
Abstract
Purpose:
Our objectives were to describe recent trends in the characteristics and in-hospital outcomes in diabetic as compared with non-diabetic patients hospitalized with ST-segment elevation myocardial infarction (STEMI).
Methods:
We reviewed the medical records of 2537 persons with (n = 684) and without (n = 1853) a history of diabetes who were hospitalized for STEMI between 1997 and 2009 at 11 medical centres in Central Massachusetts.
Results:
Diabetic patients were more likely to be older, female and to have a higher prevalence of previously diagnosed comorbidities. Diabetic patients were more likely to have developed important in-hospital complications and to have a longer hospital stay compared with non-diabetic patients. Between 1997 and 2009, there was a marked decline in hospital mortality in diabetic (20.0%–5.6%) and non-diabetic (18.6%–7.5%) patients.
Conclusion:
Despite reduced hospital mortality in patients hospitalized with STEMI, diabetic patients continue to experience significantly more adverse outcomes than non-diabetics.
Introduction
Diabetes mellitus is an important and common medical condition affecting more than 18 million American adults, and cardiovascular disease is the leading cause of morbidity and mortality in patients with diabetes. 1 In addition to being at increased risk of developing coronary heart disease, patients with diabetes experience higher hospital and post-discharge mortality rates after an acute myocardial infarction (AMI) than patients without diabetes.2–5 Increased morbidity and mortality among diabetic patients developing AMI is especially concerning given the increasing prevalence of obesity and diabetes in the United States and worldwide. 1
Although several population-based studies have described trends in the incidence, management and outcomes of diabetic patients hospitalized with AMI,2–5 few have examined these factors specifically in patients presenting with ST-segment elevation myocardial infarction (STEMI). Furthermore, despite considerable advances in the management of patients hospitalized with STEMI,6,7 several reports suggest that the frequency of important in-hospital clinical outcomes remains sub-optimal in STEMI patients with, as compared to those without, diabetes.8–10
The objectives of this population-based study were to describe overall differences, and more than decade-long trends (1997–2009) therein, in the characteristics, in-hospital management, clinical complications and in-hospital mortality in diabetic as compared with non-diabetic patients hospitalized with STEMI in all medical centres throughout Central Massachusetts.
Methods
Data from the Worcester Heart Attack Study were used for this investigation.11–13 The Worcester Heart Attack Study is an ongoing population-based investigation examining long-term trends in the descriptive epidemiology of AMI in residents of the Worcester, Massachusetts, metropolitan area (2000 census = 478,000) hospitalized with AMI.11–13 In brief, the medical records of residents of this metropolitan area admitted to all 11 hospitals in Central Massachusetts with a discharge diagnosis of AMI and related coronary disease rubrics were individually reviewed and validated according to pre-established criteria. This study sample consisted of greater Worcester residents hospitalized with AMI on a biennial basis between 1997 and 2009. This study was approved by the Institutional Review Board at the University of Massachusetts Medical School.
In this study, we focussed only on patients with STEMI which was defined as when new ST-segment elevation was present at the J point in two or more contiguous electrocardiography (EKG) leads. 7 We further classified patients as having a history of diabetes or the absence thereof, based on the review of data available in hospital medical records.3,14
Data collection
Trained nurses and physicians abstracted demographic and clinical data from the medical records of greater Worcester residents hospitalized with confirmed AMI. Quality control activities were routinely conducted on all nurse and physician data abstractors. Abstracted information included patient’s age, sex, medical history, AMI order (initial vs prior), physiologic factors, laboratory test results, length of hospital stay, time interval between patient-reported acute symptom onset and emergency department arrival and hospital discharge status.11–13,15 Information about the use of important cardiac medications, coronary angiography, percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG) surgery was collected. Development of several significant clinical complications (e.g. atrial fibrillation, cardiogenic shock, stroke, heart failure) during the patient’s index hospitalization was defined according to standardized criteria.11,13,16–19
Data analysis
Differences in the characteristics of diabetic as compared with non-diabetic patients hospitalized for STEMI were examined through the use of chi-square tests for discrete variables and t-tests for continuous variables. In-hospital case-fatality rates (CFRs) and proportion of patients developing several in-hospital clinical complications were calculated in a standard manner.
We carried out a series of multivariable-adjusted logistic regression analyses to assess the overall impact of diabetes, and the significance of changing trends between 1997 and 2009, in the odds of developing atrial fibrillation, stroke, heart failure and cardiogenic shock and dying during the acute hospitalization while controlling for several potentially confounding demographic, medical history and clinical factors that have been shown to affect these outcomes. Confounders for the multivariable regression analyses were selected based on clinical risk factors that have been commonly described in the published literature and that have been used in previously published manuscripts from the Worcester Heart Attack Study. Control variables included indicators for the following covariates: age, sex, history of various coexisting disorders (angina, heart failure, hypertension or stroke) and AMI order (initial vs prior).
Results
Characteristics of study patients
A total of 2537 residents of Central Massachusetts were hospitalized with confirmed STEMI during the years under study (Table 1). The average age of these patients was 68 years, 56% were male and 27% had been previously diagnosed with diabetes (n = 684).
Characteristics of diabetic and non-diabetic patients hospitalized with STEMI.
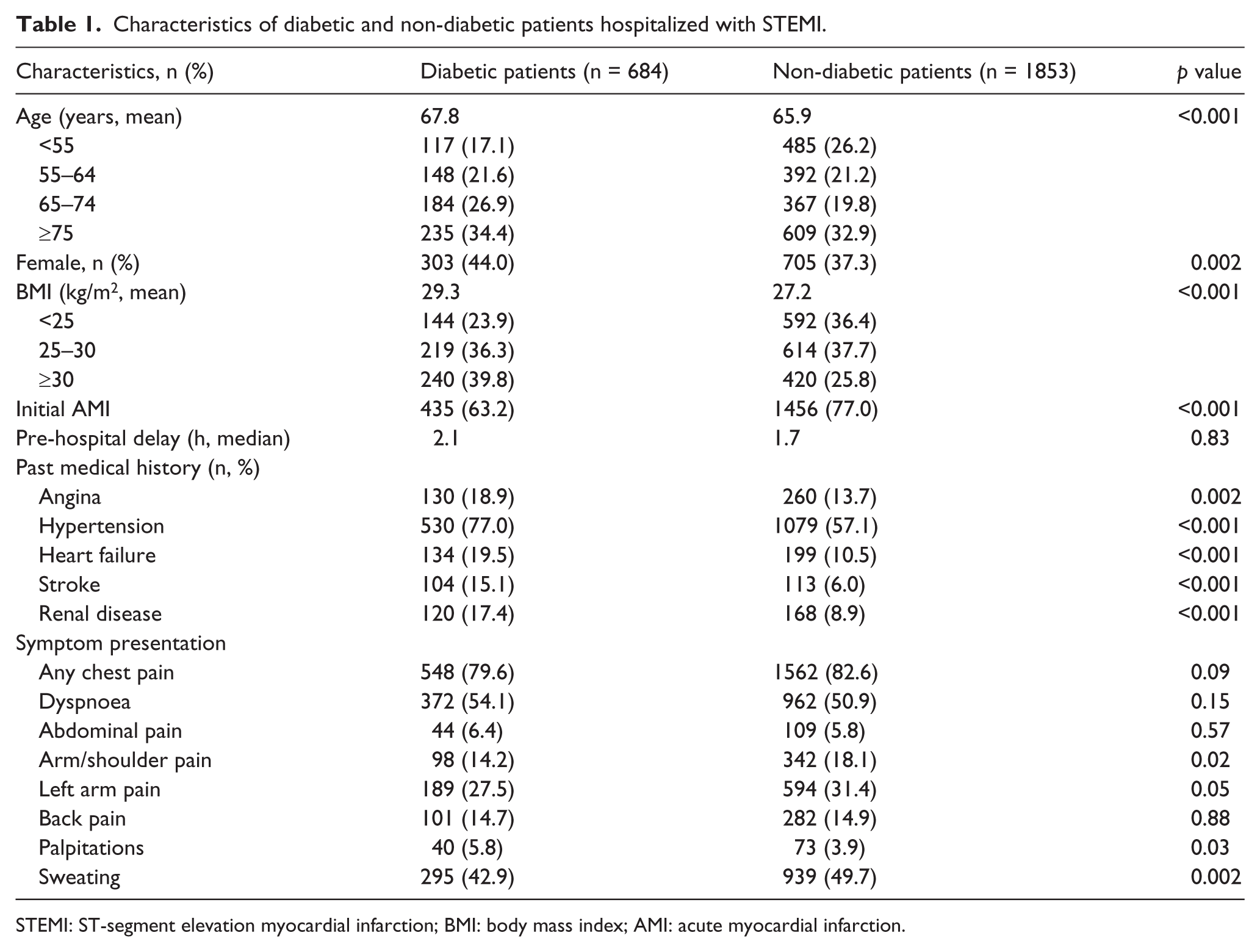
STEMI: ST-segment elevation myocardial infarction; BMI: body mass index; AMI: acute myocardial infarction.
Overall, diabetic patients were approximately 2 years older on average than non-diabetic patients and were more likely to be women. Persons with diabetes had a higher average body mass index (BMI) than non-diabetic patients and were much more likely to be obese. Diabetic patients presenting with STEMI had a higher prevalence of several important cardiovascular comorbidities as compared with non-diabetic patients (Table 1).
In terms of acute presenting symptoms, patients with previously diagnosed diabetes were less likely to have presented with classic anginal symptoms including chest pain, arm pain, shoulder pain and diaphoresis, and were more likely to have complained of dyspnoea and palpitations, than patients without diabetes. Overall, diabetic patients experienced longer delays in seeking acute medical care (median = 2.1 vs 1.7 h) and had a longer hospital stay (median = 5.0 vs 4.0 days) than non-diabetic patients (p = NS).
Hospital treatment practices
Overall, the prescribing of in-hospital cardiac medications was relatively similar in both diabetic and non-diabetic patients (Table 2). There were encouraging and significant increases over time in the use of recommended cardiac medications including angiotensin-converting enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs), β-blockers, aspirin and statins in STEMI patients with and without diabetes (Figure 1). In patients with prior diabetes, particular increases were noted in the prescribing of ACE inhibitors/ARBs (from 56% to 72%) and statins (from 20% to 99%) between 1997 and 2009. Diabetic patients were more likely to have received ACE inhibitors/ARBs, calcium channel blockers, digoxin and diuretics during their acute hospitalization as compared with non-diabetic patients.
Hospital management practices in diabetic and non-diabetic patients hospitalized with STEMI.
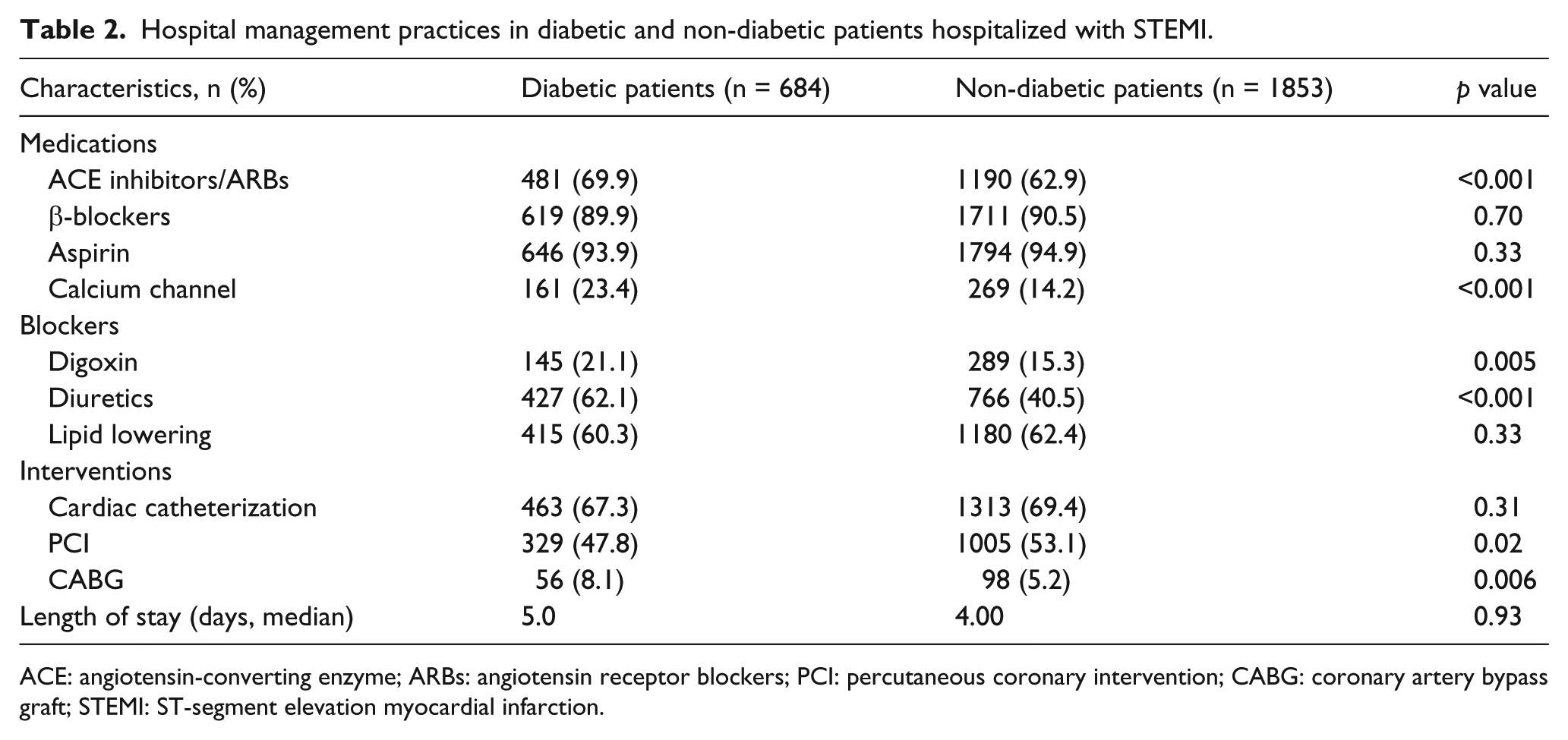
ACE: angiotensin-converting enzyme; ARBs: angiotensin receptor blockers; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; STEMI: ST-segment elevation myocardial infarction.
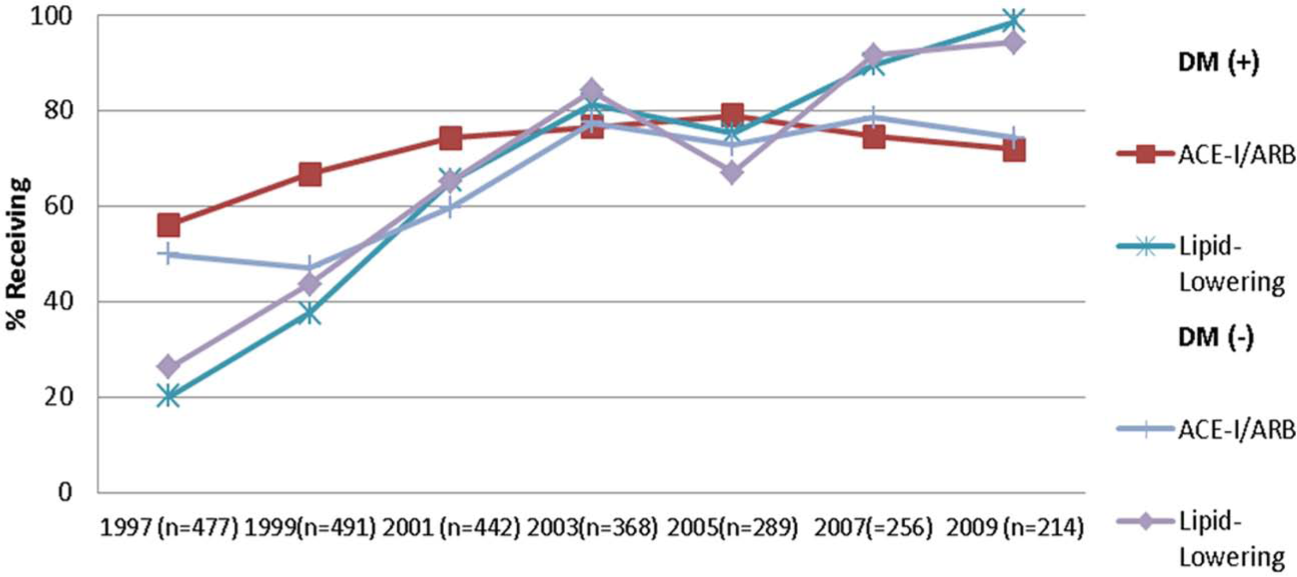
Trends in the receipt of hospital medications in diabetic and non-diabetic patients hospitalized with STEMI.
While there were marked increases over time in the proportion of patients with and without diabetes undergoing cardiac catheterization and PCI during their hospitalization, diabetic patients were as likely to have undergone cardiac catheterization (67% vs 69%) or PCI (49% vs 53%) than patients without diabetes (Figure 2). The percentage of diabetic patients undergoing CABG surgery was significantly higher than in those without previously diagnosed diabetes (8.1% vs 5.2%) (p < 0.05); these percentages remained essentially unchanged between 1997 and 2009.
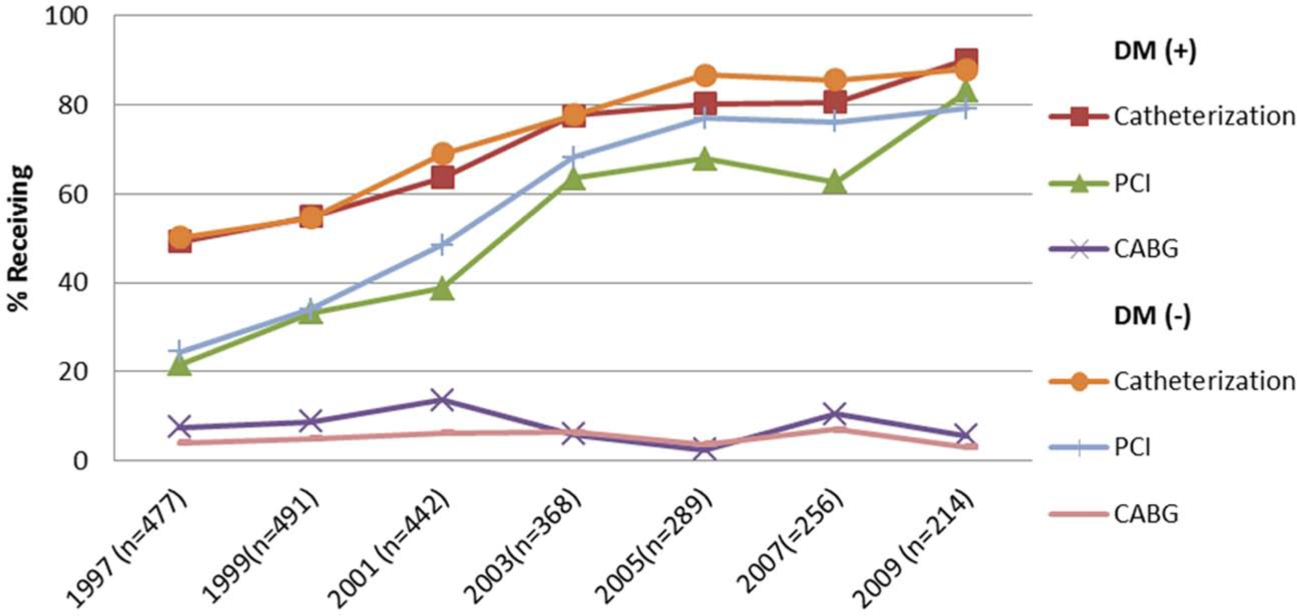
Trends in the receipt of hospital interventions in diabetic and non-diabetic patients hospitalized with STEMI.
In-hospital clinical complications and hospital death rates
Overall, diabetic patients were more likely to have developed important in-hospital complications including heart failure, atrial fibrillation and cardiogenic shock compared to those without diabetes (Table 3). Diabetic patients also experienced significantly higher in-hospital death rates as compared to those without diabetes (13.1% vs 9.9%, p = 0.02). There was no significant change in the incidence rates of these clinical complications during the years under study (Figure 3).
Hospital clinical complications in diabetic and non-diabetic patients hospitalized with STEMI.
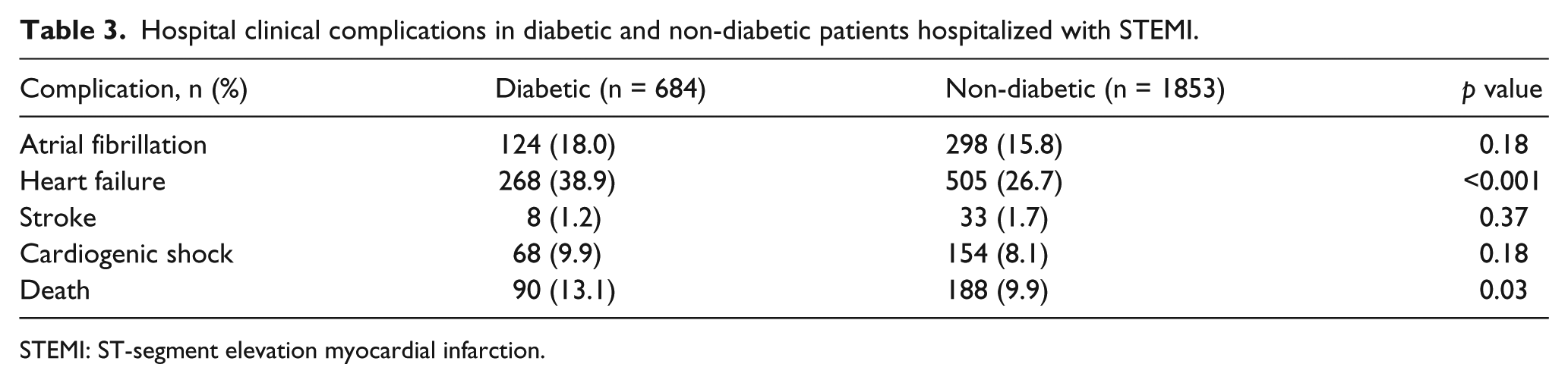
STEMI: ST-segment elevation myocardial infarction.
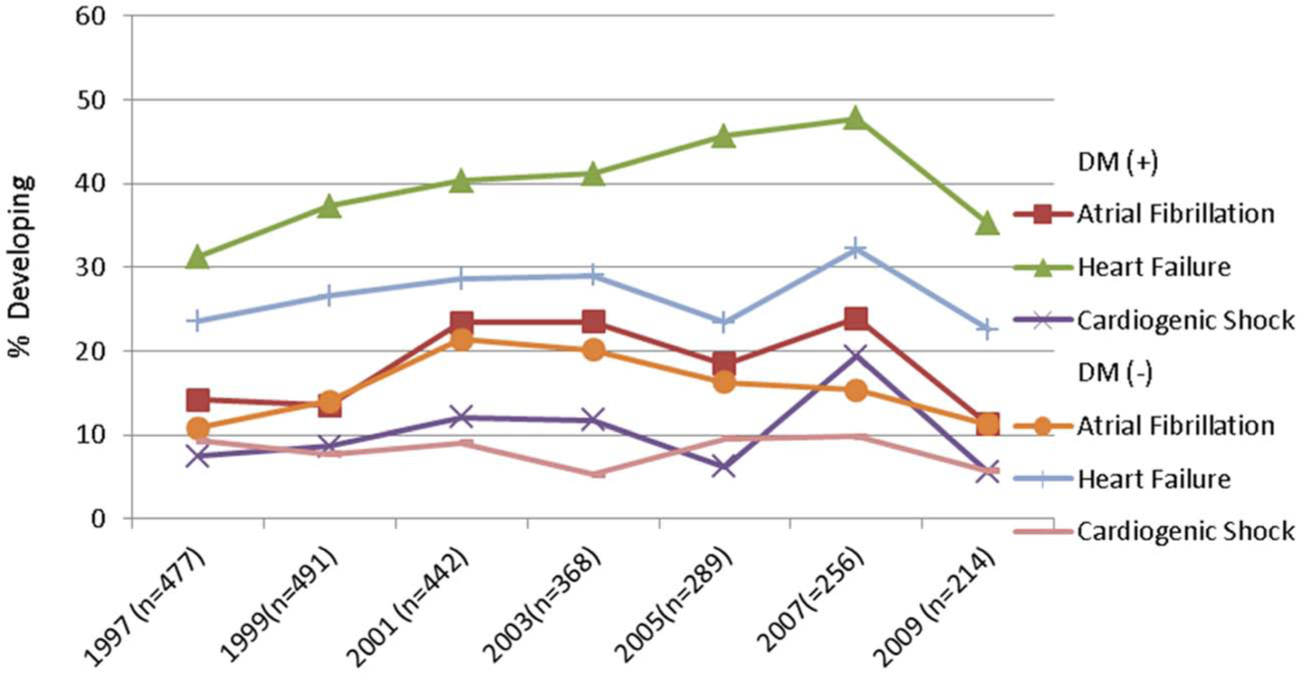
Trends in hospital complications in diabetic and non-diabetic patients hospitalized with STEMI.
We examined the risks of developing important in-hospital complications as well as dying in patients with and without diabetes, first calculating unadjusted odds ratios (ORs) and then adjusting for several confounding factors of prognostic importance. Overall, the multivariable-adjusted OR of patients with diabetes, as compared with non-diabetic patients, developing atrial fibrillation (OR: 1.10; 95% confidence interval (CI): 0.85–1.42), heart failure (OR: 1.49; 95% CI: 1.21–1.83) and cardiogenic shock (OR: 1.28; 95% CI: 0.92–1.77) or dying (OR: 1.23; 95% CI: 0.92–1.65) during hospitalization was slightly higher, although the results reached statistical significance only for the development of heart failure.
In contrast to several of the clinical complications examined, a significant decline in in-hospital death rates was observed in both diabetic (20.0%–8.3%) and non-diabetic patients (18.6%–10.9%) between 1997 and 2009; these declines in short-term death rates remained after controlling for various demographic and clinical factors of prognostic importance (data not shown).
Discussion
The principal finding of this large population-based study of residents of the Worcester metropolitan area presenting to all medical centres in Central Massachusetts with STEMI was that despite encouraging trends in both the medical and invasive treatment of these patients, and declines in hospital mortality over time, diabetic patients remained at increased risk of developing important in-hospital complications and dying as compared with non-diabetic patients.
Study sample characteristics
Our findings are consistent with those of prior studies showing that diabetic patients hospitalized with STEMI are older, more often female, more likely to present with a prior myocardial infarction (MI) and were more likely to have a variety of cardiovascular comorbidities than patients without previously diagnosed diabetes.20,21 In a large (n = 2600) single-centre registry of patients undergoing PCI for STEMI in the United Kingdom between 2005 and 2009, diabetic patients were more often older, female and had a higher prevalence of cardiovascular disease as compared to those without diabetes. 20 Similar differences were reported in the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS AMI) study in which 3000 patients with and without diabetes underwent PCI during hospitalization for STEMI at several New York City hospitals between 2005 and 2007. 21
Our results also support previous studies that have reported that diabetic patients with AMI were less likely to report classic anginal symptoms, but were more likely to complain of non-anginal symptoms, than patients without diabetes. 22
Hospital treatment practices
The prescribing of recommended in-hospital cardiac medications increased significantly during the years under study in both diabetic and non-diabetic patients hospitalized with STEMI. Notably, diabetic patients were more likely to have received ACE inhibitors/ARBs than non-diabetic patients. Similar prescribing trends were observed in the large National Registry of Myocardial Infarction that studied patients presenting with AMI between 1994 and 2006. 23 The rates of use of proven cardiac therapies increased in patients with and without diabetes throughout the study period, with greater increases in the use of aspirin and β-blockers observed in patients with diabetes during the years under study. 23
In this study, the utilization of PCI in diabetic patients was essentially similar to that of non-diabetic patients, whereas the use of CABG surgery was significantly greater in patients with diabetes. In a recent study using data from Global Registry of Acute Coronary Events (GRACE), a multinational observational study of patients hospitalized with the full spectrum of acute coronary syndromes, the use of reperfusion therapy for patients with STEMI was examined. The investigators found that patients with ahistory of diabetes were less likely to have undergone a PCI than persons without diabetes. 24 Similarly, in the CRUSADE study, an observational national registry of patients with acute coronary syndromes treated at a large number of hospitals throughout the United States, 25 patients with an STEMI and a history of diabetes were less likely to have received a PCI than patients without this metabolic disorder. 25 In our most recent study year (2009), approximately twice as many persons with diabetes, as compared to persons without diabetes, underwent CABG surgery during their index hospitalization. These findings are consistent with current evidence-based guidelines that recommend CABG surgery, rather than PCI, be used in diabetic patients with multi-vessel coronary artery disease. 26 Our results demonstrate the increasingly aggressive medical and invasive treatment of patients hospitalized with STEMI, particularly among those with previously diagnosed diabetes.
In-hospital clinical complications and death rates
In our crude unadjusted analyses, diabetic patients presenting with STEMI were more likely to have developed atrial fibrillation, heart failure and cardiogenic shock and die during their acute hospitalization than non-diabetic patients; however, after controlling for several important potentially confounding factors, persons with diabetes experienced only a slightly increased odds of developing these adverse outcomes compared to those without a history of previously diagnosed diabetes.
Some investigators have invoked the role of diabetic cardiomyopathy as a potential causative factor in the development of heart failure and other serious clinical complications in patients with diabetes and STEMI. 27 Our findings demonstrating a higher prevalence of heart failure in diabetic patients are important because diabetes might be a potential marker of more profound clinical derangements and kidney disease in these patients, leading to higher rates of heart failure. 28 Similar to our findings, in a recent study of 6700 AMI patients admitted to 27 different coronary care units in Denmark, the rates of developing cardiogenic shock were higher in diabetic as compared with non-diabetic patients. 29
In the present investigation, hospital CFRs decreased dramatically between 1997 and 2009 in patients with and without diabetes, with a greater reduction in mortality observed in diabetic patients. The increasingly effective medical treatment and timely interventional management of patients who developed a STEMI likely contributed to the improved in-hospital survival observed in these patients during the more than decade-long period under study. Given the non-randomized nature of this study, and the significant potential for confounding by treatment indication, we did not, however, control for the use of various cardiac treatment regimens in examining changing trends in hospital death rates over time. Data from more than 1.7 million patients hospitalized with AMI between 1994 and 2006 in the National Registry of Myocardial Infarction demonstrated declining trends in the diabetes-associated risk of dying during hospitalization for AMI, similar to the results of this study. 23
Study strengths and limitations
The strengths of this study include the large number of patients hospitalized with, independently validated, STEMI from a large central New England metropolitan area whose socio-demographic characteristics reflect those of the US population as a whole, supporting the potential generalizability of our study findings. Several limitations, however, need to be considered in the interpretation of the present findings. The diagnosis of diabetes was based on data contained in hospital medical records and not according to pre-defined measurements or a standardized study protocol. Additionally, since this was an observational study carried out at several hospitals over varying time periods, we were not able to systematically characterize patient’s fasting glucose levels and instead assessed random glucose levels at the time of hospital presentation with STEMI. We did not have access to systematically collected haemoglobin A1c levels, fasting glucose levels, glucose tolerance test results, type of outpatient treatment that diabetic patients were receiving, duration of time that patients were known to be diabetic or other information to further characterize patient’s chronic glycometabolic status.
Conclusion
The results of this study among residents of a large Central Massachusetts community provide insights into the characteristics, management and in-hospital outcomes of diabetic as compared with non-diabetic patients presenting with STEMI. Despite encouraging trends in both the medical and invasive treatment of patients with STEMI, and declines in hospital mortality rates over time, diabetic patients remained at increased risk of adverse in-hospital outcomes as compared with non-diabetic patients. Given the ongoing obesity epidemic in the United States, and the high morbidity and mortality associated with diabetes, there remains a significant unmet need for the improved care of these high-risk patients and their careful in-hospital monitoring if they develop an STEMI.
Footnotes
Acknowledgements
We wish to acknowledge all persons involved in the review of data for this project as well as our collaborators at all greater Worcester hospitals. All authors had access to the data and had a role in writing this manuscript.
Declaration of conflicting interest
There are no conflicts of interest to report for any of the authors.
Funding
Partial salary support is provided to Drs. McManus, Gore, and Goldberg by National Institute of Health grant 1U01HL105268-01 and to Dr. McManus by National Institutes of Health Grant KL2RR031981.