
Abstract
Background:
Patients with type 2 diabetes mellitus face an increased risk of cardiovascular events compared to non-diabetic counterparts. Chronic inflammation and activation of the immune system, including B-lymphocyte maturation is believed to play a role in atherosclerosis. Recent investigations suggest combined serum free light chains as a potential biomarker for cardiovascular events. The aim of this analysis was to investigate the association of combined serum free light chain with carotid atherosclerosis in subjects with type 2 diabetes mellitus.
Methods:
We performed a cross-sectional analysis of data from a prospective single centre 2-year study of 97 patients with type 2 diabetes mellitus and insufficiently controlled cardiovascular risk factors. Complete data on combined serum free light chain, high-sensitivity C-reactive protein were available for 75 subjects.
Results:
We analysed data of 26 female and 49 male subjects, aged 59 ± 8 years. Their mean body mass index was 31.6 ± 4.4 kg/m2, and the median B-score was 2 (interquartile range: 0–3). Significant positive correlations between combined serum free light chain and the B-score (r = 0.38; p = 0.001) as well as combined serum free light chain and high-sensitivity C-reactive protein (r = 0.35; p = 0.002) were observed. The adjusted odds ratio for a half standard deviation increase in combined serum free light chain was 1.48 (95% confidence interval: 1.05–2.05) in an ordinal regression model for carotid B-score.
Conclusion:
In our study, combined serum free light chain was associated with carotid atherosclerosis in subjects with type 2 diabetes mellitus.
Introduction
Patients with type 2 diabetes mellitus (T2DM) are exposed to a higher risk of cardiovascular disease (CVD) as compared to non-diabetic counterparts. 1 However, the excess risk cannot be explained by established cardiovascular risk factors only, leading to biomarker research with the aim to identify novel markers to predict prognosis more precisely.
Serum free light chains are polypeptide subunits of antibodies which arise as a by-product of antibody synthesis by terminally differentiated B lymphocytes which play a substantial role in the physiology of the adaptive immune system. 2 Determination of immunoglobulin κ and λ combined serum free light chain (cFLC) is an established diagnostic parameter to detect plasma cell proliferative disorders characterized by monoclonal gammopathies such as multiple myeloma or plasmacytoma. 3 However, more recently polyclonal cFLC elevations were investigated as a potential biomarker for chronic inflammatory states such as atherogenesis. Bellary et al. 4 demonstrated an association between cFLCs levels and CVD risk in a cohort of 352 south Asian patients with T2DM.
Moreover, recently published research identified levels of monoclonal cFLC and abnormalities of the κ to λ free light chain ratio as potential biomarkers for overall survival in the general population 5 or in populations such as subjects with heart failure, 6 acute coronary syndrome 7 or autoimmunity disease. 8
Whether this observed association between cFLC levels and CVD outcome might be explained by more progressive atherosclerosis triggered by an activation of the humoral immune response remains unexplored thus far. In this analysis, we used a data set of a prospective cohort study in subjects with T2DM to investigate associations between cFLC and carotid atherosclerosis.
Materials and methods
Study population and design
In this analysis, we present data of a subgroup of the CARDIONOR (treatment of CARDIOvascular Risk in Patients with Diabetes Mellitus Type-2: Identification of Treatment Non-Responders) study, 9 which was performed in 97 patients with T2DM without previous cardiovascular events and at least two insufficiently controlled risk factors, that is, low-density lipoprotein (LDL) cholesterol >3.1 mmol/L (>120 mg/dL), blood pressure >140/90 mm Hg (either or), HbA1c >7.5% (>58 mmol/mol). 9 Patients were eligible if they were 45–75 years old and had manifest T2DM. Diabetes mellitus was defined as fasting blood glucose of ⩾7 mmol/L (⩾126 mg/dL) or a history of established diabetes according to World Health Organization (WHO) criteria. For this analysis, we used a subset of 75 subjects with complete data on free light chain levels and high-sensitivity C-reactive protein (hsCRP).
This study has been approved by the local ethics committee of the Medical University of Graz (18–143 ex 06/07), Austria, and is registered at clinicaltrials.gov (NCT00660790). Written informed consent was obtained from all participants prior to enrolment.
Investigation of cFLC and carotid atherosclerosis
Serum κ and λ free light chains were measured by nephelometry (Freelite®; The Binding Site Group, Birmingham, UK) on a BN™ II analyzer (Siemens Healthcare Diagnostics, Marburg, Germany). Carotid atherosclerosis was quantified using the portable ultrasound Acuson Cypress device (Siemens Medical Solutions USA, Inc., Mountainview, CA, USA).
The Asymptomatic Carotid Artery Plaque Study (ACAPS) protocol 10 was used to quantify the degree of atherosclerotic transformation of the carotid artery. Briefly, the B-mode ultrasound was used to describe a so-called B-score: 0 (no transformation of arterial wall), 1 (wall thickness >1 mm), 2 (plaque <2 mm), 3 (plaque = 2–3 mm), 4 (plaque >3 mm) and 5 (complete luminal obstruction). A B-score >2 on any area of the carotids was classified as advanced carotid plaque.
Statistical analysis
The main variable of interest in this study is the B-score coded as an ordinal variable with six categories. An ordinal logistic regression was carried out in order to investigate the relationship between this variable and the main predictor under investigation, that is, cFLC levels adjusting for gender, age, systolic and diastolic blood pressure, HbA1c, LDL cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, hsCRP, body mass index (BMI), renal function, smoking, diabetes duration. The function ‘polr’ of the R package MASS was used to fit this ordinal logistic regression. All statistical analysis and data manipulation were carried out using the R software version 3.0.3. All hypothesis testing were carried out using an alpha = 0.05. No adjustment for multiplicity in hypothesis testing was done. We also did not use any method of data imputation and missing data on covariates and on the dependent variable were excluded from the analysis. The data were expressed as mean ± standard deviation when normally distributed and as median (interquartile range (IQR)) otherwise. Gaussian distribution was tested using the Kolmogorov–Smirnov test. Correlations between variables were calculated using Spearman’s rank coefficient test or the Pearson product-moment correlation coefficient, as appropriate.
Results
We cross-sectionally analysed data of 26 female and 49 male subjects, aged 59 ± 8 years. Their mean BMI was 31.6 ± 4.4 kg/m2, the diabetes duration was 8 ± 6 years, the median B-score of the left and right carotid artery was 2 (IQR: 0–3). Mean HbA1c was 67.0 ± 12.0 mmol/mol, and median cFLC levels was 30.2 mg/L (IQR: 24.9–39.5 mg/L).
Significant positive correlations between cFLC and the B-score (r = 0.38; p = 0.001), adjusted for age, sex and renal function, as well as for hsCRP (r = 0.35; p = 0.002) were observed. The results of fitting the ordinal logistic regression show a significant positive association between cFLC and the B-score. The adjusted odds ratio for a half standard deviation increase in cFLC was 1.45 and was significant (p = 0.028) even after adjustment for hsCRP. Table 1 displays the adjusted odds ratios along with their corresponding 95% confidence intervals (CI) of the ordinal regression model.
Results of fitting of the multiple ordinal logistic regression for the B-score.
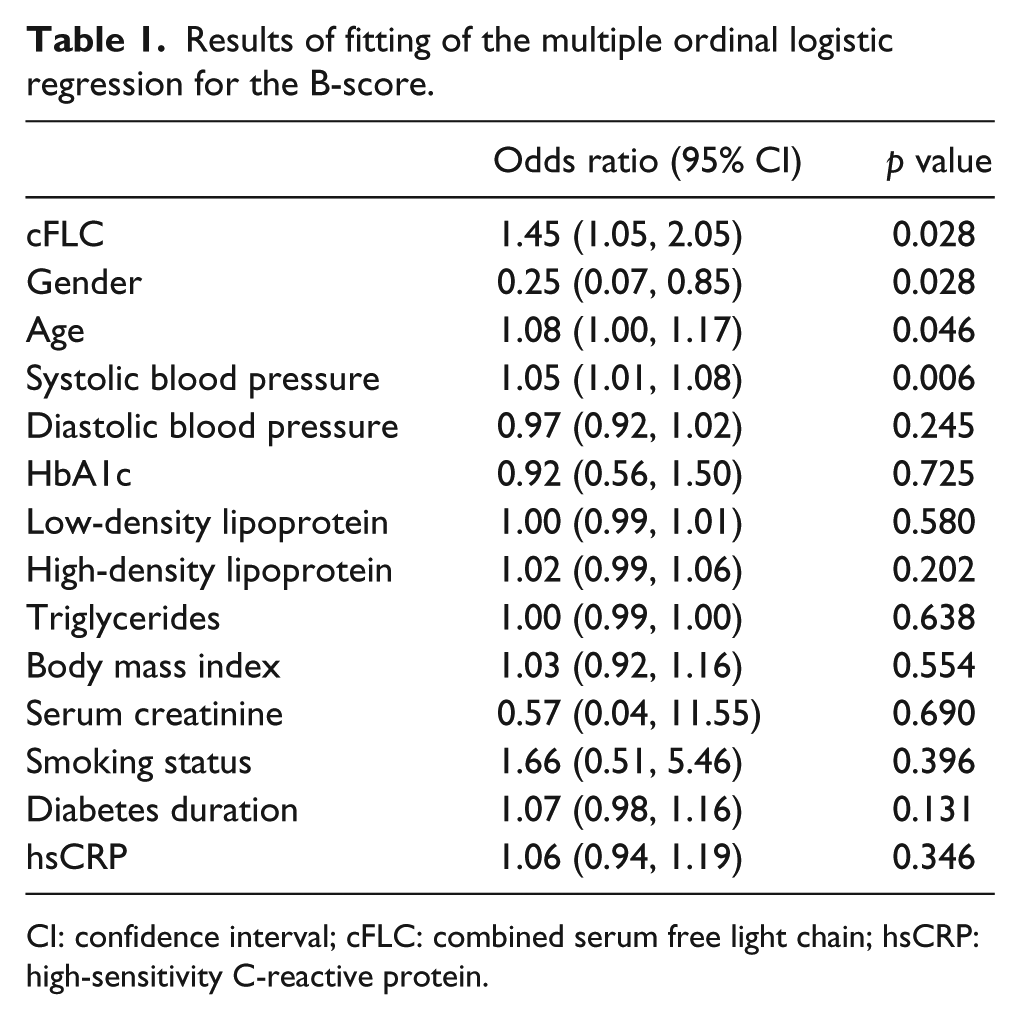
CI: confidence interval; cFLC: combined serum free light chain; hsCRP: high-sensitivity C-reactive protein.
Discussion
Aim of this cross-sectional analysis was to investigate serum free light chains as a biomarker for atherosclerosis. We showed that cFLC levels are independently associated with the extend of carotid atherosclerosis in subjects with established T2DM and are therefore extending the work of Bellary et al. demonstrating an association of cFLC with CVD in subjects with diabetes.
Limitations of our findings are the limited patient size and therefore, further prospective validation studies are needed to determine the future role of cFLC as a potential predictive biomarker for atherosclerosis and CVD in T2DM. Moreover, our research only analysed the association of cFLC with atherosclerosis cross-sectionally; hence, research focusing on whether or not interventions targeting chronic inflammation will have an impact on cardiovascular outcome like the currently ongoing Canakinumab Anti-inflammatory Thrombosis Outcome Study (CANTOS) 11 targeting inflammation in atherosclerotic disease could also help clarifying the value of cFLC as a future biomarker.
Footnotes
Acknowledgements
The Binding Site provided assay reagents (Freelite®) free of charge but did not assume any other role in the conduct of the study. F.A. and N.J.T. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This project was supported by unrestricted research grants from AstraZeneca Austria, MSD, NovoNordisk Austria, Takeda Austria, the Jubileumsfond of the Austrian National bank (project number 13699) and the Future Fund of the Styrian Government and the COMET1 center CBmed, funded by the FFG, SFG and WAW.