
Abstract
Keywords
Introduction
Critical limb ischemia (CLI) is an arterial occlusive disease that presents with chronic ischemic rest pain, ulcers, and gangrene. If not treated appropriately, 30% of CLI cases will result in limb amputation within 1 year, with a mortality rate of up to 25%. 1 Based on the idea that CLI is defined only in terms of severe limb ischemia and does not reflect the natural prognosis of the limb, the concept of chronic limb-threatening ischemia (CLTI) was proposed. The best type of revascularization should be considered based on the patient’s background, and the risks of limb amputation, such as tissue loss, neuropathy, and infection. In addition, the anatomical findings of vascular lesions should also be considered when choosing between catheterization and bypass surgery. 1
The severity of foot lesions in CLTI can be classified using the wound, ischemia, and foot infection (WIfI) classification. Global vascular guidelines recommend bypass surgery in patients with a high WIfI stage and complex arterial lesions. 2
Rheocarna® (low-density lipoprotein cholesterol (LDL-C)/fibrinogen adsorption therapy; Kaneka Corporation, Osaka, Japan) is used for arteriosclerotic obliterans with ulcers that are unsuitable for or unresponsive to revascularization. In recent years, studies have reported the effectiveness of Rheocarna® as an adjuvant therapy to increase the peripheral blood flow after increasing the main blood flow through revascularization. 3 Although there are some case reports of patients with distal bypass obstruction who were treated with Rheocarna® and obtained good results, it is difficult to improve with Rheocarna® therapy alone. 4 Although there have been reports showing the usefulness of Rheocarna® therapy after catheterization, there have been no reports on its usefulness after distal bypass surgery.
Methods
Study design and participants
This is a retrospective observational study using medical records. In all, 10 patients who underwent Rheocarna® therapy after distal bypass surgery between June 2022 and March 2023 were included in this study. Distal bypass was defined as bypass surgery involving the three branches of the lower leg (anterior tibial, peroneal, and posterior tibial arteries). Two weeks after distal bypass surgery, Rheocarna® therapy was performed in patients with poor wound healing who were judged to be nonresponsive to distal bypass. Because all patients were on dialysis, Rheocarna® therapy was performed using an internal shunt. Rheocarna® was performed twice a week, each session lasting 2 h, for a total of five sessions. The skin perfusion pressure (SPP) and continuous walking distance on the day of admission, after distal bypass surgery, and after Rheocarna® therapy were recorded and compared.
The study protocol was approved by the Matsunami General Hospital Ethical Committee (No. 558).
Statistical analysis
Data analysis was performed using JMP 17.1.0 (SAS Institute Inc., Cary, NC, USA). Values in the table and text are expressed as mean ± standard deviation (SD). Wilcoxon’s signed rank-sum test was used to compare the two groups. Statistical significance was set at p < 0.05.
Results
Baseline characteristics
Table 1 shows the patients’ preoperative conditions. The mean age was 74.7 ± 6.83 years, and nine cases (90%) were male. All patients were undergoing dialysis, with an average of 14.5 years of dialysis history. There were six cases (60%) of diabetes mellitus and five cases (50%) of hyperlipidemia. Other results were as follows: albumin 3.24 ± 0.24 g/dL, C-reactive protein 2.47 ± 3.05 mg/dL, white blood cell count 7310 ± 3394.9/µL, hemoglobin 10.8 ± 1.85 g/dL, LDL-C 82.4 ± 37.6 mg/dL, fibrinogen 407.5 ± 113.2 mg/dL, ankle-brachial index (ABI) 0.62 ± 0.36, SPP dorsalis pedis (DP) 30.6 ± 12.0 mmHg, SPP planta pedis (PP) 40.6 ± 20.1 mmHg, and continuous walking distance 8.5 ± 9.1 m.
Patient characteristics.

ABI: ankle-brachial index; Alb: albumin; CRP: C-reactive protein; DP: dorsalis pedis; LDL-C: low-density lipoprotein cholesterol; PP: planta pedis; SPP: skin perfusion pressure; WIFI: wound, ischemia, and foot infection.
The central anastomosis of the distal bypass in all cases was the popliteal artery. The peripheral anastomosis was the anterior tibial artery in five cases, the peroneal artery in three cases, and the posterior tibial artery in two cases. Minor toe amputation was performed in five cases, forefoot amputation in two cases, and metatarsal amputation in two cases.
Measurements after surgery and Rheocarna® therapy
Two weeks after distal bypass surgery, the following measurements were recorded: LDL-C 64.6 ± 22.0 mg/dL, fibrinogen 486.4 ± 139.4 mg/dL, ABI 0.98 ± 0.20, SPP DP 46.7 ± 24.8 mmHg, SPP PP 51.7 ± 18.7 mmHg, and continuous walking distance 28.4 ± 30.1 m. The distal bypass was patent in all cases. After distal bypass surgery, aspirin and clopidogrel combination therapy was administered.
After five sessions of Rheocarna® therapy, the following measurements were recorded: LDL-C 46.4 ± 16.0 mg/dL, fibrinogen 297.2 ± 115.6 mg/dL, ABI 0.936 ± 0.16, SPP DP 71.5 ± 27.0 mmHg, SPP PP 65.0 ± 26.3 mmHg, and continuous walking distance 78.5 ± 102.7 m.
LDL-C was 82.4 ± 37.6 mg/dL preoperatively and LDL-C 46.4 ± 16.0 mg/dL after five sessions of Rheocarna® therapy, showing a significant decrease from preoperative value (p = 0.0039). Fibrinogen was 407.5 ± 113.2 mg/dL preoperatively, 486.4 ± 139.4 mg/dL after distal bypass surgery, and 297.2 ± 115.6 mg/dL after five sessions of Rheocarna® therapy, showing a significant decrease after distal bypass surgery (p = 0.0059). ABI was 0.62 ± 0.36 preoperatively and 0.98 ± 0.20 after surgery, showing a significant increase (p = 0.0078). ABI was 0.936 ± 0.16 after five sessions of Rheocarna® therapy and showed no change after distal bypass. SPP DP was 30.6 ± 12.0 mmHg preoperatively and 46.7 ± 24.8 mmHg postoperatively, showing significant improvement (p = 0.0176), and 71.5 ± 27.0 mmHg after Rheocarna®, showing marked improvement from preoperative value (p = 0.0020) (Figure 1).
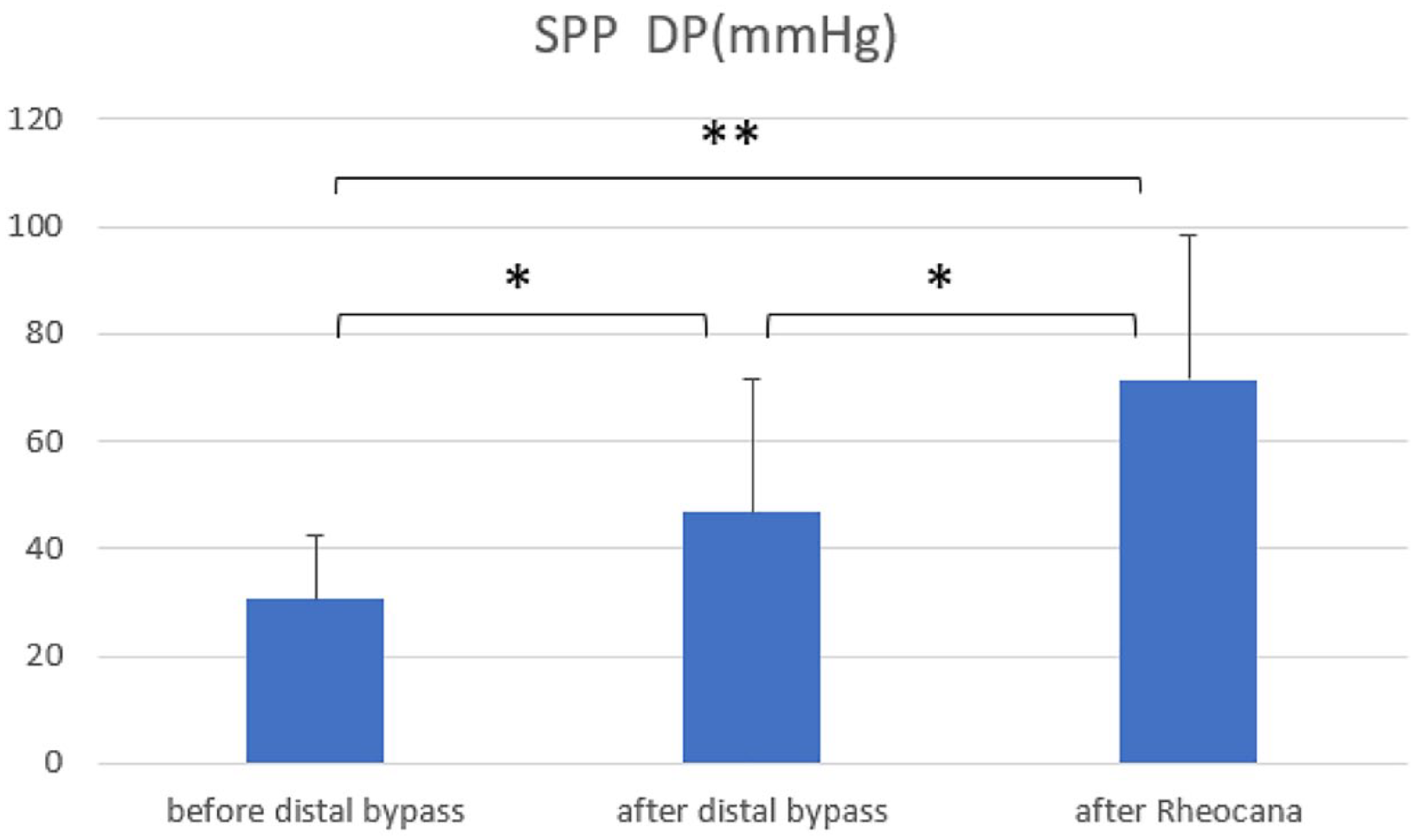
Mean pressures and SDs of SPP of DP at each observation time point.
SPP PP improved from 40.6 ± 20.1 mmHg preoperatively to 51.7 ± 18.7 mmHg postoperatively, but no significant difference was observed (p = 0.2402). However, after five sessions of Rheocarna® therapy, SPP PP was 65.0 ± 26.3 mmHg, which was a significant improvement from the preoperative value (p = 0.0293) (Figure 2).

Mean pressures and SDs of SPP of PP at each observation time point.
The continuous walking distance improved from 8.5 ± 9.1 m before distal bypass surgery to 28.4 ± 30.1 m after distal bypass surgery, but no significant difference was found (p = 0.625). However, after five sessions of Rheocarna® therapy, the continuous walking distance was 78.5 ± 102.7 m, which was a significant improvement from the preoperative level (p = 0.0039) (Figure 3).
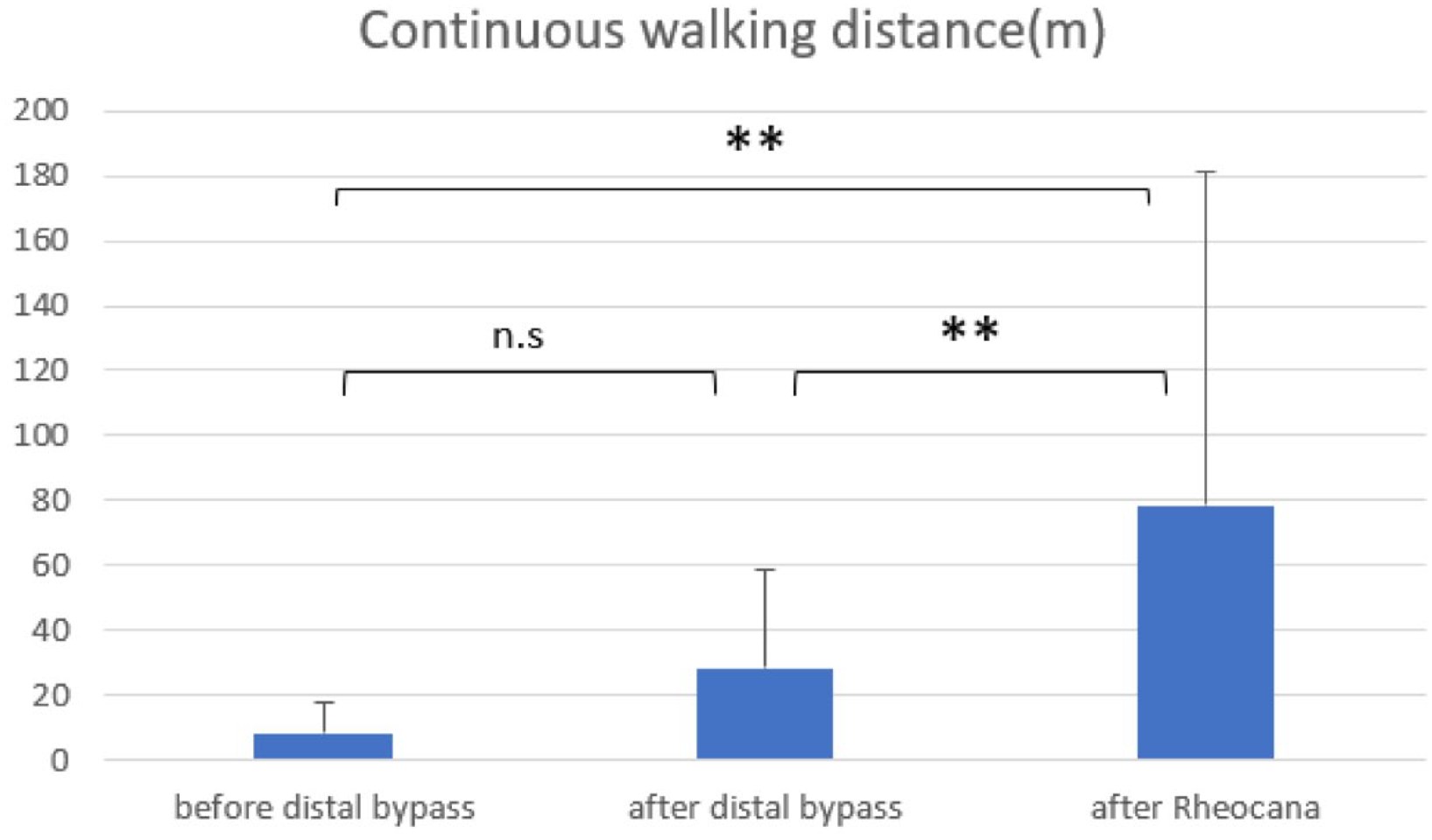
Mean pressures and SDs of continuous walking distance at each observation time point.
Discussion
CLTI is a condition caused by arteriosclerosis wherein the lower limbs become ischemic, thus having a risk of amputation. Revascularization is required to avoid amputation of the lower limbs. The size and depth of the wound, degree of ischemia, and complications of infection vary among individual cases, and appropriate treatment is given based on the severity. For CLTI, the evaluation of foot lesions using the WIfI grading is recommended.2,5 In the WIfI stage 2, revascularization is required to salvage the lower extremity. Global vascular guidelines recommend bypass surgery if the WIfI stage is high and arterial lesions are complicated.
ABI is generally used to evaluate ischemia of the lower limbs; however, it measures blood pressure at the ankle joint level and does not represent blood flow in the peripheral foot. On the other hand, SPP can measure blood flow near the wound and is useful not only for distinguishing between ischemic and non-ischemic conditions but also for predicting healing after revascularization. 6
Increased inflammatory indicators, such as CRP and procalcitonin, are important indices of infection. However, in diabetic patients, these are often not observed due to a decreased immune response. 7 Moreover, if ischemia is severe, obvious inflammatory findings may also not be observed, even if the infection is severe.
CLTI requires revascularization; however, it is important to assess whether surgery, endovascular therapy (EVT), or both are required. In addition to the minimal invasiveness of EVT, reports from the BASIL study indicate that the outcomes of EVT were similar to those of bypass surgery. However, many patients have lesions below the three branches of the lower leg and extensive tissue defects. 8 Therefore, distal bypass, which is capable of transporting large amounts of blood and potentially restoring patency for a long period, is the first choice in cases where autologous veins can be used.
EVT emphasizes the angiosome concept, wherein the blood flow increases to the dominant region.9,10 However, in distal bypass, blood flow is high, and tissue repair proceeds without direct blood flow to the ischemic site. 11 In this case, the SPP DP was significantly higher than the SPP PP. This is probably because 50% of the patients were bypassed to the anterior tibial artery, and the SPP on the dorsum of the foot was more markedly elevated.
Recently, a new LDL apheresis device (Rheocarna®; Kaneka Corporation, Osaka, Japan) has been approved for CLTI with refractory ulcers. Rheocarna® is a blood purification therapy that selectively removes the causative agents of CLTI, such as LDL-C and fibrinogen, using porous cellulose beads containing negatively charged dextran sulfate and hydrophobic tryptophan. Rheocana® can improve blood and plasma viscosity with respect to shear rate and reduce fibrinogen levels. Decreased fibrinogen levels lead to improved endothelial function and microcirculation.12,13
For LDL-adsorption-only liposorbers before Rheocarna®, the addition of liposorbers has been reported to improve re-EVT/major amputation rates compared to EVT alone. 14 In a trial conducted on Rheocana®, a maximum of 24 sessions of Rheocarna® therapy was performed on 61 cases of CLTI patients with ulcers judged to be unresponsive to revascularization. Within 24 weeks of the initial treatment, 45.9% of patients were reported to have healed ulcers. 3
In our study, wound healing was observed in all cases, and significant increases in SPP were noted. Fibrinogen levels increased postoperatively due to surgical stress but significantly decreased after Rheocana® therapy. In the current study, bypass patency was observed in all patients, and it is possible that the decrease in fibrinogen levels reduced blood viscosity and had a dominant effect on bypass patency.
A significant improvement in continuous walking distance was observed, and all patients were discharged from the hospital ambulatory. This suggests that the addition of Rheocarna® therapy may result in faster wound healing than revascularization alone.
Study limitations
As a limitation, sample size calculation (power analysis) was not performed in this study. The 10 cases included in this study are more suitable for a case series, so the statistically obtained results may not be valid.
In addition, 2 weeks after the distal bypass operation, it was judged that the wound healing was poor, and Rheocarna® therapy was performed for about 3 weeks. We cannot rule out the possibility that the improvement in SPP and continuous walking distance reflects the natural course after distal bypass surgery.
Conclusion
In CLTI patients, SPP and continuous walking distance were significantly improved by performing Rheocarna® therapy after distal bypass surgery. Thus, Rheocarna® therapy after distal bypass surgery may improve wound healing and activities of daily living by increasing blood flow.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Matsunami General Hospital Ethical Committee (No. 558).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.