
Abstract
Advanced glycation end products (AGEs) are independently related to cardiovascular disease (CVD) and favor cholesterol and oxysterol accumulation in macrophage foam cells. Soluble RAGE (sRAGE) impairs cellular AGE signaling alleviating the deleterious effects of AGE in atherogenesis. The association between plasma AGEs and sRAGE with the content of cholesterol, markers of cholesterol synthesis and absorption, and oxysterols in atherosclerotic plaques was evaluated in subjects undergoing carotid endarterectomy.
Plasma and carotid plaques were obtained from symptomatic (n = 23) and asymptomatic subjects (n = 40). Lipids from plaques were extracted and sterols (oxysterols, cholesterol, desmosterol, lathosterol, sitosterol, and campesterol) were determined by using gas chromatography/mass spectrometry. Plasma total AGEs and pentosidine were measured by using fluorimetry and sRAGE by using ELISA.
In symptomatic subjects´ atherosclerotic plaques, an increased amount of cholesterol (3x) and oxysterols [7 α-hydroxycholesterol (1.4x); 7 β−hydroxycholesterol (1.2x); 25-hydroxycholesterol (1.3x); 24-hydroxycholesterol (2.7x), and 27-hydroxycholesterol, (1.15x)], with exception to 7 ketocholesterol, were found in comparison to asymptomatic individuals. Plasma total AGEs and pentosidine significantly and positively correlated to sterols accumulated in the atherosclerotic lesion, including cholesterol, desmosterol, campesterol, sitosterol, and oxysterols. On the other hand, sRAGE inversely correlated to total AGEs and pentosidine in plasma, and with major species of oxysterols, cholesterol, and markers of cholesterol synthesis and absorption in the atherosclerotic lesion. In multiple regression analyses, it was observed a significant inverse correlation between sRAGE and 24-hydroxycholesterol and desmosterol, and a positive significant correlation between pentosidine and 24-hydroxycholesterol, 27-hydroxycholesterol, and campesterol.
In conclusion, the plasma concentration of AGEs and sRAGE is a tool to predict the accumulation of sterols in atherosclerotic lesions in symptomatic and asymptomatic individuals, helping to prevent and improve the management of acute cardiovascular complications.
Introduction
Cardiovascular disease (CVD), clinically manifested by acute myocardial infarction and stroke, is the leading cause of mortality worldwide, with atherosclerosis as the underlying mechanism.1,2 Risk factors such as dyslipidemia, hypertension, cigarette smoking, and diabetes mellitus (DM) contribute to sterols accumulation in monocyte-derived macrophages in the arterial wall and to inflammation that accompanies atherogenesis.3,4
Advanced glycation end products (AGEs) prevalent in DM, chronic kidney disease, inflammation, obesity, and dyslipidemia are independently related to CVD in different populations.5–7 Advanced glycation end products are formed by the non-enzymatic reaction between glucose or oxoaldehydes with the amino-terminal portion of lysine and arginine in the polypeptide chain, phospholipids, and nucleic acids. 8 Heterogeneous AGEs can be formed including carboxymethyllysine, carboxyethyllysine, pentosidine, pyrraline, glyoxal and methylglyoxal dimers, and others. Advanced glycation end products alter the structure and function of macromolecules, and their interaction with the receptor for AGEs (RAGE) triggers the generation of reactive oxygen species by the NADPH oxidase system and mitochondria leading to the activation of the NFKB pathway that favors the transactivation of inflammatory and apoptotic genes. 9
By interacting with RAGE, AGEs impair cholesterol efflux mediated by ATP binding cassette (ABC) transporters A1 (ABCA-1) and G1 (ABCG-1), which is related to the induction of oxidative and endoplasmic reticulum stress, and the accumulation of toxic oxysterols in macrophages.10–17
Oxysterols are derivatives of enzymatic and non-enzymatic cholesterol oxidation and their levels in cells are directly related to cholesterol accumulation. They are very active compounds involved in cellular lipid homeostasis by controlling cholesterol synthesis, secretion, and the expression of lipoprotein receptors via sterol regulatory element-binding proteins (SREBPs) and liver X receptor (LXR). Besides, the exportation of 27-hydroxycholesterol from cells to high-density lipoproteins (HDL) by passive diffusion or by an ABCG-1 dependent mechanism contributes as an additional route of the reverse cholesterol transport pathway. 18
On the other hand, oxysterols may elicit cell inflammation, pyroptosis, and apoptosis that induce plaque instability and rupture. Particularly, in foam cells the oxysterol: cholesterol ratio is much higher than in normal tissues or plasma. 19 The amount of 7-ketocholesterol was found as increased in the fibrous cap of thin atheroma in comparison to thick-cap areas. This was observed together with an elevated expression of markers of endoplasmic reticulum stress and apoptotic cells in thin atheroma. 20 Nonetheless, the mechanisms that dictate the formation of different oxysterol species are not well known since there is also the contribution of exogenous oxysterols that are transported to the arterial wall mainly by the low-density lipoproteins (LDL) and distinctively modulate atherosclerotic plaque evolution.
Soluble RAGE (sRAGE) is a C-terminally truncated soluble isoform of RAGE found in circulation and extracellular fluids that can be generated by alternative splicing or by the action of matrix metalloproteinases and A-disintegrin and metalloprotease ADAM-10 on plasma membrane RAGE. 21 Soluble RAGE is able to bind AGEs without intracellular signaling, being considered as a decoy receptor and its plasma levels have been inversely related to AGE-elicited long-term complications in DM by mitigating the deleterious effects of the activation of the full-length RAGE. 22
In an attempt to search for surrogate markers for sterol accumulation in arteries that may help to prevent and manage acute vascular events, we evaluated in symptomatic and asymptomatic subjects undergoing carotid endarterectomy the association between plasma AGEs and their contra regulator, sRAGE, with the content of total cholesterol, markers of cholesterol synthesis and absorption, and oxysterols in atherosclerotic lesions.
Materials and methods
Patients and ethical statement
Plasma and carotid plaque samples were collected from 63 individuals undergoing carotid endarterectomy at the Vascular and Endovascular Surgery Department from Hospital das Clinicas (HCFMUSP) da Faculdade de Medicina da Universidade de Sao Paulo. All participants were properly informed about the procedures and the study, and signed an informed written consent form that was previously approved by The Ethical Committee for Human Research Protocols of the Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo, HCFMUSP (#06359018.8.0000.0068), in accordance with the Declaration of Helsinki.
Eligible subjects who underwent carotid endarterectomy were classified as asymptomatic when had unilateral or bilateral carotid artery stenosis that was considered to be severe (carotid artery diameter reduction of at least 60% on ultrasound) although this stenosis had not caused any stroke, transient cerebral ischemia, or other relevant neurological symptoms in the past 6 months. Symptomatic stenosis was considered the cause of neurological symptoms in the last 6 months, following the North American Symptomatic Carotid Endarterectomy (NASCET) 23 and the Asymptomatic Carotid Atherosclerosis Study (ACAS) 24 criteria.
Measurement of carotid plaque cholesterol, markers of cholesterol synthesis and absorption, and oxysterols by using gas chromatography-mass spectrometry (CG/MS)
Lipids were extracted from 0.5 mL of plasma or from the carotid plaque samples with 6 mL chloroform/methanol (2:1; v: v) and 2 mL water containing butylated hydroxytoluene (BHT; 5 μg/mL). The homogenized content was then centrifuged at 1690 × g for 15 min, 4°C; the aqueous phase was removed and utilized for protein measurements and the lipids in the organic phase were extracted after the addition of 3 mL chloroform/methanol (2:1; v: v) and vacuum-evaporated (Genevac EZ-2 Plus, Ipswich, England). A mixture of deuterium-labeled internal standard (7α-hydroxycholesterol-d7, 7β-hydroxycholesterol-d7, 7-ketocholesterol-d7, 25-hydroxycholesterol-d7, 27-hydroxycholesterol-d7, and cholesterol-d7), 100 ng of each oxysterol, 20 μg of cholesterol, diluted in ethanol; (Avanti Polar Lipids, Alabaster, USA) was added to lipid extract. Samples were saponified by adding 10 mL 0.4M potassium hydroxide in ethanol for 2 h at room temperature. The pH was adjusted by adding 100 μL phosphoric acid. The organic phase was isolated after the addition of 20 mL chloroform and 6 mL saline following vigorous shaking and centrifugation (1690 × g for 15 min, 4°C). The aqueous phase was discarded and the organic phase vacuum-evaporated (Gene-vac EZ-2 Plus, Ipswich, England) and suspended in 1 mL toluene.
Total cholesterol and its markers of synthesis and absorption were separated from oxysterols for solid-phase extraction (Supelclean LC-Si SPE Tube). The column was washed with 1 mL of hexane; cholesterol and its markers of synthesis and absorption were eluted by 8 mL of 1.5% of isopropanol in hexane. Oxysterols were eluted in 5 mL 30% of isopropanol in hexane. All samples were dried (Genevac EZ-2 Plus, Ipswich, England), derivatized (100 μL pyridine and 100 μL BSTFA + 1% TMCS, 1h at 60°C), and injected in gas chromatography-mass spectrometry (CG/MS; Shimadzu GCMS-QP2010) equipment provided with Restek capillary column 30 m X 0.25 mm, using helium as the carrier gas, and had a constant linear velocity of 45.8 cm/s with an oven temperature maintained at 260°C. Ions were monitored by a single ion monitoring method and quantification was performed by the comparison of the sample spikes with a standard curve. The amount of all sterols was corrected per milligram of plaque protein or mL of plasma. Oxysterols and cholesterol (total cholesterol and cholesterol precursors) were detected with a limit of quantification of 15 ng and 5 μg in the total sample, respectively. Based on repetitive measurements of sterols in a control plasma sample, the intra-assay coefficient of variation was 19 and 6%, respectively, for oxysterols and cholesterol similar to previously described by Ferreira et al. (2017). 25
Biochemical analysis
A sample of venous blood was collected from subjects immediately before surgical procedures and plasma was isolated in a refrigerated centrifuge (4°C) for 15 min, at 1500 r/min. Plasma samples were aliquoted, stored, and frozen at −80°C until analysis. Circulating concentrations of glucose, total cholesterol, triglycerides, and HDLc were determined using commercial kits, according to the manufacturer’s instructions (Labtest, Minas Gerais, Brazil). Glycated hemoglobin (HbA1c) was determined in total blood by using high-performance liquid chromatography. The contents of plasma total AGE and pentosidine were determined by fluorescence measurement (Synergy HT Multi-Mode Microplate Reader, SpectraMax M5). Samples were excited at a wavelength of 370 nm and the fluorescence emitted at 440 nm and 378 nm, respectively, for total AGE and pentosidine. The levels of sRAGE were determined by using enzyme-linked immunosorbent assay (ELISA, R&D System, Minneapolis, Minnesota, USA).
Statistical analysis
Statistical analyses were performed using SPSS 21.0 IBM® and the GraphPad Prism 5 program (GraphPad Software, Inc. 2007). Continuous variables were tested for normality with the Kolmogorov–Smirnov and Shapiro–Wilk tests. The values are expressed as median and percentiles 25 and 75 for non-parametric data. The categorical data are presented as absolute values and percentages and were tested using Pearson χ2 test and Fisher exact test, if applicable. Non-parametric data were compared using the Mann–Whitney U test with a Bonferroni correction for two independent samples. The association between continuous variables was performed by using Spearman Correlation and the good performance or linearity was determined by “r” square value ≥ 0.8. Multiple Linear Regression adjusted for clinical factors and expressed by “B” coefficient and confidences intervals performed the predictive model for a continuous variable. The value of p < .05 was considered statistically significant and graphic correlations were performed by non-Linear regression.
Results
Baseline clinical characteristics of asymptomatic and symptomatic subjects
Baseline clinical characteristics of asymptomatic and symptomatic subjects who underwent carotid endarterectomy.
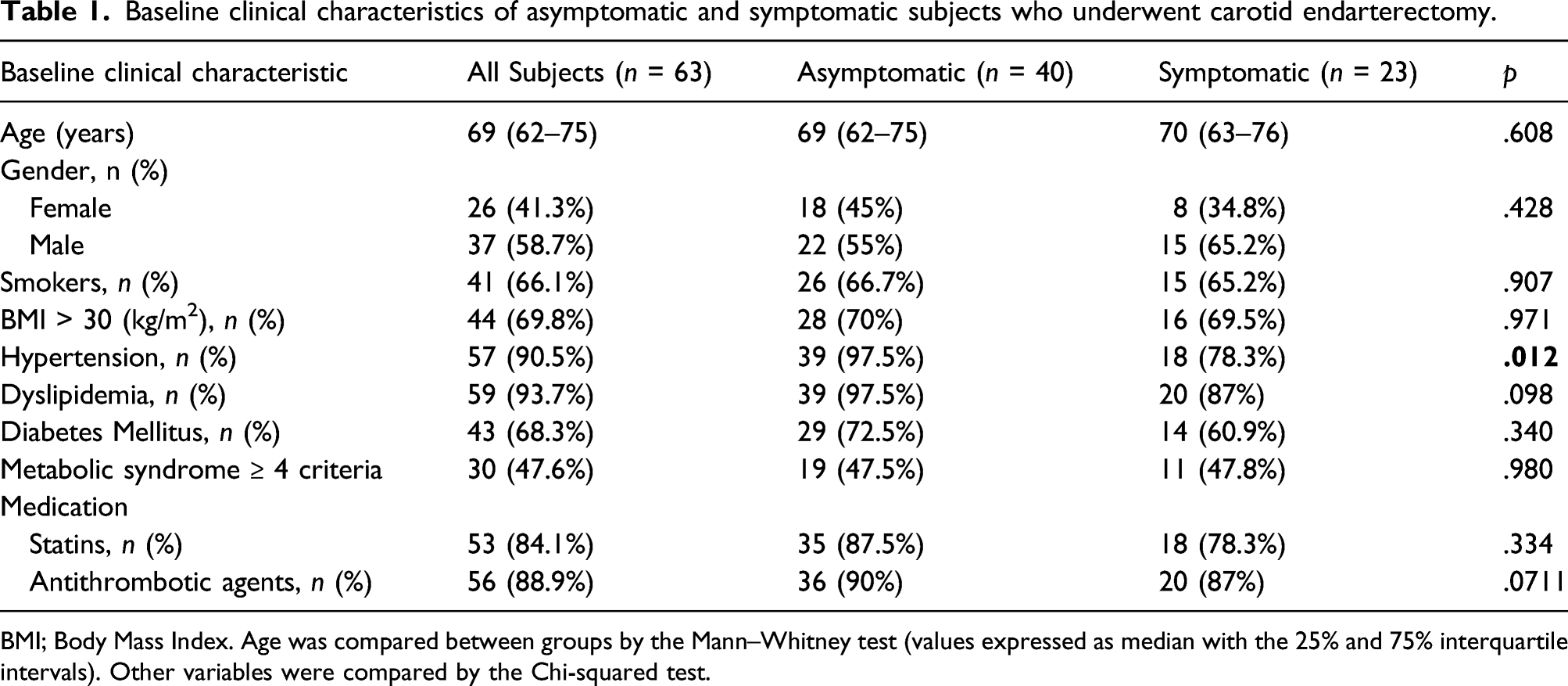
BMI; Body Mass Index. Age was compared between groups by the Mann–Whitney test (values expressed as median with the 25% and 75% interquartile intervals). Other variables were compared by the Chi-squared test.
Plasma lipids, AGEs, and sRAGE in asymptomatic and symptomatic subjects
Plasma biochemical parameters of asymptomatic and symptomatic subjects who underwent carotid endarterectomy.
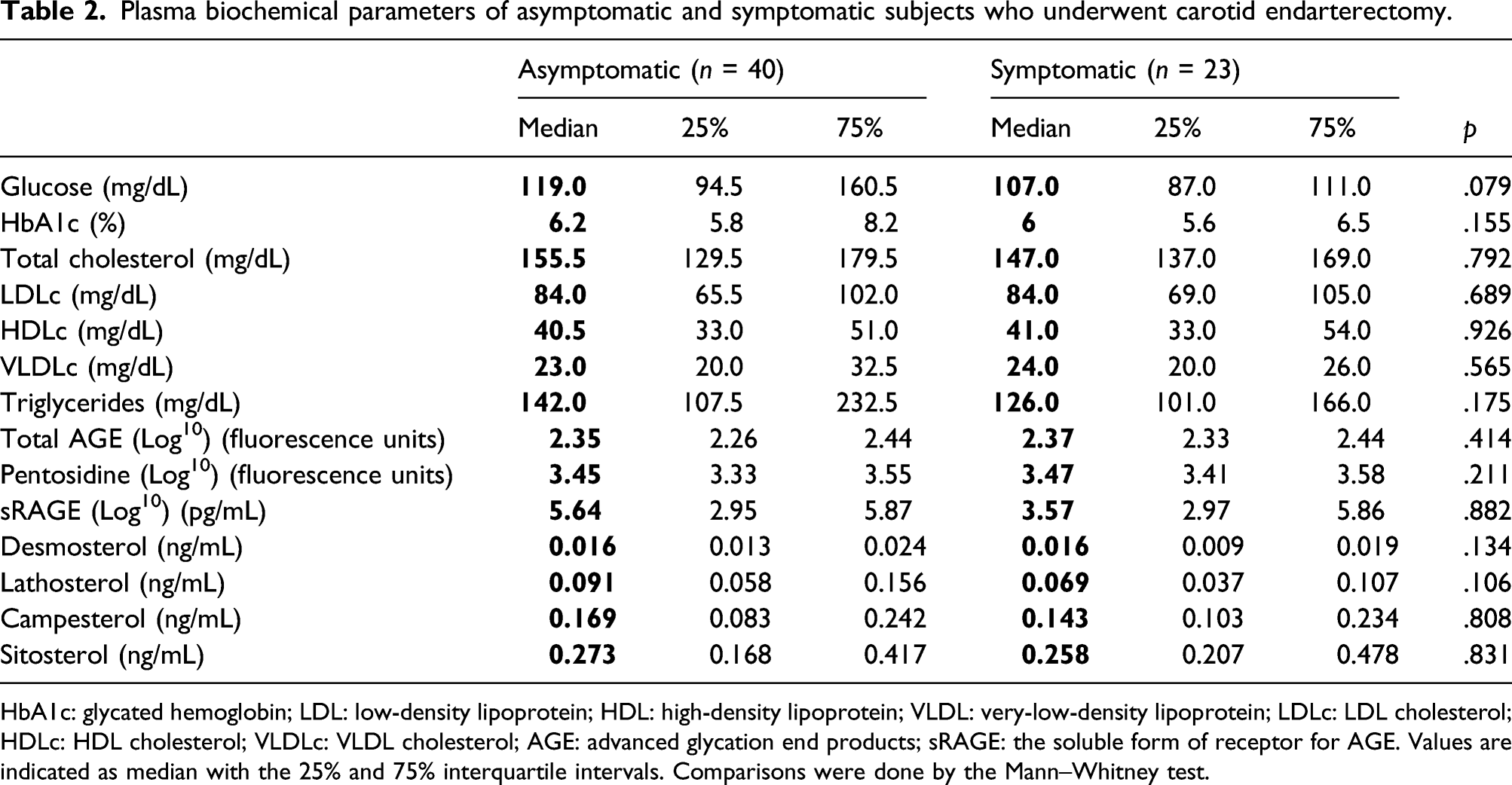
HbA1c: glycated hemoglobin; LDL: low-density lipoprotein; HDL: high-density lipoprotein; VLDL: very-low-density lipoprotein; LDLc: LDL cholesterol; HDLc: HDL cholesterol; VLDLc: VLDL cholesterol; AGE: advanced glycation end products; sRAGE: the soluble form of receptor for AGE. Values are indicated as median with the 25% and 75% interquartile intervals. Comparisons were done by the Mann–Whitney test.
Similar values of glycated hemoglobin (HbA1c), plasma glucose, total AGEs, pentosidine, and sRAGE were observed in both groups. A negative correlation between total AGEs and pentosidine with sRAGE in plasma was observed (
Sterol content in carotid atherosclerotic plaques
Sterols content in carotid atherosclerotic plaque of asymptomatic and symptomatic subjects who underwent carotid endarterectomy.
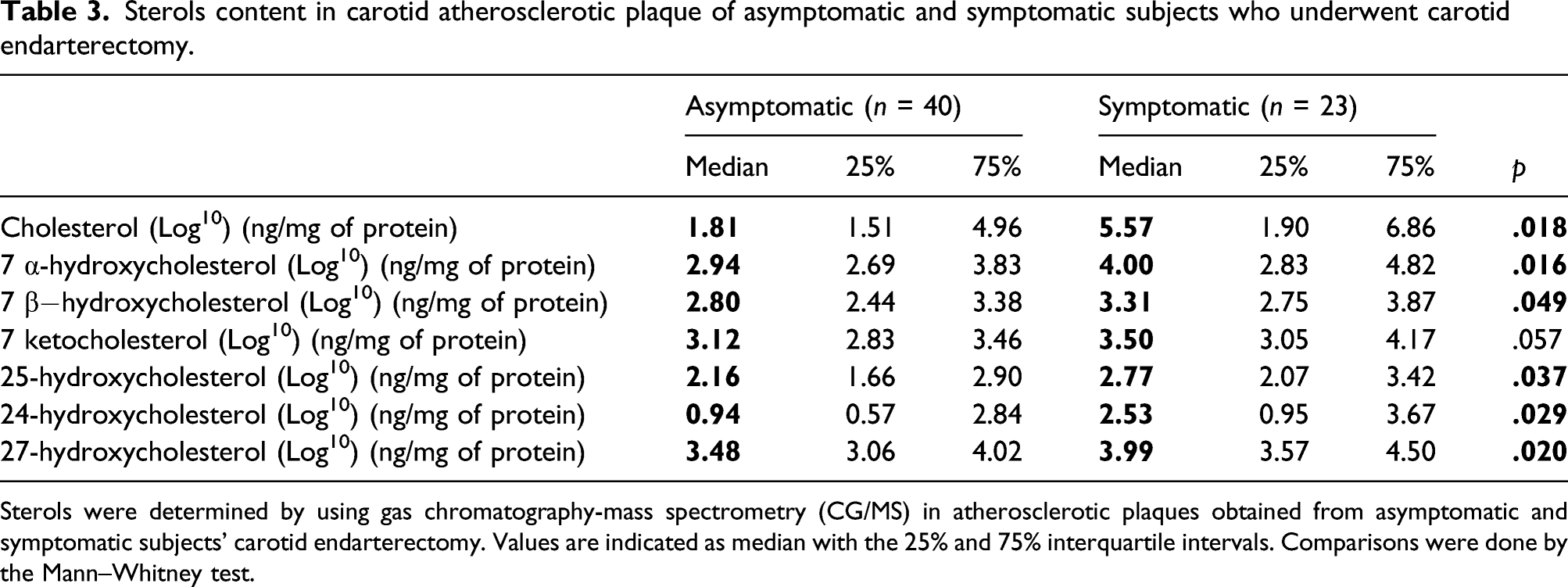
Sterols were determined by using gas chromatography-mass spectrometry (CG/MS) in atherosclerotic plaques obtained from asymptomatic and symptomatic subjects’ carotid endarterectomy. Values are indicated as median with the 25% and 75% interquartile intervals. Comparisons were done by the Mann–Whitney test.
Association of plasma AGEs and sRAGE with accumulated sterols in atherosclerotic lesions
Association of plasma AGEs and sRAGE with accumulated sterols in carotid atherosclerotic plaques of subjects who underwent carotid endarterectomy.
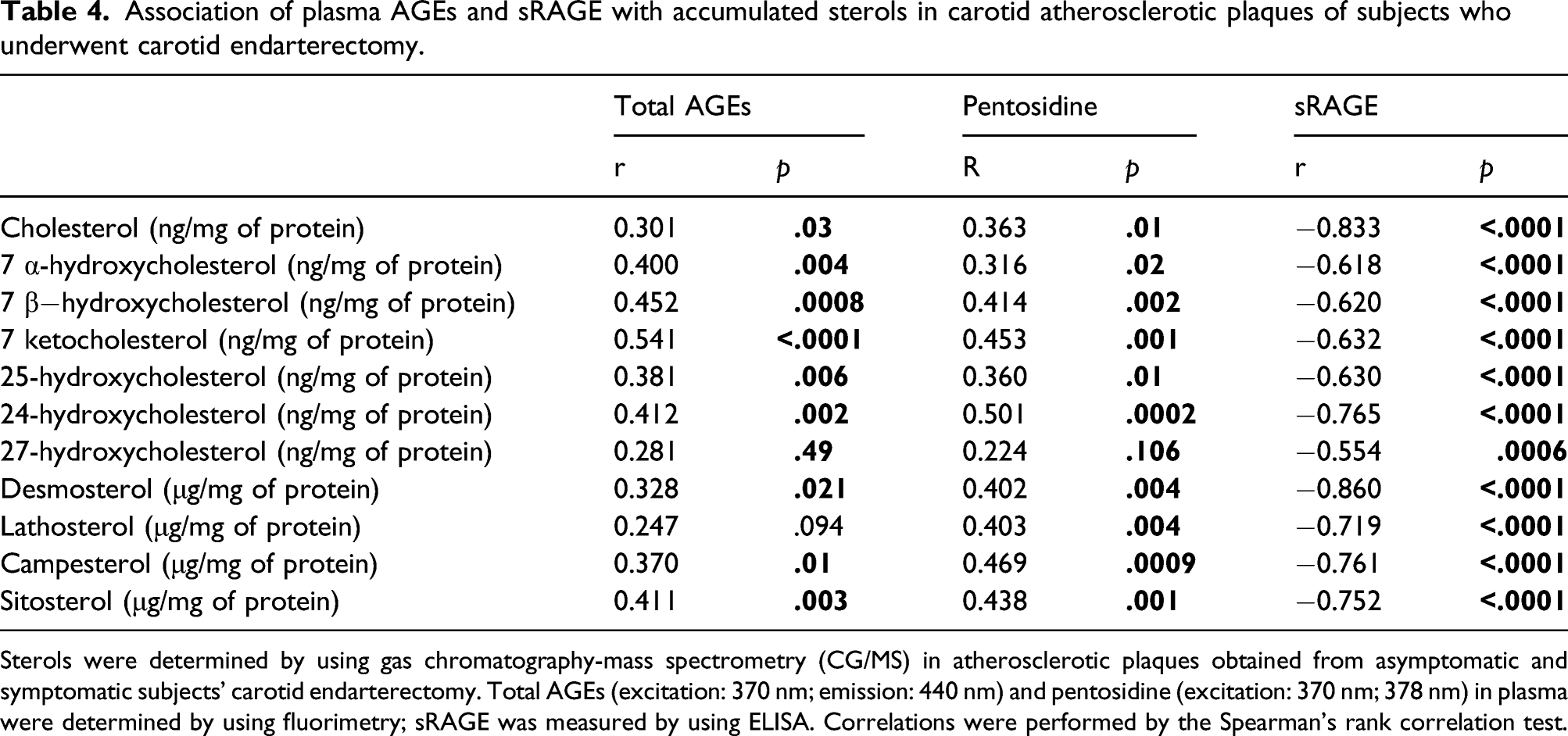
Sterols were determined by using gas chromatography-mass spectrometry (CG/MS) in atherosclerotic plaques obtained from asymptomatic and symptomatic subjects’ carotid endarterectomy. Total AGEs (excitation: 370 nm; emission: 440 nm) and pentosidine (excitation: 370 nm; 378 nm) in plasma were determined by using fluorimetry; sRAGE was measured by using ELISA. Correlations were performed by the Spearman’s rank correlation test.
Multiple linear regression for pentosidine and sRAGE as predictive factors
Multiple linear regression for pentosidine and sRAGE as predictive factors.
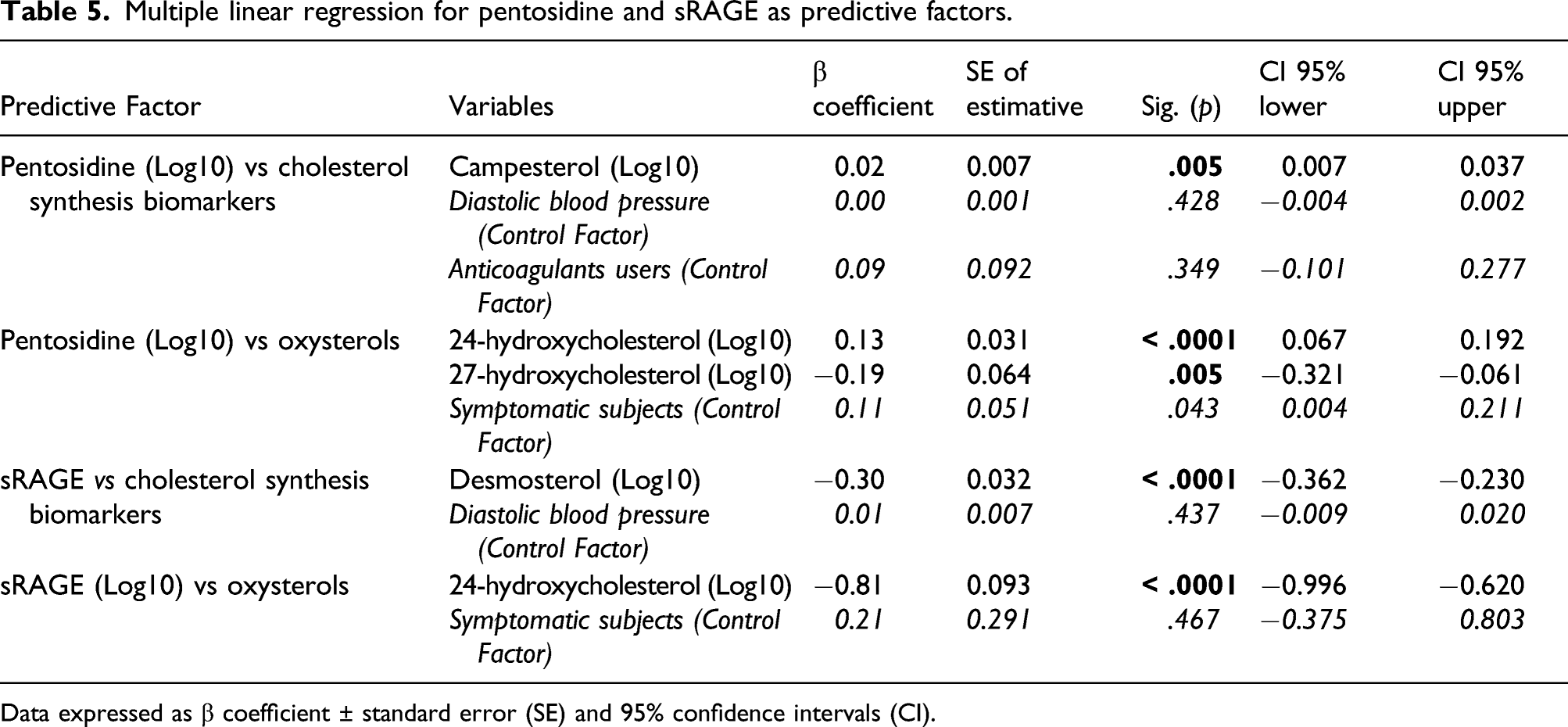
Data expressed as β coefficient ± standard error (SE) and 95% confidence intervals (CI).
Discussion
The present investigation demonstrated that total cholesterol, markers of cholesterol synthesis and absorption, and oxysterols accumulated in carotid advanced atherosclerotic lesions: (1) are greater in symptomatic as compared to asymptomatic subjects; (2) positively correlate with total AGEs and pentosidine in plasma, and (3) negatively correlate with plasma sRAGE that counteracts the deleterious signaling of AGEs in cells.
Advanced glycation end products contribute to atherogenesis being an important component of many clinical and pathophysiological features related to plaque vulnerability. 26 Considering the high heterogeneity of AGEs, measurement of different structures formed in advanced glycation is still a challenge, and mass spectroscopy as a golden standard implies high-cost analysis and high labor demand. In this context, the ability of some AGEs to emit fluorescence (excitation 370 nm) has been utilized as a basis for a simple and reliable method of determining total AGEs (440 nm) and pentosidine (378 nm) in plasma.
In this investigation, circulating AGEs were positively correlated with total cholesterol, markers of cholesterol absorption and synthesis, and major species of oxysterols. In plasma, oxysterol concentration is elevated in hypercholesterolemia, DM, and smoking, and is increased by exogenous dietary sources, which aggregate an unpredictable source of these sterols that together with the high inter-individual variability of oxysterol measurement makes it difficult to associate circulating levels of oxysterols with those in the arterial wall. In agreement with what was observed in the present analysis, Ceglarek et al. 27 did not find an association between oxysterols in plasma and atherosclerotic plaques. On the other hand, those authors demonstrated that plasma levels of plant sterols, cholesterol, and markers of cholesterol synthesis were related to symptomatic advanced carotid lesions. Plant sterols are able to diminish cholesterol absorption in the intestine although their increased concentration in plasma has been related to an increased risk of atherosclerosis, similarly to cholesterol. 28
Plasma cholesterol levels were not predictive for their corresponding levels in atherosclerotic lesions, which has also been reported by others. 27 Interestingly, cholesterol and oxysterol levels (except 7-ketocholesterol; p = .057) were greater in carotid lesions from symptomatic subjects as compared to asymptomatic, although the profile of subspecies distribution was similar between these groups.
Experimental therapies based on RAGE blocking or silencing are able to attenuate cholesterol accumulation in cultivated macrophages or in experimental models of atherosclerosis.29,30 In this regard, sRAGE appears as a natural defense avoiding deleterious effects of the AGE-RAGE axis activation. In the present investigation, sRAGE, as expected, inversely related to total AGEs and pentosidine in plasma. More importantly, sRAGE negatively correlated with oxysterols, cholesterol, desmosterol, lathosterol, and plant sterols in carotid atherosclerotic lesions. In an analysis of 1201 samples from the Atherosclerosis Risk in Communities Study (ARIC), it was found that low levels of sRAGE were associated with risk of DM, coronary heart disease, and mortality. 31 Other studies have demonstrated an association between sRAGE and the development and progression of atherosclerosis and carotid plaque calcification,32–34 and sRAGE was demonstrated higher in symptomatic subjects. 35
In acute coronary syndrome (ACS), Larsen et al. 33 found a positive association between sRAGE with major adverse cardiovascular end-points; but after 6 weeks, subjects with higher sRAGE as compared to baseline were more protected against recurrent ACS. These results point to a distinct role of sRAGE during ACS being a marker of a systemic inflammatory status as reported by others33,36,37; while in the recovery phase, it may improve the subject’s prognosis based on its ability in scavenging AGEs and other ligands of RAGE limiting plaque destabilization. Subgroups of subjects presenting four or more components of the metabolic syndrome or BMI > 30 kg/m2 had higher levels of total AGEs and pentosidine and lower levels of sRAGE. This was accompanied by increased concentrations of total cholesterol and oxysterols in carotid atherosclerotic plaques (data not show). Together, these results reassure metabolic syndrome and obesity as risk factors for carotid plaque instability, as previously described by Rosella et al. 38
Limitations of this study include the fact that AGEs were not determined in lesions, although higher content of AGEs in carotid atherosclerotic plaques has been consistently demonstrated, particularly in association with the phenotypic profile of rupture propensity. For instance, 5-hydro-5-methylimidazolone (MG-H1) and carboxymethyllysine were associated with interleukin-8 (IL-8), monocyte chemoattractant protein 1 (MCP-1), and matrix metalloproteinase 9 (MMP9) in areas susceptible to rupture. In addition, AGEs were co-localized with caspase 3 in macrophages surrounding the necrotic core. 39 A small number of subjects included may have limited the power of associations observed and could have contributed to the lack of correlation when symptomatic or asymptomatic subjects were analyzed separately. It is worth considering that endarterectomy obtained samples are very advanced atherosclerotic lesions limiting the interpretation of circulating AGEs and sRAGE as surrogate markers of atherogenesis. In this sense, new studies should be conducted on arteries in different stages and histological grades of atherosclerosis.
In conclusion, circulating AGEs and especially sRAGE are predictive of sterols accumulation in carotid plaques. Considering the direct involvement of AGEs in the phenotype of rupture-prone lesions, their determination in plasma may help predict atherosclerotic plaque evolution and instability and optimize the management and prevention of acute macrovascular complications.
Footnotes
Acknowledgments
The authors would like to thank Fundação Faculdade de Medicina and Laboratórios de Investigação Médica (LIM) do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo.
Author contributions
RSP: performed all experiments and wrote the manuscript; GSF: helped in with GC/MS analysis; MFMS: helped in experimental procedures; GCRS: helped in the preparation of carotid plaques and collected clinical data; VSN: helped in GC/MS data interpretation; LL: helped in experimental procedures; PRP: helped in experimental procedures; SISA: helped in experimental procedures; UFM: helped in data interpretation; ERS: selected subjects, supervised endarterectomy, and helped in data interpretation; MP: conceived the study and experiments and wrote the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank the financial support from Fundação de Amparo à Pesquisa do Estado de São Paulo, FAPESP (grants #2018/00172-0 to RSP, 2018/18545-4 to MMS, 2015/21072-5 to MP and 2016/15603-0 to MP and UFM, and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. MP and UFM are recipients of a research award from Conselho Nacional de Desenvolvimento Científico e Tecnológico, CNPq, Brazil.