
Abstract
Background:
The efficacy of behavioral cough suppression therapy (BCST) for refractory chronic cough (RCC) and unexplained chronic cough (UCC) remains unclear due to limited evidence from small-scale single-center studies.
Objective:
To compile and assess the quality of evidence from randomized controlled trials to evaluate the effectiveness of BCST.
Design:
This study included randomized controlled studies and self-controlled studies related to BCST involving adult patients with RCC or UCC.
Data sources and methods:
We conducted an extensive search of various English and Chinese databases (e.g., PubMed, CNKI, CBM, VIP, and Wanfang Data Journal Full-text Database) and the Clinical Trial Registration website up to April 2024. The selected studies underwent meta-analysis to investigate the impact of BCST on the patient’s quality of life and cough frequency.
Results:
The included 12 studies showed that BCST significantly improved the Leicester Cough Questionnaire scores of the patients (MD = 4.50, 95% CI (4.03, 4.97), p < 0.001) compared to the simple verbal education group. In addition, a significant reduction in objective cough frequency was observed in patients compared to before BCST, with a statistically significant difference (MD = −8.06, 95% CI (−9.71, −6.41), p < 0.001). Other measures of cough symptoms, such as symptom scores, Visual Analog Scale (VAS) scores, and Cough Severity Index (CSI) also showed improvement.
Conclusion:
This meta-analysis revealed positive therapeutic effects of BCST in patients with RCC/UCC, potentially advancing its application in broader clinical settings.
Trial registration:
This study was registered on PROSPERO with the registration number CRD42024530746.
Introduction
Chronic cough in adults refers to a group of diseases characterized by a persistent cough lasting more than 8 weeks.1 –3 It affects approximately 10% of the population and leads to various adverse symptoms, such as urinary incontinence and syncope, thereby reducing the quality of life and impacting both individuals and society.2,4
Various guidelines suggest that the diagnosis of chronic cough should be based on comprehensive clinical assessments, including physical examinations of the respiratory system, pulmonary function tests, allergen screening, imaging, and other diagnostic tools.2,3 Once the underlying causes are identified, corresponding treatments can be initiated according to the etiology. Symptoms in most patients with chronic cough can be alleviated by targeted therapy directed at the underlying causes. Potential causes of chronic cough include gastroesophageal reflux, upper airway syndrome, and eosinophilic bronchitis, among others.1 –3 However, according to published practice guidelines, some patients continue to suffer from persistent coughing even after undergoing comprehensive evaluation and treatment. This condition is known as refractory chronic cough (RCC).2,5,6 In addition, if patients with chronic cough undergo a comprehensive evaluation and the underlying cause remains difficult to confirm, they are classified as having unexplained chronic cough (UCC).2,7,8
The current treatment options for RCC and UCC are extremely limited. Guidelines advocate the use of neuroregulators, such as gabapentin, for the treatment of UCC, but their neurologically related adverse events cannot be ignored.2,9 –11 In addition, clinical studies on P2X3 receptor antagonists have been conducted in some regions, but their therapeutic effects at safe doses remain unsatisfactory.12,13 Furthermore, while some studies have confirmed the efficacy of drugs such as amitriptyline and codeine, they are not recommended as preferred treatment methods due to significant side effects and inadequate clinical evidence. Given these issues with pharmacological therapy, behavioral cough suppression therapy (BCST), a non-pharmacological intervention, is advocated in guidelines for its avoidance of the risks and side effects associated with pharmacological agents.2,10,14 Additionally, according to a survey by the European Lung Foundation, an increasing number of patients prefer self-management interventions as a treatment approach. 2
BCST is a comprehensive treatment approach that combines various intervention methods such as verbal education, psychological support, and skill training to help patients reduce cough frequency and alleviate symptoms. Specifically, this encompasses the provision of comprehensive information to patients regarding chronic cough, instruction on techniques for suppressing the urge to cough (such as active swallowing, sucking on candies, sipping water, nasal breathing, and pursed-lip breathing), guidance on vocal and throat preservation, maintenance of optimal hydration, and provision of sustained counseling and psychological support.14 –18 It is also known by different names such as speech therapy, language therapy, behavioral therapy, speech and language therapy (SLT), behavioral speech therapy, language/speech pathology management/intervention, cough-suppression physiotherapy, physiotherapy, speech and language therapy intervention (PSALTI), among others.16,19 –22 Despite the varying terminologies, the overall treatment form and intervention approach are similar.
Although several clinical studies on BCST have been conducted, many are limited by small sample sizes and single-center designs, resulting in a lower level of evidence. Therefore, we conducted a systematic review and meta-analysis to compile evidence from published randomized controlled trials (RCTs) to assess the effectiveness of BCST. We anticipate that this study will provide robust evidence supporting BCST as a safe and effective treatment for refractory and UCC, informing clinical practice and ultimately improving patient outcomes.
Methods
Criteria for considering studies for this meta-analysis
Inclusion criteria
Studies were included based on the following criteria: (1) The study design must be either a randomized controlled trial or a self-controlled study, where the control data could be derived either from another group of patients receiving simple verbal education or from the same patients prior to receiving cough suppression therapy. In this context, “simple verbal education” refers to education focused solely on healthy lifestyle practices, excluding the cough suppression techniques employed in BCST; (2) Participants must be diagnosed with chronic cough based on the diagnostic criteria outlined in the clinical practice guidelines for adult or pediatric cough by the American College of Chest Physicians or the Chinese clinical practice guidelines for cough diagnosis and treatment10,23; (3) The intervention must be “BCST” or have characteristics similar to BCST, such as educational techniques, symptom control approaches, or psychological counseling methods; (4) The included studies must report outcome measures that reflect the severity of cough or systemic symptoms in patients, such as cough frequency, cough reflex sensitivity, and Leicester Cough Questionnaire (LCQ) scores. In addition, we were interested in severe adverse reactions that could affect patient health.
Exclusion criteria
The following situations resulted in exclusion from the study or corresponding research: (1) Failure to include relevant indicators for detecting chronic cough in the study population; (2) Studies that used only voice-related or throat-related indicators as evaluation criteria. Studies that relied solely on binary subjective assessments (e.g., patient satisfaction with treatment effects or patient perception of improvement in cough symptoms) were also excluded; (3) Literature with obvious data abnormalities, incomplete data, or data that could not be extracted or converted; (4) Studies that repeatedly used the same study population or published the same batch of data in multiple articles, excluding low-quality or incomplete, duplicate literature; (5) Investigations conducted in specific settings or among special populations (such as military personnel, schools, factories, hospital patients, perimenopausal or postpartum women, and individuals who had experienced disasters or significant life events); (6) Nonhuman studies; 7) Reviews, case reports, comments, conference proceedings, and similar types of publications.
Search methodology
We retrieved relevant literature from the following sources:
Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Chongqing VIP Chinese Science and Technology Journals Database (VIP), Wanfang Data Journal Full-text Database, PubMed, Embase, and the clinical trial registration website (ClinicalTrails.gov).
Our search formula was: ((chronic cough) AND ((Behavioral therapy) OR (Language Therapy) OR (Speech Therapy) OR (Speech and Language Therapy) OR (Behavioral Speech Therapy) OR (Behavioral Cough Suppression Therapy) OR (Cough-suppression Physiotherapy) OR (PSALTI) OR (Language Pathology Management) OR (Speech Pathology Intervention) OR (Language Pathology Intervention) OR (Speech Pathology Management)))
Corresponding Chinese search terms were used when searching in Chinese databases. When searching clinical research websites, we restricted the disease category and intervention method and set the search to include only studies with results. The final search was conducted in April 2024.
Inclusion methodology
Data extraction and evaluation were independently conducted by two researchers. The extracted data and evaluation results were cross-checked, and any discrepancies were resolved through discussion or by involving a third researcher in decision-making.
Relevant data were extracted from eligible RCTs, including study details (such as country, authors, publication year, and study design), participants characteristics (such as age, sex, and sample size), intervention methods, and efficacy evaluations (LCQ score, cough frequency, Visual Analog Scale (VAS) symptom score, and Cough Severity Index (CSI) score). If there were missing data or key information not provided in the articles, priority was given to contacting the corresponding author via email to obtain the relevant content. If missing data in the articles could be converted using statistical methods, the converted data could also be utilized.
Assessment methodology
The inclusion and exclusion criteria for this study were established through consensus between the two researchers. Both researchers independently screened the literature, extracted relevant data, assessed the risk of bias, and resolved disputes through negotiation. In cases where a consensus could not be reached, the issue was resolved by seeking assistance from senior researchers. Additionally, it is worth mentioning that our study report adhered to the PRISMA 2020 guidelines for systematic reviews. 24 The checklist of these guidelines has been submitted as a Supplemental File along with the submission.
Analysis methodology
The meta-analysis was conducted using Review Manager 5.4 software provided by the Cochrane Collaboration. For count data, the mean difference (MD) was used as the statistical measure, along with a 95% confidence interval (CI). The heterogeneity of the included studies was assessed quantitatively using the chi-square test (α = 0.1), and the I2 statistic was used to determine the magnitude of heterogeneity. If there was no statistical heterogeneity among the studies (p > 0.1, I2 < 50%), a fixed-effects model was used for the meta-analysis. If statistical heterogeneity was present (p ⩽ 0.1, I2 > 50%), further investigation into the source of heterogeneity was conducted. After excluding obvious clinical heterogeneity, a random-effects model was used for meta-analysis.
Results
Results of the search
A total of 292 articles were identified through the search, including 9 Chinese and 284 English articles. Additionally, two studies were identified from the ClinicalTrials.gov website. After excluding duplicate studies, 291 records were retained. We screened these 291 records and excluded irrelevant articles and incorrect study types, leaving 33. After thoroughly reviewing these and applying the inclusion and exclusion criteria, 15 articles were eliminated. Subsequently, we performed data pre-collection for the remaining 18 studies. After excluding studies with missing essential data or uncommon indicators, 12 studies were included. A flow diagram of the study selection process is shown in Figure 1.

Flow diagram of study selection.
Among the 12 included studies, 9 were self-controlled experiments and 3 were RCTs. There was significant variation in sample sizes across the studies, with the smallest study including 17 participants, 16 and the largest study including 159 participants. 25 Although researchers used different terms to describe the intervention methods, all included studies adhered to the previous definition of the BCST, which includes educational techniques, symptom control methods, and psychological counseling as part of the treatment. All the participants included in the study were adults with CC or RCC. The duration of BCST varied, but all studies lasted more than 8 weeks. The 12 included studies also used different outcome measures to evaluate treatment effects, as detailed in Table 1.
Characteristics of the 12 studies included.

Duration of implementing intervention measures.
①: Cough frequency; ②: LCQ (Leicester Cough Questionnaire) score; ③: Cough severity (visual analog scale, VAS); ④: Cough reflex sensitivity (capsaicin challenge test); ⑤: Voice and laryngeal symptoms: LHQ (Laryngeal Hypersensitivity Questionnaire), VPQ (Vocal Performance Questionnaire), VHI (Voice Handicap Index), CAPE-V (Consensus Auditory Perceptual Evaluation Voice), DSI(Dysphonia Severity Index), Mean estimated subglottal air pressure, Glottal airway resistance, MPT (Maximum phonation time); ⑥: HADS (Hospital Anxiety and Depression Scale); ⑦: CSI (Cough Severity Index); ⑧: Subjective evaluations of treatment effectiveness, satisfaction, etc. by self-report from patients.
BCST, Breathing control strategy training; BST, Behavioral speech therapy; CC, Chronic cough; CCT, Cough control therapy; CST, Cough suppression therapy; PSTLAI, Physiotherapy, speech and language therapy intervention; RCC, Refractory chronic cough; SPT, Speech pathology treatment.
Quality assessment of the included studies
A summary of the risk assessment is presented in Figure 2, with the rationale for the assessment detailed in the subsequent text.
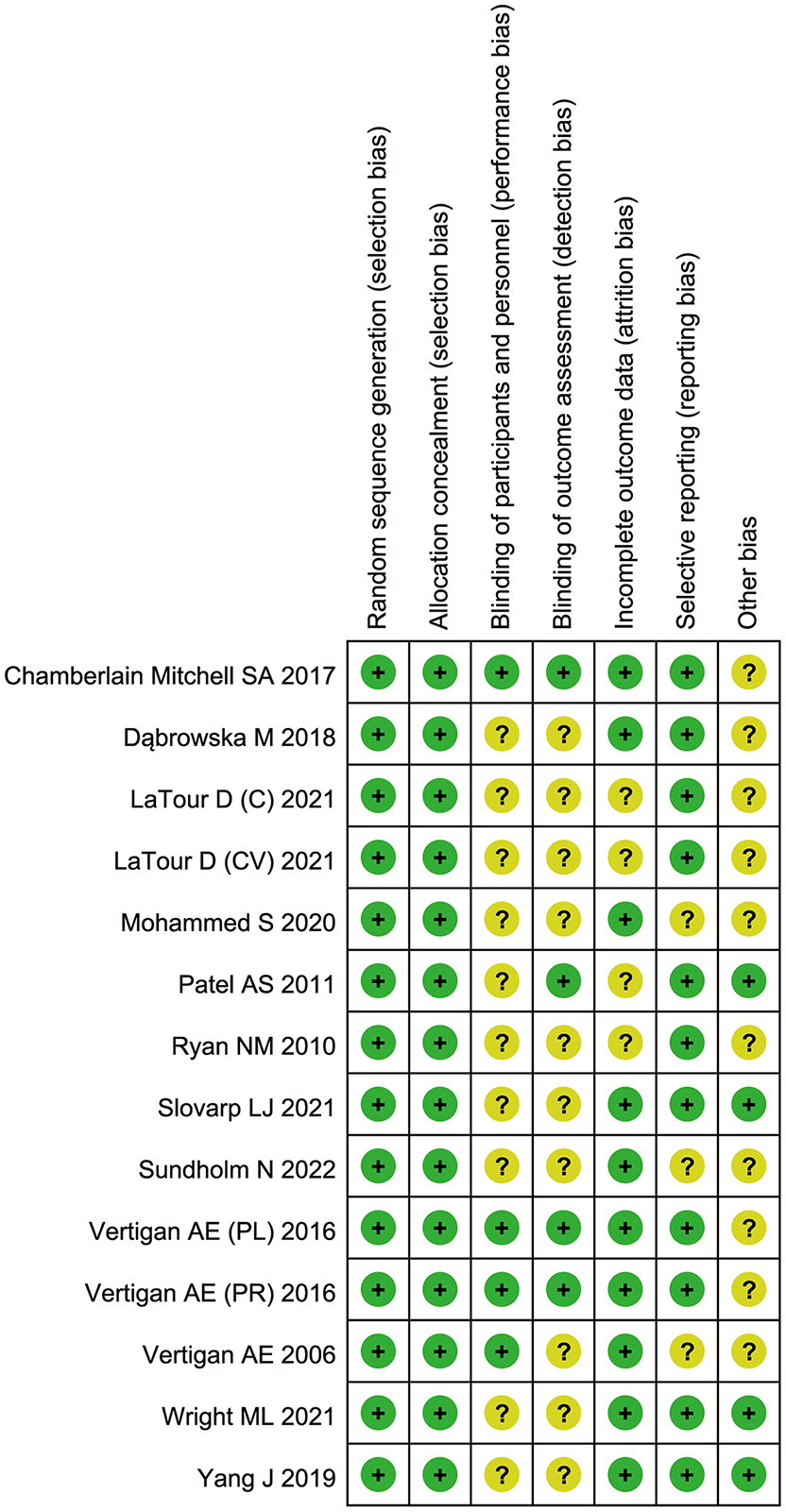
A summary of the risk of bias assessment for the included studies.
In all included studies, the risk of selection bias was generally evaluated as “low risk.” Since BCST is a non-pharmacological treatment, it is difficult to completely blind patients to whether they are receiving comprehensive BCST or simple verbal education. This limitation may introduce unconscious bias during the intervention. The individualized nature of treatment regimens for chronic cough in BCST necessitates a tailored approach to address specific patient needs, which limits the feasibility of blinding in related research. Consequently, “performance bias” was categorized as “unclear risk” in the self-controlled studies, whereas, in RCTs, it was categorized as “low risk.”
For “detection bias,” we judged whether blinding was mentioned during the methods stage. If blinding was not explicitly stated, it was evaluated as an “unclear risk.” For “attrition bias,” we assessed it based on the reported statistics of participants lost to follow-up. If attrition information was not provided, the risk was evaluated as “unclear.” Regarding “reporting bias,” since obtaining the original protocols for each study was difficult, we relied on the protocols outlined in the Methods section. If all evaluation indicators mentioned in the Methods section were reported in the Results section, the study was considered to have a “low risk” of reporting bias. For “other bias,” because the effectiveness of BCST heavily depends on patient compliance, studies that evaluated or confirmed good participant compliance through additional methods were categorized as “low risk,” while others were classified as “unclear risk.”
Outcomes
LCQ scores
Eight studies reported LCQ scores (ranging from 3 to 21, with lower scores indicating a greater impact of cough on patients, leading to a lower quality of life).Six of these studies were self-controlled trials and two were RCTs. A total of 464 patients were included, with 442 and 453 patients in the experimental and control groups, respectively. Statistical heterogeneity was observed among the studies (p < 0.0001, I2 = 75%). Sensitivity analysis revealed that the study by Patel AS in 2011 may be a source of this heterogeneity, as shown in Figure 3. After excluding this study, heterogeneity disappeared (p = 0.46, I2 = 0.0%), and a random-effects model was used for the meta-analysis. The results showed a statistically significant improvement in LCQ scores among patients with chronic cough who underwent BCST, compared to those who only received simple verbal education or before undergoing BCST (MD = 4.50, 95% CI (4.03, 4.97), p < 0.001), as shown in Figure 4. Publication bias was tested using Eggers’ test (p = 0.642), with the bias plot shown in Figure 5. Subgroup analysis based on sex (M/F 0%–25%, 26%–50%, 51%–100%) revealed that the effectiveness of BCST was significant across populations with different sex ratios. However, the effect of BCST was more pronounced when the proportion of females was higher compared to males (MD 4.99 vs 4.36 vs 3.40).

Results of the sensitivity analysis of the studies with LCQ scores.

Forest plot showing the comparison of pre- and post-treatment LCQ scores.

Egger’s publication bias plot.
Objective cough frequency
Three studies reported cough frequency, including a total of 115 patients. However, statistical heterogeneity was observed among the studies (p = 0.07; I2 = 57%). Sensitivity analysis revealed that the study by Ryan in 2010 may be the source of this heterogeneity, as shown in Figure 6. After excluding this study, heterogeneity disappeared (p = 0.93, I2 = 0.0%), and a random-effects model was used for the meta-analysis. Results showed a statistically significant reduction in cough frequency among patients with chronic cough compared to those receiving simple verbal education or before undergoing BCST (MD = 8.05, 95% CI (6.60, 9.50), p < 0.001), as shown in Figure 7.

Results of the sensitivity analysis of the studies with cough frequency.

Forest plot showing the comparison of pre- and post-treatment cough frequency.
Other outcome indicators
Compared to those who received only simple verbal education or before undergoing BCST, patients with chronic cough showed a statistically significant reduction in the CSI (MD = 4.71, 95% CI (2.79, 6.62), p < 0.001), as well as in other indicators such as VAS (MD = 23.23, 95% CI (14.42, 32.04), p < 0.001), total symptom score (MD = 13.21, 95% CI (7.59, 18.83), p < 0.001), symptom score for cough (MD = 3.78, 95% CI (2.66, 4.90), p < 0.001), and Laryngeal Hypersensitivity Questionnaire (LHQ) score (MD = 2.19, 95% CI (1.52, 2.86), p < 0.001).
Discussion
Evaluation of included literature
During the literature screening phase, 18 articles related to BCST for chronic cough were identified. However, due to a lack of standardized evaluation criteria and necessary research data, only 12 relevant articles were included. These 12 articles used different evaluation indicators, and all provided detailed data to support their research findings. The remaining six excluded articles had various issues, including (1) the use of inappropriate evaluation indicators, focusing solely on vocal ability while neglecting the more important improvement of cough symptoms; (2) the use of appropriate indicators but lacking crucial data for meta-analysis; (3) the use of uncommon evaluation indicators not adopted by other articles, making them unsuitable for inclusion in the meta-analysis.
Evaluation of bias risk
When evaluating the risk of bias in the included articles, we encountered challenges in determining the presence of specific biases due to insufficient information. For instance, assessing “detection bias” was difficult because many articles did not explicitly state whether blinding methods were used in the Methods section, making it unclear whether the effects of BCST were exaggerated. Additionally, incomplete reporting of missing data in several articles made it difficult to assess the impact of “attrition bias.”
To mitigate the potential inaccuracies stemming from missing information, we attempted to obtain further details by contacting the corresponding author via email. Unfortunately, we did not receive helpful responses. Assessing the risk of bias relies heavily on comprehensive information about the reviewed studies, especially in research investigating the effectiveness of BCST, which is susceptible to subjective influences from both interveners and participants. This makes it challenging to accurately assess patient compliance regarding “performance” and “other biases.” Insufficient disclosure of key information increases uncertainty among readers and peers regarding the risk of bias, leading to doubts about the quality of the evidence.
Evaluation of main results
Based on the results of this meta-analysis, we believe that speech therapy improves patients’ LCQ and LHQ scores while reducing CSI and symptom scores. Improvement in VAS scores and reductions in cough frequency indicate both subjective and objective decreases in cough severity after treatment. Overall, patients’ quality of life, cough severity, and the impact of cough symptoms on their emotional well-being and social abilities have improved. Thus, BCST is a promising and widely recognized method for treating RCC/UCC.
Additionally, differences were observed among the indicators. The LCQ, cough frequency, and VAS scores reflect the severity of the cough and its impact on patients. Cough frequency is a completely objective indicator, while LCQ and VAS scores quantify the patient’s subjective perceptions. When comparing the standard MD among these three indicators, we found that the improvement in LCQ and VAS scores was more significant than that in objective cough frequency (1.25 and 1.06 vs 0.66, respectively). This suggests that patients’ perceptions of the effectiveness of BCST may be more pronounced than the actual improvement. The assistance provided by BCST goes beyond merely reducing cough frequency; therefore the resulting improvement in quality of life may be more important. For patients who have experienced recurrent coughs and immense pressure in their work, social interactions, and daily life, BCST helps them gain control over their symptoms through their own efforts. This sense of accomplishment boosts confidence, which is more crucial than simply alleviating physical symptoms. These underlying forms of assistance may explain why subjective improvement was more significant than objective improvement in the symptoms of patients with chronic cough. In the subgroup analysis, we observed that as the proportion of females in the population increased, the effect of BCST (based on the change in the MD before and after treatment) seemed to improve. This could be attributed to the varying side effects of chronic coughing in patients of different sexes. For instance, stress urinary incontinence is more prevalent in females with chronic cough compared to males.2,31 Consequently, following an improvement in cough symptoms, female patients may experience a more pronounced improvement in their quality of life. In addition, these differences may stem from variations in lifestyle habits, thought patterns, and adherence levels between male and female patients. However, due to the limited number of subgroups analyzed the conclusions drawn were not rigorous enough; therefore, we did not conduct further in-depth analysis of the reasons behind this.
Possible mechanisms of BCST
The BCST for RCC/UCC involves various factors, such as education, identification of triggers, guidance on suppression techniques, breathing exercises, voice hygiene, hydration techniques, and psychological counseling.17,26 However, the mechanisms underlying the effectiveness of BCST have not yet been fully elucidated. We have summarized the mechanisms underlying the occurrence of chronic cough and discussed the reasons why BCST is effective.
According to existing research, both central and peripheral mechanisms play important roles in the pathogenesis of RCC/UCC. Numerous inflammatory mediators are released peripherally, including protons, pro-inflammatory cytokines, neurotrophic factors, and Adenosine Triphosphate (ATP), can activate corresponding receptors on the vagus nerve, leading to the generation of action potentials in sensory neurons or a decrease in the threshold for activation by other stimuli.32,33 Action potentials at the nerve terminals are initiated through voltage-gated sodium channels (NaVs), which regulate airway sensory nerve excitability and contribute to cough hypersensitivity. 34 Certain viruses, such as rhinovirus, can infect neuronal cells, resulting in increased expression of TRPA1 and TRPV1, as well as the release of NGF, IL-6, and IL-8, which are associated with persistent cough. 35
In the central nervous system, reduced activity in regions responsible for cough suppression in patients with chronic cough may be a crucial mechanism contributing to their decreased ability to control coughing.36,37 Additionally, inflammatory mediators released in the respiratory tract can activate nociceptive fibers, leading to neuropathic inflammation, which in turn can exacerbate the cough reflex and result in persistent coughing.38–40 Furthermore, prolonged exposure to cough-related stimuli can lead to central sensitization, causing exaggerated and persistent coughing responses.7,41 –44 Dysfunction of the brainstem, cough centers, and neural circuits that regulate coughing can disrupt the normal cough reflex and contribute to chronic cough.44 –47 Lastly, psychological factors such as anxiety, stress, and depression can also affect cough perception and regulation, contributing to RCC.47 –49
BCST may help suppress coughing by reducing triggers, improving the cough threshold, and involving the central mechanisms. Lifestyle changes, such as reduced caffeine and alcohol intake, can help avoid triggers and reduce cough frequency.15,16,19 Breathing exercises can relax the throat, neck, and shoulder muscles, potentially reducing the movement of the vocal cord adductors during expiration. Maintaining throat hygiene and proper hydration can attenuate or delay an increase in phonation threshold pressure, reduce the risk of laryngeal injury risk, and decrease stimulation of cough receptors.50,51 According to the recent perspectives, humidification of inhaled air occurs through the evaporation of water over the mucus lining the upper airways. Therefore, maintaining water balance in the upper airways is crucial for respiratory health. This highlights the importance of educating patients with RCC/UCC on how to keep their airways moist. 52 Although throat hygiene is crucial for treating RCC/UCC, current methods for assessing throatsymptoms remain insufficient. Some researchers have suggested that principles and methodologies from chemosensory science could offer new insights into the evaluation of throat symptoms. 53
It is possible that BCST may modify the central nervous system’s response pattern to coughing through cognitive-behavioral techniques, including cognitive restructuring, behavioral regulation, and biofeedback. BCST helps patients recognize the conditions and triggers of coughing and changes their cognitive and emotional responses to it. This helps reduce excessive attention and anxiety related to coughing, thereby decreasing cough reflex sensitivity.15,17,26 Furthermore, BCST enhances patients’ awareness of the urge to cough. When patients perceive the sensation as reaching the cough threshold, they activate voluntary motor responses such as swallowing or relaxed throat breathing, to suppress coughing.54,55 In addition, BCST can utilize biofeedback techniques to help patients become aware of their physiological responses, such as breathing patterns and throat muscle tension. By observing and adjusting these responses, patients can learn to better control their cough.51,55 Through these approaches, BCST can alter the response pattern of the central nervous system to coughing, thereby reducing the frequency and severity of coughs. Moreover, a reduction in cough frequency decreases mechanical damage to the airway epithelium, preventing further exacerbation of airway inflammation. This results in a reduction in the release of inflammatory mediators, and helps avoid further increases in central sensitization, ultimately breaking the vicious cycle of coughing. However, these changes in the central nervous system may require further clarification through techniques such as functional magnetic resonance imaging before and after treatment.
The clinical characteristics of RCC are similar to those of chronic pain caused by central sensitization, including abnormal sensations, hyperalgesia, and allodynia (pain in response to non-painful stimuli). These clinical features are also present in RCC, such as throat sensations, itching, or coughing in response to non-cough stimuli (such as talking or cold air).40,46,56 Studies suggest that enhanced brain activity in patients with cough hypersensitivity mirrors that seen in patients with chronic pain, 37 implying a shared neurobiological mechanism between cough and pain. Several researchers believe that both conditions are neurogenic in nature.40,57 In the field of psychological therapy for chronic pain, various treatment methods have been developed, including cognitive behavior therapy, multimodal treatment, and acceptance and commitment therapy, among others. 58 Andrews et al. conducted research on the use of chatbots to assist patients with chronic pain. 59 These studies indicated that psychological therapy plays a crucial role in the treatment of chronic pain. Considering the similarities between RCC and chronic pain, as well as the similarities between BCST and various psychological therapies, we believe that BCST operates through centrally related mechanisms.
In summary, although we have identified several potential reasons for the effectiveness of BCST, further research is needed to fully understand the complete mechanism, particularly the central mechanisms involved.
Development and application of BCST
Overall, the results from both meta-analyses and individual studies have been encouraging, indicating that BCST can improve cough symptoms and enhance the overall quality of life of patients with RCC/UCC. It has the potential to become a mainstream treatment for RCC/UCC. However, several issues remain unresolved.
First, since BCST is a complex and comprehensive treatment approach, establishing standardized protocols and providing systematic training for therapists is essential to mitigate variations in proficiency. However, due to the varying symptoms, severity, duration, comprehension, and compliance levels among patients, personalized therapies are imperative.53,60 Balancing standardized and personalized treatment modalities poses a significant challenge. Additionally, although many studies have found that BCST can improve the quality of life for patients with chronic cough, not only during but also after the course of treatment, some researchers point out that the therapeutic effects tend to decline after patients have completed their course of treatment. According to Chamberlain et al., the difference in quality of life improvement between the experimental and control groups was no longer significant at the 3-month follow-up after treatment. 21 Therefore, further research is needed to address how BCST can help improve patients’ quality of life over a longer period. Furthermore, more methods are needed to assess and improve patient compliance, as it plays a crucial role in achieving better treatment outcomes. Preventing treatment failure due to patient-related factors is essential. The issue of overcorrection during therapy should also be considered, as excessive behavioral correction may lead to the development of concerns and repetitive behaviors, such as swallowing, pursed-lip breathing, or excessive fluid intake. Although BCST generally improves a patient’s overall quality of life, researchers should pay attention to the potential harm of overcorrection in non-pharmacological therapy. Finally, a treatment method reliant on patient compliance and understanding may yield varying results across different age groups and educational backgrounds. While Fujiki et al. published research on cough suppression therapy in pediatric populations, 61 further studies may be necessary to explore compliance variations and treatment outcomes across diverse demographic groups in the context of the BCST.
Limitations
This study has some limitations. First, the search strategy may not have been sufficiently thorough. As different researchers use different names for BCST, we adopted an awkward approach to include all possible terms related to BCST in the search. Nonetheless, some researchers may have referred to this treatment in unusual ways, which could have led us to overlook some studies. Searching for articles based on the specific content of BCST or selecting articles that do not involve pharmacological therapy from the broader literature on chronic cough treatment for further screening may help address this issue.
In addition, the participants in the included studies appeared to be predominantly female, with some studies including only female participants, which may limit the generalizability of the results. Finally, our data analysis was relatively simple. In the subgroup analyses, we used only sex as a basis for grouping; however, there should be more diverse criteria for subgrouping. When conducting specific analyses, the volume of data in each subgroup should be considered to avoid unreliable conclusions from a small sample size in any group.
Conclusion
In summary, most studies indicate positive outcomes regarding the effectiveness of BCST in treating RCC/UCC. However, further high-quality RCTs with standardized research indicators are required to strengthen the evidence.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241305952 – Supplemental material for Efficacy of behavioral cough suppression therapy for refractory chronic cough or unexplained chronic cough: a meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-tar-10.1177_17534666241305952 for Efficacy of behavioral cough suppression therapy for refractory chronic cough or unexplained chronic cough: a meta-analysis of randomized controlled trials by Baiyi Yi, Shengyuan Wang, Xianghuai Xu and Li Yu in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.