
Abstract
Introduction:
We examined whether circulating adiponectin levels are associated with further cardiovascular events in patients with type 2 diabetes.
Methods:
Between December 2004 and February 2005, 349 patients with type 2 diabetes were enrolled and followed-up until December 2015. Blood levels of total, middle-molecular weight and high-molecular weight adiponectin were measured at baseline. The primary composite outcome was the occurrence of the following events: cardiovascular death, non-fatal myocardial infarction, non-fatal stroke or hospitalization for unstable angina and heart failure.
Results:
During a median follow-up of 9 years, cardiovascular events occurred in 14% of patients (50/349, 1.9% per year). Median blood levels of total, middle-molecular weight and high-molecular weight adiponectin were 4.8, 3.2 and 1.8 μg/mL, respectively. The cumulative incidence of cardiovascular events was not significantly different between the three groups based on total, middle-molecular weight, high-molecular weight or high-molecular weight/total adiponectin. After adjustment for potential confounding factors, blood adiponectin levels were positively associated with an increased number of cardiovascular events, but between tertiles, there was no significant difference.
Conclusion:
This observational cohort study suggested that blood adiponectin levels are not related to further cardiovascular events in patients with type 2 diabetes.
Introduction
The focus of this study is adiponectin, detectable in the circulation in low-molecular weight (LMW; trimer), middle-molecular weight (MMW; hexamer) and high-molecular weight (HMW; 12- to 18-mer) forms. 1 The active form is HMW adiponectin, based on its greater biological activity compared with LMW or MMW adiponectin. 2 A strong association between hypoadiponectinemia and the development of type 2 diabetes has been consistently reported. 3 Although adiponectin has vasoprotective and anti-inflammatory properties, 4 clinical studies of different populations have yielded controversial results regarding the relationship between circulating adiponectin and cardiovascular morbidity and mortality, especially in Asian populations. Therefore, in this study, we measured the levels of circulating isoforms of adiponectin and assessed their potential association with cardiovascular events in Korean patients with type 2 diabetes.
Methods
Study design and population
This was an observational cohort study performed in a single tertiary hospital. The 349 patients 20 years of age or older who satisfied the diagnostic criteria of type 2 diabetes set by the American Diabetes Association in 2004 were enrolled between December 2004 and February 2005. All participants were requested to regularly visit the hospital, at 3- or 6-month intervals, and were followed-up until the end of 2015. Data, including cardiovascular events, were collected from the patients after their enrolment, by interview and medical chart review. Venous blood samples were drawn from the patients after they had fasted overnight. Levels of HbA1c, plasma glucose, C-reactive protein, insulin and serum creatinine, as well as lipid profiles were measured at baseline. Adiponectin assays were performed using plasma samples previously frozen as rapidly as possible to −70°C and thawed immediately before their use. Total, HMW and MMW forms of plasma adiponectin were analysed using an enzyme-linked immunosorbent assay kit (Daiichi, Pure Chemicals, Tokyo, Japan). The intra-assay variation was 5.3% (total adiponectin), 4.1% (MMW and HMW adiponectin) and 3.3% (HMW adiponectin). The primary outcome was the time to first occurrence of any of the following adjudicated components of the composite endpoint: cardiovascular death, non-fatal myocardial infarction (MI), non-fatal stroke or hospitalization for unstable angina pectoris or heart failure. Patients hospitalized for unstable angina pectoris received percutaneous coronary intervention or coronary artery bypass surgery.
Statistical analyses
Curves of cardiovascular events were plotted using the Kaplan–Meier method and compared using the log-rank test according to each isoform of plasma adiponectin and the HMW/total adiponectin ratio. A hazard ratio for the occurrence of cardiovascular events was determined in a Cox proportional hazard regression analysis. Two-sided p-values < 0.05 were considered to indicate statistical significance. All data were analysed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA) and SPSS (version 23.0; SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics at baseline
The study patients were followed-up for a median (interquartile range [IQR]) duration of 9.0 (4.2–10.8) years. Their mean (SD) age and duration of diabetes was 54.7 (11.3) and 9.0 (6.8) years, respectively (Table 1). Mean (SD) systolic and diastolic BP was 135.5 (15.8) and 78.3 (10.3) mm Hg, respectively. The mean (SD) body mass index (BMI) was 25.4 kg/m2 (3.1) and the median HOMA-IR was 2.5 (1.6–4.8). The mean (SD) HbA1c and fasting glucose level at baseline was 7.6% (1.4) and 146.7 mg/dL (45.3), respectively. A previous diagnosis of cardiovascular disease (coronary artery disease or cerebrovascular disease) was reported in 14% and a history of diabetic retinopathy in 22%. The level of total, MMW and HMW adiponectin was 4.8, 3.2 and 1.8 μg/mL, respectively, and the HMW/total adiponectin ratio was 0.4.
Demographic data and baseline characteristics of the study patients.
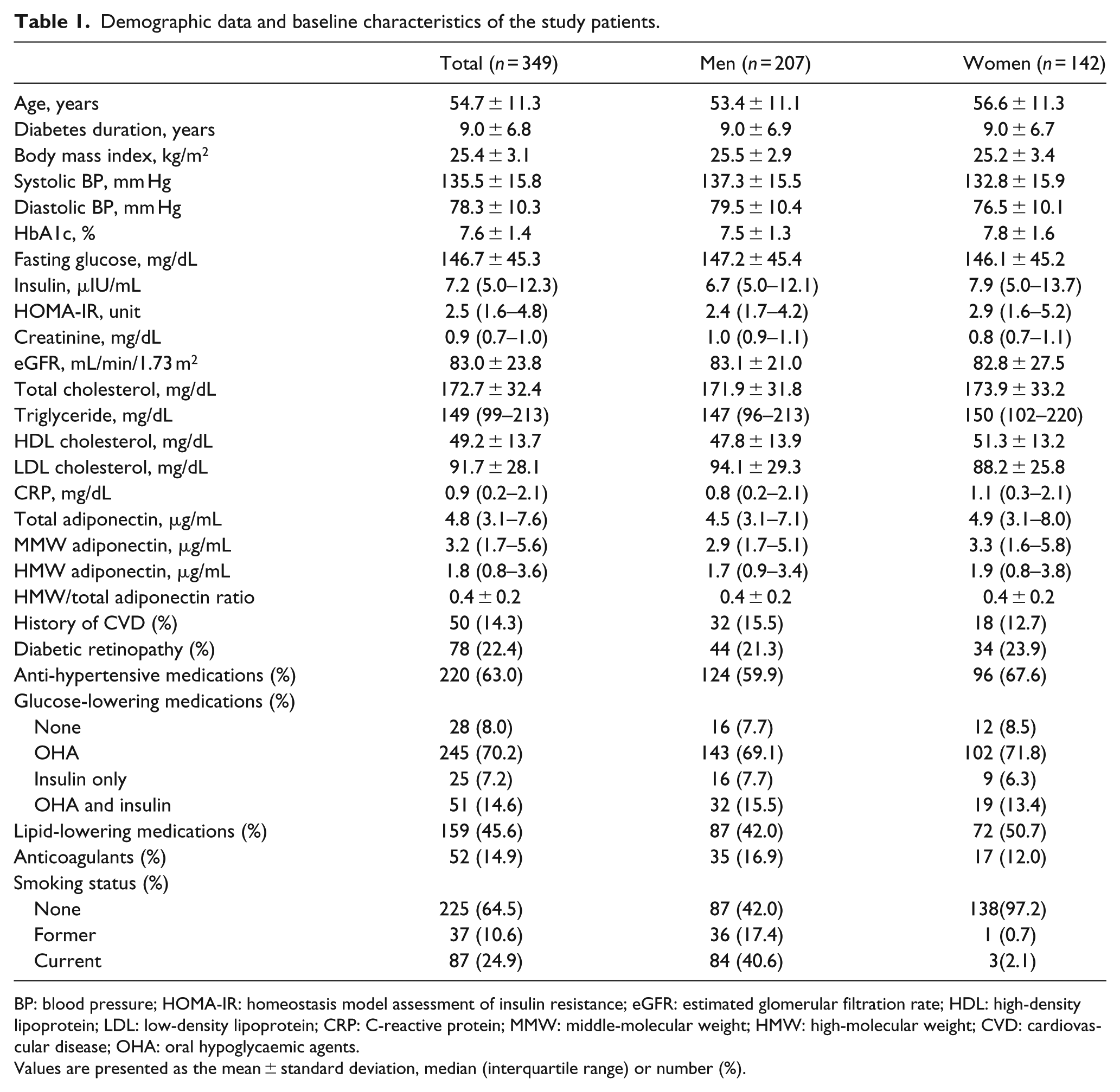
BP: blood pressure; HOMA-IR: homeostasis model assessment of insulin resistance; eGFR: estimated glomerular filtration rate; HDL: high-density lipoprotein; LDL: low-density lipoprotein; CRP: C-reactive protein; MMW: middle-molecular weight; HMW: high-molecular weight; CVD: cardiovascular disease; OHA: oral hypoglycaemic agents.
Values are presented as the mean ± standard deviation, median (interquartile range) or number (%).
Cardiovascular events developed in 50 (14%) of the 349 patients during the follow-up period, corresponding to a rate of 1.9% per year. Cardiovascular events experienced during the follow-up period consisted of fatal events (n = 10, 2.9%), non-fatal MI (7, 2%), non-fatal stroke (11, 3.2%), hospitalization for unstable angina (29, 8.3%) and hospitalization for heart failure (5, 1.4%), including duplicate events.
Relationship between circulating adiponectin levels and the incidence of cardiovascular events
Figure 1 shows the cumulative incidence curves for cardiovascular events as a function of the tertiles of the blood adiponectin level. The incidence of cardiovascular events was higher in the highest compared with the lowest total adiponectin tertile, but the difference was not statistically significant (log-rank test, p = 0.433). The trend seen in the cardiovascular event curves according to the tertiles of MMW adiponectin, HMW adiponectin and the HMW/total adiponectin ratio were similar to those of total adiponectin (log-rank test; MMW, p = 0.676; HMW, p = 0.630; HMW/total adiponectin ratio, p = 0.413). After adjustment for age, sex and cardiovascular risk factors, there was no significant association between total, MMW and HMW adiponectin or the HMW/total adiponectin ratio and the risk of cardiovascular events; however, overall, the hazard ratio of the highest tertile was higher than that of the lowest tertile for the three forms of adiponectin and the HMW/total adiponectin ratio.
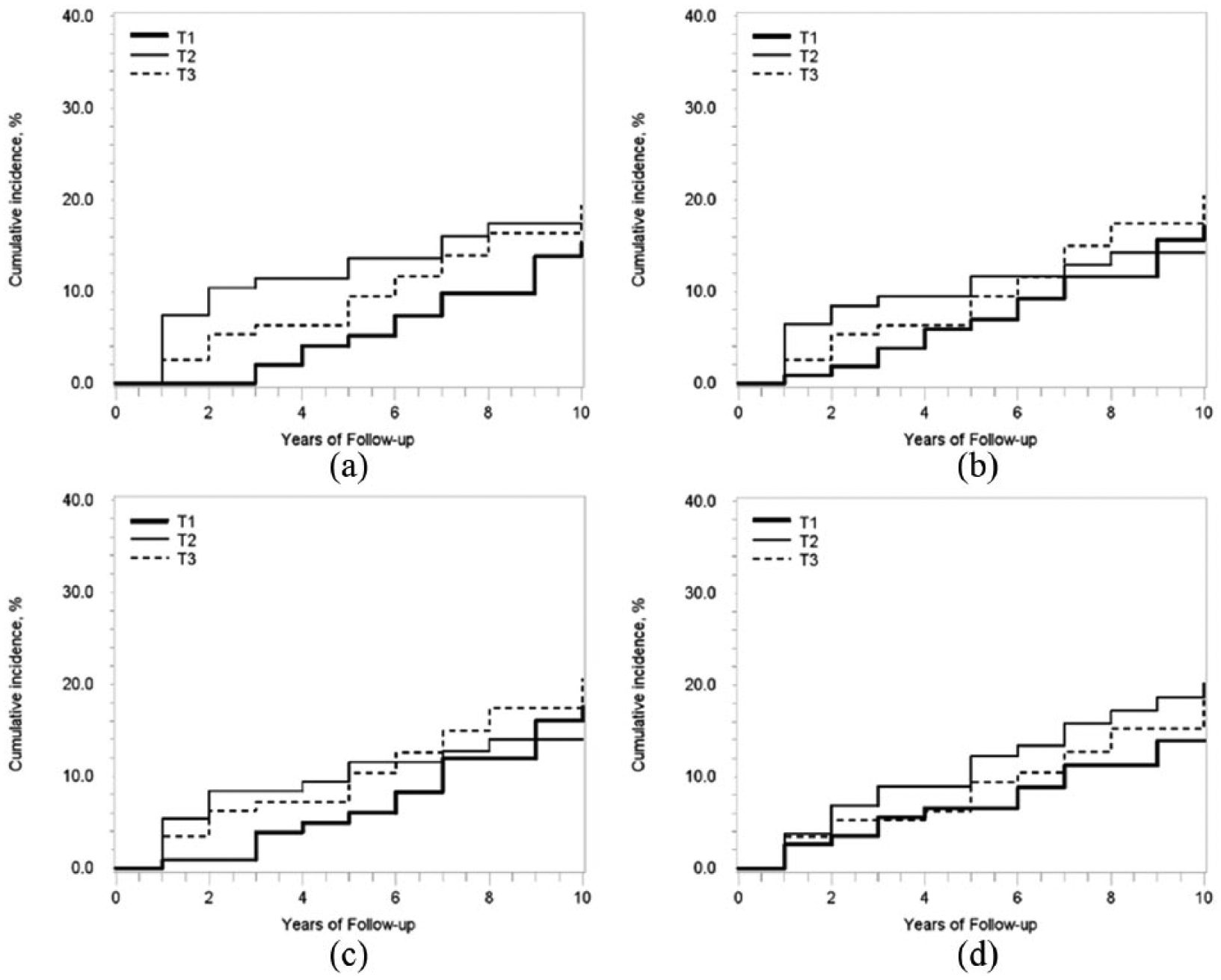
Cumulative incidence curves of cardiovascular events by tertile of blood adiponectin levels (log-rank test; total adiponectin, p = 0.433; middle-molecular weight [MMW], p = 0.676; high-molecular weight [HMW], p = 0.630; HMW/total adiponectin ratio, p = 0.413): (a) total adiponectin, (b) MMW adiponectin, (c) HMW adiponectin and (d) HMW/total adiponectin.
Discussion
This is a long-term observational study (median follow-up time of 9 years) that investigated the implications of adiponectin on further cardiovascular events in Koreans with type 2 diabetes. Our results suggest that the levels of circulating adiponectin, regardless of the isoform, are not associated with the occurrence of further cardiovascular events in this population. However, patients whose adiponectin levels were in the highest tertile suffered more events than patients whose adiponectin levels were in the lowest tertile, although the difference was not statistically significant.
Despite several studies of the potential association between adiponectin concentrations and cardiovascular morbidity or mortality in various populations, the results have been conflicting. Zoccali et al. 5 found an inverse association between the levels of circulating adiponectin and cardiovascular events among patients with end-stage renal disease. Meanwhile, in several prospective studies and another meta-analysis, there was no association between circulating adiponectin levels and cardiovascular disease.6–9 Specifically, in studies investigating this association in patients with type 2 diabetes who have high risk of cardiovascular disease and in those examining the association of cardiovascular disease and HMW rather than total adiponectin, there was either an inverse or unexpected paradoxical association or no association between the adiponectin concentration and a risk of the subsequent development of cardiovascular disease or death.10–13 In studies of Asian populations, including data from a Korean study, the effects of adiponectin on the risk of cardiovascular disease or death were likewise inconsistent.14–16 Our results support the lack of evidence for a strong association between adiponectin level, regardless of the isoform and a further risk of cardiovascular disease in Korean patients with type 2 diabetes.
Previous studies examined the unexpected causality between adiponectin levels and cardiovascular mortality or morbidity. The data suggested a compensatory elevation of adiponectin under metabolically unfavourable conditions or an increase in adiponectin as a marker of a disease state characterized by wasting. 16 In contrast to the protective effect of adiponectin on the development of diabetes, our results suggest an impact on atherosclerosis, albeit a weak one, compared with the other cardiovascular risk factors evaluated; thus, the ambiguous results regarding the effect of adiponectin on cardiovascular disease may reflect a combination of a vasoprotective effect and a compensatory increase due to the underlying disease state. An elucidation of the relationship between adiponectin and cardiovascular events therefore awaits further studies.
A limitation of our study was the small number of events, due to the fact that our study patients were relatively young at baseline. This might have led to a lack of power of the study, even though all of the patients had type 2 diabetes, a strong risk factor of cardiovascular events, and a relatively long observation time. Although various confounding factors present at baseline were considered, residual factors that emerged during follow-up, such as the level of physical activity, weight change, change of medications, degree of glycemic control or BP, could not always be taken into account.
In conclusion, our study of Korean patients with type 2 diabetes who were followed for 9 years demonstrated that blood adiponectin levels, regardless of the adiponectin isoform, were unlikely to affect the development of subsequent cardiovascular events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.