
Abstract
Objective
To compare the results of endovascular therapy for chronic limb-threatening ischemia (CLTI) in patients categorized under the gray and yellow zones of the patient risk, limb severity, and anatomic pattern (PLAN) concept over a 2-year follow-up period.
Methods
Patients who underwent endovascular therapy for peripheral artery disease and presented with CLTI from February 2017 to February 2019 were retrospectively reviewed. The patients were grouped into yellow and gray zones based on the PLAN concept. Preoperative and postoperative walking distances, Rutherford classes, and postoperative target vessel patency rates were recorded and compared between the groups. Follow-up evaluations were performed at 1, 6, 12, and 24 months post-procedure.
Results
Of the 387 patients evaluated, the yellow and gray groups comprised 88 patients each. The overall patency rates were similar between the groups (84 (95.45%) vs. 81 (92.05%), respectively). The occlusion-/stenosis-free survival times, amputation-free survival time, and mean survival time were not significantly different. However, the gray group had a significantly higher number of atherectomy interventions (74 vs. 59) and crosser devices used (62 vs. 42).
Conclusion
Endovascular therapy is an effective treatment option for patients in the gray zone of the PLAN color coding system.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) is characterized by chronically inadequate tissue perfusion, and it has a high prevalence and is associated with significant healthcare costs. 1 However, the rapid development of diagnostic tools, devices, and medications has offered new treatment options for patients with CLTI.
In the treatment of CLTI, the Global Vascular Guidelines (GVG) have espoused for evidence-based revascularization (EBR) as a conceptual framework. 2 EBR relies on a structured management system that incorporates patient risk, limb severity, and anatomic pattern of disease (PLAN) to facilitate clinical decision-making. Within the PLAN concept, the initial revascularization strategies for infrainguinal disease are classified as open bypass (coded by green), endovascular (coded by yellow), indeterminate (coded by gray), or no revascularization (coded by red) based on the Wound, Ischemia, and foot Infection (WIfI) stage and the Global Limb Anatomic Staging System (GLASS) stage.
This retrospective study was performed to compare the outcomes of patients in the gray and yellow zones of the PLAN concept who underwent endovascular therapy (EVT) during a 2-year follow-up period.
Methods
We retrospectively evaluated patients who underwent endovascular interventions for infrainguinal peripheral artery disease (PAD) from February 2017 to February 2019 at our institution. Patients with concomitant or solitary suprainguinal disease, concomitant aortic disease, and acute limb-threatening ischemia were excluded. When patients underwent endovascular interventions for bilateral lower extremity PAD, the extremity with the most severe disease was included in this study.
The patients were color-coded according to the GVG on the Management of CLTI published in 2019. 2 Classifications of all patients were determined by preoperative computed tomography angiography and physical examination. As outlined in the guidelines, the WIfI classification was used to determine the WIfI stage, and the GLASS was used to determine the GLASS stage. The Vascular Quality Initiative CLTI Mortality Prediction Model, which was published by Simons et al. 3 in 2019, was used to determine the patients’ mortality risk.
The study protocol was approved by the Baskent University Institutional Review Board and Ethics Committee (Project No: KA20/195). The study protocol was developed in accordance with the Declaration of Helsinki. All patients provided written informed consent for the procedures, data collection, and future analysis for academic purposes. In accordance with ethical guidelines, all patient details have been de-identified to ensure their complete anonymity and privacy. No personally identifiable information is disclosed in this study.
Procedures
All procedures were performed under local anesthesia. Prior to the procedure, all patients were premedicated with clopidogrel (75 mg/day), aspirin (100 mg/day), and atorvastatin (20 mg/day); additionally, cilostazol (200 mg/day) was initiated at least 1 week before the procedure and continued for at least 1 year thereafter. Treatment of significant stenosis or occlusion of the inflow superficial femoral artery was prioritized before treating infrapopliteal artery lesions. The approach and timing of superficial femoral artery treatment, including single-stage or multistage procedures, were determined at the operator’s clinical discretion.
To establish vascular access, an antegrade approach from the ipsilateral common femoral artery or a retrograde approach from the contralateral femoral artery with a 7-Fr sheath was used under ultrasound guidance with a linear probe (Aloka ProSound Alpha 7; Hitachi Healthcare Americas, Twinsburg, OH, USA). After proper positioning of the sheath, unfractionated heparin (5000 IU) was routinely administered into the artery. Initial angiograms were taken, and a combination of guidewires including a 0.018-inch guidewire (Connect; Abbott Laboratories, Abbott Park, IL, USA) and one of several 0.014-inch guidewires (Command/Command ES; Abbott Laboratories) (Winn 40, 80, or 200; Abbott Laboratories) (V-14; Boston Scientific, Marlborough, MA, USA) was used to successfully cross the lesion in an antegrade direction with the support of a catheter (Seeker; Bard Peripheral Vascular Inc., Tempe, AZ, USA). Under roadmap guidance, the occlusions were crossed endoluminally by a guidewire either with the support of a Seeker catheter or with a chronic total occlusion (CTO) recanalization catheter (Crosser; Bard Peripheral Vascular Inc.).
Antegrade failure was defined as the inability to pass a guidewire through the distal portion of the occluded vessel via the access site, which was located either in the contralateral artery or proximal to the CTO lesion. Retrograde puncture was typically performed in the distal segments of the tibial or pedal arteries under fluoroscopy or ultrasound guidance, with the aim of avoiding bleeding complications and damage to the punctured artery. When traditional endoluminal revascularization failed, the parallel wire technique or retrograde distal access (percutaneous puncture and retrograde crossing–reconnection with the antegrade approach) and rendezvous technique were employed. The pedal–plantar loop technique was used to achieve adequate blood flow when the retrograde approach from the plantar arch was used to treat the target vessel (anterior or posterior tibial artery) because of the impossibility of antegrade crossing. 4 Intraluminal crossing was used to cross every lesion.
Following successful intraluminal crossing, predilatation was performed using an uncovered balloon (Bantham or Ultraverse; Becton Dickinson, Franklin Lakes, NJ, USA) that was 0.5 mm smaller in diameter than the reference vessel diameter, which was measured at both ends of the target lesion in the healthy segment and represented the intended diameter of the drug-coated balloon (DCB), at nominal pressure for 1 minute. When the lesion was hard, eccentric, severely calcified, or had advanced atherosclerotic disease, directional atherectomy was performed using a HawkOne device (Medtronic, Minneapolis, MN, USA). Control angiography was performed in two orthogonal projections to evaluate the precise diameter of the final DCB, assess recoil, and identify remaining plaques. Another DCB (Lutonix; Becton Dickinson) was subsequently applied at nominal pressure for 3 minutes, covering beyond the predilated area to avoid geographic miss and treating from healthy-to-healthy zones. If more than one DCB was used in the same vessel because of the lesion length, the DCBs were inflated from distal to proximal, with a 1-cm overlap between the DCBs to avoid geographic miss.
The use of a distal embolic protection device was not possible because of the reimbursement requirements of the social security institution.
Wound care strategy
Prior to the vascular interventions, all patients underwent sharp debridement regardless of their vascular pathology. Empirical antibiotic therapy was initiated upon admission and adjusted based on the wound culture results obtained during the initial debridement procedure. The goal was to promote formation of a granulation tissue layer using silver or negative-pressure wound dressing. Patients with complete vascular integrity and without osteomyelitis or infection received at least six doses of intralesional epidermal growth factor (Heberprot-P 75 mg; Hasbiotech İlaç San, Kayseri, Turkey) to increase the rate of granulation. Hyperbaric oxygen therapy was administered in at least 20 sessions to all patients without contraindications to this treatment. If sufficient granulation tissue formed, the wound was either closed with a split skin graft or left open for secondary healing. The Wagner scale was used to classify the depth and grade of ulcers. 5
Patient follow-up
Patients underwent regular outpatient follow-up evaluations at 1, 6, 12, and 24 months post-procedure. A multidisciplinary team comprising a vascular surgeon, a radiologist, and, if needed, a general surgeon with expertise in wound care monitored the patients during these follow-ups. Patency was evaluated using duplex ultrasound at 1, 6, 12, and 24 months, and the peak systolic velocity ratio was used to calculate the patency rates. A peak systolic velocity ratio of >3.5 or peak systolic velocity of >300 cm/s was considered to indicate >75% stenosis. Wound healing was visually evaluated for the degree of granulation tissue formation, presence of infectious discharge or debris, and other wound-related issues during the follow-up visits. If patients had concerns about wound healing, the duplex studies, angiographic evaluation, and reintervention were planned accordingly. Criteria for reintervention included recurrent symptoms of pain at rest or ulceration despite medical treatment as well as restenosis or re-occlusion diagnosed on duplex ultrasound.
Statistical analysis
The statistical analysis was conducted using SPSS for Windows, Version 16.0 (SPSS Inc., Chicago, IL, USA). Categorical variables are presented as number and percentage, and continuous variables are presented as mean ± standard deviation. The normality of the data distribution was assessed using the Kolmogorov–Smirnov test. To mitigate selection bias and potential confounding, propensity score matching was performed with a one-to-one matching ratio and nearest-neighbor matching algorithm. Logistic regression analysis was used to calculate propensity scores for preoperative baseline characteristic variables. The adequacy of the propensity score model was evaluated using the Hosmer–Lemeshow goodness-of-fit test; this yielded a chi-square value of 4.71 (P = 0.787), indicating that the model was well-calibrated. Categorical variables were analyzed using the chi-square test and Fisher’s exact test, and continuous variables were analyzed using the independent-samples t-test. The survival time from occlusion was assessed using the Kaplan–Meier method, and patency rates were compared between the groups using the log-rank test. Statistical significance was defined as a P-value of <0.05. Additionally, Bonferroni correction was applied, and a new P-value (P = 0.00083) was calculated for the chi-square comparisons of the GLASS stage and WIfI stage between the groups, with the statistical significance evaluated accordingly.
Results
Of 387 patients who were initially evaluated in this retrospective study, 307 had CLTI and were ultimately included. These patients were divided into two groups based on the PLAN concept color coding described in the GVG. 2 In total, 109 (35.50%) patients were coded as yellow (yellow group), and 198 (64.50%) patients were coded as gray (gray group). The gray group comprised patients who were not suitable for surgical intervention, lacked suitable in situ graft presence, and declined surgical intervention. Upon initial evaluation, significant differences in smoking, diabetes mellitus, coronary artery disease, and chronic kidney disease were observed between the two groups. Propensity matching was performed to minimize the impact of these differences, yielding 88 patients in each group. The details of the preoperative characteristics of the two groups before and after propensity matching are presented in Table 1.
Preoperative data.
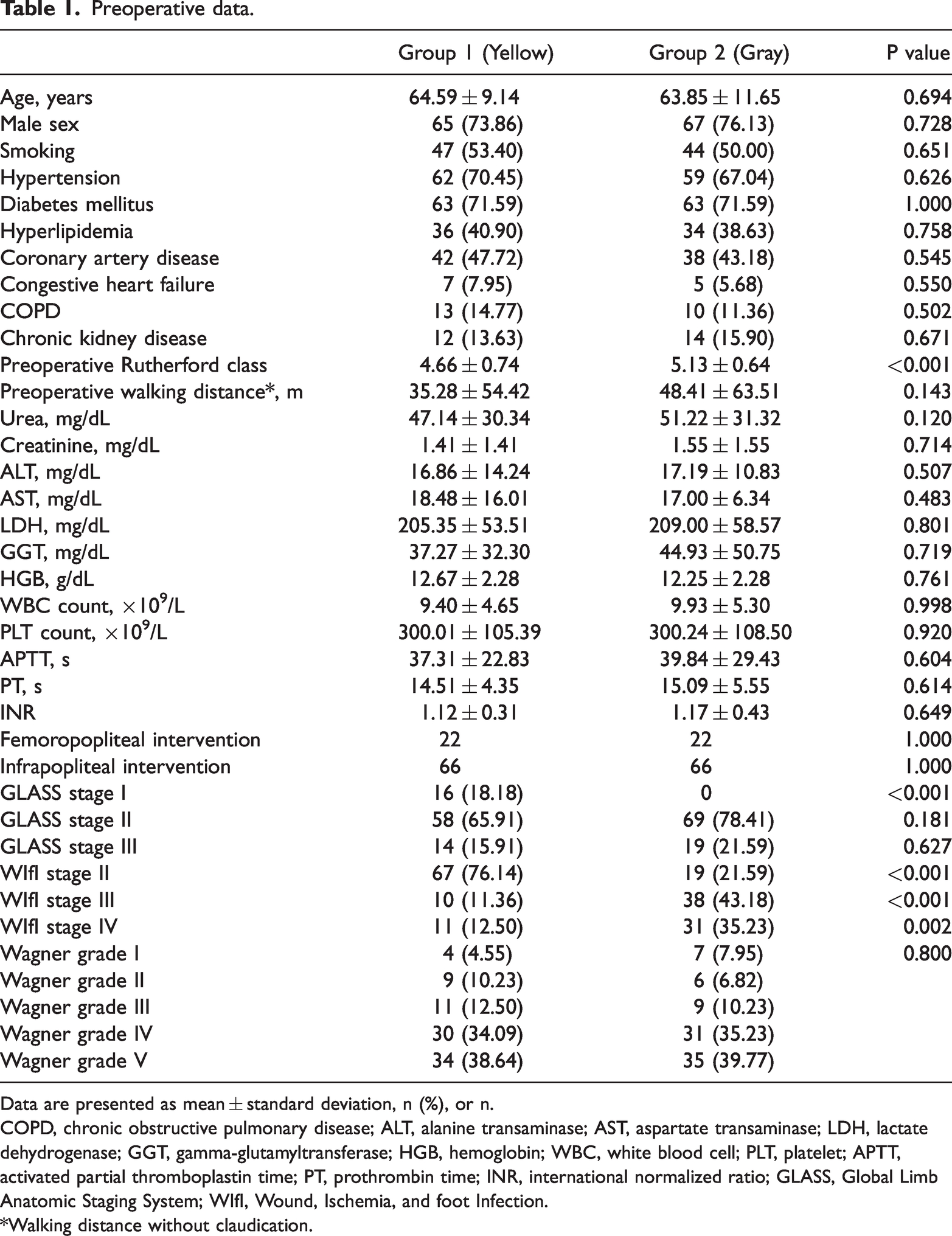
Data are presented as mean ± standard deviation, n (%), or n.
COPD, chronic obstructive pulmonary disease; ALT, alanine transaminase; AST, aspartate transaminase; LDH, lactate dehydrogenase; GGT, gamma-glutamyltransferase; HGB, hemoglobin; WBC, white blood cell; PLT, platelet; APTT, activated partial thromboplastin time; PT, prothrombin time; INR, international normalized ratio; GLASS, Global Limb Anatomic Staging System; WIfI, Wound, Ischemia, and foot Infection.
*Walking distance without claudication.
The study cohort had a mean follow-up time of 11.41 ± 8.88 months. The mean follow-up time in the yellow and gray groups was 11.18 ± 7.24 and 11.54 ± 7.75 months, respectively, with no significant difference. The yellow group demonstrated patency rates of 100.00%, 98.41%, 95.24%, and 81.77% at 1, 6, 12, and 24 months, respectively. The corresponding patency rates in the gray group were 100.00%, 98.51%, 96.04%, and 72.88%. The mean survival time from occlusion was 23.62 ± 0.61 months in the yellow group and 23.28 ± 0.60 months in the gray group, while the mean survival time from amputation was 23.68 ± 0.59 months in the yellow group and 23.58 ± 0.59 months in the gray group. The occlusion-/stenosis-free survival times and amputation-free survival times were not significantly different between the groups (Figures 1 and 2, respectively). In terms of the improvement in walking distance without claudication, the yellow group had a mean increase of 280.85 ± 149.54 m postoperatively, while the gray group had a mean increase of 253.86 ± 142.83 m. However, there was no significant difference between the two groups. The number of atherectomy interventions and crosser devices used were significantly higher in the gray than yellow group. Specifically, 74 (84.09%) patients in the gray group but only 59 (67.05%) in the yellow group underwent atherectomy interventions (P = 0.009). Additionally, 62 (70.45%) patients in the gray group but only 42 (47.73%) in the yellow group received crosser devices (P = 0.002). There was no significant difference in the number of directional atherectomy devices used between the groups. The primary success rates, amputation rates, and wound healing rates at 1 year were similar between the two groups. Additionally, the achievement of wound healing at 1 year was similar in both groups (77 (87.50%) patients in the yellow group and 73 (83.95%) patients in the gray group). No statistically significant differences were observed in any other postoperative data, which are presented in Table 2.

Occlusion-free survival.
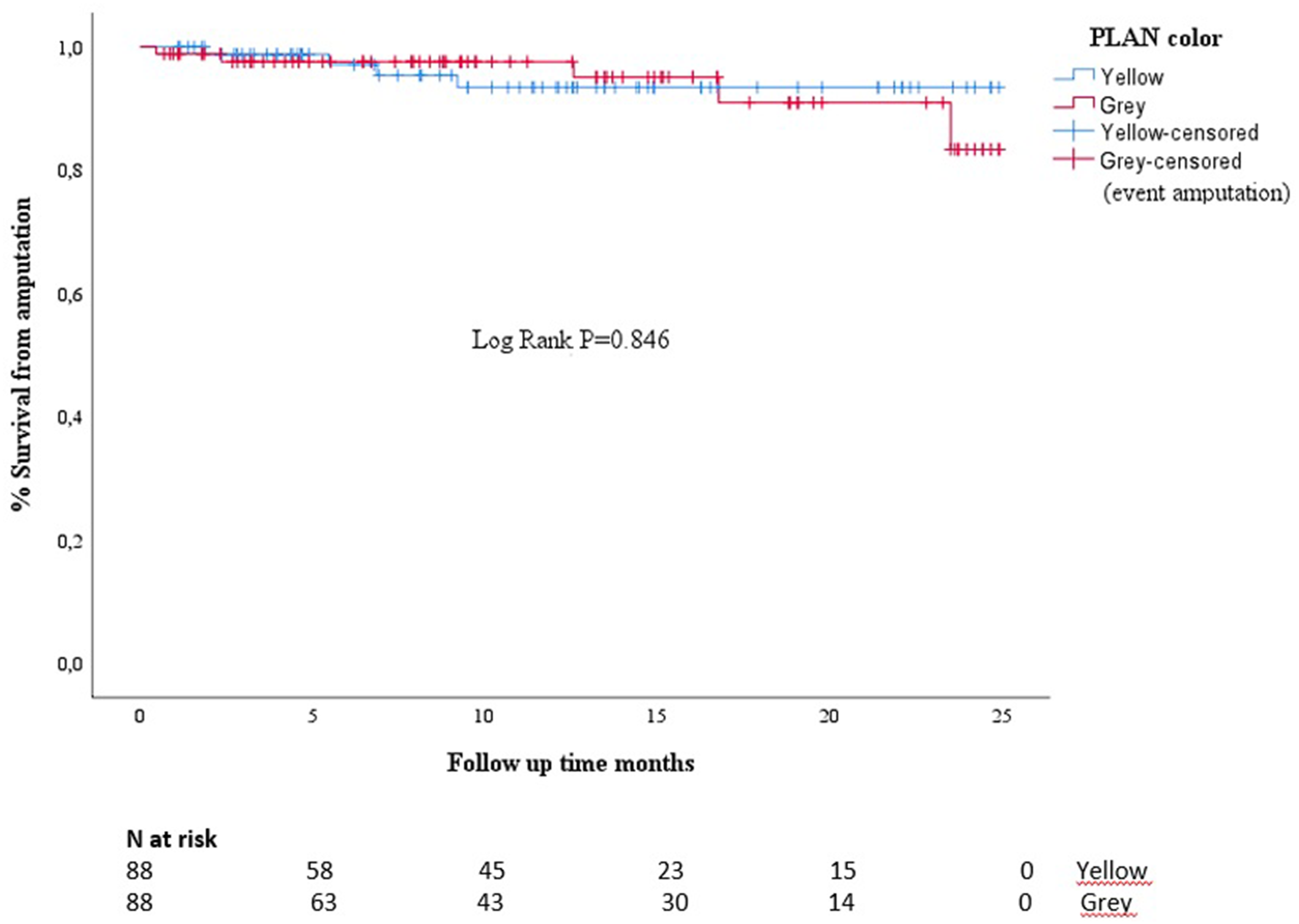
Amputation-free survival.
Postoperative data.
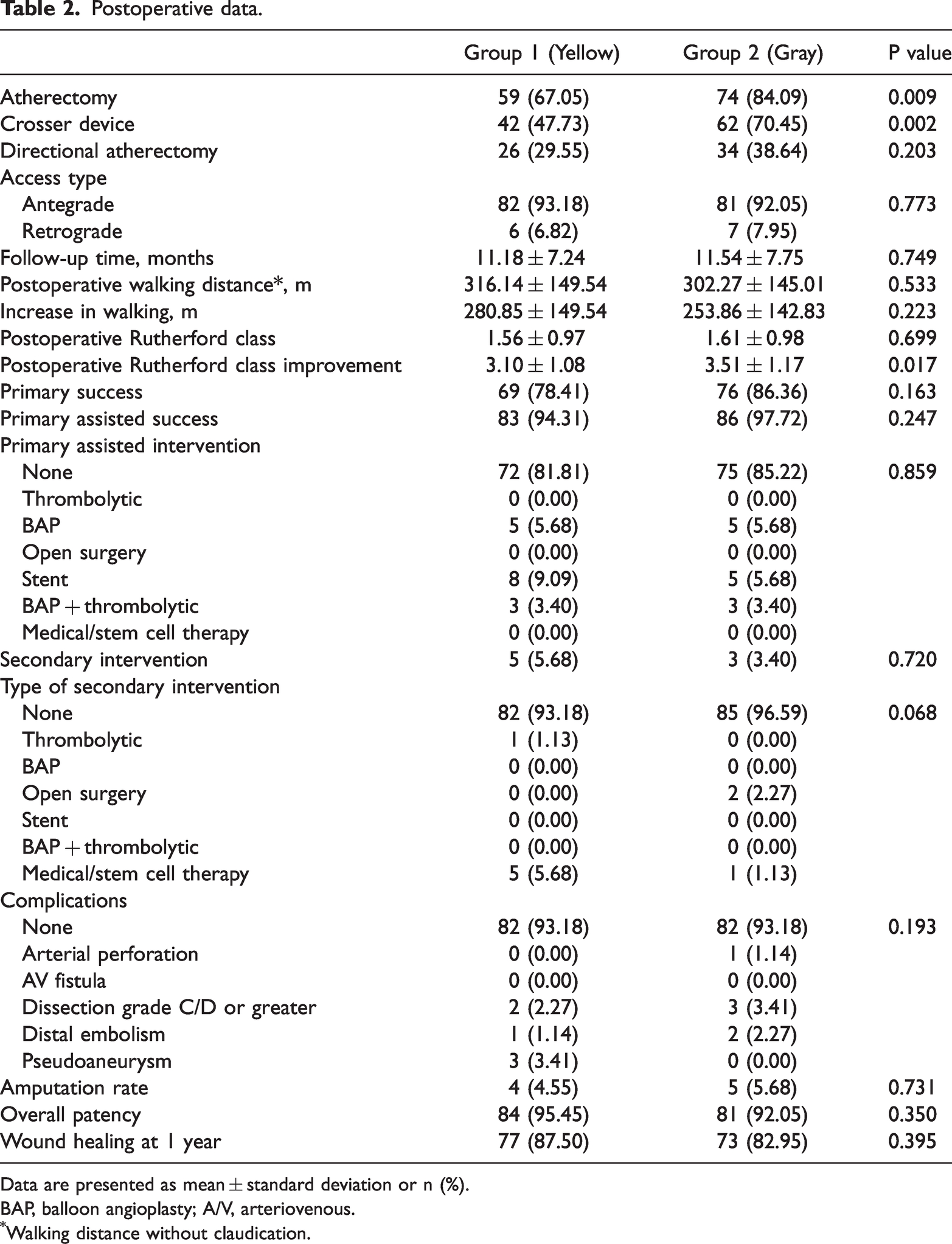
Data are presented as mean ± standard deviation or n (%).
BAP, balloon angioplasty; A/V, arteriovenous.
Walking distance without claudication.
Discussion
The results of this study show that patients in the gray zone of the PLAN classification may be effectively treated with EVT.
The concept of EBR has the potential to drive advancements in the treatment of patients with CLTI by accounting for the broad spectrum of clinical severity and anatomical complexity associated with the disease. As outlined in the 2019 GVG, EBR represents a key objective for enhancing the quality of vascular care and minimizing disparities in treatment approaches and outcomes. The PLAN concept of EBR provides a structured approach to patient management that considers the risk level, limb severity, and anatomical disease pattern. 2 However, the concept of EBR is not without its ambiguities, particularly in the context of infrainguinal PAD, for which a consensus on optimal treatment strategies may be lacking.
At our institution, we encounter a high number of patients with CLTI, and we offer both surgical and endovascular approaches based on the patient’s status and multidisciplinary management. Considering the cardiovascular morbidity of patients with CLTI, the less invasive endovascular approach has been regarded as the primary treatment modality when feasible. 6 Revascularization remains the mainstay therapy for patients with CLTI because restoring an adequate blood supply is crucial for symptom relief and wound healing. 7 If CLTI is left untreated, the overall rate of limb loss is estimated to be 25% within 1 year. 8
Below-the-knee lesions are a major contributing factor in CLTI, and their treatment poses a significant challenge because of their long length, small vessel diameter, and severe calcification of the vessel wall. Impaired or poor outflow tracts are additional contributing factors. 9 Advancements in crossing techniques for long lesions, the introduction of novel devices, and the use of distal access sites have enhanced the success rate of EVT procedures for such lesions. 10 However, endovascular treatment of infrapopliteal lesions is subject to drawbacks such as postprocedural recoil, dissection, and restenosis. 11 A meta-analysis by Romiti et al. 12 showed a primary patency rate of 58% for infrapopliteal angioplasty in patients with CLTI after 1 year.
Aihara et al. 13 reported that the 1- and 5-year primary patency rates of EVT in patients with Trans-Atlantic Inter-Society Consensus-II (TASC-II) C and D femoropopliteal disease were 67.8% and 45.2%, respectively. However, patients who underwent open surgical bypass had significantly better results in their study (82.1% and 69.4%, respectively, P = 0.001). The authors reported that the 1- and 5-year secondary patency rates were 90.1% and 85.1% in patients who underwent EVT and 93.2% and 79.5% in those who underwent open surgery, respectively. The 5-year patency rate was slightly better in patients who underwent EVT, but the difference was not statistically significant. The authors also reported a significantly lower rate of overall complications in patients who underwent EVT than in those who underwent open surgical bypass (3.5% vs. 14.4%, respectively; P. <0.01). 13
Dayama et al. 14 compared the outcomes of endovascular-first and bypass-first revascularization in 1355 patients with CLTI and isolated infrageniculate artery disease. The authors found that the unadjusted 30-day rate of major adverse limb events, such as loss of patency, major reintervention, or transtibial or proximal amputation, was 9.0% (48 patients) in the bypass-first group and 11.2% (92 patients) in the endovascular-first group. 14 Although the results were unfavorable for EVT, the difference was not statistically significant. In the present study, we study investigated the outcomes of EVT in patients with CLTI. Our findings demonstrated that the amputation rates, reintervention rates, and 1-year wound healing rates were similar between the groups. Furthermore, our observed rates were notably lower than the amputation rates reported in the aforementioned study. Based on these results, it is reasonable to suggest that well-performed EVT procedures may lead to better outcomes than open surgery.
The equivalence in the comparative efficacy of EVT and open surgical bypass for patients with CLTI, as reported in the current literature, presents a dilemma in the clinical decision-making process. Our study provides valuable insights into this debate, indicating similar or marginally better (but statistically non-significant) outcomes for patients undergoing EVT. Our findings thus offer meaningful contributions to resolving this ambiguity and underlining the viability of EVT as a promising therapeutic modality for patients with CLTI.
In this study, we employed various techniques including CTO support catheters, CTO recanalization catheters, atherectomy devices such as the Crosser, and directional atherectomy for successful passage of lesions, and we reserved the use of DCBs for the final stages of the procedures. At our institution, we adhere to the “leave-nothing-behind” approach for endovascular procedures, placing a strong emphasis on vessel preparation. The presence of heavily calcified lesions represents a mechanical barrier and may limit the benefits of DCBs. Consequently, vessel preparation techniques such as atherectomy and scoring/cutting-edge balloon angioplasty are implemented to address this challenge.15–17 Additionally, our approach has positive effects on the procedure success rates and long-term outcomes.18,19
The Rutherford symptomatic classification of CLTI was adapted in 1997 and has since been widely used. 20 In our study, the gray group comprised patients with more severe clinical presentations, resulting in a significantly higher preoperative Rutherford classification score when compared with the yellow group. However, in the postoperative period, the Rutherford class improvement score was significantly higher in the gray than yellow group, indicating that patients in the gray group derived greater benefit from EVT. This suggests that EVT may be more effective in patients with more severe disease presentations.
We hypothesize that the high rate of acute procedural success and low incidence of complications observed in our study may be attributed to the use of retrograde access following failure of antegrade access. The challenges encountered during the crossing of occlusions are thought to be associated with the characteristics of the plaque, with CTOs being particularly challenging because of their fibrous nature, presence of diffuse calcification, and harder proximal cap. As such, retrograde access may offer an effective solution for these difficult-to-treat lesions.21,22
The findings of our study align with the 2-year follow-up results of the recently published BEST-CLI and BASIL-2 trials,23,24 demonstrating parallel outcomes. This suggests that in the future, the preferred approach (especially for patients lacking suitable in situ venous grafts) is likely to lean towards endovascular treatment, much like our current practice.
De Athayde Soares et al. 25 evaluated 95 patients who underwent infrapopliteal endovascular procedures. They grouped the patients according to the angiosome concept and WIfI staging. They found no significant differences in the limb salvage or wound healing rates between the groups. They concluded that the angiosome concept was no longer important in the endovascular treatment of infrapopliteal peripheric artery disease. 25 In our study, the WIfI stage was higher in the gray group, but the wound healing rates and amputation-free survival were not significantly different between the groups. Our results are in agreement with the aforementioned study.
Limitations
Because this was a retrospective study, randomization and comparison were conducted among patients with follow-up observations, and the results were evaluated accordingly.
Few diagnostic techniques are available to precisely measure critical parameters such as blood flow, tissue oxygenation, and perfusion. These parameters are important for evaluating the rate of limb ischemia and assessing the efficacy of various treatments. We did not employ quality-of-life assessments in our study because symptom relief is closely associated with target vessel patency. Assessing a patient’s quality of life is a complex process that is influenced by several confounding factors, making it considerably more challenging.
The inability to use a distal embolic protection device because of the reimbursement conditions of the healthcare system is also among the limitations of our study.
Finally, one important topic that we did not address in this study was the relationship between the reasons for endovascular treatment and the treatment outcomes in patients in the gray zone. This subject should ideally be addressed more comprehensively in future studies.
Conclusion
EVT is an effective treatment option for patients in the intermediate or gray zone of the PLAN color coding system, in which neither surgical bypass nor primary amputation is the preferred option. However, more randomized controlled trials are necessary.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231211768 - Supplemental material for Evaluation of endovascular treatment of chronic limb-threatening ischemia for patients in the PLAN gray zone
Supplemental material, sj-pdf-1-imr-10.1177_03000605231211768 for Evaluation of endovascular treatment of chronic limb-threatening ischemia for patients in the PLAN gray zone by Ali Baran Budak, Levent Altınay, Orhan Eren Günertem, Muhammet Sefa Sağlam, Emre Külahçıoğlu, Naim Boran Tümer, Betül Keskinkılıç Yağız, Serdar Gökay Terzioğlu, Tonguç Saba, Kanat Özışık and Serdar Günaydın in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231211768 - Supplemental material for Evaluation of endovascular treatment of chronic limb-threatening ischemia for patients in the PLAN gray zone
Supplemental material, sj-pdf-2-imr-10.1177_03000605231211768 for Evaluation of endovascular treatment of chronic limb-threatening ischemia for patients in the PLAN gray zone by Ali Baran Budak, Levent Altınay, Orhan Eren Günertem, Muhammet Sefa Sağlam, Emre Külahçıoğlu, Naim Boran Tümer, Betül Keskinkılıç Yağız, Serdar Gökay Terzioğlu, Tonguç Saba, Kanat Özışık and Serdar Günaydın in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.