
Abstract
Cough is one of the three major symptoms reported by chronic obstructive pulmonary disease (COPD) patients. The Leicester Cough Questionnaire (LCQ) is a questionnaire exploring the impact of cough, but it does not exist in French. The aim of this study was to develop a French version of LCQ and to assess its psychometrics properties. A forward–backward translation process was used to develop the French version of the LCQ. COPD patients completed LCQ and Cough and Sputum Assessment Questionnaire (CASA-Q) to determine concurrent validity, content validity and internal consistency. Two weeks later, the LCQ was repeated to evaluate the reproducibility. Seventy-four COPD patients were recruited. The concurrent validity showed highly significant correlations between all scores of LCQ and CASA-Q (p < 0.001). The content validity was good with domain total scores correlations ranging from 0.918 to 0.953. The LCQ domains and total scores showed a very good internal consistency with Cronbach’s α coefficients ranging between 0.802 and 0.917. The test–retest reliability was high in COPD patients with no change in cough. In conclusion, The French version of the LCQ is a valid and reliable instrument to measure health status in COPD patients.
Introduction
Nowadays, an approach integrating basic sciences, psychosocial and economic parameters is promoted in medicine. Assessing health-related quality of life (HRQoL) helps the clinician to evaluate and quantify the effects of disease on patients’ daily life. Today, it is also an important tool in the evaluation of treatment effect. 1 Different questionnaires are available for this purpose. They can be generic or specific to a disease, and they measure parameters other than strictly clinical.
In chronic diseases like chronic obstructive pulmonary disease (COPD), specific questionnaires are necessary to optimally target symptoms specific to the disease condition, to explore their physical effects and the subsequent restrictions in daily life and to evaluate the effect of treatment.
QoL impairment is usually related to symptoms in diseases as it was demonstrated in COPD. 2 Moreover, importance of symptoms in COPD is now highlighted in the new classification of the Global Initiative for Chronic Obstructive Lung Disease (GOLD). Cough is one of the three major symptoms reported by COPD patients. 3 Its importance evolves depending on the stage of the disease. 4
Surprisingly, cough is poorly studied in COPD. It is probably due to the lack of valid evaluation tools. Beside cough counters, some questionnaires include items evaluating impact of cough on QoL. They are more valid than cough diaries and visual analogue scale because they measure a combination of aspects of cough severity that include cough frequency and intensity, mood and QoL. 5 The Leicester Cough Questionnaire (LCQ) is a validated HRQoL questionnaire initially developed for patients presenting chronic cough. 6 It explores the impact of cough severity across physical, psychological and social domains and focuses specifically on cough contrarily to the other questionnaires that encompass multiple respiratory symptoms. Its Dutch version was validated in COPD patients, 7 and its potential use was explored in different conditions in this population. 8 –10
Unfortunately, no specific questionnaire exists in French to evaluate cough as a single symptom. For this purpose, the multilingual Cough and Sputum Assessment Questionnaire (CASA-Q) seems the better one as suggested by its name, and it includes evaluation of cough and sputum symptoms and their impact in patients with COPD. 11 Its psychometric properties were assessed. 12 It was validated in seven languages including French. 11 Nevertheless, LCQ remains the international reference questionnaire for cough evaluation. Then, it is interesting to have a French version of this frequently used questionnaire.
The aim of this study was to validate the French version of the LCQ as an assessment tool in COPD patients.
Materials and methods
Ethics statement
The study was approved by the regional Ethics Committee in Cliniques Universitaires Saint-Luc and Université Catholique de Louvain in Brussels (B403201317691). All the patients provided written informed consent.
Subjects
COPD patients attending the pulmonology units of Cliniques Universitaires Saint-Luc and of Grand Hôpital de Charleroi were recruited on a voluntary basis and without financial compensation for this study. Consecutive patients fulfilling the inclusion criteria were selected by the physician after approval of the patients to enroll in the study.
The following inclusion criteria were used for both phases of the study: a diagnostic of COPD associated with the presence of cough and confirmed by spirometry according to GOLD criteria 2013, an age >18 years and native French speaker (patients born in a francophone family speaking French at home and living in the francophone part of Belgium). The patients who were unstable (defined by any modification of health outcomes or treatment) after the inclusion in the study were excluded from the second phase of the study.
Protocol
The study included two phases. During a routine visit, the patients received both questionnaires LCQ and CASA-Q. They were asked to fill out these questionnaires during the outpatient visit or at home using the online version (phase I). They also received a second package including only the LCQ. They were asked to fill out this questionnaire 15 days later and then send it back so that the responses obtained during the initial visit could be compared with the later responses for evaluating the LCQ reproducibility (phase II). For paper and online versions of the questionnaires, complete filling out of the items were checked. No assistance in completing the questionnaires was provided.
Procedure
Permission to use and adapt the questionnaire was obtained from its developers. The process was based on Beaton’s guidelines. 13 The original version of the LCQ questionnaire was translated from English to French using two bilingual translators with a medical background whose primary language was French. From these translated versions, any resulting issues were resolved to obtain a complete agreement. The back translation of this new version was performed by an independent English native speaker. This translation was compared with the original version and validated by authors of this article. Finally, a pilot testing of this French version was performed on six patients and one physiotherapist considering readability and comprehensiveness.
Leicester Cough Questionnaire
It is a 19-item, self-completed questionnaire as described previously. 6 It is divided into three domains and contains a seven-point Likert-type response scale for each item. The LCQ score is calculated by aggregating the points assigned to each question in each domain and then dividing this total by the number of questions in the respective domain. The total severity score ranges from 3 to 21 and is calculated from 8, 7 and 4 items for physical, psychological and social domains, respectively. A lower score indicates a greater impairment of health status due to cough or sputum. It assesses the impact of symptoms over the last two weeks.
Cough and Sputum Assessment Questionnaire
The CASA-Q is a multilingual questionnaire comprising a French version. It was described elsewhere 11 and includes 20 items assessing 4 hypothesized concepts over the last 7 days: cough symptoms (COU-SP), cough impact, sputum symptoms (SPUT-SP) and sputum impact. Questions are answered on a scale from ‘never’ to ‘always’ (for frequency) or from ‘not at all’ to ‘a lot/extremely’ (for intensity). All items are transformed to score from 1–5 or 0–4. Then, the scores are reversed to obtain higher scores for better responses. Within each domain, items are summed and rescaled by calculating the sum of items score divided by the range of rescored item sum and multiplied by 100. CASA-Q domain scores were obtained ranging from 0 to 100. Higher scores were associated with fewer symptoms/less impact due to cough or sputum. No overall score was calculated.
Statistical analysis
The sample size needed (n = 62) to compare LCQ to CASA-Q (phase I) with a power of 80 was determined. The data were computed using SPSS 22.0 (IBM software) for Windows. A descriptive analysis was performed for demographic parameters and for the results of the questionnaires. Pearson correlation between the scores for the domains from both instruments was performed to determine the concurrent validity which represents the instrument performance. The content validity was verified by the correlation between domain and total scores of the LCQ. The internal consistency was assessed by Cronbach’s α to determine the relationship between domains and total scores of LCQ. Floor and ceiling effects were verified if at least 15% of participants get to the lowest or the highest score respectively in a particular domain. The test–retest reliability was evaluated using an intra-class coefficient (ICC) for total score and for each item and domain of LCQ. 14 –16 Bias in the LCQ scores and limits of agreement were estimated using the Bland and Altman method. The effect size was calculated for each domain and total scores by calculating the mean of the differences between baseline and follow-up scores and dividing this mean by the standard deviation of these differences between scores. All of the tests were two tailed, with a statistical significance level fixed at a p value of 0.05.
Results
Seventy-four consecutive patients (male/female = 43/31, age = 65.9 ± 11.4 years and forced expiratory volume in 1 second = 39.1 ± 11.9% of pred.) met the inclusion criteria and completed the LCQ French version and the CASA-Q in phase I. The distribution of patients was 15.8%, 57.9% and 26.3% between GOLD groups 2, 3 and 4 respectively.
The domain and the total scores obtained in the LCQ and the CASA-Q are presented in Table 1. The concurrent validity showed highly significant correlations between all scores of LCQ and CASA-Q (p < 0.001; Table 2). Only Pearson coefficient between psychological domain of LCQ and SPUT-SP was weak (lower than 0.5). The content validity and the internal consistency for LCQ are presented in Table 3. The content validity was good with domain total scores correlations ranging from 0.918 to 0.953. They were all highly significant (p < 0.001). The LCQ domains and total scores showed a very good internal consistency with Cronbach’s α coefficients ranging between 0.802 and 0.917.
Scores obtained in both questionnaires.a

LCQ: Leicester Cough Questionnaire; CASA-Q: Cough and Sputum Assessment Questionnaire; SD: standard deviation.
aResults are expressed as mean ± SD (extremes values).
Concurrent validity.

LCQ: Leicester Cough Questionnaire; CASA-Q: Cough and Sputum Assessment Questionnaire. COU-SP: cough symptom; COU-I: cough impact; SPUT-SP: sputum symptom; SPUT-I: sputum impact.
Content validity and internal consistency for LCQ.

LCQ: Leicester Cough Questionnaire.
The analysis of the scores distribution in our patient population revealed an absence of ceiling and floor effects for all of the domains of LCQ with less than 8% of the patients having the lowest or highest scores.
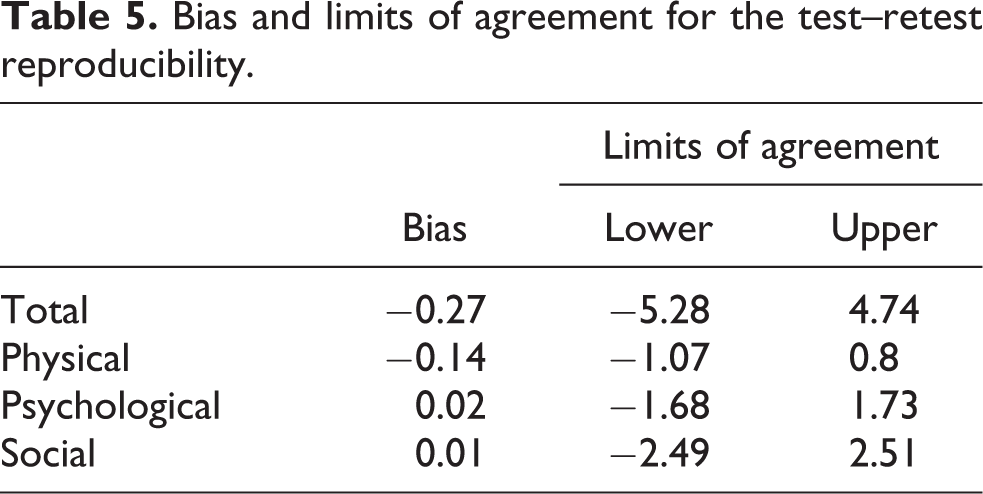
The test–retest reliability was evaluated on 24 stable COPD patients. ICCs were statistically significant for total score and for each domain scores (Table 4 and Figure 1). The Bland and Altman method revealed a low bias between the measurement days for the LCQ total and domain scores (Table 5 and Figure 2). The effect size was small for total LCQ (d = 0.11), psychological (d = 0.03) and social (d = 0.008) domains and medium for physical domain (d = 0.45).

Test–retest reliability for total and domains scores of LCQ. LCQ: Leicester Cough Questionnaire.

Bland–Altman plot of total and domains scores of LCQ in stable COPD patients. Solid lines represent bias means; upper and lower dashed lines represent upper and lower limits of agreement respectively. LCQ: Leicester Cough Questionnaire; COPD: chronic obstructive pulmonary disease.
Test–retest reliability for LCQ.

LCQ: Leicester Cough Questionnaire; ICC: intra-class correlation coefficient.
Bias and limits of agreement for the test–retest reproducibility.
Discussion
Based on the results of this study, we reported a good concurrent and content validity and a good internal consistency for the French version of LCQ. Moreover, the test–retest reliability was verified for this translated version. These results confirm the validation of the French version of the LCQ in COPD patients.
The results obtained to LCQ by our COPD patients are in agreement with the validation of the initial LCQ version in COPD patients. 7 The CASA-Q scores we found in our patients seem slightly worse than CASA-Q scores measured 43 days after a treated exacerbation in COPD patients. 12 The concurrent validity of the LCQ was very good between LCQ and the CASA-Q scores with strong and statistically significant correlations. Only the psychological domain was moderately but highly significantly correlated to SPUT-SP domain. The scientific value of this concurrent validity is particularly high. Indeed, contrarily to validations of other translations, we had the opportunity to use a highly specific questionnaire (CASA-Q) for the validation process. This questionnaire was previously validated for cough evaluation. 11 Even though a significant correlation was found between all domains of LCQ and CASA-Q, the hypothesized relationship of LCQ with sputum-related domains of CASA-Q should be discussed. Indeed, LCQ is specific to cough and its impact on daily life, whilst CASA-Q includes two domains related to sputum symptoms and their impact on daily life. This difference probably explains the moderate correlation we found between psychological domain of LCQ and SPUT-SP domain of the CASA-Q. However, sputum production is likely to mechanically stimulate coughing 17 on one hand, and sputum wet weight was related to cough symptom evaluation by COU-SP part of the CASA-Q 11 on the other hand, which justifies the investigation of this hypothesized relationship.
The content validity of the questionnaire was assessed by Pearson’s correlation coefficients between domains and total score of LCQ. Values greater than 0.30 are associated with an acceptable result. 18 The content validity of the questionnaire was very good with all of the coefficients higher than 0.90. The internal consistency was also excellent for all domains with Cronbach’s α scores varying between 0.802 and 0.917 and exceeding 0.7, which is classically considered as the acceptable cut-off for this purpose. 19 Our results are similar to the validations of this questionnaire in other languages showing Cronbach’s α varying between 0.67 and 0.93. 20,21
Ceiling and floor effects occur when 15% or more of the patients respond with a highest or lowest score, respectively. Similar to the English LCQ validation in COPD patients, 7 we did not observe these effects for any domain in our patients. Therefore, the validity can be considered as acceptable with discriminative extreme values.
The ICC for agreement was used to evaluate the test–retest reliability. It is the most suitable reliability parameter, 19 and it is more adequate than the ICC for consistency. 14 Reliability is considered as good when ICC is higher than 0.70. 22 Test–retest reliability was verified in our study for all of the domains and for the total score. Moreover, using the Bland and Altman method, we found bias of −0.27 and lower than −0.14 for total and domains scores, respectively. This bias is lower than the bias measured for total score of LCQ in its validation in COPD patients. 7 The Bland and Altman method 23 is an adequate method to observe absolute measurement errors between two repetitive tests. 19 Both instruments were administered again after 2 weeks, considering that this period is long enough to prevent the patients from remembering the previous test but as short enough to avoid changes in health status.
The effect size (ES) quantifies the difference between two measurements and is defined as small (d < 0.2), small to moderate (d between 0.2 and 0.5), moderate to large (ES between 0.51 and 0.79), and large (ES > 0.79). 24 In our study, the the values of ES were lower than 0.2 for all scores except for psychological domain (d = 0.45) highlighting good agreement between the measurements.
Besides the intrinsic known weaknesses of the questionnaires in general, one limitation of this study is the use of a single questionnaire for the validation process, but we believe that this limitation is countered by the specificity of the chosen questionnaire. Moreover, the stability of the patients between both administrations of the questionnaires could be discussed since it was only based on a subjective appreciation. Finally, responsiveness remains to be tested. However, all of the psychometric properties of a scale cannot be established in a single study. 25
In conclusion, the French version of LCQ is valid for the evaluation of the cough in COPD patients through GOLD stage 2 to 4. It was demonstrated by a significant correlation with a validated specific questionnaire related to symptoms and impact of cough and sputum (CASA-Q). Moreover, the reproducibility of the LCQ was verified in our sample of COPD patients.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.