
Abstract
Objective:
Determine the prevalence of diabetes using 2-h plasma glucose among people who otherwise would be categorized as having prediabetes based on A1c and fasting glucose, and to determine whether those people were more likely to have cardiometabolic risk factors.
Methods:
Among 3644 adults with prediabetes based on A1c and fasting glucose in the 2005–2014 National Health and Nutrition Examination Survey, a cross-sectional survey of the US general population, we estimated the percentage who would be categorized as having diabetes based on having a 2-h plasma glucose ⩾200 mg/dL. We calculated odds ratios of cardiometabolic risk factors associated with having 2-h plasma glucose ⩾200 mg/dL.
Results:
A total of 6.9% would be categorized as having diabetes based on 2-h plasma glucose. The adjusted odds ratios (95% confidence interval) associated with having 2-h plasma glucose ⩾200 mg/dL were significant for total hypertension (2.06, 1.35–3.14), high triglycerides (1.64, 1.10–2.44), low high-density lipoprotein cholesterol (1.55, 1.01–2.39), albuminuria (2.05, 1.33–3.14) and elevated alanine aminotransferase (1.78, 1.09–2.91), but not for other cardiometabolic risk factors.
Conclusion:
A total of 6.9% of people categorized as having prediabetes based on A1c and fasting glucose would be categorized as having diabetes based on 2-h plasma glucose. They were more likely to have hypertension, high triglycerides, low high-density lipoprotein cholesterol, albuminuria and elevated alanine aminotransferase.
Introduction
The American Diabetes Association (ADA) recommends diabetes being diagnosed based on one of three markers: glycated haemoglobin (A1c), fasting plasma glucose (FPG) or 2-h plasma glucose (2HPG) after an oral glucose tolerance test (OGTT). 1 The ADA recommends repeat testing in clinical settings but has not expressed a preference for any one marker. The three markers are not perfectly aligned in that each will identify a different subset of diabetes. Although 2HPG was previously considered a ‘gold standard’ in the diagnosis of diabetes, it is currently used infrequently in clinical practice or research because the OGTT is more time-consuming, costly and burdensome to administer and for the patient to undergo. 2 However, an increase in postprandial glucose concentration is considered more sensitive because it usually occurs before an increase in fasting glucose. 2 In the US general population, the prevalence of undiagnosed diabetes increased from 3.1% when based on only A1c and FPG to 5.2% when additionally including 2HPG as a criterion. 3 This suggests that there may be many cases of diabetes that are missed since 2HPG is not routinely measured. This may have important public health implications since diabetes is a well-established risk factor for cardiovascular disease (CVD), microvascular complications and other health outcomes,4,5 and early detection and treatment is important for reducing the risk of complications.
The objective of our analysis was to determine the prevalence of diabetes using 2HPG as a criterion among people who would otherwise be categorized as having prediabetes based on A1c and FPG. Additionally, among people who would be categorized as having prediabetes based on A1c and FPG, we determined the association between having 2HPG above the diabetes cut point and cardiometabolic risk factors, including total hypertension, undiagnosed hypertension, high low-density lipoprotein (LDL) cholesterol, high triglycerides, low high-density lipoprotein (HDL) cholesterol, previous history of CVD, chronic kidney disease (CKD), albuminuria and elevated alanine aminotransferase (ALT). To do so, we used data from the 2005–2014 National Health and Nutrition Examination Survey (NHANES), a cross-sectional sample of the US general population.
Methods
Study population
NHANES was a stratified multistage sample of the civilian noninstitutionalized US population that was conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC). 6 NHANES has collected data continuously in 2-year cycles since 1999. We limited our analysis to 2005–2014 because those were the only years in which an OGTT was administered to participants. The examination response rate for the 2-year cycles ranged from 69% to 77%. 7 Participants were randomly selected to participate in either a fasting morning examination or an afternoon/evening examination. Eligible participants from the morning examination were administered an OGTT (excluding those with haemophilia, with recent chemotherapy, who used diabetes medications, pregnant women and those who refused). We used data from the OGTT-administered sample for our analysis. Of 10,480 adults ⩾20 years of age, we excluded people with diagnosed diabetes (n = 1391), those who did not meet the A1c or FPG prediabetes criteria (n = 5173), people who self-reported liver disease (n = 69), people who self-reported undergoing dialysis in the past year (n = 5) and those taking opioid medications (n = 198), resulting in a final sample of 3644 participants. Thus, these are individuals with neither diagnosed diabetes, an A1c ⩾6.5%, nor an FPG ⩾126 mg/dL, but with an A1c value of 5.7%–6.5% and/or an FPG value of 100–126 mg/dL.
The protocol for the 2005–2014 NHANES was approved by the NCHS research ethics board. All participants gave written informed consent.
Data collection
During an in-home interview, NHANES participants were administered standardized questionnaires to collect data on age, race/ethnicity, sex, education, household income, smoking status, alcohol consumption and medication usage. In addition, participants were asked if a doctor or other health professional had ever told them that they had a heart attack or a stroke or have heart failure, coronary heart disease or angina; those who reported any of these conditions were considered to have a history of CVD.
During a visit to the mobile examination centre, participants had their height and weight measured and body mass index (BMI) was calculated as weight in kilograms divided by height in metres squared. Waist circumference was measured at the iliac crest, and we defined abdominal obesity as a waist circumference >102 cm in men and >88 cm in women. Blood pressure was measured up to three times in participants and, after excluding the first measurement, we defined hypertension as an average systolic blood pressure ⩾140 mm Hg, an average diastolic blood pressure ⩾90 mm Hg or current use of antihypertensive medication. We defined undiagnosed hypertension as participant self-report of never receiving a diagnosis of hypertension from a doctor and having either an average systolic blood pressure ⩾140 mm Hg or an average diastolic blood pressure ⩾90 mm Hg.
After fasting 8–24 h overnight, a trained phlebotomist obtained a blood sample according to a standardized protocol. Total cholesterol, HDL cholesterol and triglycerides were measured, and LDL cholesterol was estimated based on the Friedewald equation. 8 Low HDL cholesterol was defined as levels <40 mg/dL in men and <50 mg/dL in women. High triglycerides were defined as levels ⩾150 mg/dL. High LDL cholesterol was defined as having levels ⩾100 mg/dL or use of lipid-lowering medication. Serum creatinine was measured using the Jaffe rate method, and we calculated estimated glomerular filtration rate (eGFR) using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. 9 Participants were considered to have CKD if they had an eGFR <60 mL/min/1.73 m2. Urine albumin and creatinine were measured, and albuminuria was defined as having urine albumin ⩾30 mg/g of creatinine. ALT was measured, and we categorized men >43 IU/L and women >31 IU/L as having elevated levels (cut points based on the 95th percentiles among those with low risk of liver injury: no hepatitis, alcohol consumption ⩽two drinks/day for men and ⩽one drink/day for women, BMI <25 kg/m2, waist circumference ⩽102 cm for men and ⩽88 cm for women, no diagnosed diabetes and A1c <6.5%). 10
Immediately after a blood sample was obtained to measure A1c and FPG, an OGTT was administered to participants. The OGTT included a calibrated dose (75 g) of glucose and a venipuncture 2 h (plus or minus 15 min) later to obtain a blood sample. 2HPG was measured by a hexokinase method using a Roche/Hitachi 911 Analyzer (2005–2006), a Roche/Hitachi Modular P Chemistry Analyzer (2007–2012) and a Roche/Hitachi Cobas C Chemistry Analyzer (2013–2014) (Roche Diagnostics, Indianapolis, IN, USA). The interassay coefficient of variation ranged from 0.9% to 2.6%.
Statistical analysis
We calculated means and percentages of participant characteristics for those with 2HPG below and above 200 mg/dL. We then estimated the percentage with 2HPG ⩾200 mg/dL overall and stratified by participant characteristics, calculating p values for differences by participant characteristics using pairwise t-tests. We used logistic regression to estimate the odds ratios and 95% confidence intervals (CIs) of cardiovascular risk factors including total hypertension, undiagnosed hypertension, high LDL cholesterol, high triglycerides, low HDL cholesterol, history of CVD, CKD, albuminuria and elevated ALT, in separate models, associated with having a 2HPG ⩾200 mg/dL. We adjusted for the potential effects of sociodemographic and behavioural factors, in order to ascertain the independent association of 2HPG with CVD and CVD risk factors. Initial models were unadjusted and a subsequent model adjusted for age, race/ethnicity and sex. A final model additionally included education, income, smoking status, alcohol and BMI. We repeated the analysis among people (N = 4494) who would be classified as having normal glucose based on A1c (<5.7%) and FPG (<100 mg/dL), and investigated those above the prediabetes cut point for 2HPG (⩾140 mg/dL).
For all analyses, we used OGTT sample weights to account for unequal probabilities of selection and non-response so that the results were representative of the total civilian noninstitutionalized US population. Data analyses were conducted using SUDAAN (version 10.0.1; RTI International, Research Triangle Park, NC, USA) accounting for the stratified, clustered sample design used by NHANES.
Results
Participant characteristics
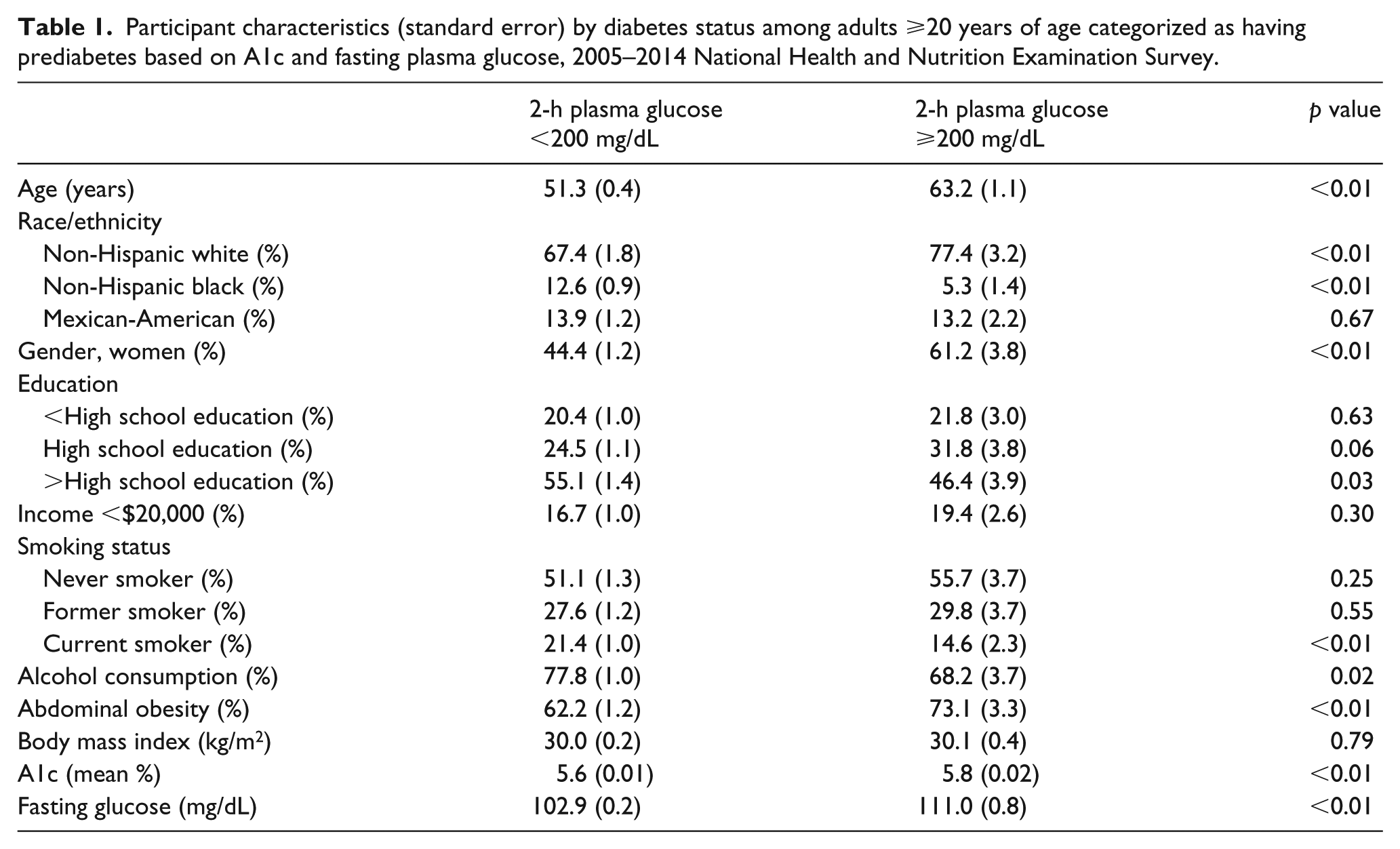
People with 2HPG ⩾200 mg/dL (compared to those with 2HPG <200 mg/dL) were older (63.2 years compared to 51.3 years), more likely to be non-Hispanic white (77.4% compared to 67.4%) and female (61.2% compared to 44.4%) (Table 1). They were less likely to have more than a high school education (46.4% compared to 55.1%), to currently smoke (14.6% compared to 21.4%) and to consume alcohol (68.2% compared to 77.8%); these differences were explained by the difference in age. There was no difference by income or BMI, but those with 2HPG ⩾200 mg/dL were more likely to have abdominal obesity (73.1% compared to 62.2%). People with 2HPG ⩾200 mg/dL had a higher mean A1c (5.8% compared to 5.6%) and fasting glucose (111.0 mg/dL compared to 102.9 mg/dL).
Participant characteristics (standard error) by diabetes status among adults ⩾20 years of age categorized as having prediabetes based on A1c and fasting plasma glucose, 2005–2014 National Health and Nutrition Examination Survey.
Prevalence of diabetes
Among the overall population of people who would be classified as having prediabetes based on A1c and FPG, the percentage (95% CI) who would be categorized as having diabetes based on 2HPG (⩾200 mg/dL) was 6.9% (6.0–7.9) (Table 2). This increased with age and was 15.0% (12.4–18.0) among people ⩾65 years of age. It was lower among non-Hispanic blacks (3.0%) compared to non-Hispanic whites (7.8%) and higher among women (9.2%) compared to men (4.9%). It was lower among people who currently smoke (4.8%; compared with 7.4% among those who have never smoked) and consume alcohol (6.1% vs 9.7%). The percentage with 2HPG ⩾200 mg/dL was higher in those with abdominal obesity, with higher levels of A1c and FPG, and with both A1c and FPG above the prediabetes cut point.
Weighted percent with 2-h plasma glucose ⩾200 mg/dL overall and stratified by participant characteristics among adults ⩾20 years of age categorized as having prediabetes based on A1c and fasting plasma glucose, 2005–2014 National Health and Nutrition Examination Survey.
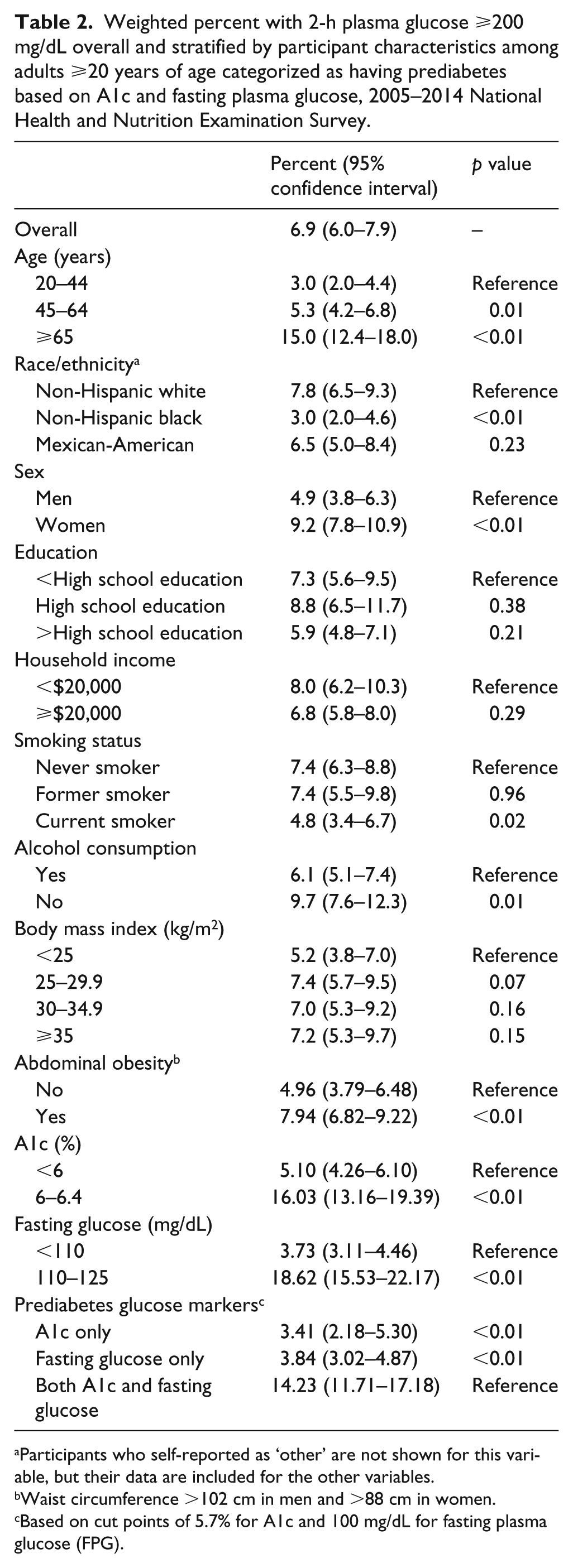
Participants who self-reported as ‘other’ are not shown for this variable, but their data are included for the other variables.
Waist circumference >102 cm in men and >88 cm in women.
Based on cut points of 5.7% for A1c and 100 mg/dL for fasting plasma glucose (FPG).
Association with cardiometabolic risk factors
Among those classified as having prediabetes based on A1c or FPG, having a 2HPG ⩾200 mg/dL was associated with total hypertension (odds ratio 3.46, 95% CI 2.45–4.89), undiagnosed hypertension (odds ratio 3.02, 95% CI 1.68–5.42), high triglycerides (odds ratio 1.57, 95% CI 1.13–2.19), previous CVD (odds ratio 2.15, 95% CI 1.49–3.09), CKD (odds ratio 3.36, 95% CI 2.29–4.95) and albuminuria (odds ratio 3.00, 95% CI 2.05–4.38), but not with high LDL cholesterol, low HDL cholesterol or elevated ALT in unadjusted models (Table 3). After multivariable adjustment, having a 2HPG ⩾200 mg/dL was associated with total hypertension (odds ratio 2.06, 95% CI 1.35–3.14), high triglycerides (odds ratio 1.64, 95% CI 1.10–2.44), low HDL cholesterol (odds ratio 1.55, 95% CI 1.01–2.39), albuminuria (odds ratio 2.05, 95% CI 1.33–3.14) and elevated ALT (odds ratio 1.78, 95% CI 1.09–2.91), but not with undiagnosed hypertension, high LDL cholesterol, history of CVD or CKD.
Odds ratios (95% CIs) of cardiometabolic risk factors associated with having 2-h plasma glucose ⩾200 mg/dL among adults ⩾20 years of age categorized as having prediabetes based on A1c and fasting plasma glucose, 2005–2014 National Health and Nutrition Examination Survey.
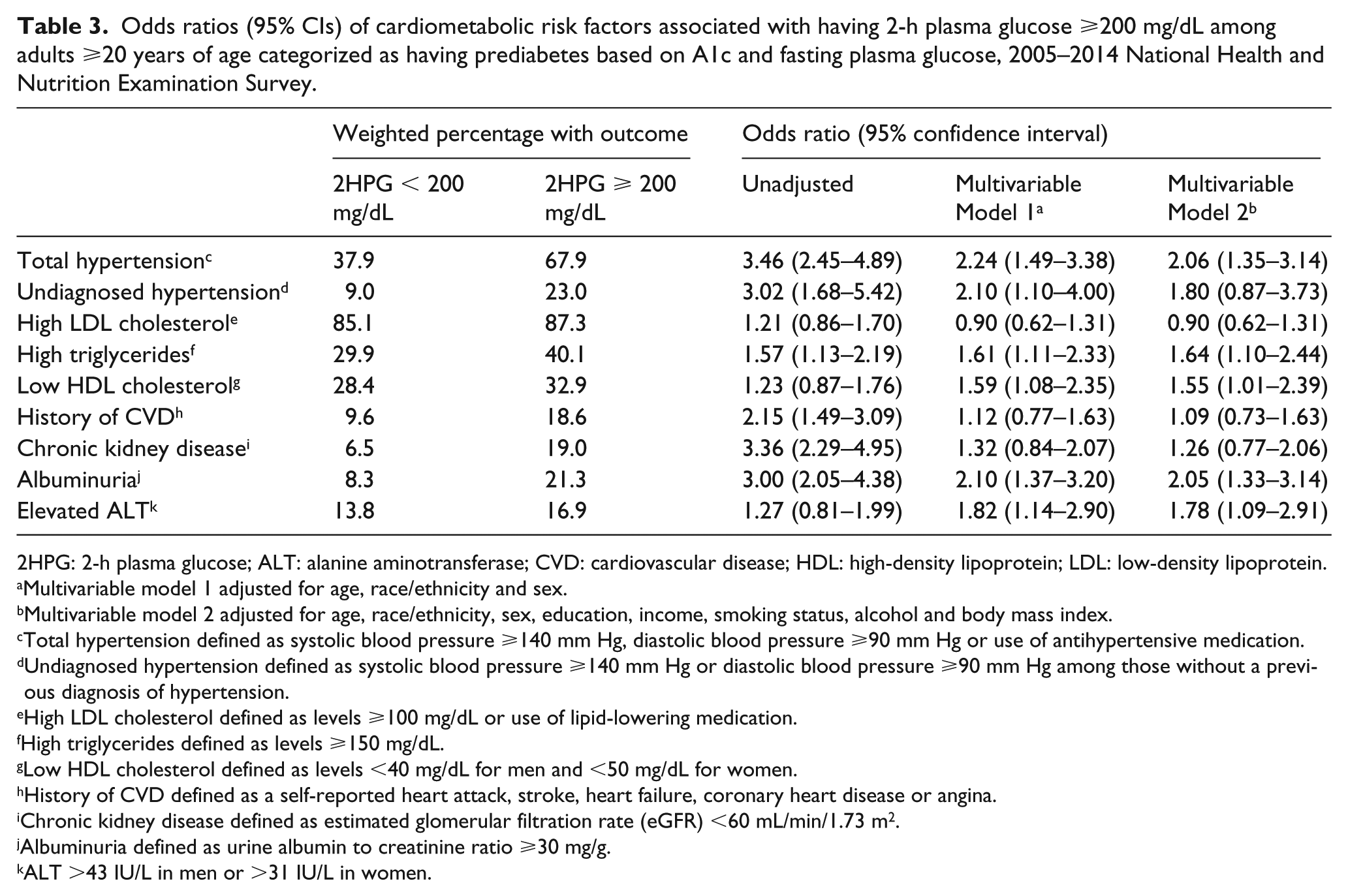
2HPG: 2-h plasma glucose; ALT: alanine aminotransferase; CVD: cardiovascular disease; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
Multivariable model 1 adjusted for age, race/ethnicity and sex.
Multivariable model 2 adjusted for age, race/ethnicity, sex, education, income, smoking status, alcohol and body mass index.
Total hypertension defined as systolic blood pressure ⩾140 mm Hg, diastolic blood pressure ⩾90 mm Hg or use of antihypertensive medication.
Undiagnosed hypertension defined as systolic blood pressure ⩾140 mm Hg or diastolic blood pressure ⩾90 mm Hg among those without a previous diagnosis of hypertension.
High LDL cholesterol defined as levels ⩾100 mg/dL or use of lipid-lowering medication.
High triglycerides defined as levels ⩾150 mg/dL.
Low HDL cholesterol defined as levels <40 mg/dL for men and <50 mg/dL for women.
History of CVD defined as a self-reported heart attack, stroke, heart failure, coronary heart disease or angina.
Chronic kidney disease defined as estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2.
Albuminuria defined as urine albumin to creatinine ratio ⩾30 mg/g.
ALT >43 IU/L in men or >31 IU/L in women.
In logistic regression models, we found significant interaction between 2HPG ⩾200 mg/dL and age for total hypertension (p = 0.01) and undiagnosed hypertension (p = 0.03) and marginally significant interaction with elevated ALT (p = 0.05). Therefore, we repeated the analysis for those three outcomes after stratifying by age and found that the odds ratios were higher in younger age groups (Figure 1). Among those 20–44 years of age (N = 1088), the multivariable adjusted odds ratios (95% CI) associated with having a 2HPG ⩾200 mg/dL were 4.65 (1.85–11.70) for total hypertension, 8.76 (2.23–34.37) for undiagnosed hypertension and 3.22 (1.03–10.06) for elevated ALT. Among those 45–64 years of age and ⩾65 years of age, the associations were attenuated and generally not significant.
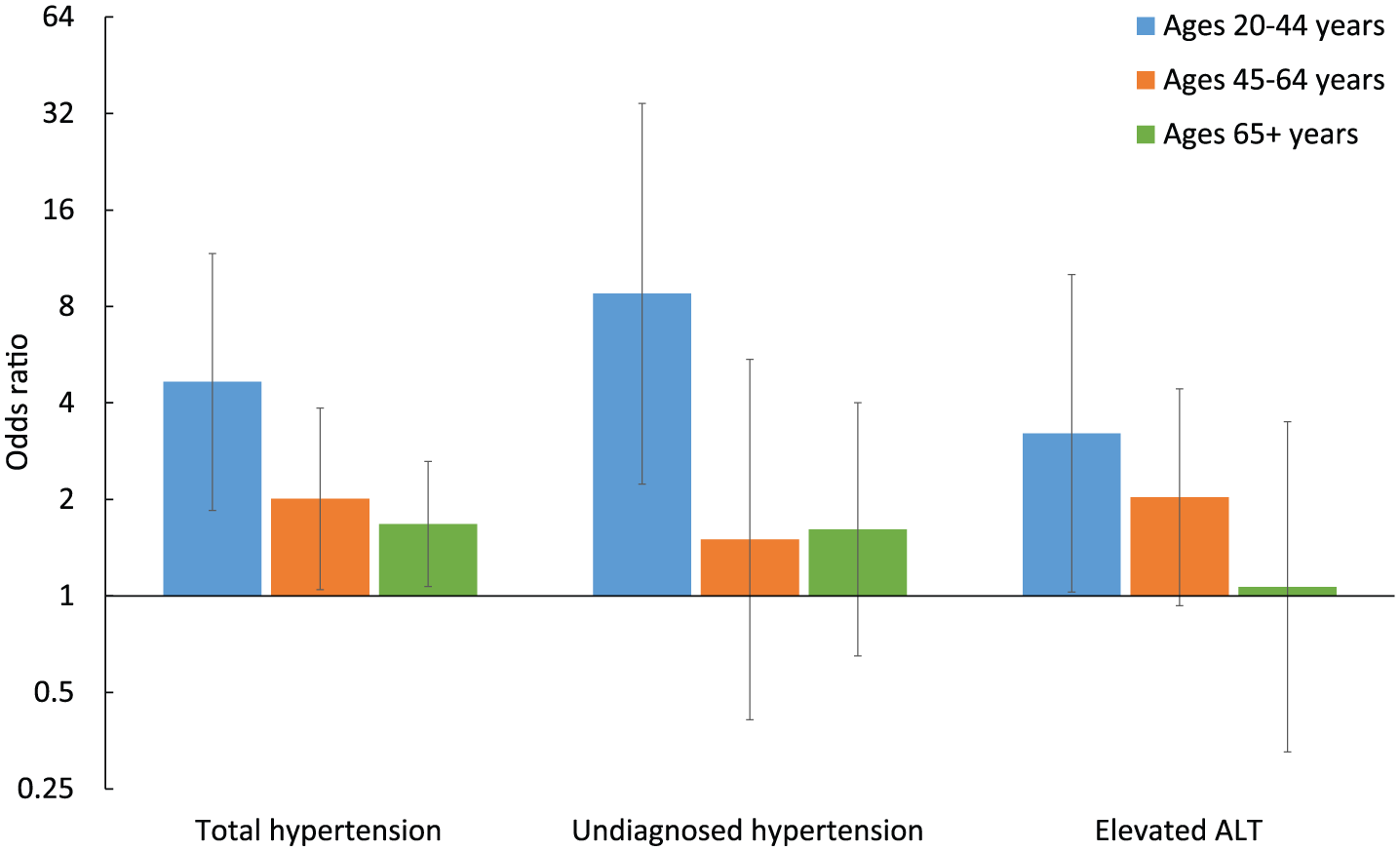
Age-stratified adjusted odds ratios (95% CIs) of total hypertension, undiagnosed hypertension and elevated ALT associated with having 2-h plasma glucose ⩾200 mg/dL among adults ⩾20 years of age categorized as having prediabetes based on A1c and fasting plasma glucose, 2005–2014 National Health and Nutrition Examination Survey. Adjusted for age, race/ethnicity, sex, education, income, smoking status, alcohol and body mass index. Error bars represent 95% CIs.
Prediabetes defined by 2-h glucose
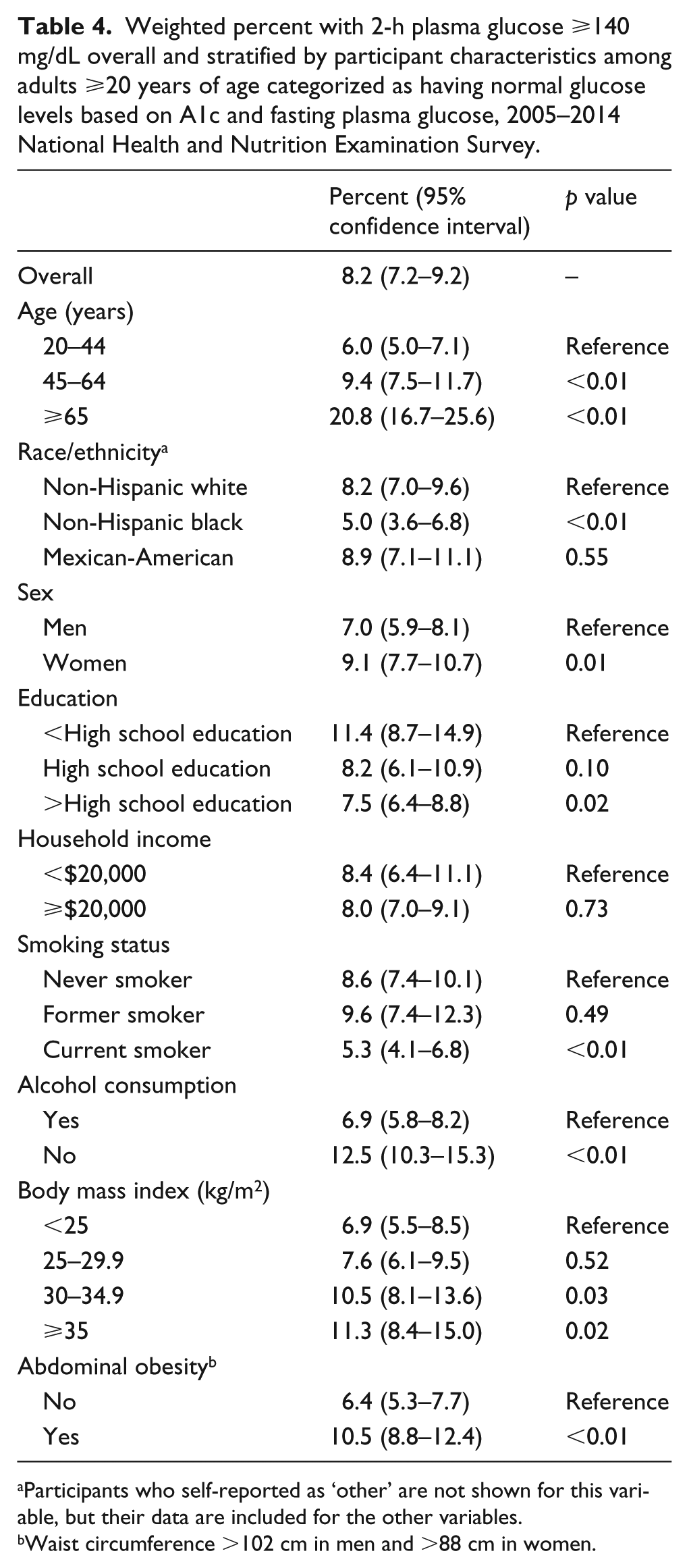
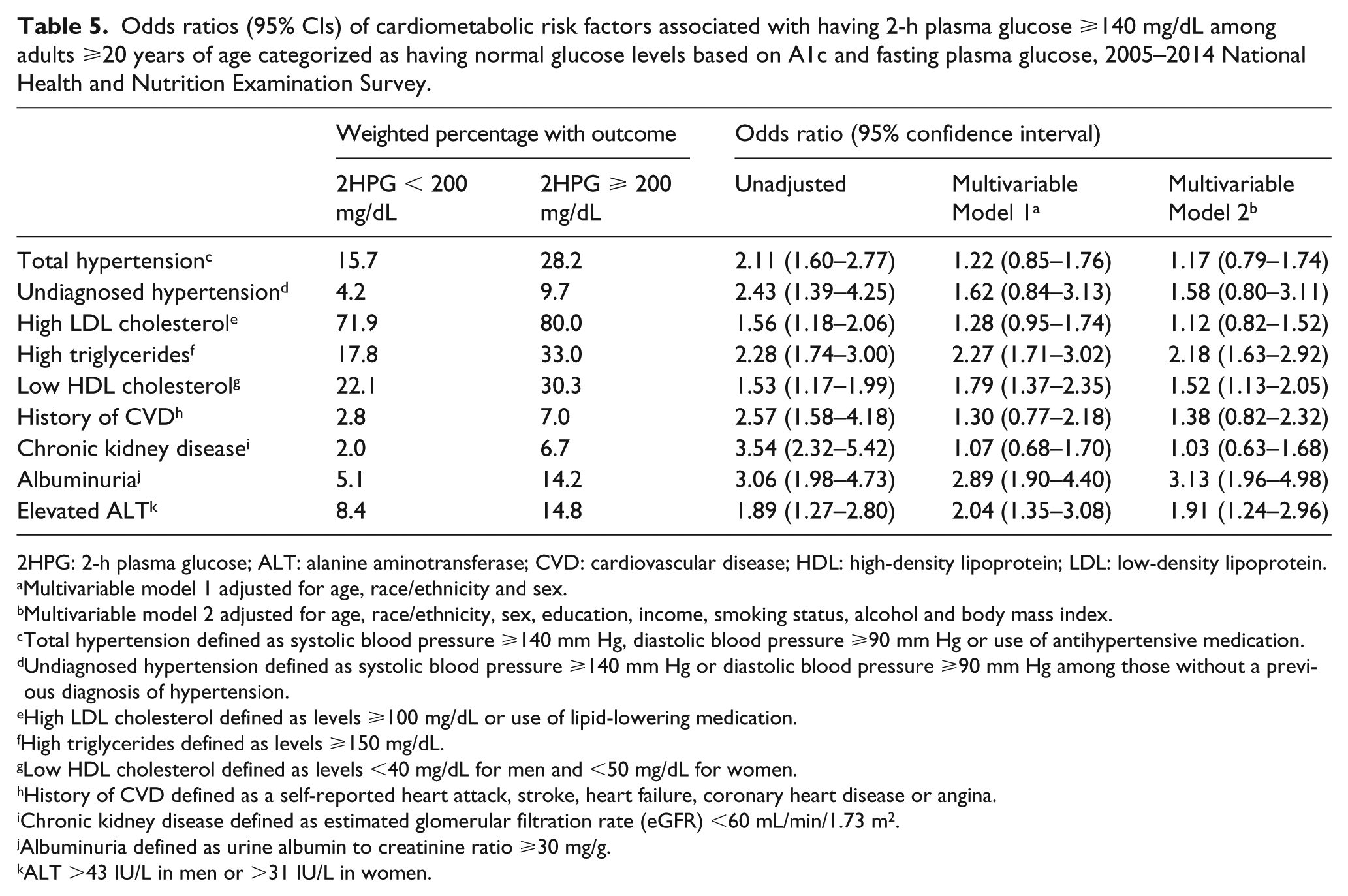
In a secondary analysis, we focused on a population who would be categorized as having normal glucose based on A1c (<5.7%) and FPG (<100 mg/dL). The percentage (95% CI) who had prediabetes based on a 2HPG ⩾140 mg/dL was 8.2% (7.2–9.2) overall (including 0.5% with 2HPG ⩾200 mg/dL), and differences by participant characteristics were generally consistent with differences in the percentage ⩾200 mg/dL in the main analysis (Table 4). After multivariable adjustment, having 2HPG ⩾140 mg/dL was not associated with total or undiagnosed hypertension, high LDL cholesterol, previous CVD and CKD (Table 5). However, the odds ratios (95% CI) associated with high triglycerides was 2.18 (1.63–2.92), low HDL cholesterol was 1.52 (1.13–2.05), albuminuria was 3.13 (1.96–4.98) and elevated ALT was 1.91 (1.24–2.96).
Weighted percent with 2-h plasma glucose ⩾140 mg/dL overall and stratified by participant characteristics among adults ⩾20 years of age categorized as having normal glucose levels based on A1c and fasting plasma glucose, 2005–2014 National Health and Nutrition Examination Survey.
Participants who self-reported as ‘other’ are not shown for this variable, but their data are included for the other variables.
Waist circumference >102 cm in men and >88 cm in women.
Odds ratios (95% CIs) of cardiometabolic risk factors associated with having 2-h plasma glucose ⩾140 mg/dL among adults ⩾20 years of age categorized as having normal glucose levels based on A1c and fasting plasma glucose, 2005–2014 National Health and Nutrition Examination Survey.
2HPG: 2-h plasma glucose; ALT: alanine aminotransferase; CVD: cardiovascular disease; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
Multivariable model 1 adjusted for age, race/ethnicity and sex.
Multivariable model 2 adjusted for age, race/ethnicity, sex, education, income, smoking status, alcohol and body mass index.
Total hypertension defined as systolic blood pressure ⩾140 mm Hg, diastolic blood pressure ⩾90 mm Hg or use of antihypertensive medication.
Undiagnosed hypertension defined as systolic blood pressure ⩾140 mm Hg or diastolic blood pressure ⩾90 mm Hg among those without a previous diagnosis of hypertension.
High LDL cholesterol defined as levels ⩾100 mg/dL or use of lipid-lowering medication.
High triglycerides defined as levels ⩾150 mg/dL.
Low HDL cholesterol defined as levels <40 mg/dL for men and <50 mg/dL for women.
History of CVD defined as a self-reported heart attack, stroke, heart failure, coronary heart disease or angina.
Chronic kidney disease defined as estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2.
Albuminuria defined as urine albumin to creatinine ratio ⩾30 mg/g.
ALT >43 IU/L in men or >31 IU/L in women.
Discussion
In this representative study of the US general population, 6.9% of people categorized as having prediabetes based on the more frequent clinical use of A1c or FPG would be categorized as having diabetes based on 2HPG. After adjusting for easily assessed clinical factors, these people were more likely to have hypertension, high triglycerides, low HDL cholesterol, albuminuria and elevated ALT compared to those with a 2HPG below the diabetes cut point; the associations with hypertension and elevated ALT were stronger among younger participants. When focusing on a population that would be categorized as having normal glucose levels based on A1c and FPG, 8.2% had 2HPG above the cut point for prediabetes. These people were more likely to have high triglycerides, low HDL cholesterol, albuminuria and elevated ALT compared to those with a 2HPG below the prediabetes cut point after adjustment; the association with elevated ALT was stronger among younger participants.
The use of different ADA-recommended biomarkers (i.e. A1c, FPG7 and 2HPG) will identify a different subset of people with diabetes. Previous studies using NHANES data found that 2HPG identified substantially more people with diabetes than using only A1c and FPG.3,11 Furthermore, in a pooled analysis of nine population-based studies, using only 2HPG identified 2.7 times more cases than using only A1c including nearly all (99.8%) of the cases identified using only A1c; similarly, in a pooled analysis of 33 population-based studies, using only 2HPG identified 80% more cases than using only FPG including nearly all (98.9%) of the cases identified using only FPG. 12 While these previous studies demonstrate that using only A1c and FPG to diagnose diabetes misses a substantial number of individuals that would be diagnosed with diabetes based on 2HPG, our study quantifies it as almost 7% among those who otherwise would be categorized as having prediabetes in the US general population.
Diabetes is a well-established risk factor for CVD and is associated with numerous CVD risk factors.4,5 However, it is unclear if CVD risk differs based on which markers (i.e. A1c, FPG, 2HPG) are above the cut point for diabetes. Several studies,13–20 but not all studies,21–24 found 2HPG was more strongly associated with cardiovascular events and mortality than FPG. The pathophysiological mechanisms of abnormal glucose metabolism may differ in those with isolated elevated 2HPG and those with isolated elevated FPG, which may result in different rates of progression of glucose abnormalities.25,26 Fewer studies have compared A1c and 2HPG in association with cardiovascular events and mortality, and the results of those studies were inconsistent.13–15 We found that having a diabetic 2HPG among people who would be categorized as having prediabetes based on A1c and FPG was associated with cardiometabolic risk factors including hypertension, high triglycerides, low HDL cholesterol, albuminuria and elevated ALT; unadjusted differences in history of CVD and CKD were not significant after adjustment including age. Although those 20–44 years of age had a lower prevalence of elevated 2HPG, the association with hypertension and elevated ALT was stronger in this age group than older age groups.
The major deterrent to using 2HPG is the burden of conducting an OGTT, including having the participant fast at least 8 h prior to the appointment, consume a glucose solution that some find unpalatable and then wait for 2 h before measurement of plasma glucose. 2 The added time commitment and expense of the test need to be considered in clinical and research settings. Another important limitation of the 2HPG is the high intra-individual variability of the test, as demonstrated by a coefficient of variation of 16.7% compared to 5.7% for FPG and 3.6% for A1c. 27
The ADA suggests a repeat measurement after a positive test based on A1c, FPG or 2HPG, but we were not able to do this because NHANES participants had only one study visit. As a result, there may be some participants that were misclassified, but it is uncertain how frequently this occurred.28,29 NHANES did not collect data on the classic symptoms of hyperglycaemia. Another limitation is that the cross-sectional nature of our study did not allow us to investigate whether having diabetes based on 2HPG was associated with the development of CVD or CVD risk factors. Also, there were certain outcomes such as peripheral arterial disease, elevated C-reactive protein and microvascular outcomes that we could not investigate because we did not have data for all years of the study.
Despite these limitations, our study had a number of key strengths including the use of NHANES data, which were representative of the US noninstitutionalized, civilian population. The 2005–2014 NHANES data were collected using a rigorous study protocol that did not meaningfully vary over time and included thorough quality-control procedures and the use of technicians trained and certified in data collection. Additionally, NHANES had a large sample size that allowed us to restrict our analysis to adults who underwent an OGTT and would otherwise be classified as having prediabetes based on A1c or FPG.
The use of 2HPG among people with A1c/FPG defined prediabetes identified a substantial portion of people who would be categorized as having diabetes and these individuals were more likely to have cardiometabolic risk factors including hypertension, high triglycerides, low HDL cholesterol, albuminuria and elevated ALT. This is particularly important in groups that we found to have a relatively high prevalence of 2HPG-defined diabetes, such as those at older age, women, those with an A1c of 6.0%–6.4% and those with an FPG of 110–125 mg/dL. These findings emphasize the value of conducting OGTTs in clinical and research settings when attempting to identify new cases of diabetes. This has important public health implications considering the benefits of identifying and treating diabetes early during the course of the disease.5,30
Footnotes
Acknowledgements
A.M., K.F.R. and C.C.C. designed the study. A.M. conducted the statistical analysis and drafted the manuscript. K.F.R. and C.C.C. guided the statistical analysis and critically revised the manuscript for important intellectual content. All authors approved the final manuscript. A.M. and C.C.C. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. NANES data are available online at ![]() .
.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by a contract from the National Institute of Diabetes and Digestive and Kidney Diseases (GS00F173CA). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute of Diabetes and Digestive and Kidney Diseases.