
Abstract
Type 2 diabetes mellitus is a pathology of heterogeneous etiology characterized by hyperglycemia resulting from lack of insulin action, insulin secretion, or both, and the population with diabetes mellitus is predicted to be about 439 million worldwide by 2030. Prolong diabetes has been related with microvascular complications especially diabetic nephropathy. DN is the most common complication of type 2 diabetes mellitus, and it is the leading cause of end-stage renal disease worldwide. It is crucial to diagnose patients who are more sensible to develop DN for better control of the process of disease. Several factors and mechanisms contribute to the development and outcome of diabetic nephropathy. Microalbuminuria is an early marker of DN and use it as a routine for screening, but the renal damages may be happening even without microalbuminuria. There are several significant kidney damage and disease biomarkers which helps in early detection of DN. An early biomarker may allow earlier diagnosis, treatment reduces DN prevalence and slows DN progression. Therefore, this review focuses on laboratory biomarkers that are earlier, more validation of an early and specific biomarker could potentially make it possible for early diagnosis, treatment, and retardation of progression of diabetic nephropathy.
Keywords
Introduction
Type 2 diabetes mellitus is a pathology of heterogeneous etiology characterized by hyperglycemia resulting from defects of insulin action, insulin secretion, or both, 1 and the population with diabetes mellitus is predicted to be about 439 million worldwide by 2030. 2 Chronic diabetes is relative with damage, dysfunction, and failure of several organs, especially the eyes, nerves, foot, blood vessels, kidneys, and heart . 3 Prolong diabetes has been related with microvascular complications such as retinopathy, neuropathy, and nephropathy. 4
The microvascular complications of diabetes induce to renal damage known as diabetic nephropathy (DN), the most common complication of type 2 diabetes mellitus, 5 and it is the leading cause of end-stage renal disease worldwide, which is associated with high morbidity and mortality. 6 It develops in approximately 40% of patients with diabetes, 7 after 10 years of type 2 diabetes mellitus were diagnosed. 4 DN is characterized by persistent albuminuria (or albuminuria excretion rate of >300 mg/d or 200 μg/min) measured at least twice within three to 6 months interval, progressive decreasing in glomerular filtration rate (GFR), 8 which often occur in association with an elevate in blood pressure, ultimately leading to end-stage renal disease. 9
It is critical to diagnose patients who are more sensible to develop DN for better control of the process of disease. Several factors and mechanisms enhance to the development and outcome of diabetic nephropathy. Albuminuria has been one of the biomarkers to screen renal function 10 and it has generally been examined to primarily reflect glomerular injury and increased glomerular permeability to macromolecules. 11 However, it may not be detectable in early stage. 10 Albuminuria has lots of limitations such as larger variability and low sensitivity, it cannot predictably lead to a renal outcome nor are specific for DN. 12 There are several significant kidney damage and disease biomarkers which helps in early detection of DN. 7 Biomarkers are defined as characteristic factors that can be objectively measured and assessed as an indicator of normal physiologic or pathogenic processes. Examples of biomarkers are proteins, lipids, microRNAs, genomic, metabolic or proteomic patterns, electrical signals, imaging determinations, and cells present on a urine analysis. 13
An early biomarker may allow earlier diagnosis, treatment reduces DN prevalence and slows DN progression, thereby raising life expectancy among people with diabetes while increasing healthcare spending by less than one percent. 14 A several of biological markers associated with diabetic nephropathy were found in recent years, which was significant for predicting the occurrence and development of the disease. Therefore, this review focuses on laboratory biomarkers that are earlier, more specific and sensitive biomarkers with greater predictability than microalbuminuria or those appearing at that time for early detection of DN.
Materials and methods
The researcher performed a review of the literature with Medline, Google Scholar, and Cochrane Library databases search for English language and human study articles registered from January 2011 to June 2021. The researcher used the following search terms: “early detection,” “diabetic nephropathy,” “Diabetes kidney disease,” “biomarker,” “early diagnosis,” and “type 2 diabetes mellitus” The keywords were searched alone or in combination with other keywords.
The abstracts and conference proceeding from the ICS annual meetings were also searched. Abstracts presented at international conferences and additional relevant publications were selected from the reference lists of identified articles were also included. No language restriction was defined. Abstract and conventional reports were excluded
Result
Studies of biomarker of early detection in diabetic nephropathy patients.
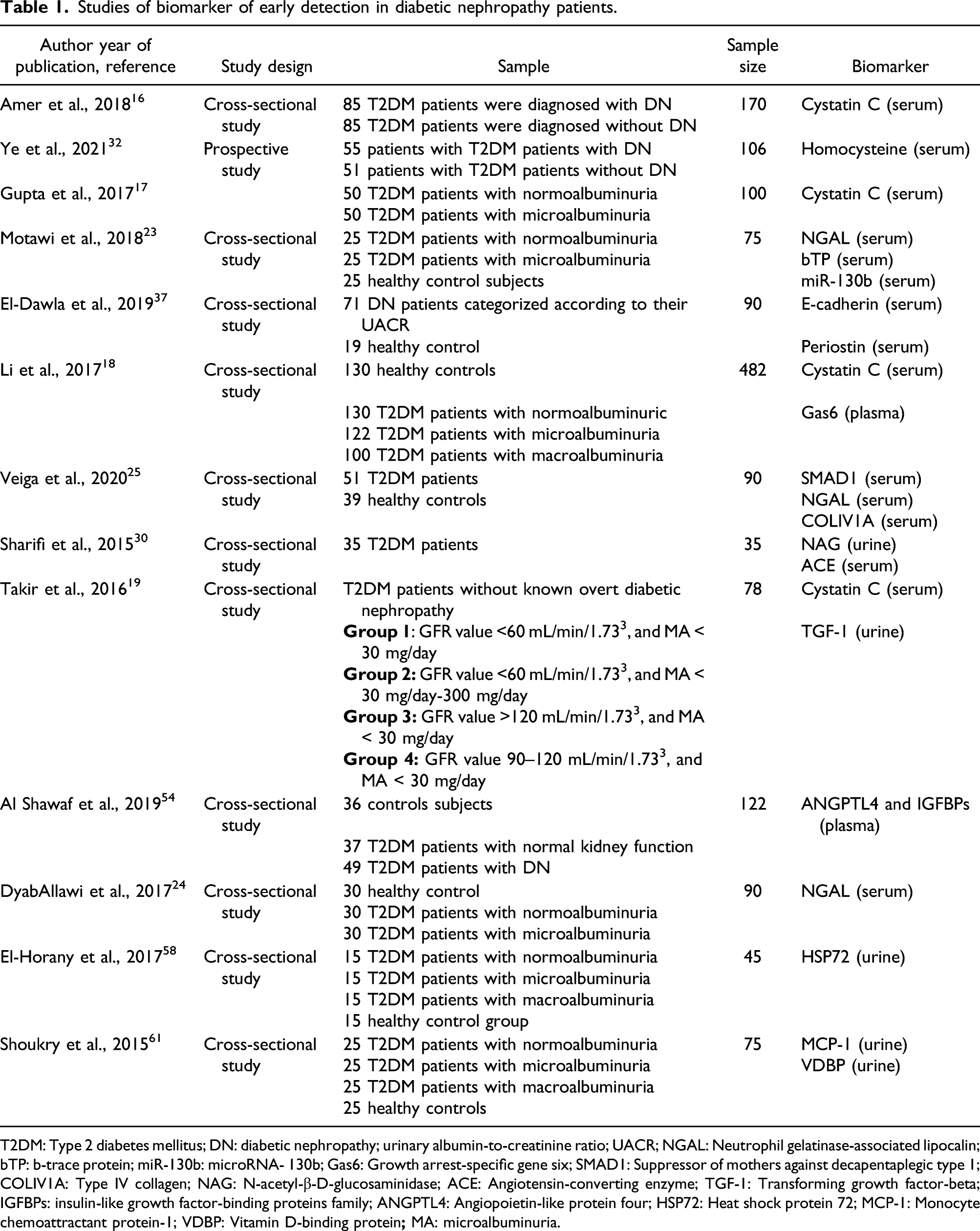
T2DM: Type 2 diabetes mellitus; DN: diabetic nephropathy; urinary albumin-to-creatinine ratio; UACR; NGAL: Neutrophil gelatinase-associated lipocalin; bTP: b-trace protein; miR-130b: microRNA- 130b; Gas6: Growth arrest-specific gene six; SMAD1: Suppressor of mothers against decapentaplegic type 1; COLIV1A: Type IV collagen; NAG: N-acetyl-β-D-glucosaminidase; ACE: Angiotensin-converting enzyme; TGF-1: Transforming growth factor-beta; IGFBPs: insulin-like growth factor-binding proteins family; ANGPTL4: Angiopoietin-like protein four; HSP72: Heat shock protein 72; MCP-1: Monocyte chemoattractant protein-1; VDBP: Vitamin D-binding protein
Serum cystatin C
Cystatin C, a 13 kDa cysteine protease inhibitor, a small protein that freely filtered by the renal glomeruli, is a novel biomarker of kidney failure. Cystatin C has been associated with the decrease of eGFR and predictors of the progression of type 2 DN. 15 Serum cystatin C is a marker of kidney function. The mean serum cystatin C level was higher in diabetic nephropathy patients (1.87 ± 0.51 mg/L) than non-diabetics nephropathy (1.025 ± 0.30 mg/L), and the difference was significant with p-value <0.001. The results revealed a significant correlation between serum cystatin C with creatinine (r = 0.55; p < 0.001) was higher in all the patients who had an abnormally high serum creatinine level. The study suggested that serum cystatin C measurement is useful for the early detection of renal impairment in a way better than serum creatinine in the patients with diabetes. 16 Another study showed that the mean serum cystatin C values in type 2 diabetes with normoalbuminuria were 1.73 and in type 2 diabetes with microalbuminuria were 2.07 17 . The results show that the serum cystatin C values were raised in the patients with microalbuminuria. The study suggested that serum cystatin C may be considered as an early marker than microalbuminuria and serum creatinine. Emphasizing in serum cystatin C was significantly higher in diabetic patients with microalbuminuria or macroalbuminuria, as compared with diabetic subjects with normoalbuminuria. 18 One study reported that serum cystatin C level was significantly higher in normoalbuminuric group and was found to negatively correlate with eGFR in group two patients (r = −0.892, p < 0.001). Finally, there was a negative correlation between eGFR and serum cystatin C in all the patient groups (r = −0.726, p = 0.001). The study suggested that serum cystatin C level was indicated to be used as an early biomarker of diabetic nephropathy. 19 All these data suggest that serum cystatin C is a promising biomarker for early DN in type 2 diabetics.
Neutrophil gelatinase-associated lipocalin
Neutrophil gelatinase-associated lipocalin (NGAL)L is a 25-kDa molecule which was produced in the distal nephron and increased in response to kidney injury within a few hours after damaging. 20 NGAL excretion in serum and urine were found to be early predictive biomarkers of acute kidney injury. 21 The appearance of NGAL in the urine may indicate early glomerular injury, and this has been showed at earlier stage than the appearance of microalbuminuria, the gold standard marker for early DN. 22 Recent study reported that serum NGAL was significantly higher in T2DM with microalbuminuria group compared to T2DM with normalbuminuria and control groups with significant positive correlation with age and duration of DM. The best cut-off value of NGAL for early detection of DN is 77.72 ng/mL with sensitivity 96%, specificity 80%, PPV 82.6%, NPV 95.24%, and accuracy 88%. 23 Another study found that the mean value of serum NGAL was significantly higher in microalbuminuria than normal albuminuria and healthy control group (p < 0.05). 24 Another study including non-diabetic subjects with aged 21 years or older. The type 2 DM group consisted of patients diagnosed with Type 2 DM for at least 5 years without impaired renal function, aged ≥21 years and under pharmacological treatment for DM2. Peripheral blood NGAL gene expression was increased in patients with type 2 DM compared with healthy individuals (type 2 DM 0.09758 ± 0.1914* 2−ΔCq vs CTL 0.02293 ± 0.04578). 25 The results showed a positive correlation between serum NGAL and HbA1c in T2DM patients with normoalbuminuria, 23 which is in agreement with DyabAllawi et al. 2017 who showed significant correlation between serum NGAL and HbA1c % (r = 0.394, p = 0.03) 24
NGAL is filtered from plasma through glomerular filtration and after filtration the NGAL is reabsorbed by endocytosis via the megalin system in proximal tubule. 26 When proximal tubule is injured by tubular necrosis filtered NGAL can leave tubular reabsorption and secreted in urine, high serum NGAL and high filtered saturates tubular capacity that lead to increase urinary and serum NGAL, 27 so that it is recommended that serum NGAL can be used as a biomarker of glomeruli injury which precedes the appearance of microalbuminuria. 28
N-acetyl-β-D-glucosaminidase
N-acetyl-β-D-glucosaminidase (NAG), an enzyme (MW 130 kDa) involved in carbohydrate metabolism, cannot be filtered from blood through an intact glomerular membrane due to its high molecular weight (140 kDa), thus presence in urine is exclusively secreted by tubular cells lysosomes of the proximal tubule epithelial cells. 29 Its activity detected in urine may reflect an early sign of renal disorder. One study showed that urine NAG level in the diabetic group was higher compared with controls (p < 0.05), which indicates that the elevated urine NAG, as an early indicator of renal damage. 30
Serum homocysteine
Homocystein (Hcy) is the intermediate product of cysteine and methionine. 31 One study showed that the serum Hcy levels were 15.49 ± 5.40 and 9.23 ± 3.15 μmol/L for DN and Type 2 DM patients, respectively, which indicated that serum Hcy in DN was higher than Type 2 DM patients and correlated with patient’s renal damage. Applying serum Hcy as the reference, the diagnostic sensitivity, specificity, and AUC were 84.31 (71.41–92.98) %, 74.55 (61.00–85.33) %, and 0.85 (0.78–0.92) %, respectively, with the cut-off value between DN and Type 2 DM groups is 12.08, serum Hcy can also be used as a serological marker for early diagnosis of DN with relatively high sensitivity and specificity. 32
b-trace protein
b-trace protein (bTP), known as lipocalin prostaglandin D2 synthase (L-PGDS), is an emerging marker of GFR. It is also a low-molecular-weight glycoprotein that belongs to the lipocalin superfamily. 33 One study reported that bTP was significantly elevated in Type 2 DM patients with microalbuminuria compared with Type 2 DM patients with normoalbuminuria and control subjects. They suggest that serum bTP as glomerular and tubular markers, respectively, may be reliable and independent biomarkers for early detection of DN. 23
microRNA-130b
MicroRNA-130b (miR-130b) has been shown to play roles in mesenchymal differentiation, hypoxic response immune cell function, modulation, and aging process. 34 One study showed that serum miR-130b was significantly lower in Type 2 DM with microalbuminuria group than that in Type 2 DM with normalbuminuria and control groups, and its level was markedly and gradually declined in the Type 2 DM patients with normoalbuminria group and Type 2 DM with microalbuminuria group. So, reduced serum miR-130b level can be appraised as a good predictor for DN even before the presence of albuminuria in view of its reno-protective role by inhibiting lipid peroxidation reaction, renal fibrosis, chronic inflammation, and extracellular matrix deposition. 23
E-cadherin levels
E-cadherin is a transmembrane integral protein which is detected at the adherent junction of the epithelial cells. It is plenty in the distal tubules. 35 In the early stages of epithelial-to-mesenchymal transition, losing of E-cadherin expression occurs and the separation of cells within the epithelial sheet happens. 36 One study reported that E-cadherin levels were significantly declined in all groups (0.94, 0.52, and 0.14 ng/mL in normoalbuminuria, microalbuminuria, and macroalbuminuria groups; respectively), when compared with control group. UACR was negatively correlated with E-cadherin. ROC curve analyses showed that the AUC to diagnose established microalbuminuria using E-cadherin was 0.998 (95% CI 0.932–1). The study suggests that serum E-cadherin could be considered as reliable markers involved in DN pathogenesis and coordinated to its stages. 37
Periostin
Periostin is one of markers lead expression of mesenchymal phenotype in renal cells.
38
It is discharged when distal tubules are injured
Growth arrest-specific gene 6 (Gas 6)
Growth arrest-specific gene 6 (Gas 6) is a newly found vitamin K-dependent protein, interacting with the TAM family (Tyro-3, Axl, and Mer).
40
Gas/TAM signaling has been revealed to be involved in the pathogenesis of diabetic renal disease
Suppressor of mothers against decapentaplegic type 1
Suppressor of mothers against decapentaplegic (SMADs) are intracellular proteins capable of regulating transcription factors and expression of target genes; once activated, these proteins migrate to the nucleus, where they trigger or suppress the transcription of different target genes. 42 Recent studies have found that SMADs can be detected in the urine of patients with DN. 43 A study revealed that gene expression data: peripheral blood SMAD1 (blood: DM2 0.01102 ± 0.04059* vs CTL 0.0001317 ± 0.0003609; urine: DM2 0.7195 ± 2.344* vs CTL 0.09812 ± 0.4755). These genes demonstrated perfect specificity and sensitivity in the receiving operating characteristic curve evaluation. They suggest the potential use of SMAD1 gene expression in peripheral blood and urine samples as early biomarkers of DN. 25
Type IV collagen
Type IV collagen (COLIV) is a protein that is part of the base of basement membranes
Angiotensin-converting enzyme
The urinary enzymes which have low activity in urine in normal status and may rise after renal tubular cells injuries can be used for the assessment of the kidney function.
46
There were various studies reported that angiotensin-converting enzyme (ACE) activity can cause vascular smooth muscle cell proliferation and also leads the release of platelet-derived growth factor and transforming growth factor which among patients in diabetic vasculopathy.
47
A study showed that mean serum ACE levels in the diabetic group was higher than control groups (p < 0.001) but urine ACE levels in diabetes patients did not differ between two group
Transforming growth factor-beta
Transforming growth factor-beta (TGF-1) is relative in DN pathogenesis. It causes mesangial extension by promoting renal cellular hypertrophy and by leading the extracellular matrix expansion. 48 Urinary TGF-1 levels are raised as commensurate to the severity of the nephropathy. 49 The results of serum and urine TGF-1, they found that the levels in group 2 (GFR value <60 mL/min/1.733, and microalbuminuria (MA) < 30 mg/day-300 mg/day) were significantly higher than group 4 (GFR value 90–120 mL/min/1.733, and MA < 30 mg/day) (p = 0.012; p = 0.012). In three patient groups (GFR value >120 mL/min/1.733, and MA < 30 mg/day), which do not have MA in their study, they have found the serum and urine TGF-1 levels were significantly higher in the groups with MA. 19 Previous studies showed that TGF-1 concentration from renal vein was found positive in diabetic patients 50 and TGF-1 level from urine in the diabetic patients raised fourfold than the non-diabetic patients. On the other hand, the result of this study was different from previous study, increased urine TGF-1 excretion was demonstrated in all diabetic patients regardless of MA status. 19
Angiopoietin-like protein 4 and insulin-like growth factor-binding proteins family (IGFBPs)
Angiopoietin-like protein 4 (ANGPTL4) is a glycoprotein (≈45–65 kDa) emitted by a wide range of cells such as hepatocytes, adipocytes, macrophages, myocytes, endothelial, and intestinal cell. 51
Insulin-like growth factor-binding proteins family (IGFBPs), can enhance development of the diabetic kidney syndrome. This group of proteins comprises six high-affinity binding proteins (IGFBP1–IGFBP6). 52 At a state of diabetic kidney syndrome, renal IGFBP1 was found to rise at both protein levels and mRNA. Although the involvement of IGFBP3 in diabetic microalbuminuria and DN has been studied also. 53
ANGPTL4 level was raised in people with DN (241:56 ± 14:1 μg/mL) compared to the control group (178:43 ± 24:09 μg/mL). The increase in ANGPTL4 related with clinical parameters of DN including albumin-to-creatinine ratio (r = 0:271, p = 0:002), serum creatinine (r = 0:381, p = 0:0001), and eGFR (r = −0:349, p < 0:0001). Furthermore, ANGPTL4 related positively with both IGFBP1 (r = 0:202, p = 0:026) and IGFBP4 (r = 0:364, p < 0:0001). Multiple regression analysis presented increased IGFBP1 and TG as predictors of higher ANGPTL4 in patients with DN. In patients with Type 2 DM, only IGFBP1 acted as a positive predictor of an increase in ANGPTL4. In this study, their data revealed a significant increase in circulating ANGPTL4, IGFBP1, and IGFBP4 in patients with DN. The elevation in ANGPTL4 correlated significantly with clinical markers of DN such as serum creatinine, ACR, and eGFR, as well as IGFBP1 and IGFBP4. Totally, this supports ANGPTL4 as a biochemical marker for the detection of a diabetic kidney disease in Type 2 DM patients. 54
Heat shock protein 72
Heat shock protein 72 (HSP72
Monocyte chemoattractant protein-1
Monocyte chemoattractant protein-1 (MCP-1) is a one member of the CC chemokine family produced by a variety of cell types, including mesangial cells, glomerular endothelial cells, tubular epithelial cells, and monocytes in response to inflammatory cytokines (IL-1, TNFα, and INFγ). 59 Previous evidence has investigated the role of MCP-1 in DN and presented it as a major factor influencing macrophage recruitment and accumulation in renal disease. Some studies have reported that urinary monocyte chemoattractant protein-1 (uMCP-1) levels are increased in inflammatory renal diseases and diabetic nephropathy. 60 One study showed that, a significant elevation in the uMCP-1 levels was found in macroalbuminuric (p < 0.001) and microalbuminuric (p < 0.01) diabetic patients compared to that in normoalbuminuric diabetic patients and control subjects (p < 0.001). Correlation study showed that uMCP-1 was importantly positively related to urinary albumin/creatinine ratio (r = 0.968, p < 0.001), serum urea (r = 0.461, p = 0.001), and serum creatinine (r = 0.475, p = 0.001) and significantly inversely correlated to glomerular filtration rate (r = −0.983, p < 0.001). Receiver operating characteristic (ROC) curve analysis of uMCP-1 levels for early detection and diagnosis of DN showed that the cut-off value of uMCP-1 was 110 pg/mg with 100% specificity and 92% sensitivity. The findings suggest that uMCP-1 may be considered as novel potential diagnostic biomarkers for the early detection of diabetic nephropathy. 61
Vitamin D-binding protein
Vitamin D-binding protein (VDBP), is a 58–kDa glycoprotein and is show in the serum at a concentration of 300–600 mg/mL. In the kidney, VDBP is involved in the endocrine biosynthetic process of 1,25-dihydroxyvitamin D [1,25(OH)2D] within renal proximal tubules.
62
Current article revealed that urine vitamin D-binding protein (uVDBP) is raised compared to that in non-diabetics, especially when albuminuria is present.
63
A significant elevation in the uVDBP levels was found in macroalbuminuric (p < 0.001) and microalbuminuric (p < 0.01) diabetic patients compared to that in normoalbuminuric diabetic patients and control subjects (p < 0.001). Correlation study showed that uVDBP was significantly positively correlated to urinary albumin/creatinine ratio (r = 0.973, p < 0.001), serum urea (r = 0.456, p = 0.002), and serum creatinine (r = 0.448, p = 0.004) and significantly inversely correlated to glomerular filtration rate (r = −0.988, p<0.001). Receiver operating characteristic (ROC) curve analysis of uVDBP levels for early diagnosis and detection of DN revealed that the cut-off value of uVDBP was 550 ng/mg with 84% specificity and 96% sensitivity. The results of the present study suggest that uVDBP may be appraised as novel diagnostic biomarkers for the early detection of diabetic nephropathy.
61
The role of VDBP in the pathogenesis of DN is not clear
Conclusion
Microalbuminuria is an early marker of DN. Measurement of microalbuminuria is a routine clinical practice for screening, but the injury to the kidney may be happening even without microalbuminuria. It is significant to implement different strategies for earlier detection of DN because of an early biomarker may allow earlier diagnosis, treatment reduces DN prevalence and slows DN progression and increasing quality of life among people with diabetes mellitus. Mostly biomarkers were significantly higher in type 2 diabetic patients with normoalbuminuria, microlbuminuria, and macrolbuminuria compared with non-diabetic group and could be used as early markers before the development of DN. However, multicenter prospective studies are still needed to confirm these biomarkers in order to use for screening in everyday setting.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Excellence Center of Community Health Promotion, School of Nursing, Walailak University