least 1 week apart according to the individual needs of patients. The LCQ was administered at baseline and again after 2 months following cough-suppression physiotherapy. Patients were asked to complete the LCQ by a receptionist in a room separate from the treating physiotherapist and were told another researcher would analyse the data.
Session 1
General assessment: History, symptoms, triggers and social circumstances.
Education and lifestyle advice: The aims of cough-suppression physiotherapy and self-management education were explained. The lack of physiological benefit of excessive cough and its negative impact were emphasised and patients were encouraged to modify their response to cough stimuli appropriately. Education was aimed at facilitating empowerment, garnering trust to enable patients to make these lifestyle changes. Setting realistic goals and time frame, promoting self-efficacy and motivation were also important components. Lifestyle and stress management were advised where appropriate.
Physiotherapy: Patients were prescribed and taught one or more of the following: cough control—the patient was encouraged to identify when they felt an urge to cough. A strategy was prescribed to suppress the urge and control cough using distraction (drinking water, chewing gum or sucking sweets or lollies) and substituting the cough with a swallow or relaxed throat breathing (dropping/relaxing shoulders). Patients were informed that suppressing their cough may break the cycle of cough itself exacerbating their condition.
Breathing pattern retraining and vocal hygiene: Identification of dysfunctional breathing and vocal cord dehydration to reduce irritation of the upper airways. Nasal rather than mouth breathing was promoted. Breathing retraining involved teaching patterns of breathing designed to reduce respiratory rate.
12
Techniques taught included controlled breathing, pursed lip breathing and relaxed throat breathing. Patients were asked to avoid factors that cause vocal dehydration: smoky atmosphere, excessive consumption of alcohol and caffeine. Vocal cord hydration was encouraged by drinking water before speaking for long periods, sucking sweets and inhalation of steam. Gentle throat massage was advised if muscle tension from excess cough was suspected.
Reinforcement: Patients were given written information sheets to help reinforce these techniques.
Session 2
Review compliance with cough-suppression physiotherapy (verbal). Patients were encouraged to discuss their goals and problems with the techniques. Holistic advice was given as needed including coping strategies for cough.
Analysis of data
Data are presented as mean (standard error of mean [SEM]). Paired t tests were used to compare the LCQ scores pre- and post-cough-suppression physiotherapy intervention and unpaired t tests to compare idiopathic versus explained cough groups. A p value <0.05 was considered significant. SPSS software version 17 was used for the analysis. The purpose of this study was to assess the potential benefits of cough-suppression physiotherapy and generate data to calculate the number of patients needed for a randomised controlled trial. A sample size of 19 subjects would have 95% power of detecting significance at the 5% level for a change in the primary outcome measure of LCQ of 3.1 as seen in a study investigating the effects of physiotherapy on cough in bronchiectasis. 13 The mean (SD) LCQ score in 179 patients with chronic cough has been reported as 14.03 (3.87). 14 All subjects gave informed consent and the study protocol was approved by the local research ethics committee (Leicestershire Ethics Committee).
Results
Twenty-three patients were recruited (patient demographics, Table 1 ) and no patient declined to participate or withdrew from the study. The causes of the chronic cough were idiopathic chronic cough (n = 18), cough variant asthma (n = 2), upper airway cough syndrome (n = 1), GERD (n = 1) and eosinophilic bronchitis (n = 1). Cough control and breathing retraining/vocal hygiene were administered to all patients. A mean (SEM) of 2 (0.1) cough-suppression physiotherapy sessions were administered per patient. At the follow-up visit, all patients reported compliance with prescribed exercises at least once a day.
Patient characteristics a
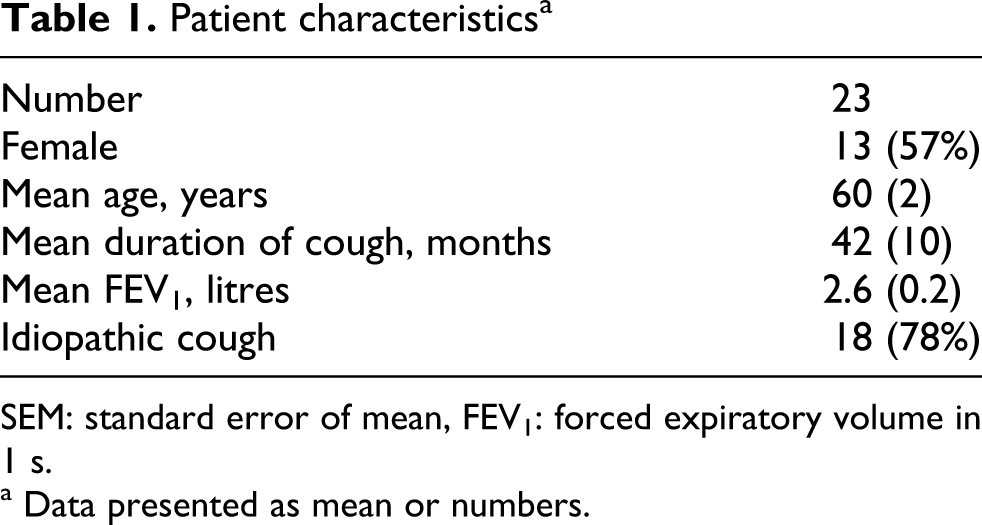
SEM: standard error of mean, FEV1: forced expiratory volume in 1 s.
a Data presented as mean or numbers.
There was a significant improvement in health status following cough-suppression physiotherapy; mean (SEM) LCQ total score before 12.4 (0.9) versus after 15.1 (0.9); mean difference 2.7; 95% confidence interval of difference −4.1, −1.3; p < 0.001 (Figure 1 ). The improvement in QOL was greater than the LCQ MID of 1.3. Health status improved in 19 (83%) of the patients and greater than the LCQ MID in 16 (70%) of the patients. A significant improvement was seen in all LCQ health-related domains such as physical (p = 0.001), psychological (p < 0.001) and social (p < 0.04; Figure 2 ). There was no significant effect of age (r = 0.31, p = 0.14) or duration of cough (r = −0.17, p = 0.5) on change in LCQ HRQOL. There was no significant difference in change in LCQ HRQOL between patients with explained and idiopathic cough (p = 0.98). No adverse effects of cough-suppression physiotherapy were reported. There was a significant reduction in reported cough frequency scores (5.4 vs. 4.3; mean difference 1.1; 95% confidence interval of difference 0.5–1.8; p = 0.002) and sleep disturbance scores (4.5 vs. 3.6; mean difference 0.9; 95% confidence interval of difference 0.1–1.6; p = 0.02).

Cough-specific health-related quality-of-life total score before and after cough-suppression physiotherapy. HRQOL: health-related quality of life, LCQ: Leicester Cough Questionnaire; range 3–21; high score = better quality of life. Error bars represent standard error of mean (SEM).

Cough-specific health-related quality-of-life domain scores before and after cough-suppression physiotherapy. HRQOL: health-related quality of life, LCQ: Leicester Cough Questionnaire; LCQ domain score range 1–7; high score = better quality of life. Error bars represent standard error of mean (SEM).
Discussion
This is the first study to evaluate cough-suppression physiotherapy for patients with chronic cough. We have shown that cough-suppression physiotherapy can lead to a reduction in cough frequency, sleep disturbance and improves cough-specific HRQOL. The improvement in cough-specific HRQOL was large and clinically and statistically significant. It was greater than the LCQ minimal important clinical difference and was seen in most patients. Furthermore, it was greater in magnitude to that seen with opiates for idiopathic cough and physiotherapy for bronchiectasis-associated cough. 13,15 Patients were compliant with cough-suppression physiotherapy and reported no side effects.
Cough-suppression physiotherapy may have reduced cough by a number of mechanisms. The avoidance of triggers of cough was an important component of patient education. Common triggers reported by patients include smoky atmosphere, cold air, exercise, perfumes and other strong odours, eating, speech and laughter. They are thought to activate airway nerve cough receptors such as transient receptor potential vanalloid 1 (TRPV-1) and transient receptor potential Ankyrin type 1 (TRPA-1) since temperature, pH, noxious stimuli and stretch are well-described stimuli. 16,17 Most patients with chronic cough have a heightened cough reflex. 18 It is possible that cough-suppression physiotherapy reduced cough reflex sensitivity, both peripherally and centrally. Strategies to reduce upper airway irritation, vocal dehydration and dysfunction may have reduced peripheral cough sensitivity. The reduction of anxiety by modification of behaviour may have altered central cough pathways. Voluntary cough suppression, a key component of therapy was prescribed to reduce both voluntary and reflex cough. Lastly, advice given to minimise adverse impacts of coughing may have improved HRQOL. Further studies that incorporate measures of cough reflex sensitivity, urge to cough and anxiety are needed to understand the mechanisms by which cough-suppression physiotherapy reduced the impact of cough.
There is evidence that some of the components of cough-suppression physiotherapy reduce cough severity. A recent randomised controlled trial of a speech therapy programme in patients with cough reported a significant reduction in cough severity. 8 This programme consisted of interventions that addressed vocal hygiene, dysfunction and irritation in addition to cough suppression and behaviour modification. The key components of speech therapy for cough were similar to cough-suppression physiotherapy. However, there were some differences between the two studies. It is possible that the speech therapy programme may have had a greater emphasis on therapy for voice and vocal cord dysfunction. The HRQOL benefits of speech therapy were not investigated in this trial. In contrast, we used a validated cough-specific quality of life tool to assess the benefits of cough-suppression physiotherapy. The setting of cough-suppression therapy may also be important to the success of delivering a clinical service. In our outpatient set-up physiotherapy and respiratory services are integrated which facilitates the provision of cough-suppression therapy. Cough-suppression physiotherapy provides a combination of physiotherapy and speech therapy interventions relevant to persistent cough. The benefit of each component of cough suppression is worth investigating in future to determine the optimal programme. It is likely that individual tailoring of therapy for patients is important since this was a feature of both treatment programmes.
The largest group of patients in our study had idiopathic chronic cough, but we also included patients with explained chronic cough refractory to specific treatment. In our experience, partial reduction rather than resolution of cough following specific therapy is common in patients with explained cough; hence there is a need for additional therapy. The effectiveness of cough-suppression physiotherapy in other settings is worth investigating. It may be useful to treat cough resistant to therapy for patients with idiopathic pulmonary fibrosis, emphysema, lung cancer and sarcoidosis.
There are some limitations in our study, most notably the lack of a control group. The placebo effect is common in clinical trials of patients with cough, but this is usually more prominent in patients with acute cough. In our study, all patients had a stable chronic cough of long-standing duration. All patients had unsuccessful trials of other therapies previously. It is possible that some patients may not have been compliant with cough physiotherapy since we did not measure compliance objectively. Compliance is difficult to assess in this setting but a compliance check at the follow-up visit, although subjective, indicated that patients were administering at least one session of cough physiotherapy daily. It is possible that the professional attention of the physiotherapist delivering the intervention and the motivation of the patients could have influenced the outcome. This is difficult to measure and control for. Future studies need to evaluate this, and effects of individual components of cough-suppression physiotherapy using methodology recommended by the Medical Research Council for complex interventions. 19 Another limitation is that only subjective outcome measures were used. Further studies should incorporate objective outcome measures such as cough frequency monitoring and cough reflex sensitivity measurements. The long-term benefits of cough-suppression physiotherapy beyond 2 months are not known and deserve further investigation. Our findings should be considered preliminary and provide a platform for a large randomised controlled trial. On the basis of the change in LCQ following cough suppression physiotherapy and the standard deviation of the LCQ HRQOL scores reported in our study, we estimate a sample size of 32 patients in each group of a parallel group study to have 80% power of detecting significance at the 5% level.
In conclusion, cough-suppression physiotherapy is a safe and well-tolerated therapy that reduces the frequency of coughing, sleep disturbance and improves HRQOL in patients with chronic cough. It has the potential to be a therapeutic option for patients in whom antitussive drugs are ineffective. Further studies are required to confirm our findings in a randomised controlled trial.
Footnotes
Acknowledgements
We would like to thank the staff in the lung function units for their assistance in the characterisation of patients.
The authors declared no conflicts of interest.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.