
Abstract
Purpose:
To determine the effects of bariatric surgery on albuminuria in obese patients with type 2 diabetes mellitus.
Methods:
Retrospective analyses of clinical records of obese patients with type 2 diabetes mellitus who had either micro- or macroalbuminuria and had undergone various bariatric surgery were retrieved from a local hospital database. Their clinical data from follow-up appointments including albuminuria were analysed.
Results:
Of the 46 subjects with type 2 diabetes mellitus, 15 subjects had diabetic nephropathy and had pre- and post-bariatric surgery urine albumin-to-creatinine ratio or urine protein-to-creatinine ratio data available for analysis; 13 out of the 15 subjects (86.7%) showed improvement of urine albumin-to-creatinine ratio or urine protein-to-creatinine ratio after surgery; 2 showed equivocal results; 9 of 13 subjects (69.2%) showed remission of diabetic nephropathy; 7 of these 9 patients had microalbuminuria before surgery, 2 had macroalbuminuria before surgery.
There were significant improvements to glycosylated haemoglobin, fasting plasma glucose, blood pressure and body weight post surgery. The usage of insulin and oral medications dropped significantly post surgery for all subjects.
Conclusion:
This study shows that bariatric surgery significantly improves diabetic nephropathy in obese type 2 diabetes mellitus subjects. The results suggest that in our local type 2 diabetes mellitus patients, it is possible not only to improve metabolic parameters, but also to reverse what may be considered established microvascular complications by means of bariatric surgery.
Introduction
The incidence of diabetes mellitus has risen rapidly in the past few decades, and its prevalence in Singapore in adults aged 20–79 years has reached 12.8% in 2015. This gives an estimated number of 541,600 adults with diabetes. 1
Diabetic nephropathy (DN), or diabetic kidney disease (DKD), is one of the major microvascular complications of type 2 diabetes mellitus (T2DM) and is a leading cause of end-stage renal disease (ESRD) with high morbidity and mortality. Up to 40% of patients with T2DM develop DKD and this is associated with a fourfold increase in 10-year relative risk of death.2,3
In Singapore, DN is the leading cause of ESRD and constitutes 64.9% of incident haemodialysis and 63.4% of peritoneal dialysis in 2014. 4 Numerous studies have examined the benefits and risks of bariatric surgery (BS) versus conventional therapy in the treatment of obese patients with T2DM. BS has been shown to result in improvements in weight reduction, glycaemic control and even remission of diabetes.5,6 However, not many studies have looked at changes in microvascular complications after BS. Local data in this area are particularly lacking.
The aim of this study was to evaluate the effect of BS on DN in obese T2DM subjects as measured by changes in urine albumin-to-creatinine ratio (uACR) or urine protein-to-creatinine ratio (uPCR) in a local public hospital in Singapore.
Methods
This was an observational retrospective cohort study. In all, 150 multi-ethnic obese subjects, who had BS between January 2011 and December 2014 and had follow-up data for 2 years, were retrieved from our hospital database. The data were collected from both electronic medical records as well as their traced handwritten case notes. The subjects were followed up as outpatients post surgery. Only 46 had T2DM. Glomerular filtration rate (GFR) was computed using the modified Modification of Diet in Renal Disease (MDRD) formula and chronic kidney disease (CKD) stage was categorised based on KDIGO 2012 clinical practice guidelines. 7 This study was approved by the National Healthcare Group Institutional Review Board (Ethics Ref. No. 2015/01075).
Data collected included their demographics and pre- and post-operative parameters of fasting plasma glucose (FPG), glycosylated haemoglobin (HbA1c), estimated glomerular filtration rate (eGFR), uACR or uPCR, blood pressure (BP), low-density lipoprotein (LDL) cholesterol levels and body weight. The usage of diabetic medications including insulin, as well as renin–angiotensin–aldosterone system (RAAS) blockers, was recorded. Data on the relevant parameters were collected for up to 2 years post surgery.
Determination of micro- and macroalbuminuria was based on spot urine ACR and PCR measurements. Data from early morning urine samples (66.7%) were used as far as possible. Normoalbuminuria was defined as ⩽2.5 mg/mmol for males and ⩽3.5 mg/mmol for females. Microalbuminuria was defined as >2.5–30 mg/mmol for males and >3.5–30 mg/mmol for females. Macroalbuminuria was defined as >30 mg/mmol (equivalent to PCR >50 mg/mmol or Total Urine Protein (TUP) >0.5 g/day). Patients were monitored with urine PCR if urine ACR > 30 mg/mmol.
Patients were categorised as improved or not improved based on the change in albuminuria as well as the micro- or macroalbuminuria classification within the 2-year period of available data collection. Urine ACR or PCR readings were taken pre-BS operation and compared with the last available reading post operation within the 2-year period to determine whether there is an improvement.
Patients who improved included those who had a decrease in macroalbuminuria levels or who went from macroalbuminuria to microalbuminuria or normoalbuminuria or who went from microalbuminuria to normoalbuminuria. Those who were defined as being in remission were those who went from macroalbuminuria to normoalbuminuria or those who went from microalbuminuria to normoalbuminuria.
Analysis of the data was done using Stata 14.0 (STATA Corporation). Data were presented as number (percentages), mean ± standard deviation or median [interquartile range (IQR)] as appropriate. The differences in continuous parameters pre- and post-surgery were examined by paired t-test or Wilcoxon signed-rank test depending on the distribution of the variables. The differences in categorical variables pre- and post-surgery were examined by McNemar’s test.
Results
Of the 46 subjects with T2DM, 23 had normal uACR and eGFR >60 mL/min (1.73 m2) before the operation. One subject with eGFR in CKD3a range had normal uACR before and after the operation. Seven had missing data, that is, no uACR results either before or after surgery. Only 15 T2DM subjects had pre- and post-BS uACR data available for analysis (Figure 1).
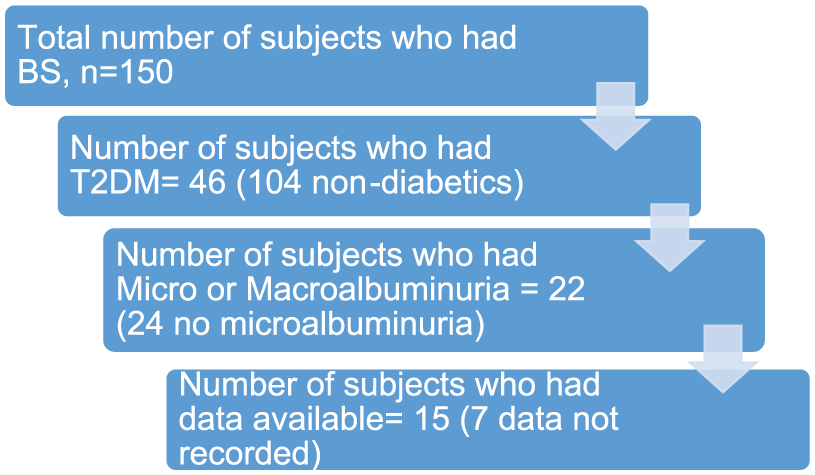
Flowchart showing process of sample selection.
Of these 15 subjects, 10 (66.7%) had eGFR > 60 mL/min (1.73 m2) before and after BS; 2 (13.3%) each had CKD stage 3a and stage 3b, respectively; and 1 (6.7%) had CKD stage 4 before and after BS. At baseline, 53.3% (8 out of 15) subjects had macroalbuminuria before BS. Baseline body mass index (BMI) ranged from 26.4 to 57.4 kg/m2 before BS. Of these subjects, 60% (9 out of 15) were Malays, 20.0% (3 out of 15) were Chinese and 20.0% (3 out of 15) were Indians (Table 1).
Baseline characteristics of 15 subjects.
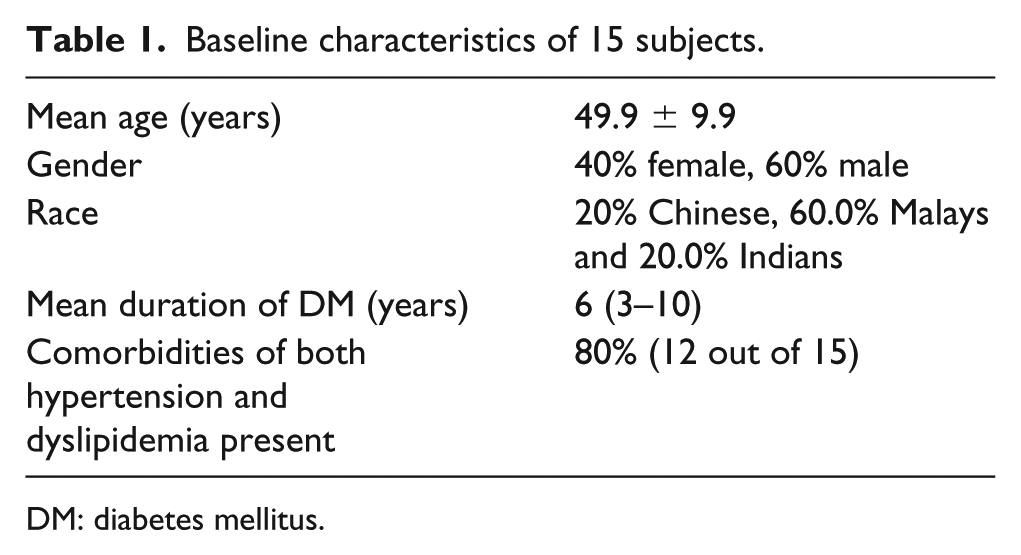
DM: diabetes mellitus.
Out of these 15 subjects, 2 had laparoscopic gastric bypass (LAGB) done, 5 had sleeve gastrectomy (SG) and 8 had Roux-en-Y gastric bypass (RYGB) done.
Overall, 13 out of the 15 subjects (86.7%) showed improvement of uACR after surgery. The remaining 2, both with CKD stage 3b and macroalbuminuria, showed equivocal results. Out of the 13 subjects, 12 (92.3%) showed a ⩾50% improvement of either uACR or uPCR results; 9 out of 13 subjects (69.2%) showed remission of DN, and all 9 had eGFR > 60 mL/min; 7 out of these 9 patients had microalbuminuria before surgery (uACR < 30 mg/mmol); 2 had macroalbuminuria before surgery.
In the 15 T2DM subjects, the uACR before and 3.5 month (median, 2–6 months) after BS was 14 mg/mmol (IQR = 7.2–92.3) and 4.3 mg/mmol (IQR = 1.3–17.0; p = 0.005), respectively. This is equivalent to a 69.3% drop in uACR (Table 2).
Parameters pre- and post-operation.
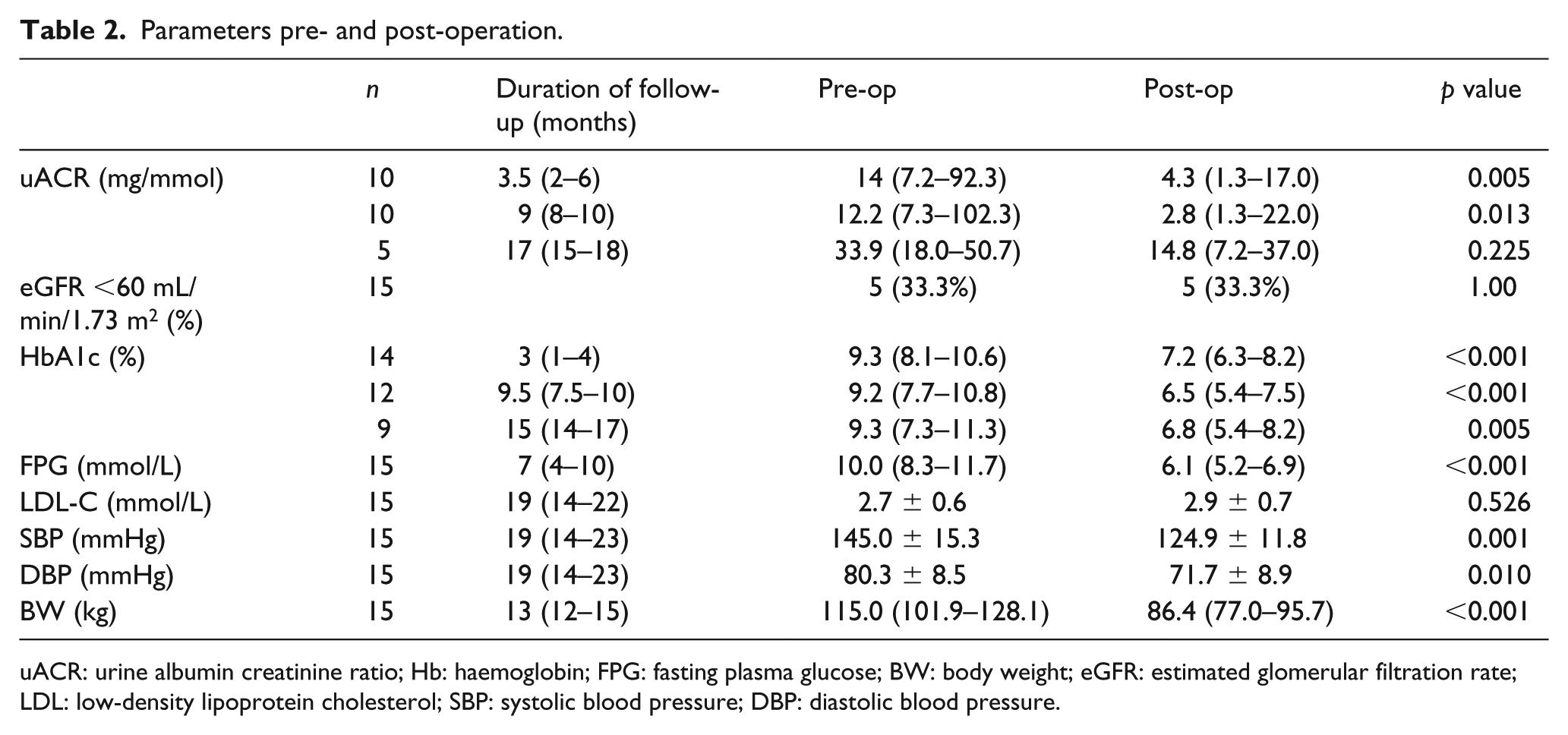
uACR: urine albumin creatinine ratio; Hb: haemoglobin; FPG: fasting plasma glucose; BW: body weight; eGFR: estimated glomerular filtration rate; LDL: low-density lipoprotein cholesterol; SBP: systolic blood pressure; DBP: diastolic blood pressure.
The uACR before and 9 months (median, 8–10 months) after BS was 12.2 mg/mmol (IQR = 7.3–102.3) and 2.8 mg/mmol (IQR = 1.3–22.0; p = 0.013). This is equivalent to a 77.0% drop in uACR (Table 2). There were significant improvements to HbA1C, FPG, both systolic and diastolic BP and body weight post surgery (Table 2). The usage of oral anti-diabetic drugs (OADs), insulin and RAAS blockers also dropped significantly post surgery for all subjects (Table 3).
Medications pre- and post-operation.
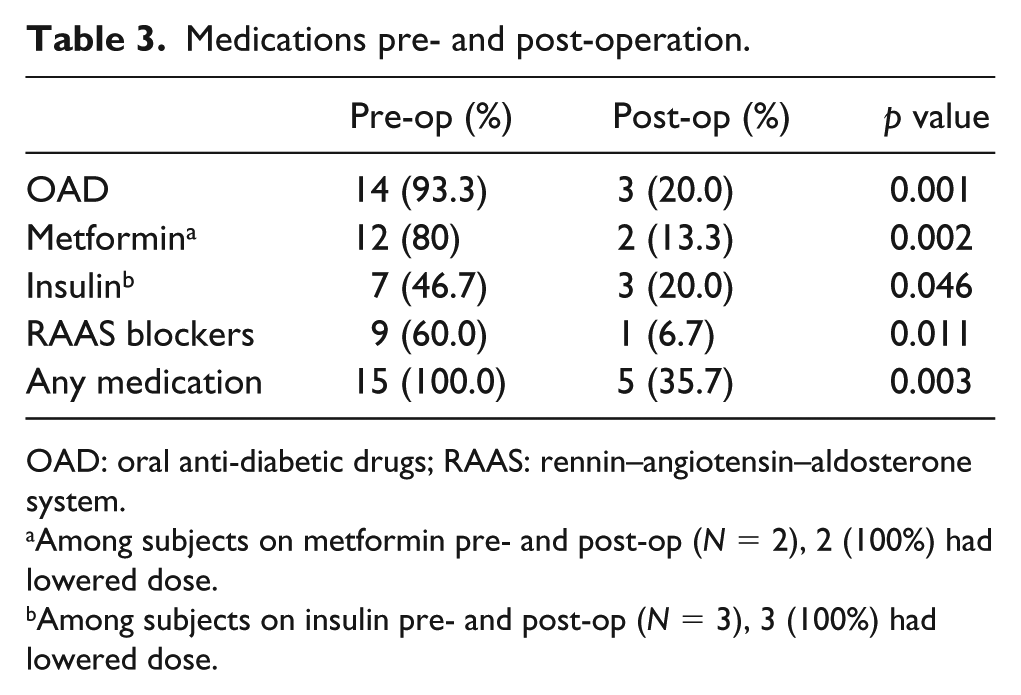
OAD: oral anti-diabetic drugs; RAAS: rennin–angiotensin–aldosterone system.
Among subjects on metformin pre- and post-op (N = 2), 2 (100%) had lowered dose.
Among subjects on insulin pre- and post-op (N = 3), 3 (100%) had lowered dose.
Discussion
To the best of our knowledge, this is the first study done in Singapore looking at the effect of BS on DN in T2DM patients. Our data suggest that BS improves DN in obese T2DM subjects. In our retrospective analysis, 13 out of 15 subjects (86.7%) showed improvement in DN and 9 out of the 15 subjects (69.2%) who improved in fact had remission of DN after BS. Out of the 9 subjects who enjoyed remission in DN 7 had microalbuminuria and 2 had macroalbuminuria pre-surgery (both had GFR > 60).
There were no significant differences in the baseline characteristics of subjects who showed improvement of albuminuria versus those who did not show improvement. The two subjects who showed equivocal results both had CKD3b and macroalbuminuria. However, 6 out of the 8 (75%) subjects with macroalbuminuria showed improvement. Both subjects with CKD3a, as well as the one subject with CKD 4, also showed improvement of uPCR up to 2 years post BS, and they all had macroalbuminuria.
The pathophysiology of diabetes and obesity is complex and multifactorial, and evidence suggests that obesity itself is an independent risk factor for DN, independent of diabetes and hypertension.8,9 Few studies have compared the effects of BS versus non-surgical treatments on hard renal endpoints. However, the studies published so far have showed improved outcomes, although the numbers are generally small.10–12
We used uACR and uPCR as a marker of kidney damage as it has a better predictive value for development of overt nephropathy and cardiovascular disease. Albuminuria is also a major clinical manifestation of DN. 13 Although we also measured and monitored the eGFR as a marker of renal function, it is not a sensitive marker of early kidney disease in diabetes. eGFR should also be interpreted with caution as it incorporates creatinine as a factor and creatinine can be reduced because of lean-mass loss after BS and lead to misleading increase in eGFR measurements. 14 In our analysis, there were no significant changes in the eGFR measurements pre- and post-surgery.
The outcomes of BS can be varied and operator dependent, and as safety is of utmost importance in the management of our patients, all the surgeries were performed by a senior bariatric surgeon with more than 10 years of BS experience. Our centre is also one of the centres which has the most number of BS done in Singapore.
Surgery performed included Sleeve Gastrectomy (SG), Roux-en-Y gastric bypass (RYGB) and Lap-Adjustable Gastric Bypass (LAGB). Our results are similar to earlier retrospective studies on effects of BS on DN, such as Zhang et al.’s 15 RYGB, Stephenson et al.’s 16 LAGB or Iaconelli et al.’s 17 prospective study on bilio-pancreatic diversion (BPD) surgery. All three studies showed improvement of DN post surgery. Zhang et al. showed improvement of both DN and DM in Chinese subjects, which was more beneficial to those with lower pre-op ACR and creatinine. Stephenson et al. showed some improvement of both macro as well as microalbuminuria, with 2 out of 7 patients with macroalbuminuria reverting to normoalbuminuria and 9 out of 16 microalbuminuria patients reverting to normoalbuminuria. Iaconelli et al.’s unblinded case-control study of BPD versus medical intervention focussed on newly diagnosed DM subjects and showed that all subjects recovered from microalbuminuria after 10 years. However, the drop-out rates were high, with only 22 out of 50 subjects completing the study.
Amor et al.’s 18 prospective study also showed improvement of proteinuria after RYGB or SG but excluded nephrotic patients and those with eGFR < 60. Reid et al.’s 19 1-year retrospective study on effect of RYGB and SG also showed improvement of microalbuminuria but mainly on non-DM subjects and excluded subjects with CKD 3–5. Heneghan et al.’s 20 retrospective study of American subjects showed the effect of RYGB, SG and LAGB on DN and demonstrated 58.3% remission of DN 5 years after BS (n = 19).
Finally, the landmark STAMPEDE trial by Schauer et al.,21,22 which although looked primarily at end point of a HBA1C of 6.0% or less, had a secondary renal end point analysis which showed improvement of uACR which was more statistically significant for the group with SG compared to the group with RYGB at 3 years. Both groups undergoing BS also had intensive medical therapy on top of surgery and were compared in a 1:1:1 ratio with a control group with only intensive medical therapy. The results also showed more remission rates with the group who had SG done compared with RYGB or control (80% vs 62% vs 25%) at 3 years. However, it showed only significant decrease in uACR in the SG group at 5 years compared with the medical therapy group. Their numbers were also small (n = 23 for the albuminuria group at baseline at 3 years and n = 21 at baseline at 5 years for the intervention arms), but the results suggest that SG may be better for reduction of albuminuria compared with RYGB.
Some of the differences between the STAMPEDE study and our study include the following:
All their subjects had baseline GFR in the normal range, whereas in our study, it ranged from CKD 1 to 4, with GFR as low as 24 mL/min pre-op.
Most of their subjects in the study had microalbuminuria rather than macroalbuminuria before surgery; 14 or 28.6% had microalbuminuria versus 3 or 6.0% who had macroalbuminuria in the RYGB group, and 11 or 22.0% had microalbuminuria versus 1 or 2.0% who had macroalbuminuria in the SG group. In our study, the majority of our subjects had macroalbuminuria (8 out of 15 or 53.3%). Out of these, 2 out of 8 or 25% had macroalbuminuria in the RYGB group, 5 out of 5 or 100% had macroalbuminuria in the SG group, and 1 out of 2 or 50% had macroalbuminuria in the LAGB group.
Their subjects’ BMI ranged 36.0 ± 3.5, whereas ours ranged from 26.4 to 57.4 kg/m2 before BS, showing a much larger range of patients’ BMI.
Our study included patients not just with SG and RYGB, but also with LAGB done.
Finally, their subjects were mainly Caucasian versus our subjects who were all Asians and also Singaporeans in particular.
Subjects with CKD stages 3–5 (eGFR < 60) are often not included in BS studies, as the outcomes are generally not perceived to be favourable. 18 Studies on effects of BS on proteinuria mostly focus on cohorts with microalbuminuria or normoalbuminuria or both, but not on cohorts with macroalbuminuria. 23
The mechanisms underlying improvement of albuminuria and remission of DN is not clear, although studies have shown that reduction of uACR correlated with reductions of other traditional risk factors of renal disease, namely, glycaemia, BP and obesity.14,18,20 The improvements are likely to be multifactorial as each risk factor is independently associated with improvement of the hard renal endpoints. The metabolic benefits of BS are associated with the reduction of insulin resistance secondary to weight loss, resulting in improved insulin sensitivity, as well as alterations to the gut hormones that control insulin, and improvement of renal perfusion determinants such as decrease in intra-abdominal and renal venous pressure and reduction of inflammatory cytokines and leptins, leading to improvement in renal outcomes.8,14
Our study showed statistical significant improvement of HBA1C, FPG, both systolic and diastolic BP as well as weight loss for all three procedures (Table 2). However, it did not show any reduction in LDL cholesterol levels post BS. Previous studies reported inconsistent and inconclusive findings on the effect of BS on dyslipidemia, and it also depended on which procedure was performed.24–26
There were statistically significant reductions of all medications pre- and post-BS (Table 3). Pre-op, 14 subjects (93.3%) were on OADs, but post-op, only 3 subjects (20.0%) were on OADs (p value = 0.001). Specifically, Metformin used dropped from 12(80%) pre-op to 2 (13.3%) post-op (p value = 0.002). The remaining 2 subjects (100%) both had their doses reduced. Insulin use decreased from 7 (46.7%) to 3 (20.0%; p value = 0.046), and all remaining 3 subjects (100%) had their insulin doses reduced. The usage of RAAS blockers also decreased from 9 (60.0%) to 1 (6.7%; p value = 0.011). The overall use of all medication dropped from 15 (100%) pre-op to 5 (35.7%) post-op (p value = 0.003). The results were not surprising and were consistent with previous studies showing improvement of glycaemia and BP post BS.
In summary, our study is different in that it looks at the effects of the three types of BS (LAGB, RYGB and SG) commonly performed on obese T2DM patients in various stages of CKD,1–4 and with established T2DM, and not just on the newly diagnosed T2DM, or those with only milder DN, such as those with only microalbuminuria or those with no renal impairment. In this study unlike most other studies, a significant proportion of our subjects have macroalbuminuria. This reflects the kind of patients we see in secondary or tertiary care rather than in prospective studies which select patients who are not so advanced in their complication stage.
We note that our retrospective analysis has the limitations inherent of such study methods. Missing data precluded analysis of several potential subjects. The final sample size of patients who had adequate data for analysis was small as only a proportion of subjects who underwent BS had T2DM; and only fewer than half had albuminuria.
Conclusion
We conclude that metabolic improvement secondary to BS is associated with reduced albuminuria in obese Asians subjects with T2DM. We observed that albuminuria ameliorated after BS in tandem with improvement in major metabolic parameters such as weight, BP and glycaemia.
We view this as preliminary evidence that in our local multi-ethnic T2DM patients, it is possible not only to improve metabolic parameters but also to reverse what may be considered established microvascular complications by means of BS.
Larger studies including randomised controlled trials across Asia-Pacific region will need to be done not only on DN but also other microvascular complications to confirm or refute the notion that BS not only improves metabolic parameters in T2DM but perhaps also reverses what may be considered moderately advanced microvascular complications. This may have important consequences on future T2DM patient selection criteria for BS.
Footnotes
Acknowledgements
Anthony TL Chao would like to thank the Diabetes Centre for providing him with the help and support to take on this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.