
Abstract
Objective
To descriptively compare the clinical outcomes of drug-coated balloons (DCB) and plain balloon angioplasty (POBA) in hemodialysis patients with Below-The-Knee (BTK) peripheral artery disease.
Methods
This retrospective study included 96 hemodialysis patients (DCB:55 POBA:41). Outcomes included changes in Rutherford grade, wound healing, freedom from target lesion revascularization (CD-TLR), survival, and amputation-free survival.
Results
Both groups demonstrated improvement in Rutherford grade at 12 months. Wound healing occurred in 60.6% (95% CI 42.1–76.8) of the DCB group and 50.0% (95% CI 32.0–67.9) of the POBA group. Amputation-free survival was 72.7% (95% CI 59.0–83.0) with DCB and 67.7% (95% CI 52.5–80.0) with POBA. Freedom from CD-TLR was 78.9% (95% CI 65.0–88.5) for DCB and 91.6% (95% CI 79.0–97.0) for POBA. No clear between-group differences were observed.
Conclusion
No significant differences were observed between DCB and POBA in this small retrospective cohort.
Keywords
Introduction
The prevalence of peripheral artery disease (PAD) in the hemodialysis population ranges from 17–48%, which is significantly higher than in the general population. 1 Chronic limb-threatening ischemia (CLTI) represents an advanced stage of PAD. While its overall occurrence is rare, it is markedly more prevalent in patients undergoing hemodialysis and is often accompanied by multi-layered Below-The-Knee (BTK) arterial disease.2,3 Advanced renal failure has been associated with an increased frequency of complex lesions in the distal arteries of the lower limbs. 4 A variety of predictive models have been developed for the CLTI population. 5 End-stage renal disease (ESRD) is one of the significant factors affecting this group. 6 In some CLTI studies, populations with ESRD are explicitly excluded.7,8
International guidelines recommend intravascular interventional therapy as a first-line treatment for CLTI patients with multi-segment lesions. 9 Specifically, for TASC B lesions, endovascular therapy (EV) is recommended as the first-line approach, particularly in cases involving multiple short occlusions. Drug balloon dilatation, also known as drug-coated balloons (DCB) or paclitaxel (PTX) coated balloons are more effective than plain old balloon angioplasty (POBA) for the treatment of femoropopliteal artery disease.10,11 Although there is an international consensus supporting the use of DCB in femoropopliteal artery disease, evidence regarding their effectiveness in BTK lesions remains conflicting. 12 The potential benefits and risks of DCB manifest in various ways across different anatomical locations and clinical settings. 13 Unlike the femoropopliteal arteries, BTK lesions are associated with problems such as small diameter leading to a lack of suitable balloons, hard plaques making expansion difficult, lesions far from the heart, and low arterial pressure. Thus although the long-term success rate of DCB for BTK lesions has been improving, it is still insufficient to meet current clinical needs. 14 We therefore retrospectively evaluated and compared the efficacy and safety of DCB and POBA in hemodialysis patients with BTK arteries.
Methods
Study design and patients
This was a retrospective, multicenter, nonrandomized study. A total of 96 hemodialysis patients diagnosed with PAD who were admitted from December 2020 to December 2022 were analyzed retrospectively, including a total of 96 affected limbs. All patients received DCB or POBA for BTK lesions. This study was approved by the local ethics committee and applicable laws as stipulated by the Chinese government authorities. All patients provided written informed consent prior to enrollment, and consent for prospective data collection and analysis was explicitly included in the consent form.
During the study period, a total of 700 patients with peripheral artery disease (PAD) underwent BTK percutaneous transluminal angioplasty (BTK PTA) at the participating centres. Among them, 106 were on maintenance hemodialysis. A subset of ESRD patients (10 cases) underwent vessel preparation (atherectomy, cutting balloons, or drug-eluting stents) and were excluded according to exclusion criterion 5. The final study population therefore included 96 hemodialysis patients treated with either POBA or DCB without adjunctive vessel preparation.
The inclusion criteria were: (1) diagnosed with BTK artery stenosis (>70%) or occlusion by lower limb artery computed tomography angiography (CTA) or color Doppler ultrasound; (2) patent inflow tract, but treatment of stenotic or occlusive lesions (<15 cm), including the iliac, femoral, and popliteal arteries, allowed before treatment of BTK lesions, including both procedures performed in a prior session and those performed during the same session; (3) met the diagnostic criteria for symptomatic PAD, with Rutherford grade ≥3. (4) only patients with technically successful DCB or POBA procedures were included, and unsuccessful cases were excluded (n = 10). (5) met the diagnostic criteria for end-stage renal disease (ESRD) 15 and undergoing hemodialysis; and (6) complete medical records and signed informed consent. The exclusion criteria were: (1) planned amputation of the target limb; (2) thrombo-angiitis obliterans, acute arterial embolism, or inflammatory vasculopathy; (3) previous bypass surgery on the affected limb; (4) severe stenosis or occlusive lesions in the inflow tract, with lesion length ≥15 cm; (5) BTK lesions treated with cutting balloon, atherectomy, drug-eluting stent implantation, or other intracavitary interventional procedures; and (6) patients with severe cardiovascular or cerebrovascular diseases, drug allergies, etc. unable to receive interventional treatment.
Data collection
Clinical data were collected by experienced medical staff using a standardized case system to ensure the reliability of the data. All data were retrospectively collected from the medical records. Target lesions were evaluated by lower limb artery CTA, color Doppler ultrasound, and intraoperative digital subtraction angiography, and surgical results and surgery-related complications were recorded. All included patients were followed-up for 12 months from the first day of hospitalization (day 1), and follow-up was performed by the attending physician at 3 and 12 months, respectively. Lesions were assessed by color Doppler ultrasound or lower limb arterial CTA during follow-up, and data related to amputation, clinically driven-target lesion revascularization (CD-TLR), and all-cause mortality were collected. The cause of death was determined based on the death certificate and autopsy report. The primary outcome of this study was change in Rutherford grade at 3 and 12 months, and the secondary outcomes were 12-months freedom from CD-TLR and wound healing rates. Clinical outcomes included amputation, amputation-free survival, and all-cause mortality. In addition, patients were followed up every 2 weeks to receive wound care.
Diagnostic criteria
Calcification of target lesions was evaluated by Peripheral Artery Calcium Scoring System (PACSS). PACSS is a grading system specifically designed for calcification of lower extremity arteries, including the inferior knee artery, and is one of the recommended methods at present. 16 According to the CTA assessment of vascular calcification, the scoring system is as follows: No calcification is assigned 0 points; point or discontinuous calcification (scattered distribution) is assigned 1 point; continuous calcification of vessel length less than 1/3 is assigned 2 points; continuous calcification of 1/3 of the vessel length, but not fully annular, is assigned 3 points; and vessels that are completely annularly calcified are assigned 4 points. The diagnosis of PAD was based on physical examination, Rutherford grade, ankle-brachial index and lower extremity artery CTA.
Study procedures
According to the patient’s wishes, after full communication with the surgeon, choose to receive DCB or POBA interventional therapy. Dual antiplatelet therapy was given before interventional therapy, i.e., 100 mg aspirin and 75 mg clopidogrel daily for ≥3 days. Ipsilateral or contralateral femoral artery puncture was carried out under local anesthesia using a 6F arterial sheath. For lesions with relatively soft plaque or partial stenosis, a 0.014 or 0.018-inch guidewire was advanced through the true lumen under fluoroscopic guidance, minimizing the risk of dissection or perforation. For chronic total occlusions or severely calcified lesions where intraluminal passage was not feasible, the guidewire was carefully navigated through the subintimal space and then re-entered the true lumen distal to the lesion. In selected cases with severe distal occlusions, retrograde puncture of the BTK arteries at the foot or ankle under fluoroscopic or ultrasound guidance was performed to facilitate crossing and improve procedural success. Subsequently, patients in the POBA group were treated with a common balloon dilatation catheter, diameter 2.0–3.0 mm, to slowly dilate the diseased segment of the vessel step by step, with the balloon diameter matching the target vessel. On this basis, patients in the DCB group were selected to receive balloons coated with paclitaxel (3 µg/mm2) of the corresponding diameter (Orchid/Dahlia, Acotec Scientific, Beijing, China), with magnesium stearate used as a carrier, and the dilation time was set to 2 min. The length of the DCB balloon should cover the distal and proximal ends of the lesion segment, and if multiple DCBs were required to cover the entire lesion length, an overlap of ≥5 mm was required.
During the procedure, every effort was made to ensure that at least one BTK artery was successfully opened to establish adequate distal perfusion. Establish a direct blood flow pathway to the foot by opening the target vessel at the foot wound site, or at least open the plantar arch vessel through collateral branches to ensure sufficient blood flow for wound healing. After surgery, all patients received a subcutaneous injection of low molecular weight heparin, 100 IU/kg body weight, once every 12 h for 3–7 days. Patients were prescribed 100 mg of aspirin daily for life and were advised to continue using clopidogrel for ≥3 months. Some patients were given rivaroxaban for anticoagulation. Patients with wounds on the target limbs received sequential wound repair treatment.
Statistical analyses
Continuous variables were summarised as mean ± standard deviation or median (i.q.r.) as appropriate. Categorical variables were reported as counts and percentages. Comparative analyses between the DCB and POBA groups were descriptive only, and no hypothesis testing or P values were reported. Effect estimates for proportions were expressed with 95% confidence intervals, which were calculated using Wilson’s method, providing reliable estimates for small to moderate sample sizes. Kaplan–Meier curves were used to descriptively illustrate survival-related outcomes, with 95% confidence intervals presented. All analyses were performed using SPSS Statistics v.26 and GraphPad Prism v.7.
Results
Baseline characteristics of the study population
Patient characteristics.

Abbreviations: CABG, coronary-artery-bypass-grafting; PTCA, percutaneous transluminal coronary angioplasty.
Lesion characteristics.
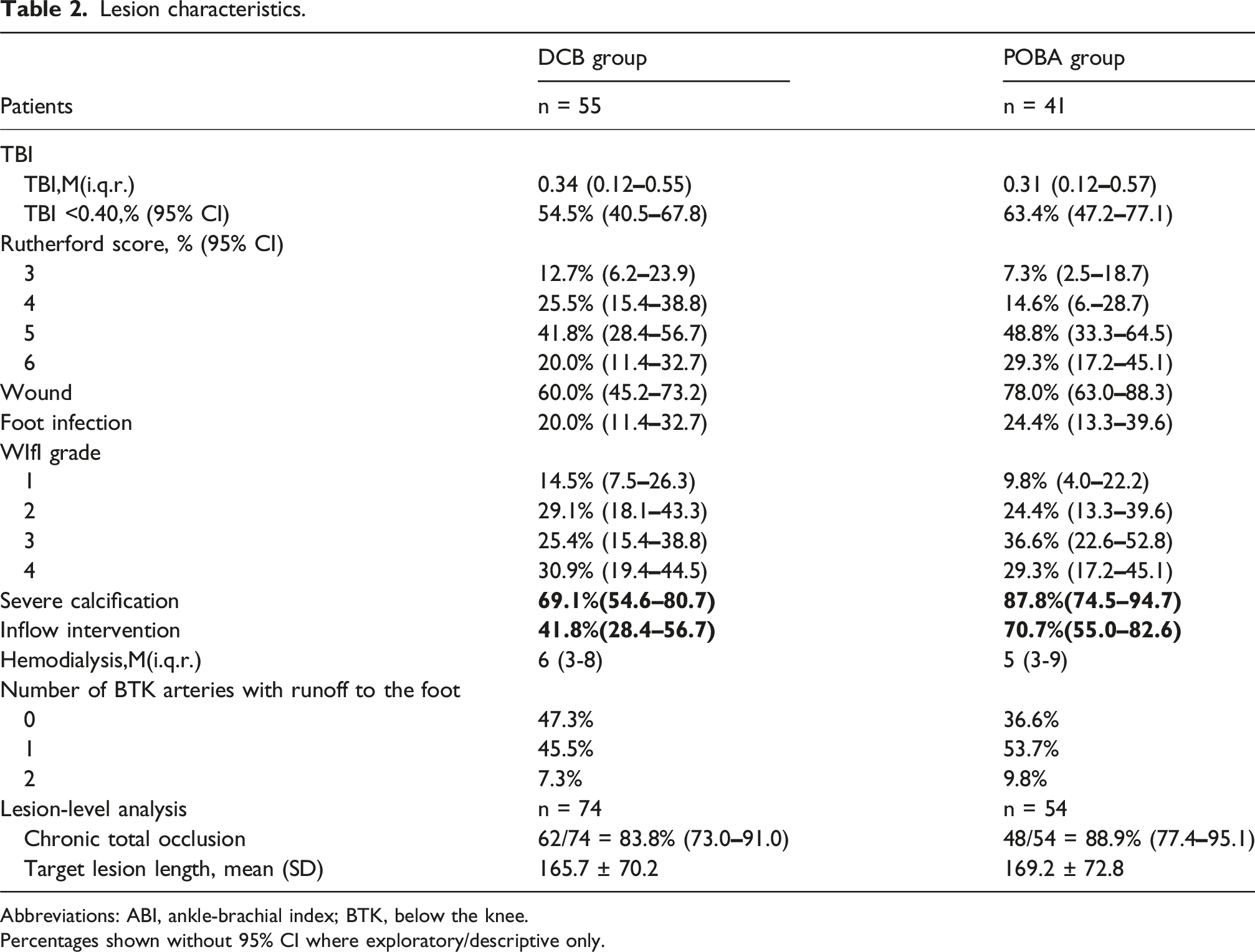
Abbreviations: ABI, ankle-brachial index; BTK, below the knee.
Percentages shown without 95% CI where exploratory/descriptive only.
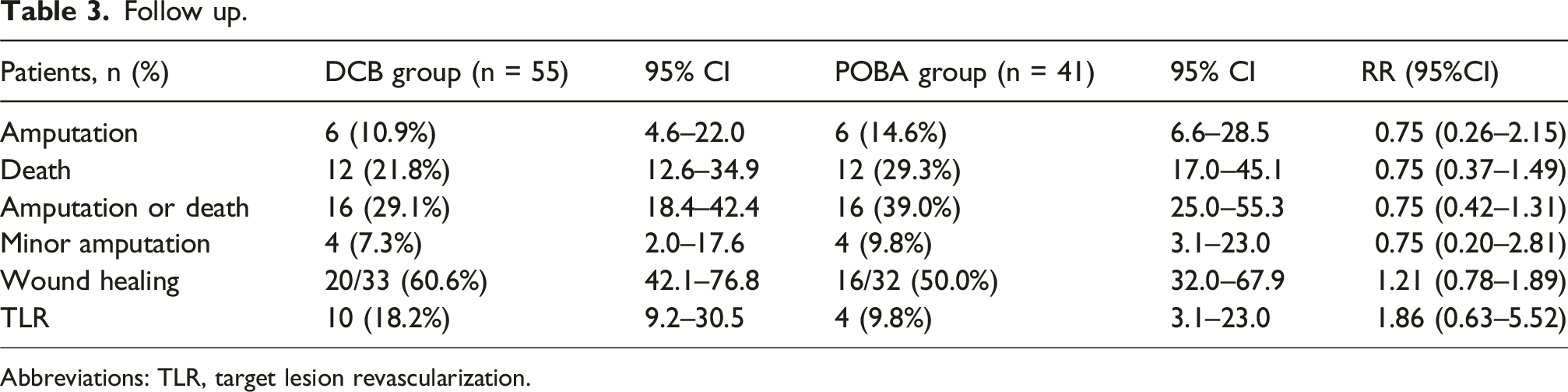
Follow-up
The improvements in Rutherford grade after interventional treatment in the two groups of patients are shown in Figure 1. The median Rutherford class decreased from 5 (IQR 4–5) at baseline to 4 (IQR 4–5) at 12 months in the DCB group, and from 5 (IQR 5–6) at baseline to 5 (IQR 4–5) at 12 months in the POBA group. Both groups demonstrated improvement over time in Rutherford grade. The follow-up data are presented in Tables 3 and 4. Among the 23 patients with Rutherford class 6, 8 underwent minor amputation. Minor amputations were not considered censoring events; subsequent wound healing of the amputation site was followed. Wound healing was assessed at the 12-months follow-up, with interim wound status monitored biweekly during dressing changes. At 12 months, wound healing occurred in 60.6% (95% CI 42.1–76.8) of the DCB group and 50.0% (95% CI 32.0–67.9) of the POBA group. 12-months survival was 81.8% (95% CI 69.1–90.3) for DCB and 79.1% (95% CI 64.9–89.0) for POBA. Amputation-free survival was 72.7% (95% CI 59.0–83.0) for DCB and 67.7% (95% CI 52.5–80.0) for POBA. Freedom from TLR occurred in 78.9% (95% CI 65.0–88.5) and 91.6% (95% CI 79.0–97.0), respectively. The differences in survival, amputation-free survival, and freedom from TLR between the DCB and POBA groups according to Kaplan-Meier analysis are shown in Figure 2. Improvement of Rutherford grade of (a) DCB; (b) POBA. Follow up. Abbreviations: TLR, target lesion revascularization. K-M survival analysis. Abbreviations: TLR, target lesion revascularization. Kaplan-Meier analysis (a) survival; (b) Amputation free survival; (c) freedom from TLR.


To further clarify outcomes by lesion type, subgroup analyses were performed according to stenosis versus occlusion. In the stenosis subgroup (n = 30), 12-months amputation-free survival was 69.7% for DCB and 73.0% for POBA, with no clear differences. In the occlusion subgroup (n = 65), amputation-free survival was 73.3% for DCB and 65.9% for POBA, also without clear differences. Freedom from clinically driven TLR at 12 months did not clearly differ between DCB and POBA in either the stenosis (75.8% vs 87.9%) or occlusion subgroup (79.3% vs 92.8%). These descriptive findings do not suggest any clear short-term differences between DCB and POBA. Subgroup findings are descriptive, confidence intervals were not calculated due to small subgroup sizes.
Discussion
Hemodialysis promotes the rapid progression of PAD 17 and is more likely to affect distal lesions. 18 Some previous studies found high amputation and long-term mortality rates in hemodialysis patients after interventional therapy.19,20 Despite a recent increase in studies assessing endovascular treatment of BTK lesions,21,22 the optimal interventional approach for BTK patients undergoing hemodialysis is still unclear. Further studies are therefore needed to investigate and compare the efficacy and safety of DCB and POBA in BTK patients undergoing hemodialysis.
In this small retrospective study, no clear differences were observed between DCB and POBA in hemodialysis patients with BTK PAD. However, further improvements are needed to enhance patient prognosis. It should also be noted that all patients received structured bi-weekly wound care throughout follow-up. This intensive wound management likely contributed to improvements in Rutherford grade and wound healing in both groups, thereby attenuating observable differences attributable to the angioplasty device itself. As such, the clinical outcomes should be interpreted within the context of combined revascularisation and wound-care strategies rather than device-specific efficacy alone.
Freedom from TLR is an important clinical endpoint for assessing the prognosis of patients with BTK lesions. 23 Previous studies indicated that the rate of freedom from TLR was higher in patients undergoing DCB compared with POBA for BTK lesions.24,25 In contrast, the present results indicated that the rate of freedom from TLR was higher in the POBA group compared with the DCB group, but no clear between-group differences were observed. This may be because most patients in the current POBA group did not pursue further treatment, and most patients included in this study were end-stage patients. Patients in the POBA group had more severe vascular calcification and more frequently underwent inflow interventions, indicating a heavier baseline lesion burden in this group. Interventional therapy is more cost-effective in ESRD patients. 26 In China, the cost of DCB is much higher than POBA, and end-stage patients with poor target lesion conditions are thus more likely to choose POBA. Other characteristics noted below may also affect the efficacy of interventional therapy for BTK in hemodialysis patients.
CKD independently increases the risk of developing PAD, with symptoms worsening as CKD progresses. 27 PAD symptoms in hemodialysis patients often manifest as ischemic ulcers or gangrene, rather than rest pain. 28 Matsumi et al. found that the long-term outcomes of interventional treatments for PAD were worse in hemodialysis compared with non-hemodialysis patients 29 ; however, the surgical success rate for BTK lesions alone was similar between patients with and without hemodialysis, although hemodialysis patients had a higher incidence of major adverse limb events. 30
Vascular calcification is a major complication of CKD, and previous studies showed a positive linear relationship between vascular calcification and mortality rates in patients with CKD and ESRD.31,32 This active, complex process involves regulatory proteins typically associated with bone formation, leading to vascular ossification. 33 Hemodialysis patients have reduced serum protection against vascular calcification, 34 which promotes PAD progression, which in turn represents a major cause of death in these patients. 35 Vascular calcification, hemodialysis, and PAD thus exacerbate each other, worsening the patient’s condition. The severe vascular calcification and poor condition of patients in the present study explain the similar outcomes between the DCB and POBA groups.
The amputation-free survival rates in the DCB and POBA groups in this study were 72.7% and 67.7%, respectively, and the wound healing rates were 60.6% and 50.0%, respectively, with no clear differences in either outcome between the DCB and POBA groups after intervention. CLTI, as the terminal stage of PAD, is closely related to patient mortality, amputation, and quality of life, 36 and is included in grades 4–6 in the Rutherford classification. 37 In this study, the majority of patients had CLTI. Notably however, in addition to ischemia, wound and foot infections are also crucial factors that contribute to amputation and mortality in CLTI patients.38,39 Among the current patients, 67.7% of the target limbs had wounds and 21.9% had foot infections.
Since the Wound, Ischemia, and Foot Infection (WIfI) classification was proposed by the Society for Vascular Surgery in 2014, 40 it has been increasingly used by clinical centers to evaluate the status and severity of CLTI patients, in order to make more effective clinical decisions. 41 The WIfI classification comprehensively evaluates patients with CLTI based on three factors: wound, ischemia, and foot infection, and has demonstrated predictive power for amputation and wound healing.42,43
Although amputation-free survival was analysed according to treatment group, patients with more advanced clinical disease severity, such as higher Rutherford grades and WIfI grade 4, may be more prone to adverse limb outcomes. This interpretation is consistent with established clinical risk stratification systems and should be interpreted as exploratory. During surgery, a direct blood flow path to the foot should be established as much as possible, and the patency of the arch of the foot will affect the blood perfusion of the ischemic area after the intervention of the BTK artery, thereby affecting the ulcer healing rate. 44 Restoring sufficient blood flow to the corresponding ulcer is essential for full wound healing, especially in CLTI patients. 45 Wounds should thus be followed-up early in PAD patients undergoing hemodialysis, and nursing management should be emphasized. 35 These findings should be regarded as hypothesis-generating rather than definitive evidence. Larger, prospective, randomized studies are warranted to validate these observations and to provide more robust guidance for clinical practice.
Limitations
This study has several limitations. First, the retrospective design may introduce information bias, and only technically successful procedures were included (n = 10 failures excluded), which may limit generalisability. The two groups were not fully balanced at baseline, and the limited sample size precluded meaningful propensity score matching, as matching would have markedly reduced the analytic cohort and produced unstable estimates. Therefore, only descriptive effect estimates with 95% confidence intervals were reported, and the findings should be considered hypothesis-generating. Second, all patients received structured bi-weekly wound care during follow-up, which may have contributed to clinical improvement and attenuated potential device-related differences. Third, this study included only hemodialysis patients with ESRD and excluded those who underwent vessel preparation. In our centres, atherectomy and specialised BTK preparation devices were not routinely used during the study period due to cost constraints, device availability, and local practice patterns favouring a simpler POBA or DCB-only strategy. Because vessel preparation is considered standard practice in many high-volume centres, caution is needed when generalising our results to broader BTK populations. Finally, outcomes were assessed only up to 12 months, and long-term prognosis and dialysis-related effects were not evaluated.
Conclusion
In this small retrospective cohort of hemodialysis patients with BTK lesions, no significant differences were observed between DCB and POBA. These hypothesis-generating findings highlight the need for larger prospective randomized studies.
Footnotes
Author note
The authors did not use AI tools for writing.
Acknowledgments
We have not received substantial contributions from non-authors. No AI tools were used in manuscript preparation.
Ethical considerations
The study was approved by the local ethics committee board and applicable laws as specified by Chinese government authorities. The study received approval from the Research Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (2023-ke-12).
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Beijing Chaoyang Hospital, Capital Medical University Science and Technology Innovation Fund (21kcjj-11) and Innovation and Technology Commission, The Government of the Hong Kong Special Administrative Region (ITP/041/19TP). They had no involvement in the study design or collection, analysis, and interpretation of data. They paid for the purchase of equipment and a professional editor to assist with writing the manuscript. They were not involved in the decision to submit the manuscript for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article.
Guarantor
Sheng-Xing Wang: MD; Department of Vascular Surgery, Beijing Chaoyang Hospital, Capital Medical University, Beijing, China