
Abstract
Objective:
This study aimed to determine the neutrophil–lymphocyte ratio (NLR) as an inflammatory biomarker among type 2 diabetes mellitus (T2DM) patients with diabetic nephropathy (DN).
Methods:
A comparative cross-sectional study design was conducted on 199 T2DM patients attending Bole 17 Health Center, Addis Ababa, Ethiopia. The urine albumin test was done by the MICRAL-II test strip. Fasting blood sugar was measured by a glucometer. Complete blood count was analyzed using an automated hematology analyzer (HUMAN GmbH, Wiesbaden, Hesse, Germany). The student’s t-test, a chi-square test, and Pearson correlation were applied to analyze the data.
Results:
Out of the 199 diabetes mellitus patients, 45 (22.6%) and 154 (77.4%) were found with DN and without DN, respectively. Interestingly, the mean NLR value (2.66 ± 0.49) was found significantly higher in diabetic patients with DN compared to the mean NLR (1.65 ± 0.20) in diabetes patients without DN (p < 0.0001). The NLR showed positive significant correlation with variables such as age (r = 0.162, p = 0.023), duration of disease (r = 0.52, p < 0.0001), absolute neutrophil count (r = 0.712, p < 0.0001), total white blood cell count (r = 0.162, p = 0.022), systolic blood pressure (r = 0.338, p < 0.0001), and diastolic blood pressure (r = 0.731, p < 0.0001). On the other hand, negatively significant correlation was found between NLR and absolute lymphocyte count (r = −0.770, p < 0.000).
Conclusion:
The NLR was significantly increased in T2DM patients with DN, suggesting that inflammation and endothelial dysfunction could be an integral part of the pathogenesis of DN, and therefore, this ratio may be considered as a predictor and a prognostic biomarker of DN.
Keywords
Introduction
Diabetes mellitus (DM) refers to a group of common metabolic disorders that are characterized by hyperglycemia. It results from defects in insulin secretion, insulin action, or both. It causes major morbidity and mortality in society. 1 DM has recently assumed epidemic proportions and affects more than 460 million individuals worldwide. Global diabetic prevalence in 2019 was estimated to be 9.3% (463 million people), rising to 10.2% (578 million people) by 2030 and 10.9% (700 million) by 2045, with the greatest increase in the developing countries of Africa, South America, and Asia. 2 It is a systemic disease having serious microvascular complications such as diabetic nephropathy (DN), diabetic retinopathy, and diabetic neuropathy, and macrovascular complications, including stroke, cardiovascular diseases (CVDs), and peripheral vascular diseases. 3
DN is characterized by a typical feature of albuminuria (albumin > 300 mg/24 h) confirmed at least twice in 3–6 months intervals, permanent and irreversible decrease in glomerular filtration rate (GFR), and arterial hypertension. 4 It is diagnosed by continuous raise of albumin or protein in urine without other known renal diseases. 5 From DM clinic reports, the prevalence of proteinuria in diabetes patients (i.e., DN) ranges from 2% to 53.1% worldwide,6,7 5.3% to 53.1% in Africa, 8 and 15.7% to 29.5% in Ethiopia. 9
Total leucocyte count is a crude, but sensitive indicator of inflammation and is studied in many non-communicable diseases as an inflammatory marker such as acute myocardial infarction (MI), stroke, and heart failure. 10 However, the sub-types, particularly the neutrophils, lymphocytes, and subsequent calculation of neutrophil–lymphocyte ratio (NLR), which is relatively more stable than individual leukocyte parameters, could be altered by various physiological, pathological, and physical factors. 11 . The NLR is a simple and cheap laboratory tool studied as an inflammatory marker that is used to predict the prognosis of many non-communicable diseases such as acute MI, stroke, heart failure, appendicitis, cardiac diseases, cancer, and DN.12,13 Many developed countries use different biomarkers for diagnosis and follow-up of DN, but in Ethiopia, only limited biomarkers such as kidney function tests and albumin tests are used to diagnose DN. To the best of our knowledge, there are limited studies that determined inflammatory biomarkers, including NLR that are associated with DN in Ethiopia. Therefore, this study aimed to assess the NLR as an inflammatory biomarker of DN among type 2 DM (T2DM) patients.
Materials and methods
A cross-sectional study was conducted on 199 T2DM patients at Bole 17 health center, Bole sub-city, Addis Ababa, Ethiopia for a period of 7 months (from October 15, 2019 to April 14, 2020). The study was conducted following set down standards and after an ethical clearance letter was obtained from the Department Research and Ethics Review Committee, Department of Medical Biochemistry, College of Health Sciences, Addis Ababa University (Ref. No. SOM/BCHM/152/2011, Protocol No. MSc. 07/19). In addition, permission was obtained from Addis Ababa Health Bureau, Bole Sub-city, and Bole 17 health center medical director to conduct the study.
The sample size was estimated using the general formula for a single population proportion. The value of proportion (P) for the study was taken from a study conducted in Ethiopia, which was 29.5%,9,14,15 at 95% confidence interval, and 1.96 for Z and 5% for d, the sample size was determined using the formula: n = Zα/2 2 P (1 − P)/d2. Using this formula, the calculated sample size is 319. Averagely, 25 patients are admitted to the diabetic outpatient department daily, so monthly, around 550 patients are admitted. Since the study population is less than 10,000, finite population correction formula was used to calculate the actual sample size. So, corrected sample size = (sample size)*(population)/sample size + (population − 1) = 202. A convenient sampling technique was employed to recruit the study participants.
The purpose of this study was briefly explained to the study participants and they were informed through written consent that their responses will be treated with strict confidentiality. The samples and data were collected after the study participants gave full consent by signing the form. Confidentiality, anonymity, neutrality, and accountability were maintained throughout the study. All diagnosed T2DM patients who were attending the health center during the study period and voluntary to participate were included in the study. The patients with acute and chronic infections such as urinary tract infection, upper respiratory tract infection, lower respiratory tract infections, viral hepatitis, tuberculosis, HIV/AIDS CVD, chronic kidney disease, chronic liver disease, blood disorders and malignancy, patients on anti-inflammatory drugs like systemic or topical steroids, smokers, and alcoholic patients were excluded from the study. The study participants (T2DM patients) were grouped as “with DN” if their urine albumin tests on occasions were positive (from +1 to +4) and “without DN” if their urine albumin tests on occasions were negative.
Socio-demographic characteristics and other data related to T2DM were collected from participants using a structured questionnaire by experienced health professionals. Before data collection, the questionnaire was pretested in 5% of the sample size at Garji Health center, Addis Ababa. Body mass index (BMI) was calculated by dividing weight (kg) by height square (m2).16,17,18 Blood pressure was measured using a mercury sphygmomanometer with a cuff deflation rate of mmHg. The average of the two measurements from the left-arm 5 min apart in the sitting position was recorded.16,17,18
Laboratory measurements
Ten milliliters of urine were collected and albuminuria was tested by MICRAL-II test strips by the dipstick method. In Ethiopia, DN is diagnosed with persistent albuminuria (>300 mg/dl) that is confirmed on at least two occasions (3–6 months apart). Furthermore, progressive decline in the GFR and elevated arterial blood pressure are also used as additional screening criteria. 19 Urinary albumin excretion of greater than 300 mg/dl (from +1 to +4) was considered as macroalbuminuria (reported as albumin positive) and the test was repeated within 3 months of interval. Approximately, 4 or 5 mL of venous blood was withdrawn in the EDTA vacutainer tube. The laboratory technologist confirmed that the patient is on overnight fasting by asking each patient before blood sample collection. The fasting blood sugar (FBS) level of participants was measured by a glucometer. The leukocyte, neutrophil, and lymphocyte counts were carried out using the automated hematology analyzer (HUMACOUNT PLUS) and expressed in cells/mm3. The test for blank was ⩽ % 0.2 × 109 cells/l. Then, NLR was calculated by dividing the neutrophil by the lymphocyte count.
Statistical analysis
Simple descriptive statistics such as mean, standard deviation, percentiles, and percentages were used to present socio-demographic characteristics, clinical parameters, NLR, and other laboratory tests, and the values were compared between DN and without DN patients. The data were entered using Epi-data statistical software version 3.1, and then exported to SPSS software version 21.0 for analysis. Student’s t-test and a chi-square test were used to test significant differences between the means of dependent quantitative variables and independent categorical variables of the two groups (T2DM with and without DN) and Pearson correlation was applied to analyze the relationship between NLR and other independent and dependent variables. The p values <0.05 were considered to be statistically significant in all analyses.
Operational definition
DN: Patients already diagnosed with T2DM and with urine albumin test positive on two separate urine albumin tests in the interval of 3 months.
Albumin positive: Is defined as the presence of albumin in the urine using two separate urine dipstick tests, which is from +1 to +4.
Albumin negative: Is defined as the absence of albumin in the urine on two separate urine dipstick tests.
Results
In this study, diagnosed T2DM patients (age 30 and above) were screened for DN with their written informed consent. A total of 202 patients were enrolled in this study; however, three patients were excluded because of incomplete data; therefore, 199 patients (about 99%) were included as the study participants. Out of 199 study participants, 45 (23%) were T2DM patients with DN (albumin positive) and 154 (77%) were T2DM patients without DN (albumin negative).
Patients with DN were significantly (p = 0.001) older than patients without DN (60.36 ± 10.30 vs. 53.85 ± 11.900 years) and had a significantly (p < 0.0001) longer duration of disease. Concerning the education status, T2DM patients with DN scored significantly lower education levels (p = 0.0001) than T2DM patients without DN. However, other demographic parameters, including marital status, occupation, gender, residence, and monthly income did not show a significant difference between the two groups (Table 1).
The comparison of sociodemographic characteristics between T2DM patients with DN and without DN.

The mean difference is significant at p < 0.01 (two-tailed).
The mean difference is significant at p < 0.001 (two-tailed).
Values are expressed as frequency and percentage.
Statistical analyses were performed by student’s t-test and chi-square test.
ETB: Ethiopian Birr; DN; diabetic nephropathy; n: sample size (indicated separately for each group of T2DM patients); T2DM: type 2 diabetes mellitus.
In this study, the mean values of TWBC, ANC, and NLR were significantly higher in T2DM patients with DN than in T2DM patients without DN. Similarly, the systolic blood pressure (SBP) and diastolic blood pressure (DBP) records were also significantly higher in T2DM patients with DN compared to T2DM patients without DN (p < 0.0001 for both SBP and DBP). However, the mean value of absolute lymphocyte count (ALC) was significantly lower in T2DM patients with DN than in T2DM patients without DN (Table 2).
The comparison of some clinical parameters between T2DM patients with DN and without DN.
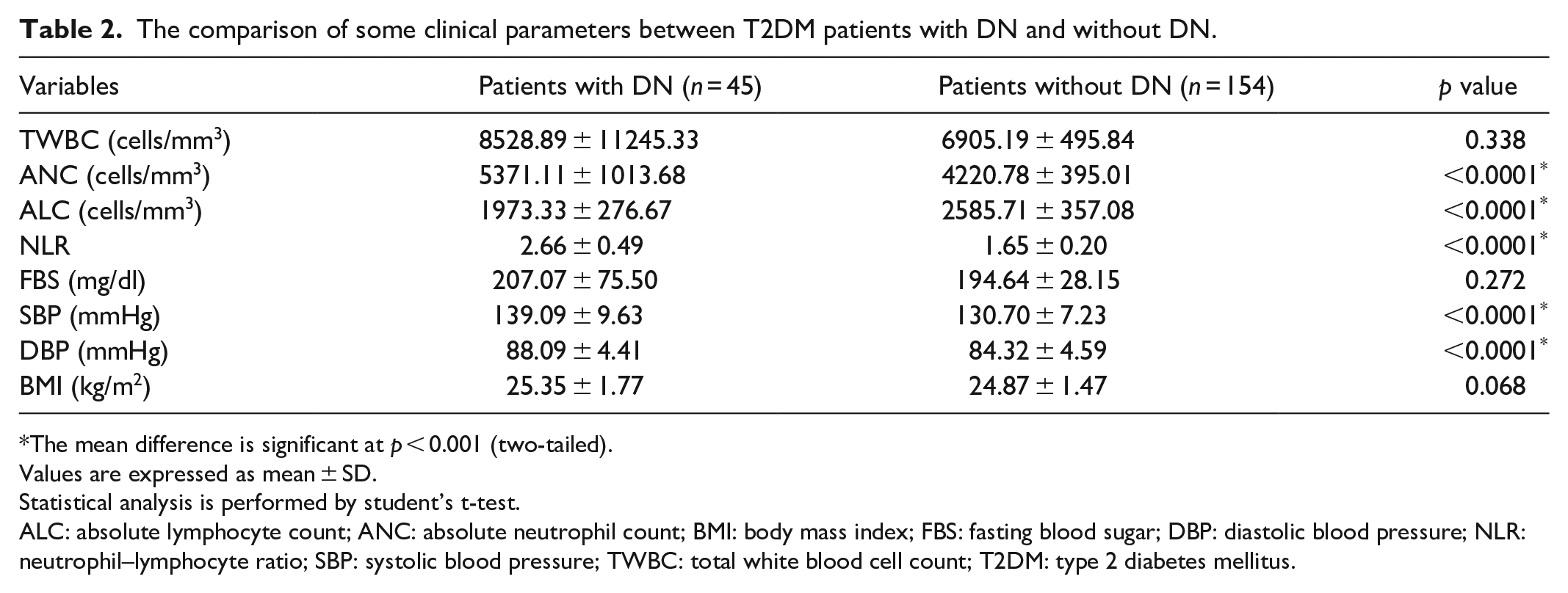
The mean difference is significant at p < 0.001 (two-tailed).
Values are expressed as mean ± SD.
Statistical analysis is performed by student’s t-test.
ALC: absolute lymphocyte count; ANC: absolute neutrophil count; BMI: body mass index; FBS: fasting blood sugar; DBP: diastolic blood pressure; NLR: neutrophil–lymphocyte ratio; SBP: systolic blood pressure; TWBC: total white blood cell count; T2DM: type 2 diabetes mellitus.
Correlation study between NLR and other study variables
Significant positive correlation was observed between NLR and each of the other variables such as age (r = 0.162, p = 0.023), duration of illness (r = 0.521, p < 0.001), SBP (r = 0.338, p < 0.001), DBP (r = 0.317, p < 0.001), total leucocyte (r = 0.162, p = 0.022), and ANC (r = 0.712, p < 0.001). On the other hand, NLR showed a significant negative correlation with ALC (r = −0.770, p < 0.001), (Table 3).
Correlation between NLR and other study variables of T2DM with DN and without DN.
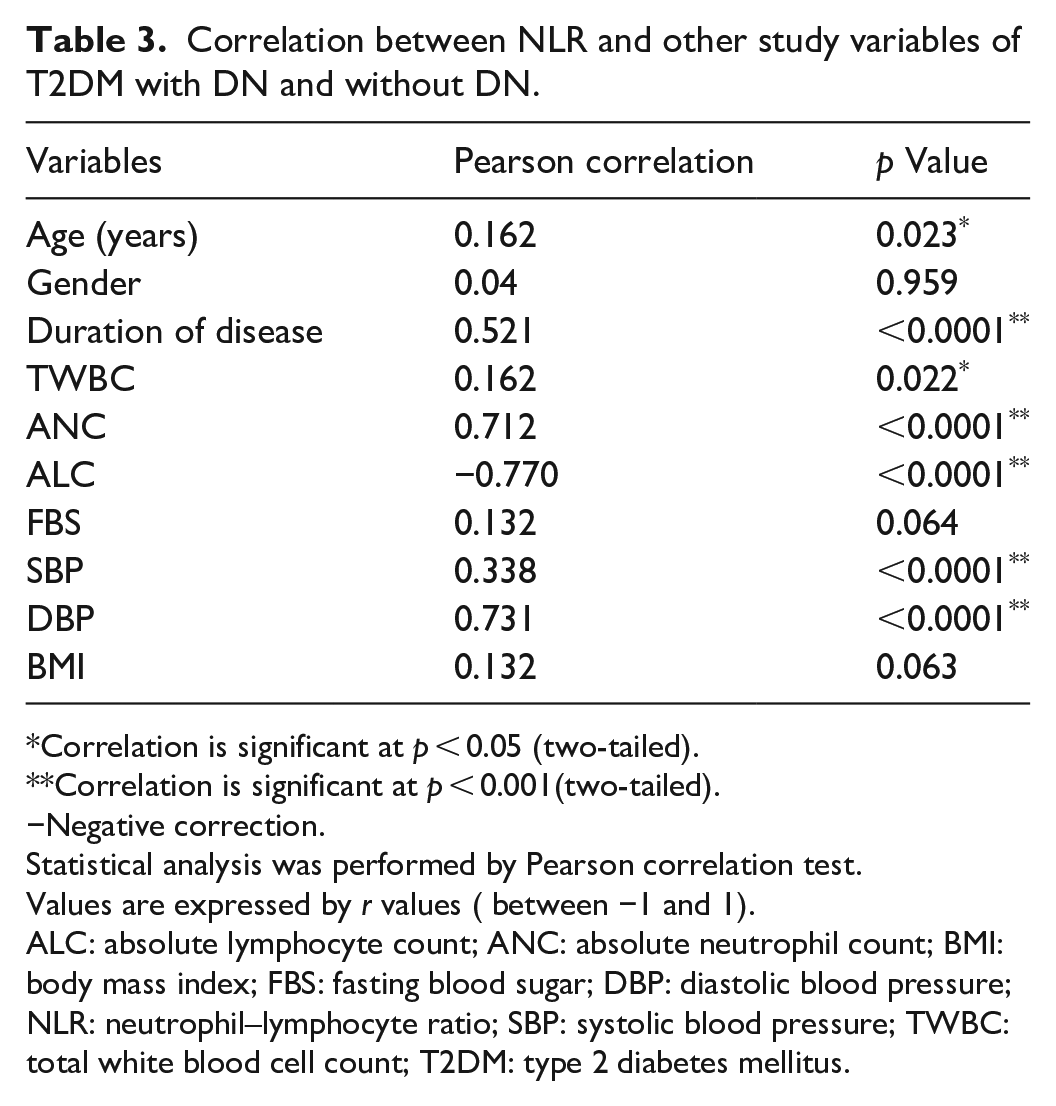
Correlation is significant at p < 0.05 (two-tailed).
Correlation is significant at p < 0.001(two-tailed).
−Negative correction.
Statistical analysis was performed by Pearson correlation test.
Values are expressed by r values ( between −1 and 1).
ALC: absolute lymphocyte count; ANC: absolute neutrophil count; BMI: body mass index; FBS: fasting blood sugar; DBP: diastolic blood pressure; NLR: neutrophil–lymphocyte ratio; SBP: systolic blood pressure; TWBC: total white blood cell count; T2DM: type 2 diabetes mellitus.
Discussion
Several studies that have described the association between inflammation and vascular disease showed that chronic inflammation can accelerate the development of micro and macrovascular complications in diabetic patients. Leucocyte count (especially, ANC and ALC) is one of the useful inflammatory biomarkers in clinical practice. In addition to leucocyte count, NLR is studied in many non-communicable diseases as an inflammatory marker and is used to predict the prognosis of diseases such as acute MI, stroke, heart failure, and DN.20,21 It is also a useful indicator of inflammatory process progress in various diseases, including appendicitis, cardiac diseases, and cancers. 2 This study is the first study conducted in Ethiopia to evaluate the NLR as an inflammatory biomarker of DN among T2DM patients.
In this study, the mean value of TWBC did not show any significant difference between T2DM patients with DN and T2DM patients without DN at (p = 0.338). This finding is in line with Elhadi et al. 22 However, it contradicts the study done by Gupta et al., which reported a statistically higher mean value of TWBC in T2DM patients with macroalbuminuria than in T2DM patients with normoalbuminuria and microalbuminuria. 23 This difference might be due to the difference in sample size used.
The mean value of ANC was significantly raised in T2DM patients with DN (5371.11 ± 1013.68) compared to T2DM patients without DN (4220.78 ± 395.01), (p < 0.0001). The finding of our study is in line with the studies done by Khandare et al., and Ünal et al.24,25 On the other hand, the mean value of ALC was significantly lower in T2DM patients with DN (1973.33 ± 276.67) than in T2DM patients without DN (2585.71 ± 357.08), (p < 0.0001).
The mean value of NLR in our study was also found to be significantly higher among diabetic patients with DN (2.66 ± 0.49) compared to those without DN (1.65 ± 0.20), (p < 0.0001). This result is similar to studies conducted by Zahorec and Khandare et al.13,24 A study done by Huang et al. has shown that NLR values of diabetic patients with DN (2.48 ± 0.59) were significantly higher than NLR values of diabetic patients without DN (2.20 ± 0.62) and healthy controls (1.80 ± 0.64). 26
The main factor involved in the development of DN is advanced glycation end (AGE) product activation, which causes oxidation of proteins and lipids that leads to tissue damage. Hence, in diabetic patients, the AGEs activate leucocytes that secrete different kinds of cytokines and transcription factors playing a crucial role in inflammation and thereby contributing to glomerulosclerosis. AGE products can also directly interact with various cellular components that trigger numerous intracellular signaling pathways; elicit abnormal immune responses and lead to cellular damage.27,28 A study done by Evans et al. also confirmed that hyperglycemia-induced oxidative stress has also a crucial role in the pathogenesis of DN. 29
Regarding correlation analysis, a significant positive correlation was found between NLR and each of the following variable: age (r = 0.162, p = 0.023), duration of the disease (r = 0.521, p < 0.001), SBP (r = 0.338, p < 0.001), DBP (r = 0.317, p < 0.001), TWBC (r = 0.162, p = 0.023), and ANC (r = 0.712, p < 0.001). Similar to this study, many researchers concluded that older age is a high-risk factor for developing DN. As age increases, the probability of developing kidney diseases will be high, and mostly reflected by proteinuria, because as age increases the immunity status of any individual will be reduced. 13
Our study findings are similar to other findings of different studies that reported, positive correction between NLR and age, WBC, ANC, duration of diseases, and blood pressure.30,31 A study conducted by Hintsa et al. reported that up to 35% of all patients with T2DM eventually develop nephropathy after 25–30 years of suffering from diabetes. 30 The DN is a chronic inflammatory disease that increases with age. As the age of diabetic patients increases by 1 year, the chance of developing DN increases by 3.7%, which means for 10 years increases in the duration of illness after diagnosis, the probability of developing diabetic microvascular complication increases by 1.43 times (43%). 32 On the other hand, NLR showed significant negative correlation with ALC (r = −0.770, p < 0.0001). 31
Furthermore, a study done by Azab et al. indicated that NLR can be used as a prognostic marker to assess the severity of renal function. 33 Similarly, Afşar has explained that NLR was related to DN and also associated with ESRD. 34 Another study has proved that NLR was correlated with DN in diabetic patients, which indicated there was a relationship between inflammation and endothelial dysfunction in DN. 35 There was no significant correlation between NLR and other variables such as sex, FBS level, and BMI among T2DM patients with and without DN. Similar to our result, Kahraman et al. reported the absence of a significant relationship between NLR and gender. 36 This study has the following limitations: (1) Biomarkers such as interleukin 1, 6, interferon gamma, and tumor necrosis factor alpha (due to unavailability of the tests) and HBA1c (budget constraints) were not measured. (2) The data regarding the type of treatments the patients were using were also not collected.
Conclusion
Overall, this study revealed that the NLR was significantly raised in T2DM patients with DN than in those without DN. It was found that NLR showed a significantly positive correlation with age, disease duration, blood pressure, and total leucocyte count, whereas it showed a significantly negative correlation with educational level. The study also indicated there was a significant positive correlation between NLR and DN implying that inflammation and endothelial dysfunction could be an integral part of the pathogenesis of DN. Therefore, NLR could be considered a potential predictor and a prognostic biomarker of DN among T2DM patients. Based on the finding of our study, we would like to recommend that NLR could be included in clinical practice for the diagnosis and prognosis of DN in Ethiopian health facilities. We also suggest that further investigations using a more appropriate study design and large sample size are needed to be conducted.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221140231 – Supplemental material for Neutrophil–lymphocyte ratio as an inflammatory biomarker of diabetic nephropathy among type 2 diabetes mellitus patients: A comparative cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221140231 for Neutrophil–lymphocyte ratio as an inflammatory biomarker of diabetic nephropathy among type 2 diabetes mellitus patients: A comparative cross-sectional study by Mesfin Zewude Gurmu, Solomon Genet, Solomon Tebeje Gizaw, Teka Obsa Feyisa and Netasan Gnanasekaran in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our earnest gratitude to Arsi University and Addis Ababa University for funding this research project. We are extremely grateful to the Department of Medical Biochemistry, Addis Ababa University, for its indispensable support and coordination in the smooth running of this project. Our sincere appreciation also goes to Bole 17 Health Center staff and our study participants for their positive cooperation during this study.
Disclosure
The authors disclose that this article is prepared from an original thesis by Mesfin Zewude (the first Author), which is entitled, “Assessment of Neutrophil–lymphocyte Ratio as an Inflammatory Marker among type 2 Diabetes Mellitus patients with and without Diabetic Nephropathy.” The authors also declare that the article has not been published or is not under consideration for publication anywhere; however, available online at ![]() (AAU Institutional Repository).
(AAU Institutional Repository).
Authors’ contributions
MZG conceived and designed the study, collected, analyzed, and interpreted the data, and wrote the article. SG, ST, and NS designed the study and interpreted the data, and TOF assisted in study designing, data analysis, interpretation, and writing the article. All the authors have read, commented on, and contributed to the final version of the article.
Availability of data and materials
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the Department of Research and Ethics Review Committee, Department of Medical Biochemistry, College of Health Sciences, Addis Ababa University (Ref. No. SOM/BCHM/152/2011, Protocol No. MSc. 07/19).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Arsi University and Addis Ababa University. The funders had no role in designing the study, collection, analysis, and interpretation of data as well as in the writing of the article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.