
Abstract
Objective:
To investigate the association between admission plasma glucose and cardiovascular events in patients with acute myocardial infarction treated with modern therapies including early percutaneous coronary intervention and modern stents.
Methods:
Patients (n = 5309) with established diabetes and patients without previously known diabetes with a reported admission plasma glucose, included in the VALIDATE trial 2014-2016, were followed for cardiovascular events (first of mortality, myocardial infarction, stroke, heart failure) within 180 days. Event rates were analysed by four glucose categories according to the World Health Organization criteria for hyperglycaemia and definition of diabetes. Odds ratios were calculated in a multivariate logistic regression model.
Results:
Mean age was 67 ± 11 years. Previously known diabetes was present in 21.2% (n = 1124). Cardiovascular events occurred in 3.7%, 3.8%, 6.6% and 15.7% in the four glucose level groups and 9.9% in those with known diabetes (p < 0.001), while bleeding complications did not differ significantly (9.1%, 8.5%, 8.4%, 12.2% and 8.5%, respectively). After adjustment, odds ratio (95% confidence interval) was 1.00 (0.65–1.53) for group II, 1.62 (1.14–2.29) for group III and 3.59 (1.99–6.50) for group IV compared to the lowest admission plasma glucose group (group I). The corresponding number for known diabetes was 2.42 (1.71–3.42).
Conclusion:
In a well-treated contemporary population of acute myocardial infarction patients, 42% of those without diabetes had elevated admission plasma glucose levels with a greater risk for clinical events already within 180 days. Event rate increased with increasing admission plasma glucose levels. These findings highlight the importance of searching for undetected diabetes in the setting of acute myocardial infarction and that new treatment options are needed to improve outcome.
Diabetes is associated with an adverse prognosis after acute coronary syndrome (ACS) with high rates of myocardial infarction (MI), heart failure (HF), stroke and mortality 1 despite improvements in preventive and coronary care over the last 20 years. A large proportion of those with MI have undiagnosed diabetes or prediabetes which severely impact outcomes. However, screening for glucose disturbances in the coronary care unit (CCU) is seldom routine and hampered by shorter hospitalisation times for MI. 2 Since new glucose-lowering agents have shown impressive cardiovascular protective effects in patients with diabetes and established cardiovascular disease, updated information on the prognostic impact of admission plasma glucose (APG), besides the previously demonstrated association with APG on mortality, 3 is warranted. Such new knowledge could further increase mandate and support the rationale to screen for undiagnosed glucose disturbances associated with adverse prognosis after ACS.
We included 5309 patients with ST-segment elevation myocardial infarction (STEMI) or non-ST-segment elevation myocardial infarction (NSTEMI) between 2014 and 2016 and with recorded APG in the registry-based randomised VALIDATE-SWEDEHEART trial where patients were randomised to bivalirudin or heparin during percutaneous coronary intervention (PCI) at 25 participating PCI centres. The trial reported neutral effects on the primary endpoint, a composite of bleeding, MI or death during 6 months of follow-up with no interaction in those with or without diabetes (p-value for interaction = 0.82). 4 Information on comorbidities and diabetes was extracted from the comprehensive national registry for heart disease, SWEDEHEART. Known diabetes was defined as reported diabetes and/or diabetes treatment at discharge. Patients without diabetes were classified by APG into four categories according to the World Health Organization (WHO) criteria for hyperglycaemia and definition of diabetes. 5 Patients were followed for MI, stroke, hospitalisation for HF and all-cause death until 6 months or death with a complete follow-up in 99% of the patients. Logistic regression analyses were performed to calculate associated odds ratios (OR) and 95% confidence limits (CLs) before and after adjusting for important clinical variables as age, gender, previous MI and indication for PCI (STEMI or NSTEMI).
Mean age was 67 ± 11 years and 73% were men. Known diabetes was present in 1124 patients (21.2%). Among those without established diabetes, the number and proportion in different glucose categories were as follows: group I [APG < 6.1 mmol/L (<110 mg/dL)]: n = 1406 (33.6%); group II [6.1–6.9 mmol/L (110–125 mg/dL)]: n = 1048 (25.0%); group III [7.0–11.0 mmol/L (126–198 mg/dL)]: n = 1616 (38.6%) and group IV [>11.0 mmol/L (>198 mg/dL)]: n = 115 (2.8%). The proportion of the clinical composite outcome in each glucose group was 3.7%, 3.8%, 6.6% and 15.7%, respectively, and 9.9% for known diabetes. Figure 1 depicts the proportion of outcomes and adjusted OR. The event rate increased with increasing APG with the highest proportion seen in individuals without known diabetes but with APG > 11 mmol/L (198 mg/dL) followed by subjects with established diabetes. After adjustments, patients with elevated APG > 7.0 mmol/L (126 mg/dL) and with no previous reported diabetes (group III) were associated with increased event rate, while patients without diabetes and APG < 7.0 mmol/L (126 mg/dL) had similar event rates as those with normal glucose levels. Limitations with the present study are the lack of HbA1c and information if APG were fasting or influenced by recent glucose intake.
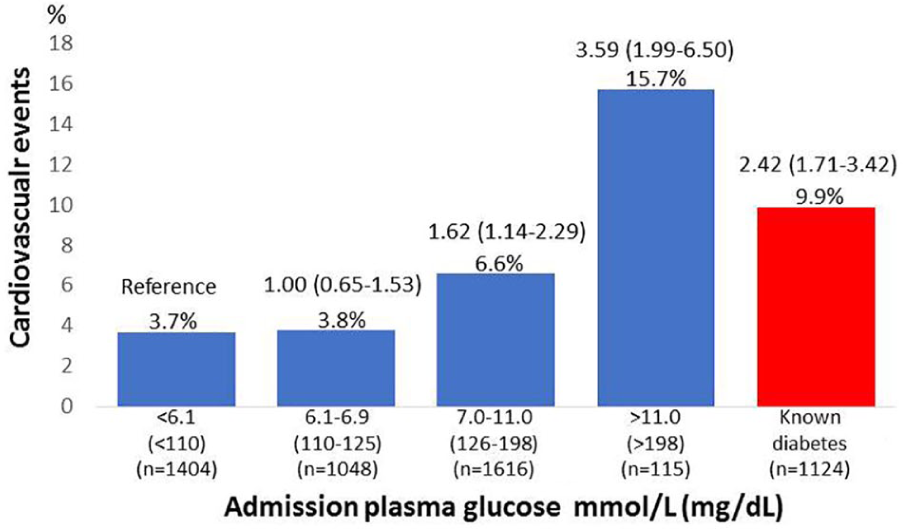
Proportion of cardiovascular events (myocardial infarction, heart failure, stroke, all-cause death) at 180 days and odds ratios (95% confidence limits) in known diabetes (red) or by admission plasma glucose (blue).
Our findings from this large randomised cohort indicate that not only patients with established diabetes but also those without diabetes with elevated APG > 7.0 mmol/L (126 mg/dL), present in 42% of the patients, are at an increased risk for MI, HF, stroke and mortality in the following 6 months. Our findings indicate a need to initiate protective treatment already before discharge from the CCU. Future studies should address if novel cardiovascular preventive glucose-lowering drugs are safe and effective to institute as early as during intensive coronary care.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: V.R. has received honoraria from AstraZeneca, Novo Nordisk and Boehringer Ingelheim on expert group participation. S.K. has received honoraria from AstraZeneca, BMS and Pfizer. O.F. has received honoraria from AstraZeneca and GE Medical. D.E. has received honoraria from AstraZeneca and the Medicines Company. S.J. has received grants from AstraZeneca, the Medicines Company, the Swedish Heart and Lung Foundation and the Swedish Research Council. A.N. has received honoraria on expert group participation from AstraZeneca, Merck Sharp & Dohme, Eli Lilly and Company, Novo Nordisk and Boehringer Ingelheim. B.L., E.O., D.O. and J.J. report no potential conflicts of interest relevant to this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Swedish Heart and Lung Foundation, Department of Research and Development Region Kronoberg, the Kamprad Family Foundation, the Swedish Research Council, AstraZeneca, the Medicines Company and the Swedish Foundation for Strategic Research.