
Abstract
To evaluate the influence of type 2 diabetes mellitus on the long-term outcomes of Chinese patients with previous myocardial infarction, we studied 864 patients with previous myocardial infarction, including 251 with type 2 diabetes mellitus and 613 without type 2 diabetes mellitus, over a median follow-up time of 2.9 years. The type 2 diabetes mellitus patients were subdivided into 95 insulin-treated diabetes mellitus and 156 non-insulin-treated diabetes mellitus subjects. The crude incidences (per 1000 patient-years) in the type 2 diabetes mellitus subjects versus the non-type 2 diabetes mellitus subjects were 43.7 versus 25.1 for recurrent myocardial infarction, 68.7 versus 28.3 for all-cause death and 99.8 versus 49.9 for the composite end point (i.e. recurrent myocardial infarction or all-cause death). Cox regression analysis showed that the adjusted hazard ratios for recurrent myocardial infarction, all-cause death and their combination were 1.67 (95% confidence interval: 1.06–2.74), 1.90 (1.25–2.90) and 1.72 (1.23–2.40), respectively. Significant associations were also observed between insulin treatment and all-cause death. Our findings suggested that type 2 diabetes mellitus is an independent risk factor for recurrent myocardial infarction, all-cause death and the composite end point among previous myocardial infarction patients.
Introduction
Myocardial infarction (MI) is a major cause of death and disability worldwide, and the recurrent rate of MI remains relatively high, accompanied by an increased risk of complications and death.1,2 Diabetes is a major risk factor for coronary artery disease (CAD), and CAD is the most common cause of death among people with diabetes.3,4 Repeated CAD events with higher mortality is a well-known feature of the progression of type 2 diabetes mellitus (T2DM).5,6 A few reports have been published on the incidence of repeated CAD events or the outcomes of T2DM patients,7–9 but these studies have usually represented only certain populations, and might be not suitable for general global population. In China, with the rapid economic development, the population of patients with T2DM and/or MI has risen dramatically.10,11 However, due to racial differences (genetic factors, lifestyle and environmental circumstances), little is known about the impact of T2DM on Chinese people, particularly those surviving previous myocardial infarction (Pre-MI). Furthermore, patients with T2DM undergoing insulin treatment often have inadequate glycaemic control, and these patients are at increased cardiovascular risk compared with nonusers of insulin.12,13 Currently, only limited information is available about the clinical outcomes of Pre-MI patients undergoing insulin treatment. Our retrospective study enrolled Chinese Pre-MI patients as the study population to assess the influence of T2DM and insulin treatment on the incidences of recurrent myocardial infarction (Re-MI) and mortality.
Patients and methods
Study population
At Zhengzhou University People’s Hospital and the First Affiliated Hospital of Zhengzhou University, a total of 948 consecutive patients with acute myocardial infarction (AMI) were registered from June 2008 to May 2010. All of the patients had their medical reports reviewed during their hospitalisation. At the same time, they were divided into two groups, both of which were followed up by two independent investigators. Participants or family members lacking responses during telephone follow-up were excluded. When we contacted the patients or their families, we informed them about our studies (written information or oral information, if needed) and asked whether they would like to participate. Patients who did not provide informed consent were excluded. An experienced physician blinded to patients’ personal information, such as their names and telephone numbers, reviewed the medical records. Complete data were available for 897 patients (94.6%), and 33 patients (3.5%) were lost or excluded during follow-up; finally, 864 patients (91.1%) were enrolled in our study. For the release of such information, ethics approval was obtained from the Health Ethics Research Association of Zhengzhou University.
According to the diagnosis of T2DM before admission or within 28 days after admission, the eligible subjects were classified into non-T2DM and T2DM groups, and the T2DM subjects were subdivided into insulin-treated diabetes mellitus (ITDM) and non-insulin-treated diabetes mellitus (NITDM) subjects according to hypoglycaemic treatment on admission. During the enrolment and follow-up visits, a standard questionnaire was used to collect information on lifestyle and habits, drug therapy, clinical history and cardiovascular complications. Data on the patients’ characteristics were carefully collected and recorded.
We defined current smokers as individuals who smoked any tobacco product during the previous 12 months, as well as those who had quit within the previous year. Former smokers were defined as those who had quit more than 1 year earlier. Regular alcohol use was defined as consumption three or more times per week.
Diagnosis of MI and type 2 diabetes mellitus
A diagnosis of AMI was made if the patients fulfilled at least two of the following three criteria: (1) history of chest pain or tightness lasting ≥20 min, (2) typical electrocardiogram (ECG) changes (ST-segment elevation ≥0.1 mV in one standard limb lead or two continuous precordial leads; ST-segment depression ≥0.1 mV in two leads, abnormal Q waves, or T-wave inversion in two leads) and (3) elevation of cardiac biochemical markers [preferably cardiac troponin (I, T) exceeding the upper reference limit].
T2DM was diagnosed by the centres’ physicians. Non-T2DM patients were placed in the diabetic group, if they were diagnosed with T2DM within 28 days after admission, or they were excluded if they were diagnosed with T2DM after 28 days. T2DM was confirmed if any of the following criteria were met: (1) one or more classic symptoms (excessive thirst, polyuria, unexplained weight loss, hunger) plus a fasting plasma glucose level of >7.8 mmol/L or a random plasma glucose level of >11.1 mmol/L, (2) at least two elevated plasma glucose concentrations on different occasions (a fasting level of >7.8 mmol/L or a random level of >11.1 mmol/L and/or a concentration of >11.1 mmol/L after 2 h of oral glucose tolerance testing) in the absence of symptoms or (3) treatment with hypoglycaemic medications (insulin, oral hypoglycaemic agents or both).
Follow-up and definition of endpoints
Over a median follow-up time of 2.9 years, all of the patients were followed up until the censoring date of 31 May 2012. The primary outcome was defined as Re-MI. Re-MI was diagnosed as the first occurrence of MI at least 72 h after the first MI. MI caused by percutaneous coronary intervention (PCI) procedures was not defined as Re-MI. The secondary outcomes were all-cause death and a composite outcome of all-cause death or Re-MI. Death was documented according to all available information, such as responses to follow-up questionnaires by family members, death certificates or medical records.
Statistical analysis
Data analysis was performed with the SPSS computer program for Windows (Chicago, IL, USA). The results for continuous and categorical variables are, respectively, shown as mean ± standard deviation (SD) and as percentages. Differences in baseline characteristics were accessed by the χ2 test for categorical variables and the t test for continuous variables. We analysed the incidence rates of MI and death over the follow-up period, expressed in events/1000 person-years. To determine whether T2DM and insulin treatment were independent predictors of Re-MI and all-cause death, Cox proportional hazards ratio models were used to control for potential confounding variables. Statistical significance was defined as a p value < 0.05.
Results
Baseline characteristics and treatment of patients with Pre-MI
Overall, the study included 251 (29.1%) T2DM and 613 (70.9%) non-T2DM patients; there were 30 (12.0%) T2DM patients with non-ST-elevation infarction and 92 (15.0%) of such patients among non-T2DM patients. The baseline characteristics and treatment of all of the patients are shown in Table 1. Compared with non-T2DM, T2DM patients were slightly older (median 65.74 vs 63.96 years old). T2DM patients had more frequent histories of dyslipidaemia, hypertension, stroke and peripheral vascular diseases and more often presented with significant higher values of body mass index (BMI) and creatinine, but they tended to smoke less. In addition, the left ventricular ejection fraction (LVEF) values among T2DM patients were slightly lower compared with non-T2DM patients, but the difference did not attain statistical significance.
Patients’ characteristics and treatments of T2DM and non-T2DM population.
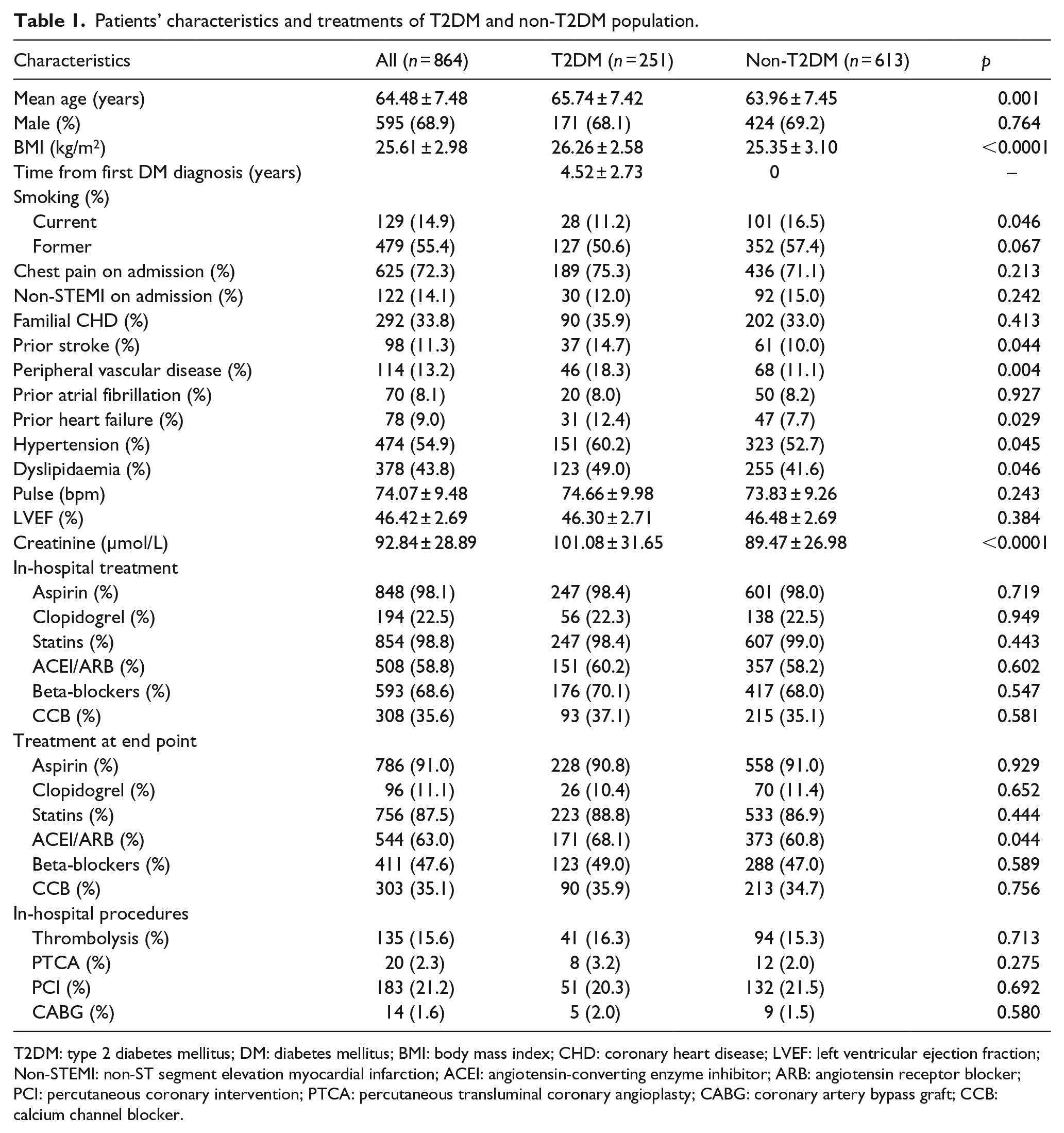
T2DM: type 2 diabetes mellitus; DM: diabetes mellitus; BMI: body mass index; CHD: coronary heart disease; LVEF: left ventricular ejection fraction; Non-STEMI: non-ST segment elevation myocardial infarction; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; PCI: percutaneous coronary intervention; PTCA: percutaneous transluminal coronary angioplasty; CABG: coronary artery bypass graft; CCB: calcium channel blocker.
As shown, use of standard treatment for MI was widespread during hospitalisation. Approximately 60% of the patients were treated with angiotensin-converting enzyme inhibitor (ACEI)/angiotensin receptor blocker (ARB) and 70% were treated with beta-blockers, as recorded during hospitalisation, and both rates were lower than the results reported in studies from Western countries. At the end of this study, 47.6% of the patients were treated with beta-blockers, 91% with aspirin, 87.5% with statins and 11.1% with clopidogrel, with no significant differences between the two groups. However, a significant difference was observed in the use of ACEI/ARB at the end of the study, with usages rates of 68.1% versus 60.8% among T2DM and non-T2DM patients, respectively.
We only had information about revascularisation procedure during hospitalisation, and non-significant differences were observed. The rates of in-hospital thrombolysis, percutaneous transluminal coronary angioplasty (PTCA) and coronary artery bypass graft (CABG) were slightly higher among T2DM patients, while PCI, the predominant revascularisation procedure in both groups, was performed in 20.3% of T2DM patients and 21.5% of non-T2DM patients (Table 1).
T2DM and long-term outcomes
In the primary analysis, there were 31 and 45 Re-MIs in the T2DM and non-T2DM groups, respectively, while the average time-to-reinfarction was 1.6 versus 1.5 years, with crude incidence rates of 43.7 versus 25.1 events per 1000 person-years [risk ratio (RR): 1.74; 95% confidence interval (CI): 1.01–2.75; p = 0.042]. Re-MI-free survival curves are shown in Figure 1. In the secondary analysis, T2DM patients had a crude incidence rate of 68.7 events per 1000 person-years for all-cause death, which was 1.43-fold higher than that of non-T2DM patients (28.3 events per 1000 person-years; RR: 2.43; 95% CI: 1.64–3.60; p < 0.0001), and survival curves are shown in Figure 2(b). Moreover, the crude incidence rates of the composite end point for T2DM and non-T2DM were, respectively, 99.8 versus 49.9 events per 1000 person-years (RR: 2.0; 95% CI: 1.46–2.76; p < 0.0001) (Table 2).
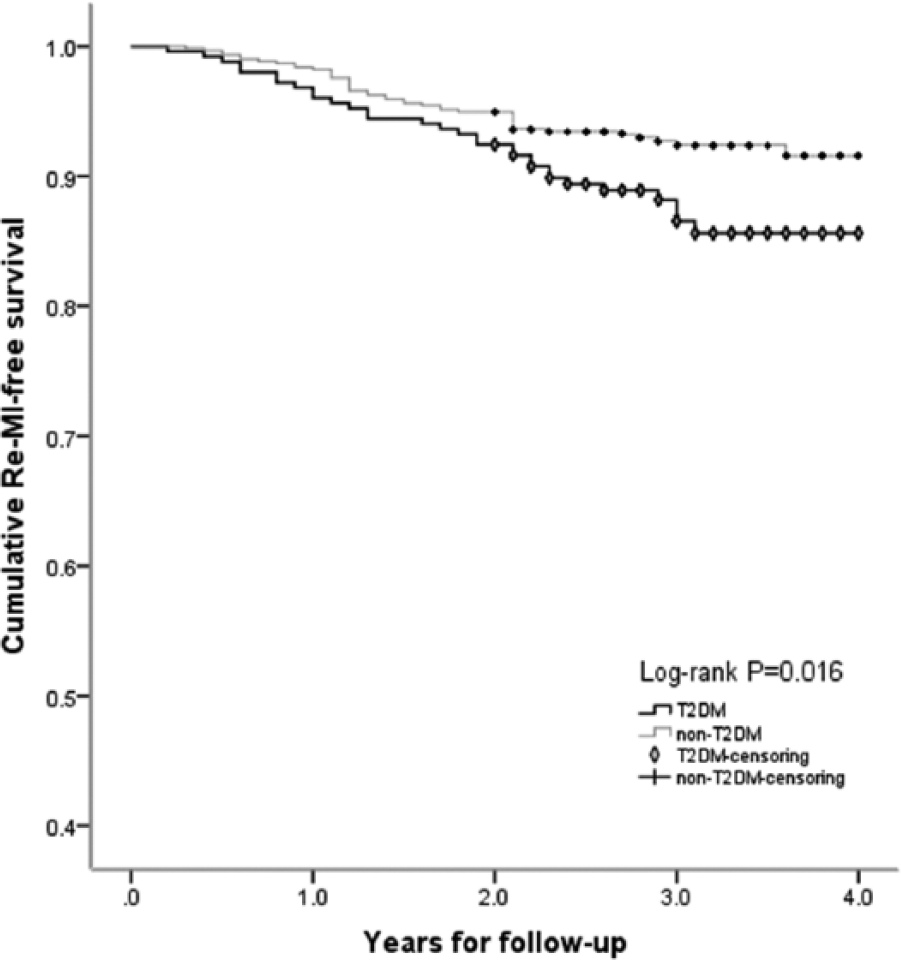
Cumulative Re-MI-free survival curves between T2DM and non-T2DM subjects. (Censoring means patients survive without Re-MI until end of follow-up.)
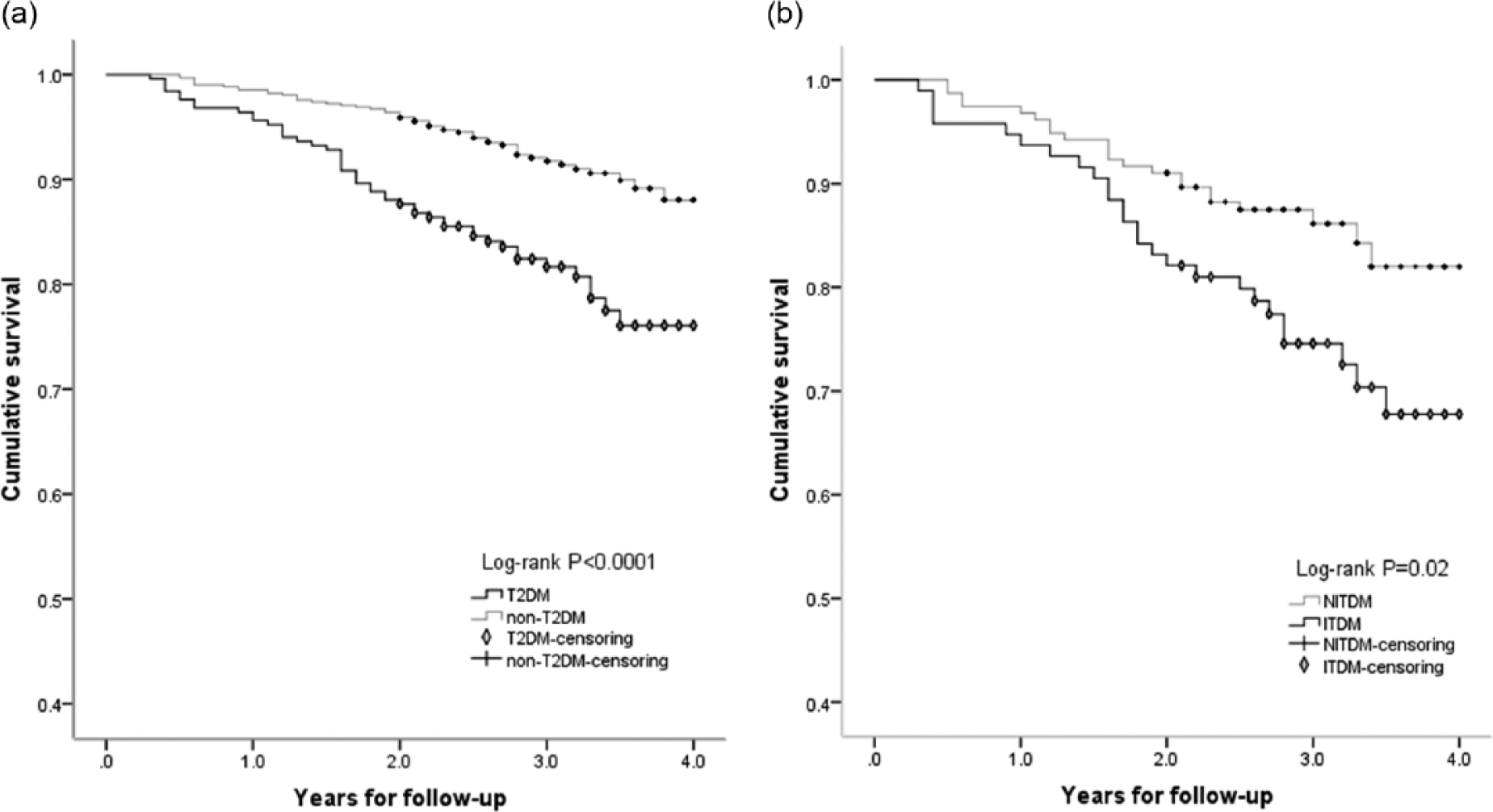
Cumulative survival curves (all-cause death) (a) between T2DM and non-T2DM patients and (b) between ITDM and NITDM patients. (Censoring means patients survive until end of follow-up.)
Crude incidence rates and rate ratio of primary outcome (Re-MI) and secondary outcomes (all-cause death and the composite end point of all-cause death and Re-MI) in T2DM and non-T2DM patients (rates are shown as events per 1000 person-years and 95% CI).
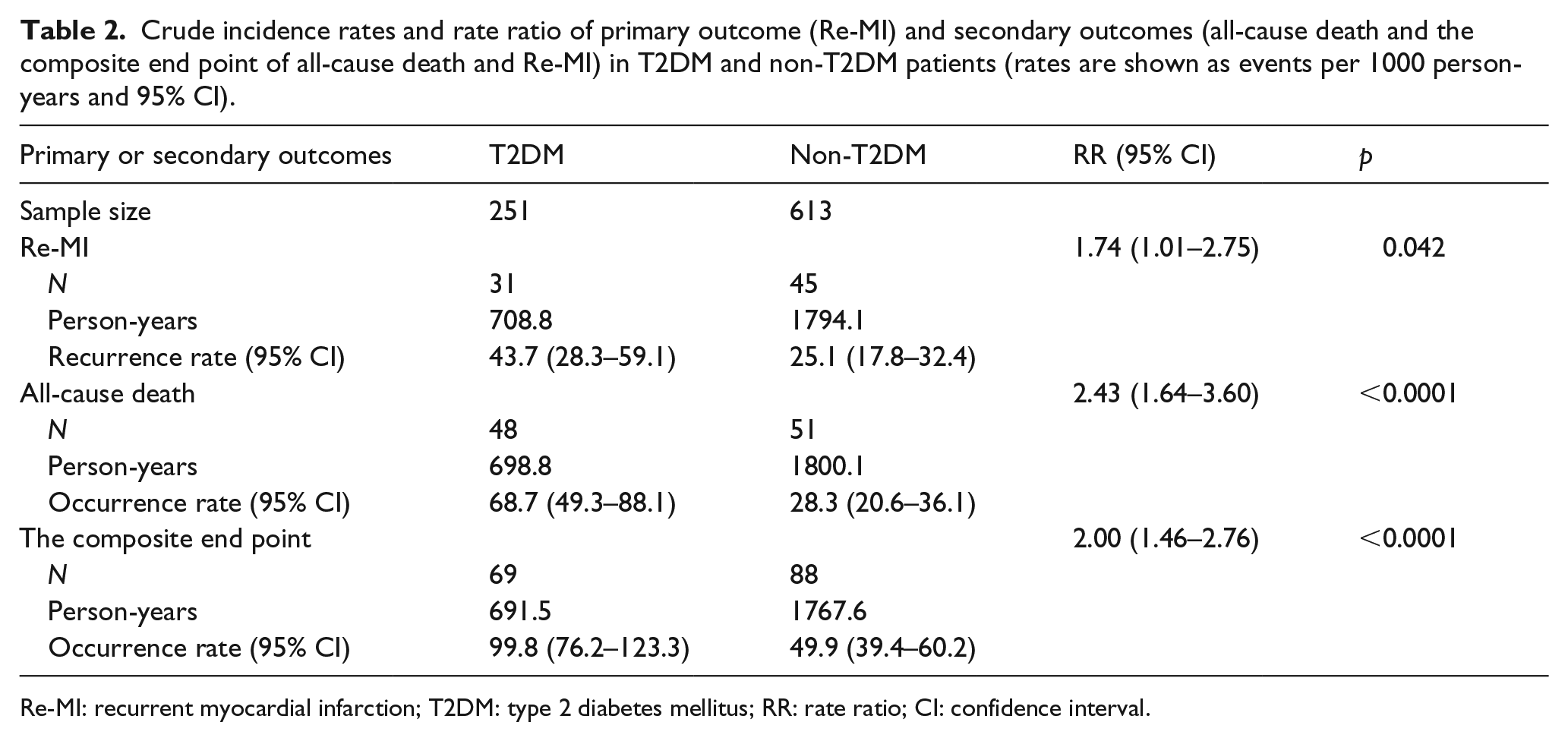
Re-MI: recurrent myocardial infarction; T2DM: type 2 diabetes mellitus; RR: rate ratio; CI: confidence interval.
After correction for baseline confounding factors (age, dyslipidaemia, hypertension, current smoking, BMI, creatinine, prior stroke, ACEI at end point, peripheral vascular disease, prior heart failure, T2DM), multivariate Cox regression analysis revealed that T2DM was an independent predictor of Re-MI [adjusted hazard ratio (HR): 1.67; 95% CI: 1.03–2.74; p = 0.039], all-cause death (adjusted HR: 1.90; 95% CI: 1.25–2.90; p = 0.0003) and the composite end point (adjusted HR: 1.72; 95% CI: 1.23–2.40; p = 0.002). Among all of the baseline characteristics, predictive factors of primary and secondary outcomes in the T2DM and non-T2DM population are shown in Table 3.
Predictive factors of primary and secondary outcomes in the T2DM and non-T2DM population: results from multivariate analysis.
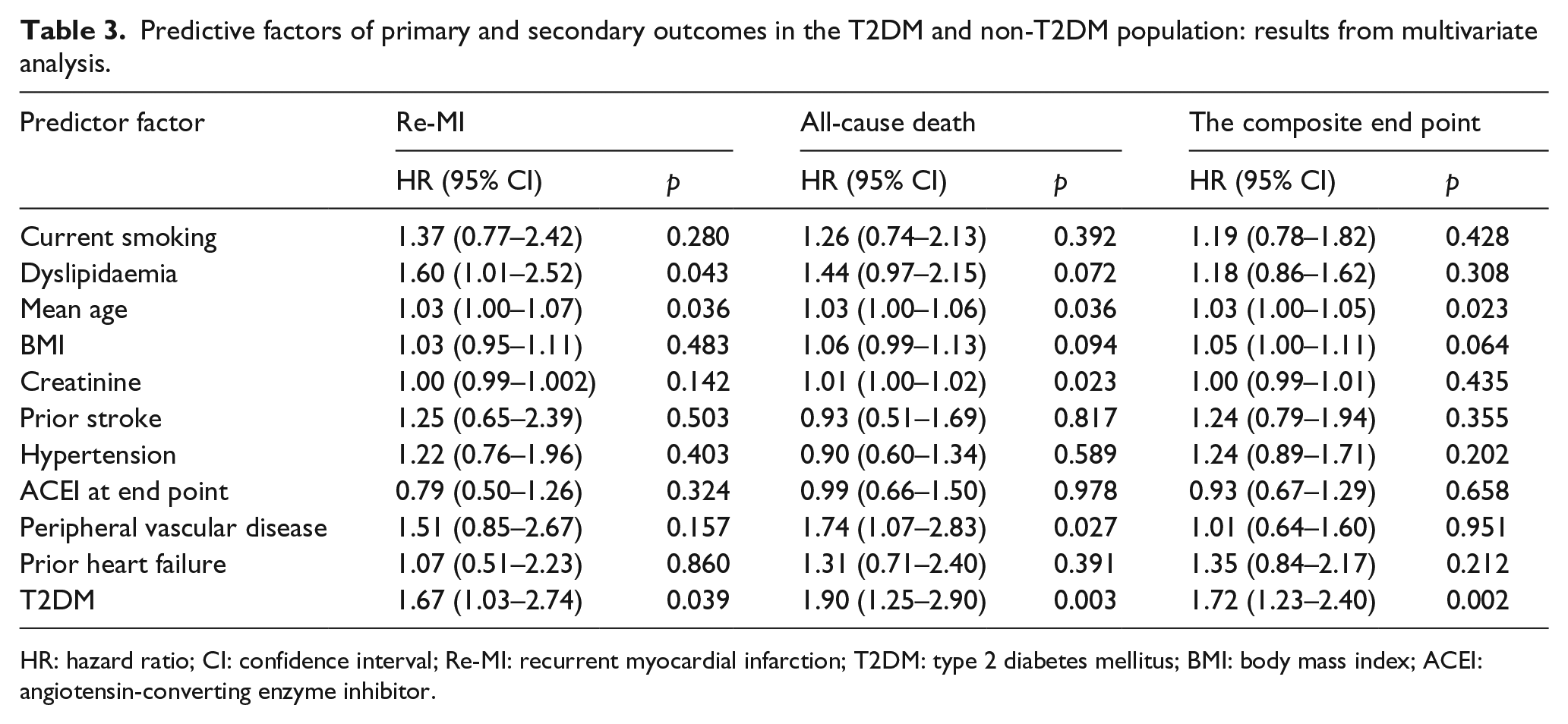
HR: hazard ratio; CI: confidence interval; Re-MI: recurrent myocardial infarction; T2DM: type 2 diabetes mellitus; BMI: body mass index; ACEI: angiotensin-converting enzyme inhibitor.
Subgroup analyses of T2DM patients
The baseline characteristics and treatments of ITDM and NITDM patients are shown in Table 4, the crude incidence rates of the long-term outcomes appear in Table 5 and multivariate Cox regression analysis appears in Table 6. There were a total of 95 patients (37.9%) treated with insulin to control their blood glucose. The proportions of non-ST-elevation infarction were, respectively, 11.6% versus 12.2% in the ITDM and NITDM groups. Newly detected T2DM, which was defined as diagnosis on admission or during the 28 days after admission, represented 23.4% and 24.0% of the ITDM and NITDM patients, respectively. ITDM patients were younger than NITDM patients and more often female. They had a higher prevalence of dyslipidaemia and higher BMI values, but their LVEF values were lower. The incidence rates of Re-MI were not significantly different (RR: 1.34; 95% CI: 0.66–2.72; p = 0.478) between the two groups, but there were higher rates of all-cause death (RR: 1.95; 95% CI: 1.11–3.44; p = 0.028) and the composite end point (RR: 1.85; 95% CI: 1.15–2.97; p < 0.0001) among ITDM patients. The survival curves are shown in Figure 2(b). When the Cox proportional hazards ratio models were fitted into the secondary outcomes, significant influences of insulin treatment on all-cause death and the composite end point were identified (respectively, for all-cause death, HR: 2.05; 95% CI: 1.04–4.03; p = 0.039; for composite end point, HR: 1.96; 95% CI: 1.09–3.53; p = 0.025) (Table 6).
Patients’ characteristics and treatments of ITDM and NITDM patients.
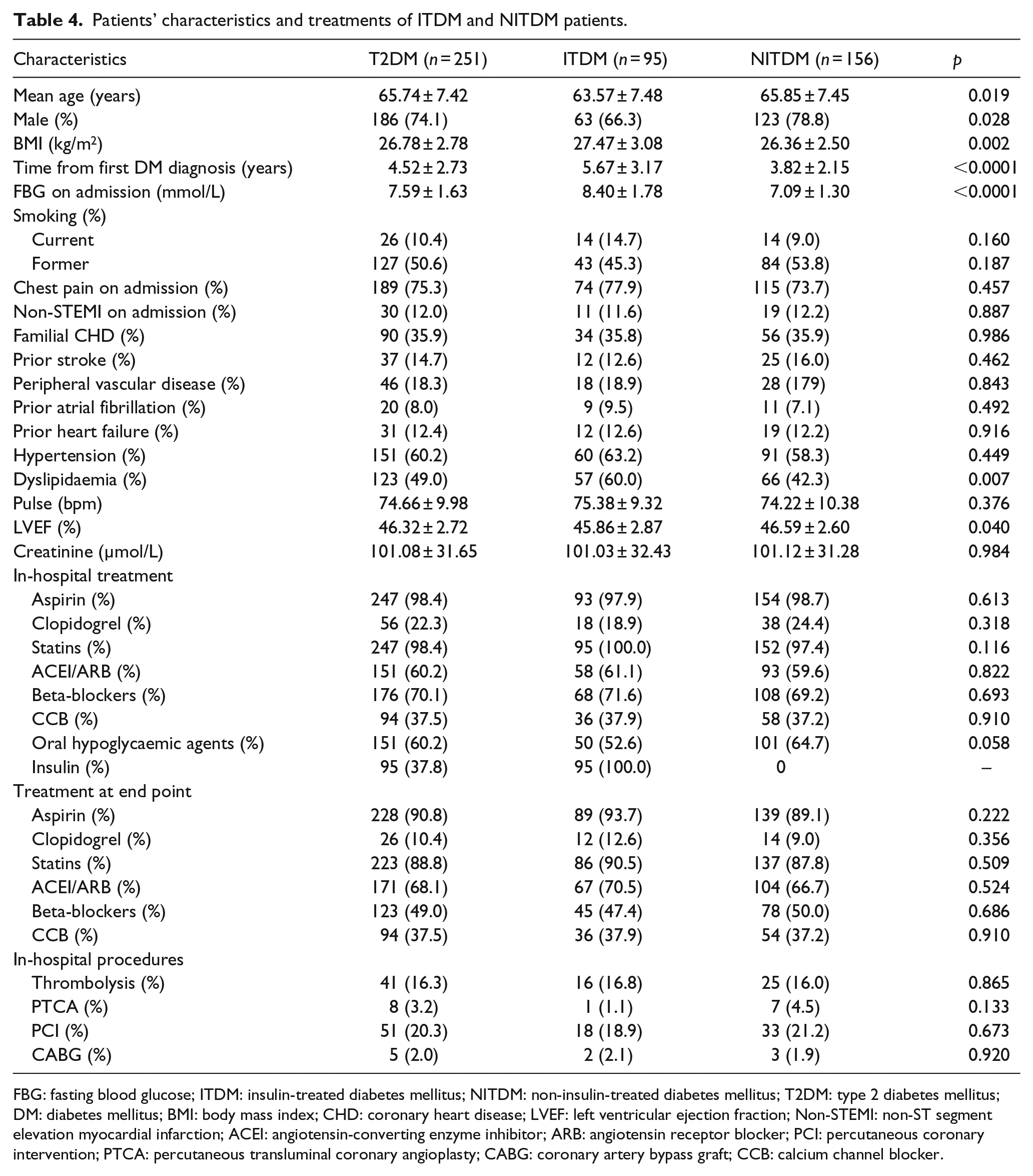
FBG: fasting blood glucose; ITDM: insulin-treated diabetes mellitus; NITDM: non-insulin-treated diabetes mellitus; T2DM: type 2 diabetes mellitus; DM: diabetes mellitus; BMI: body mass index; CHD: coronary heart disease; LVEF: left ventricular ejection fraction; Non-STEMI: non-ST segment elevation myocardial infarction; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; PCI: percutaneous coronary intervention; PTCA: percutaneous transluminal coronary angioplasty; CABG: coronary artery bypass graft; CCB: calcium channel blocker.
Crude incidence rates and rate ratio of primary and secondary outcomes among ITDM and NITDM patients (rates are given as number of events per 1000 person-years and 95% CI).
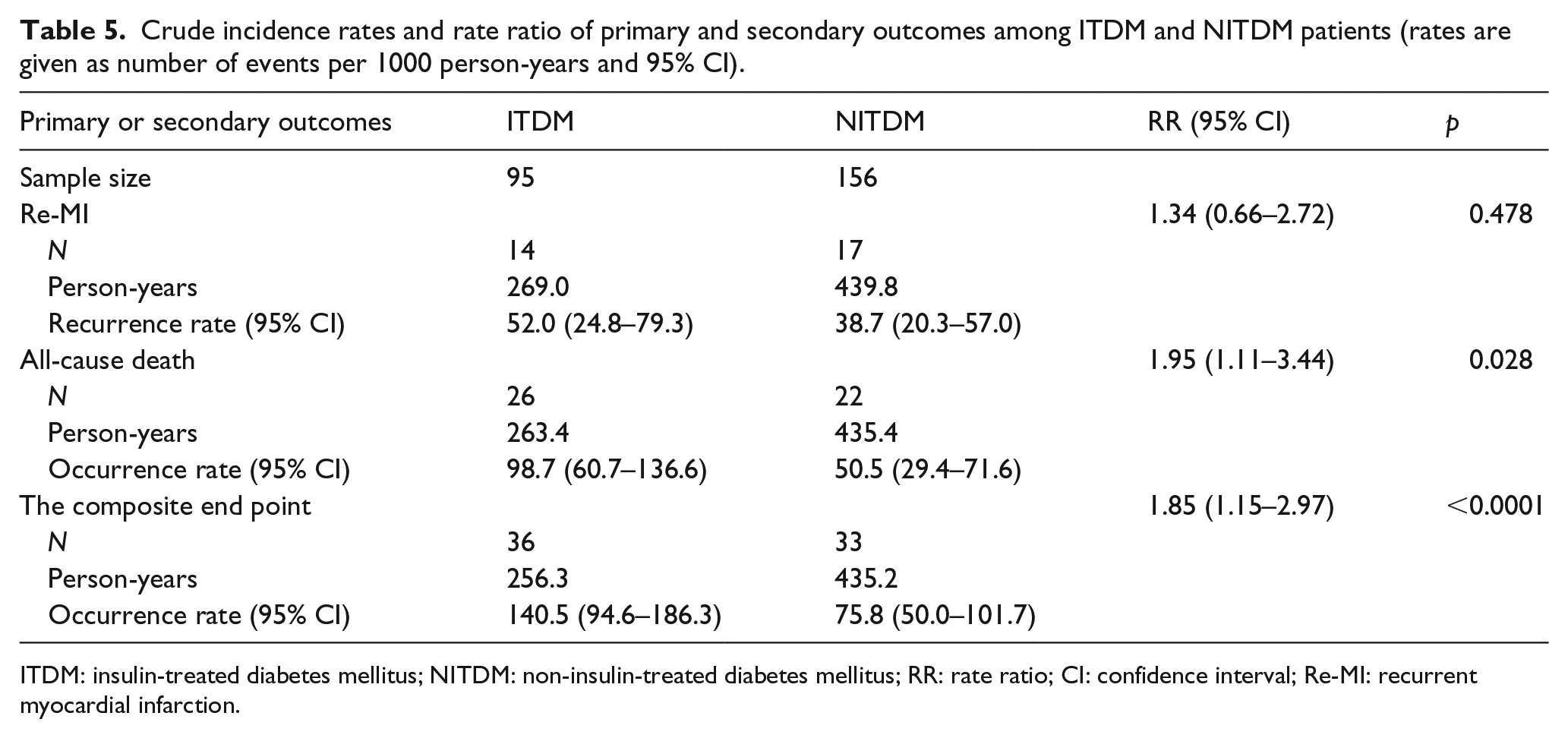
ITDM: insulin-treated diabetes mellitus; NITDM: non-insulin-treated diabetes mellitus; RR: rate ratio; CI: confidence interval; Re-MI: recurrent myocardial infarction.
Predictive factors of primary and secondary outcomes in T2DM population: results from multivariate analysis.
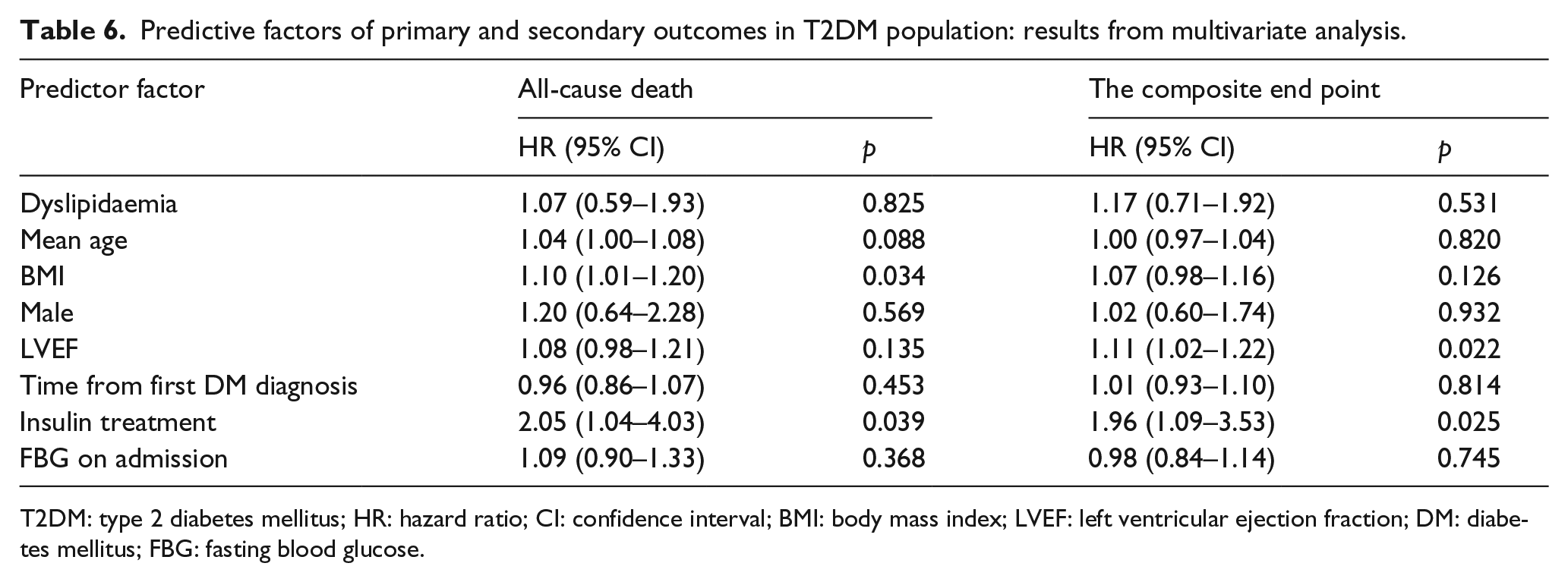
T2DM: type 2 diabetes mellitus; HR: hazard ratio; CI: confidence interval; BMI: body mass index; LVEF: left ventricular ejection fraction; DM: diabetes mellitus; FBG: fasting blood glucose.
Discussion
To the best of our knowledge, this was the first study aiming to describe the associations between T2DM and the risks of Re-MI and all-cause death among Chinese people. This retrospective study confirmed that, in Pre-MI patients, T2DM was a significant and independent predictor of Re-MI, all-cause death and the composite end point; when stratified for diabetic status reflected by insulin use, insulin treatment was also an independent predictor of all-cause death and the composite end point, but not of Re-MI.
Fast economic development in China has improved most people’s living conditions, but it has also resulted in some unhealthy, energy-dense food and tobacco products becoming affordable, especially in rural and in younger populations, those who lack sufficient knowledge about preventing cardiovascular disease and do not have adequate healthcare service. The increasing incidences of hypertension, dyslipidaemia and overweight in Chinese population are being observed. 14 In our study, the percentages of patients with hypertension or dyslipidaemia are almost as high as some studies from western countries,15,16 but the values of BMI are still lower than westerner. On the other hand, patients with Pre-MI in our study still experienced lower percentage of PCI and other revascularisation, which may be restricted to the development of economic and medical level in China.
With the pro-atherosclerotic, pro-inflammatory, hypercoagulable state and more cardiovascular risk factors engendered by T2DM, Pre-MI patients with T2DM might have a higher risk of Re-MI. Consistent with previous reports,4,16,17 we observed that the risk of Re-MI among T2DM patients was 67% higher, compared with non-T2DM subjects. Haffner et al. 4 first reported a higher incidence of fatal or nonfatal MI among T2DM subjects with Pre-MI, with an unadjusted relative risk of 2.39. However, due to advances in the treatment of MI and prevention of its long-term sequelae, studies conducted in prior decades should be applied cautiously to today’s population of MI survivors. In 2011, using data from the EPHESUS clinical trial, Deedwania et al. 7 reported that diabetes mellitus (DM) was significantly and independently associated with recurrent nonfatal MI (HR: 1.68; 95% CI: 1.23–2.31), but not with fatal MI or all-cause death. Regarding the different outcomes of our study and that of Deedwania et al., some differences might be relevant: (1) Deedwania et al. used data from the EPHESUS clinical trial, and their diabetic subjects were well matched with nondiabetic subjects and (2) Deedwania et al. chose subjects with heart failure, and patients with type 1 diabetes mellitus were also included. In 2014, Liang et al. 9 also reported that the adjusted HRs for subsequent MI were 1.41 (1.27–1.56) in women and 1.23 (1.14–1.34) in men, which were a little lower than our findings. With the consideration that patients with Re-MI might more commonly experience fatal arrhythmia or heart failure, the incidence of death among the Re-MI patients was higher.2,18 Together with a higher risk of Re-MI, T2DM patients also experienced a higher risk of developing heart failure, 19 stroke 20 and end-stage renal disease. 21 Thus, based on these previous findings, diabetic patients tend to suffer from a higher risk of mortality, compared with nondiabetic subjects. As expected, our findings showed that T2DM subjects had much higher mortality than non-T2DM subjects, similar to previous studies.15,22,23 In 1999, Melchior et al. 22 reported the positive influence of diabetes on mortality in patients with AMI (diabetic vs nondiabetic subjects, RR for 4–6 years: 1.74; 95% CI: 1.36–2.23); in 2007, a study conducted by Norhammar et al. 23 also showed that fatal outcomes remained more common among diabetic patients (adjusted RR for 8 years: 1.38; 95% CI: 1.32–1.43); in 2014, Liang et al. 9 reported that the adjusted HRs for all-cause death were 1.50 (1.41–1.60) in women and 1.40 (1.33–1.47) in men; and in recent years, two other studies in succession also reported higher risks of mortality among diabetic subjects, ranging from 1.4- to 1.76-fold compared with nondiabetic subjects.4,15
As we know, T2DM is often accompanied by a disturbed metabolic condition, which includes obesity, dyslipidaemia, hypertension and hypercoagulability. 24 With more common presentation of more diffuse artery atherosclerosis and accentuated plaque vulnerability, T2DM patients can have a higher prevalence of the co-morbidities of stroke and peripheral vascular diseases. 25 Consistent with previous studies among different races,4,7,9 our study revealed that Chinese patients with T2DM also presented with worse baseline characteristics, such as older age, higher BMI and creatinine values, and more frequent histories of hypertension and dyslipidaemia. In 1979, the Framingham study showed that the risk of developing CAD among diabetics was twice that among nondiabetic men and thrice that among nondiabetic women. 26 In 1998, Haffner et al. 4 suggested that diabetic patients without Pre-MI had as high a risk of MI as nondiabetic patients with Pre-MI, indicating the importance of diabetes in prognosis. In our study of patients with one MI event, the adjusted HR for Re-MI in diabetics was 1.67 fold that among nondiabetic patients. From previous findings,9,23 we might conclude that the occurrence of Pre-MI did not nullify all of the differences between T2DM and non-T2DM in some different races, while, in our study, it is confirmed that T2DM also independently contributed to a higher risk of Re-MI among Chinese patients, despite differences among races. Moreover, in 2013, Nakatani et al. 2 studied a total of 7870 Japanese patients who survived AMI, and they found that DM, history of MI and advanced age were independently associated with an increased risk of Re-MI. It seems that the influence of T2DM on patients with Pre-MI among yellow race or Asians may be the same as other races.
In the subgroup analysis of T2DM patients, our findings demonstrated a close association between ITDM and all-cause mortality, which was suggested in the study by Murcia et al. 17 However, being the same as Murcia et al., we also did not find that insulin treatment had a significant influence on MI recurrence among patients with T2DM and Pre-MI, regardless of worse glucose control in ITDM group. Antoniucci et al. 27 reported that the adjusted RR of insulin-requiring DM for 6-month mortality was 1.94 (95% CI: 1.17–3.22) after undergoing PCI for AMI, and they speculated that the relationship might be explained by myocardial reperfusion being less effective (52% vs 78%; p < 0.001). In 2014, Hoebers et al. 28 also reported that the adjusted mortality risks among ITDM patients were 1.7- and 1.9-fold those of NITDM and non-DM patients, respectively. According to previous reports, several proposed explanations could be possible, such as cardiovascular end points 27 and cancer 29 among ITDM patients. Insulin is an accelerated factor known for its atherogenic and mitogenic effects, which can lead to an adaptive advantage for malignant foci and the development of atherosclerotic vascular disease. 13 In addition, insulin treatment for T2DM seems to be linked to poor control of glucose, more severe vascular diseases and so on. However, conversely, insulin treatment might also restore impaired platelet function and decrease the activity of plasminogen activator inhibitor. 17 Considering the complex influences of T2DM and insulin treatment on metabolism, detailed studies of mechanism and cause are needed.
The higher risks of Re-MI and mortality in Chinese Pre-MI patients with T2DM reinforce the importance of available prevention among these patients. Our findings could help Chinese clinicians improve their estimates of patients’ future and enable more effective identification of high-risk patients for more intensive treatments. However, our study also had some weaknesses. First, it was not a randomised clinical trial, and the differences in baseline characteristics might have influenced the clinical outcomes, although multi-variable Cox regression was used to adjust for these factors. Second, our study only chose patients from two centres in Henan province, so it was limited by the lack of a nationwide and validated population database of all patients with diabetes. Furthermore, the use of dural antiplatelet was low and short in duration in our study compared with other studies. Third, although attention was paid to minimise bias, some bias might still remain and might have influenced the clinical outcomes, for example, we did not have information on individuals who suffered silent MI prior to their admission or death. Fourth, because the data on the cause of death were incomplete in this retrospective study, we could only conclude that there was a higher risk of all-cause death in T2DM, but the detailed causes of death were unknown. Further study should be undertaken. Despite these limitations, our study provided interesting information about prognosis among Chinese patients with Pre-MI and T2DM.
Conclusion
In China, among Pre-MI patients, T2DM was associated with higher risks of Re-MI and all-cause death; in particular, ITDM patients were also at higher risks for all-cause death compared with NITDM patients. These findings could prompt future research and more intensive risk factor modification to manage Pre-MI patients, especially those with T2DM who are receiving insulin treatment.
Footnotes
Acknowledgements
The authors thank the participants for participating in the study and provide their continued assistance and take public responsibility for the design, methods, and data collection. The authors would like to thank Dr Wen Zhao, from Zhengzhou University School of Pharmaceutical Sciences, for help during the manuscript’s writing and editing.
Author’s contribution
Wentao Li and Muwei Li contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.