
Abstract
Objective:
To investigate long-term prognostic importance of newly discovered glucose disturbances in patients with acute myocardial infarction (AMI).
Methods:
During 1998–2001, consecutive patients with AMI (n = 167) and healthy controls (n = 184) with no previously known diabetes were investigated with an oral glucose tolerance test (OGTT). Patients and controls were separately followed up for cardiovascular events (first of cardiovascular mortality/AMI/stroke/heart failure) during a decade.
Results:
In all, 68% of the patients and 35% of the controls had newly detected abnormal glucose tolerance (AGT). Cardiovascular event (n = 72, p = 0.0019) and cardiovascular mortality (n = 31, p = 0.031) were more frequent in patients with newly detected AGT. Regarding patients, a Cox proportional-hazard regression analysis identified AGT (hazard ratio (HR): 2.30; 95% confidence interval (CI): 1.24
Conclusion:
An OGTT at discharge after AMI disclosed a high proportion of patients with previously unknown AGT which had a significant and independent association with long-term prognosis.
Background
The global prevalence of diabetes mellitus (DM) and its forerunner impaired glucose tolerance (IGT) is rapidly increasing, and about half of the people with disturbed glucose metabolism are unaware of their condition. 1 Both diabetes and IGT are risk factors for the development of coronary artery disease causing the epidemic rise to be a threat to global health in a not-too-distant future.2–4 There is an ongoing debate regarding the most efficient test to identify people at risk. HbA1c is considered easier and more convenient to perform while an oral glucose tolerance test (OGTT) will identify more individuals at risk.5–7 In patients with acute myocardial infarction (AMI), an OGTT performed within a week after the event reveals that at least 60% of them have previously unknown abnormal glucose tolerance (AGT – either newly detected diabetes or IGT).8–10 These individuals are at increased risk for cardiovascular events during the next 1–2 years,11–13 but information on the long-term prognostic impact of screen detected AGT is lacking.
This report presents information on cardiovascular events and mortality during a decade of follow-up of the Glucose Tolerance in Patients with Acute Myocardial Infarction (GAMI) cohort 8 comprising patients with AMI without previously known AGT and matched controls. The hypothesis tested was that newly identified AGT will constitute an important prognostic marker of long-term outcome.
Research design and methods
Patients and controls
The present analysis is based on individuals included in the GAMI trial from November 1998 to December 2000. A total of 181 patients with AMI, admission capillary blood glucose of < 11.1 mmol/L and without known diabetes were prospectively enrolled when admitted to Karolinska and Västerås Hospital coronary care units. Exclusion criteria were age (>80 years) and serum creatinine (>200 µmol/L).8,11 An OGTT was performed at the day of hospital discharge, that is, 4–5 days after the AMI to be repeated after 3 and 12 months. A control group of 185 individuals matched for age, gender and catchment area and without a prior diagnosis of diabetes, cardiovascular disease apart from mild hypertension or any acute illness during the preceding 3 months was recruited to enable comparisons with the prevalence of glucose abnormalities and cardiovascular outcomes in people without cardiovascular disease. 14
All patients were treated for their AMI according to established national and international guidelines at that time. 15 None of the patients received information on the OGTT results at discharge but was referred to their ordinary physician for further management if the OGTT at 3 months indicated diabetes. Controls performed only one OGTT and were referred for further handling if this indicated diabetes.
The patients and controls were followed up until 31 December 2011. One patient and one control were lost to follow-up, and 13 patients were not investigated with an OGTT at discharge 11 due to death during hospitalisation (2), refusal (2), illness (7) or technical problems (2) leaving 167 classified patients (4 patients had overt diabetes according to several fasting glucose levels and 163 had an OGTT performed) and 184 controls as the final study cohort.
Laboratory analyses
Glucose concentration was measured in whole capillary blood immediately after sampling by means of a HemoCue® portable photometer (HemoCue AB, Ängelholm, Sweden).
HbA1c was analysed as MonoS standard by high-performance liquid chromatography on whole blood applied on filter paper (Boehringer-Mannheim Scandinavian AB, Bromma, Sweden). 16 The upper normal limit was 5.3% and the coefficients of variation <3%. The results obtained with this method can be recalculated to the International Federation of Clinical Chemistry (IFCC) standard (10.11 × MonoS − 8.90) or Diabetes Control and Complications Trial (DCCT) (0.925 × MonoS + 1.34). 17 In this article, we report values of HbA1c in MonoS and IFCC (mmol/mol) standards.
The glucometabolic state was classified according to World Health Organization (WHO) criteria
18
based on a standardised OGTT (75 g glucose in 200 mL water) during stable conditions 4–5 days after the index infarction in the patients and at enrolment of the controls. As glucose concentration was measured in whole capillary blood, normal glucose tolerance (NGT) was defined as fasting glucose of <6.1 mmol/L and 2-h post-load glucose of <7.8 mmol/L. IGT was recognised as fasting glucose of <6.1 mmol/L and 2-h post-load glucose of 7.8
Plasma lipids were measured in the fasting state by standard methods at the local laboratory. Plasma insulin and intact proinsulin were quantified with commercially available immunoassays (DAKO Ltd, Cambridgeshire, UK). Insulin resistance was estimated at a fasting steady state by homeostasis model assessment (HOMA; homeostasis model assessment of insulin resistance (HOMA-IR)).
Outcome measures and definitions
Information on cardiovascular events was derived from hospital and outpatient clinical records supplemented if possible by a telephone interview with the survivors (or close relatives when needed). Death certificates were obtained from the Swedish National Death Registry, and the cause of death given in these certificates was checked against available hospital records. Mortality reasons were categorised as cardiovascular (caused by AMI/stroke/aortic dissection or sudden death without any obvious reason), cancer or other. AMI was diagnosed according to the joint recommendations of the European Society of Cardiology (ESC) and American College of Cardiology (ACC). 19 To be accepted as a re-infarction, the time to the event had to be >72 h after the index infarction.
Stroke was defined according to WHO criteria as a neurological deficit observed by a physician and persisting >24 h without any other disease explaining the symptoms. 20 Severe congestive heart failure (CHF) was defined as necessitating hospital admission including intensified treatment. Major cardiovascular event was defined as the first occurrence (only one could be recorded) of re-infarction/AMI, stroke, severe CHF or cardiovascular death.
Statistics
Baseline characteristics are presented as median (lower and upper quartiles) for continuous and numbers and percentages for categorical variables. Only patients and controls whose glucometabolic state was classified were included in the analyses on the relation of various clinical and biochemical parameters to the occurrence of events. The comparison between patients and controls was analysed by groups and not by pair-ways comparison. The χ2 or when appropriate Fisher’s exact test and Wilcoxon rank-sum test were used to compare baseline characteristics between different glucose tolerance groups.
Cardiovascular events were analysed in patients and controls separately. The independent prediction of AGT for a future cardiovascular event was analysed in three different Cox proportional-hazard regression models. The first model included the covariates AGT and age; the second included AGT, age and previous myocardial infarction (MI) (prior to the index event); and the third model included AGT, age, body mass index (BMI) and previous (prior to the index event) angina pectoris/MI/coronary artery bypass graft (CABG)/CHF. It was estimated that with a number of events of 72 among patients, a total number of seven covariates could be used in the final model. Only variables recorded at admission and considered clinically relevant with a p < 0.10 and the outcome of the OGTT at discharge were introduced, while laboratory variables (e.g. HOMA and high-sensitivity C-reactive protein (hs-CRP)) and pharmacological treatment (e.g. Statins that were not randomised or given to all patients) were not included. Laboratory values were not included due to missing values reducing the numbers in the model from 167 to 123, and admission values were considered stress influenced. The same selection pattern of covariates (p < 0.10) was used in the controls. Among controls, the final multivariable model was based on all 184 individuals and included remaining variables with a p value < 0.10: age, hypertension, gender and AGT. Kaplan–Meier curves were computed to assess time to major cardiovascular event in patients and controls separately and split on those with NGT or AGT and for cardiovascular death in patients. Based on the proportionality test, the result revealed that the assumption of a proportional hazard was not violated in any of the models. A two-sided p value < 0.05 was accepted as statistically significant. All analyses were conducted using SAS statistical program (SAS version 9.2), software from SAS Institute, Cary, NC, USA.
Ethical consideration
The local ethics committee of the Karolinska Institute approved the study protocol that complies with the Declaration of Helsinki. All recruited participants provided their written informed consent for the initial study and the follow-up.
Results
Baseline characteristics
Patients
Baseline characteristics and biochemical variables by glucose tolerance category (NGT vs AGT) of the 167 patients in the final cohort are presented in Table 1. The median age was 63.5 years (interquartile range (IQR): 57
Clinical and laboratory characteristics in patients by glucose tolerance state.
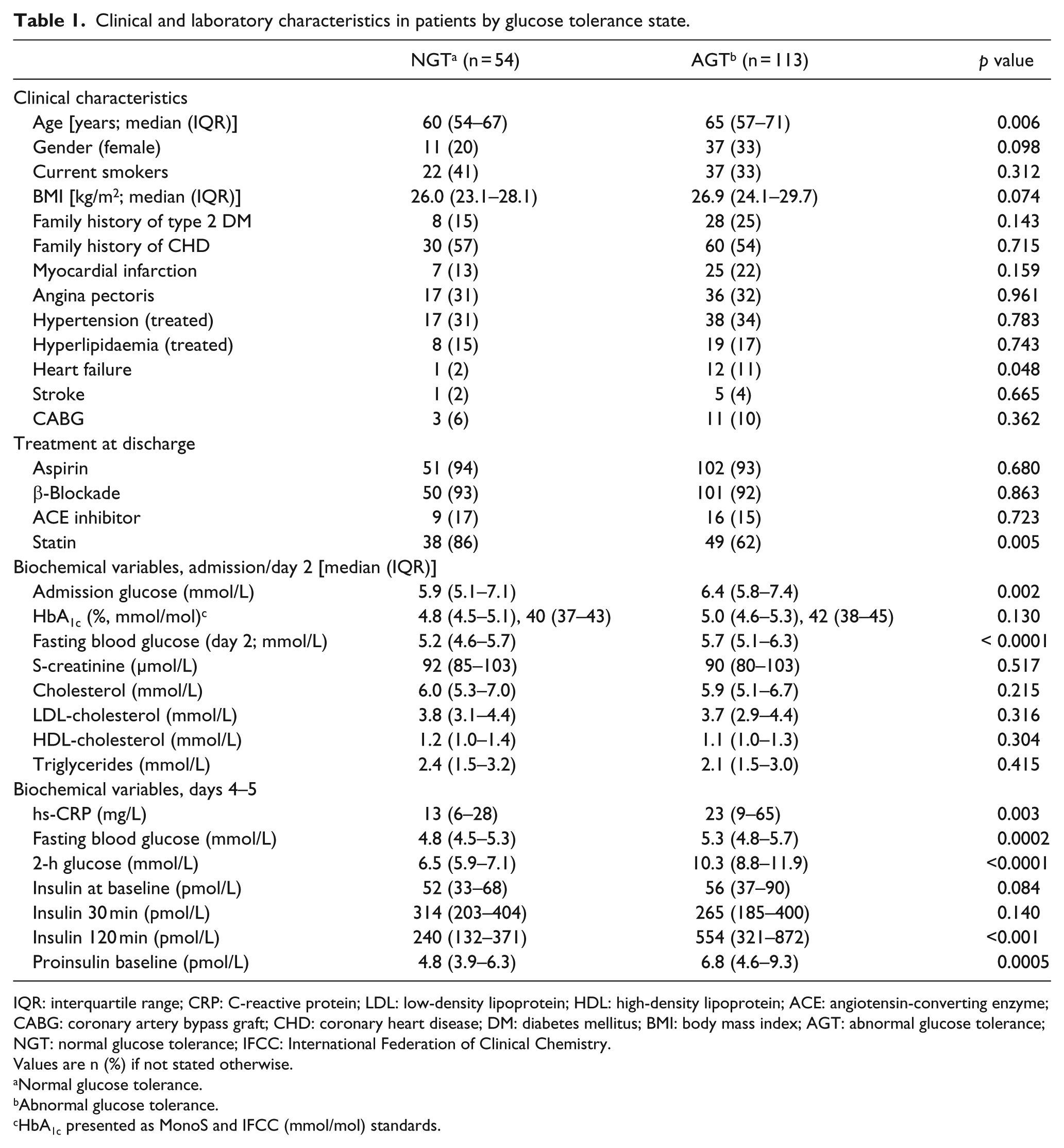
IQR: interquartile range; CRP: C-reactive protein; LDL: low-density lipoprotein; HDL: high-density lipoprotein; ACE: angiotensin-converting enzyme; CABG: coronary artery bypass graft; CHD: coronary heart disease; DM: diabetes mellitus; BMI: body mass index; AGT: abnormal glucose tolerance; NGT: normal glucose tolerance; IFCC: International Federation of Clinical Chemistry.
Values are n (%) if not stated otherwise.
Normal glucose tolerance.
Abnormal glucose tolerance.
HbA1c presented as MonoS and IFCC (mmol/mol) standards.
Controls
Baseline characteristics and biochemical variables by glucose tolerance category (NGT vs AGT) of the 184 control subjects are presented in detail in Table 2. Their median age was 64.5 years (IQR: 58–72), and 69% were males. Among controls, 119 (65%) had NGT and 65 (35%) AGT of which IGT = 45 and diabetes = 20. Controls with AGT were older (67 vs 64 years) and had more often previous hypertension than those with NGT (29% vs 12%). Biochemical variables related to glucose disturbances were significantly higher in controls with AGT.
Clinical and laboratory characteristics in controls by glucose tolerance state.
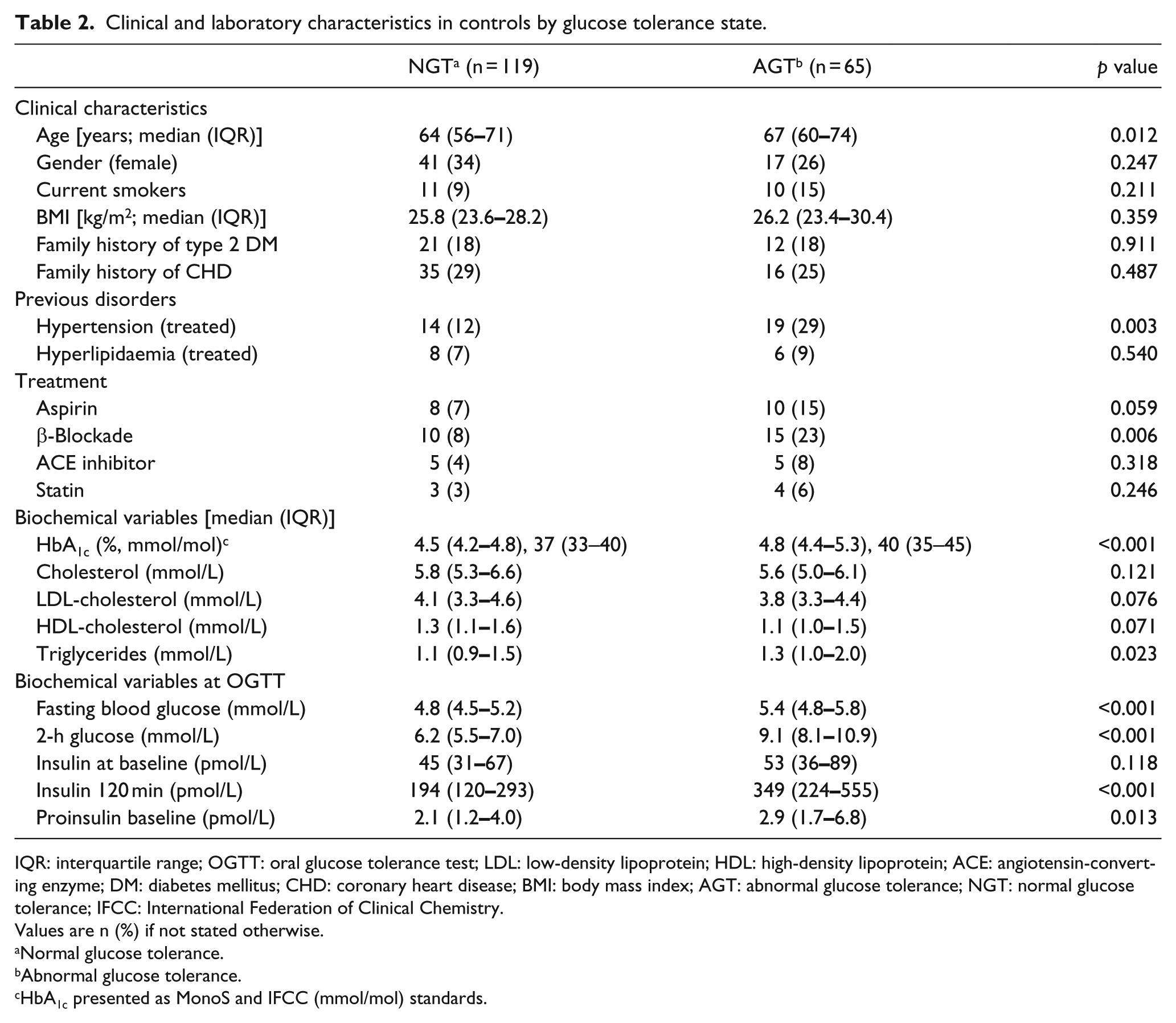
IQR: interquartile range; OGTT: oral glucose tolerance test; LDL: low-density lipoprotein; HDL: high-density lipoprotein; ACE: angiotensin-converting enzyme; DM: diabetes mellitus; CHD: coronary heart disease; BMI: body mass index; AGT: abnormal glucose tolerance; NGT: normal glucose tolerance; IFCC: International Federation of Clinical Chemistry.
Values are n (%) if not stated otherwise.
Normal glucose tolerance.
Abnormal glucose tolerance.
HbA1c presented as MonoS and IFCC (mmol/mol) standards.
Outcome regarding patients
Patients were followed during a median time of 11.6 years (IQR: 9.6–12.1). Events by glucometabolic category are presented in Table 3. Total mortality was 32% (n = 53), and 43% (n = 72) experienced a major cardiovascular event. Cardiovascular reasons were behind 58% of the deaths. Cardiovascular events were significantly more frequent in patients with AGT than among those with NGT (p = 0.0019) as was cardiovascular death (p = 0.031), while total mortality did not differ significantly (p = 0.265). Cancer mortality (28%) was significantly more prevalent in patients with NGT than among those with AGT (p = 0.017).
Events in patients and controls by glucometabolic status until death or 31 December 2011.
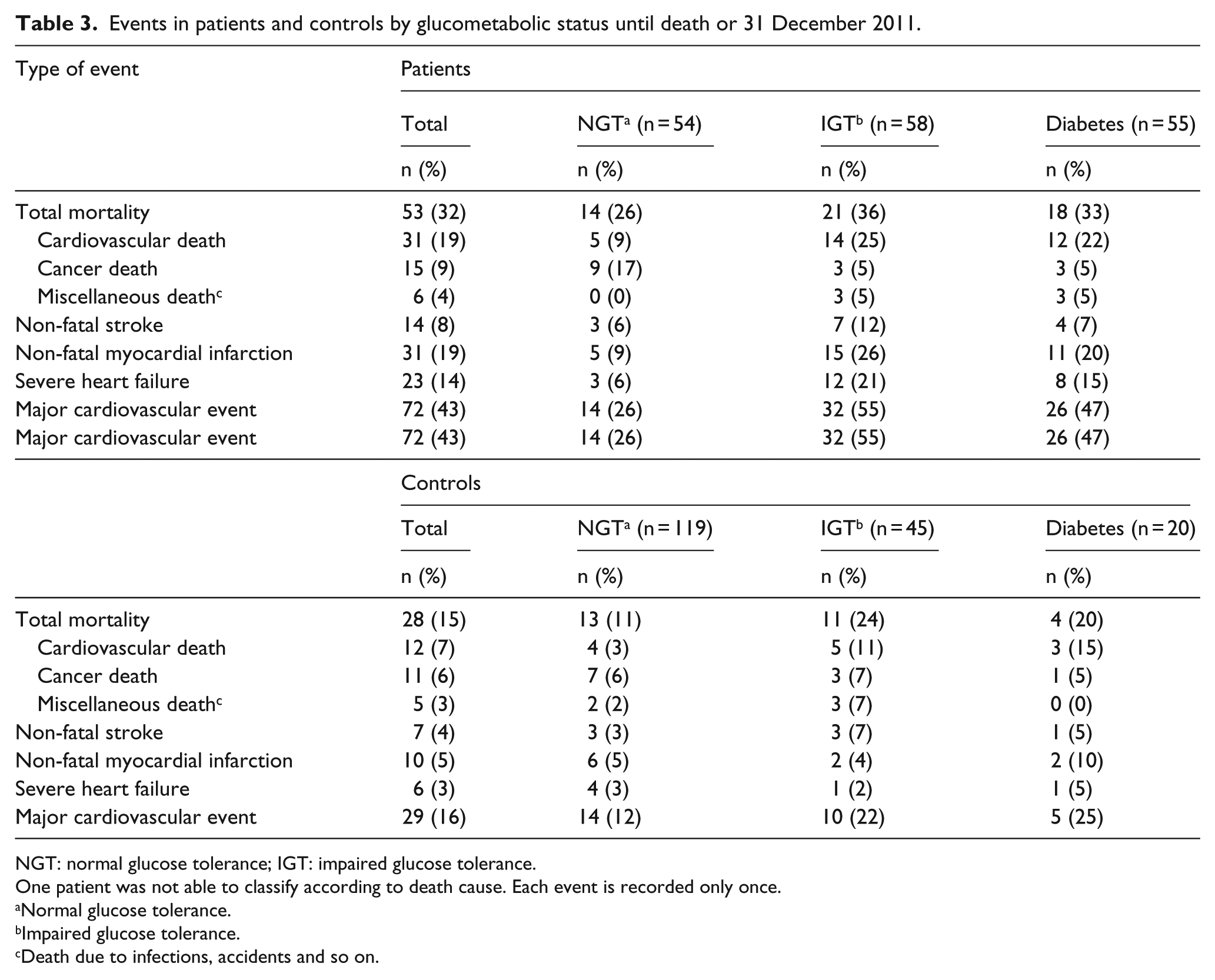
NGT: normal glucose tolerance; IGT: impaired glucose tolerance.
One patient was not able to classify according to death cause. Each event is recorded only once.
Normal glucose tolerance.
Impaired glucose tolerance.
Death due to infections, accidents and so on.
In univariate analyses, AGT was related to a major cardiovascular event (hazard ratio (HR): 2.46; 95% confidence interval (CI): 1.37
Univariate predictors for major cardiovascular event in 167 patients classified at discharge.
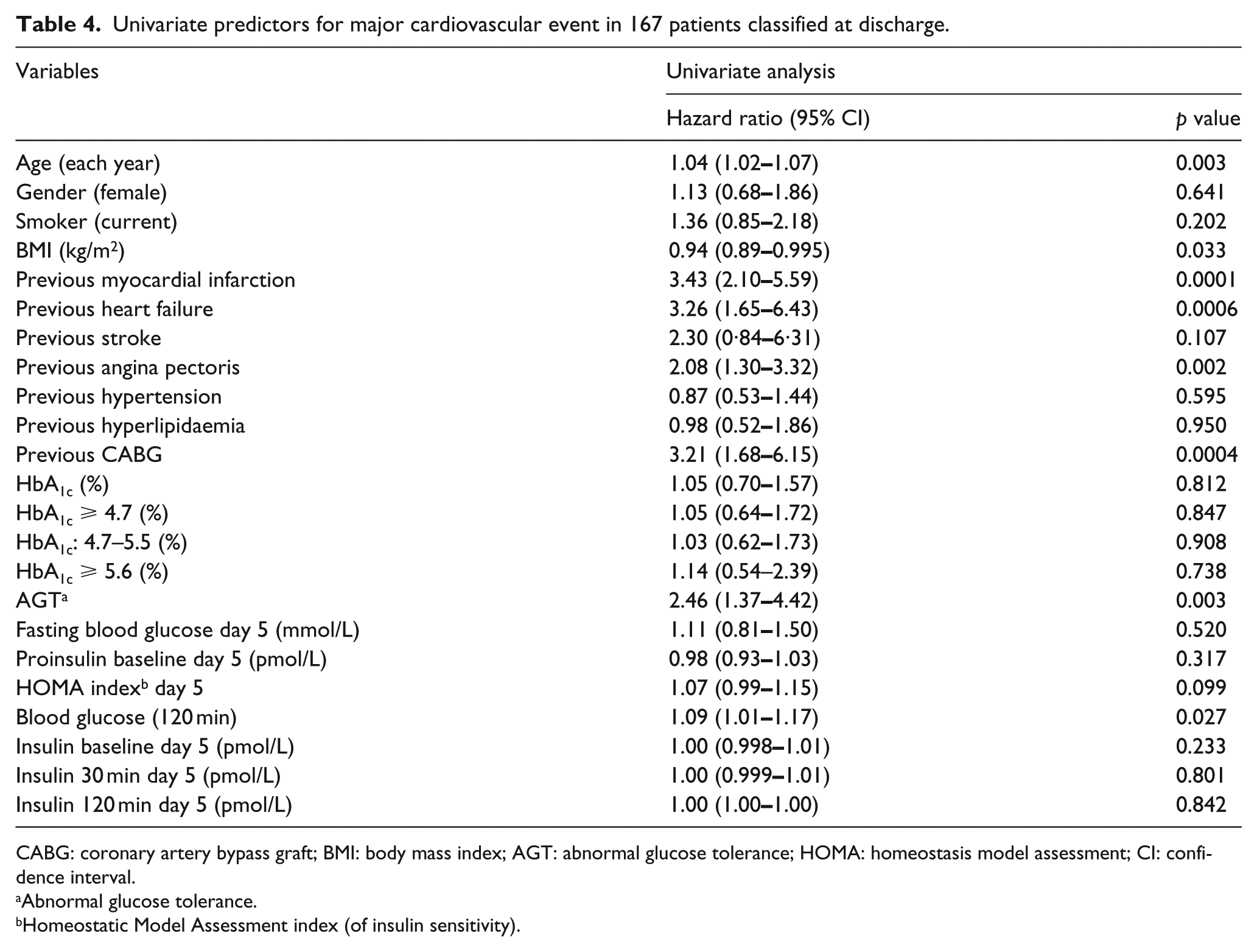
CABG: coronary artery bypass graft; BMI: body mass index; AGT: abnormal glucose tolerance; HOMA: homeostasis model assessment; CI: confidence interval.
Abnormal glucose tolerance.
Homeostatic Model Assessment index (of insulin sensitivity).
Outcome regarding controls
Controls were followed during a median time of 10.4 years (IQR: 9.9–10.7), and events by glucometabolic status are presented in Table 3. Total mortality was 15% (n = 28), and 16% (n = 29) experienced a cardiovascular event. Cardiovascular reasons were behind 42% of the deaths. Total mortality (p = 0.028), cardiovascular death (p = 0.019) and major cardiovascular event (p = 0.044) were significantly more common in controls with AGT than NGT. The proportion dying of cancer was 6% (n = 11) and did not differ between those with NGT or AGT (p = 0.941). Univariate predictors related to major cardiovascular event are shown in detail in Table 5. A Cox proportional-hazard regression model including age, gender, hypertension and AGT identified age (HR: 1.09; CI: 1.04–1.14; p = 0.0002), female gender (HR: 0.11; CI: 0.03–0.46; p = 0.003) and hypertension (HR: 3.05; CI: 1.36–6.85; p = 0.007) as remaining predictors for major cardiovascular event, while AGT did not remain as an independent predictor.
Variables in controls related to major cardiovascular event in a univariate Cox regression model.
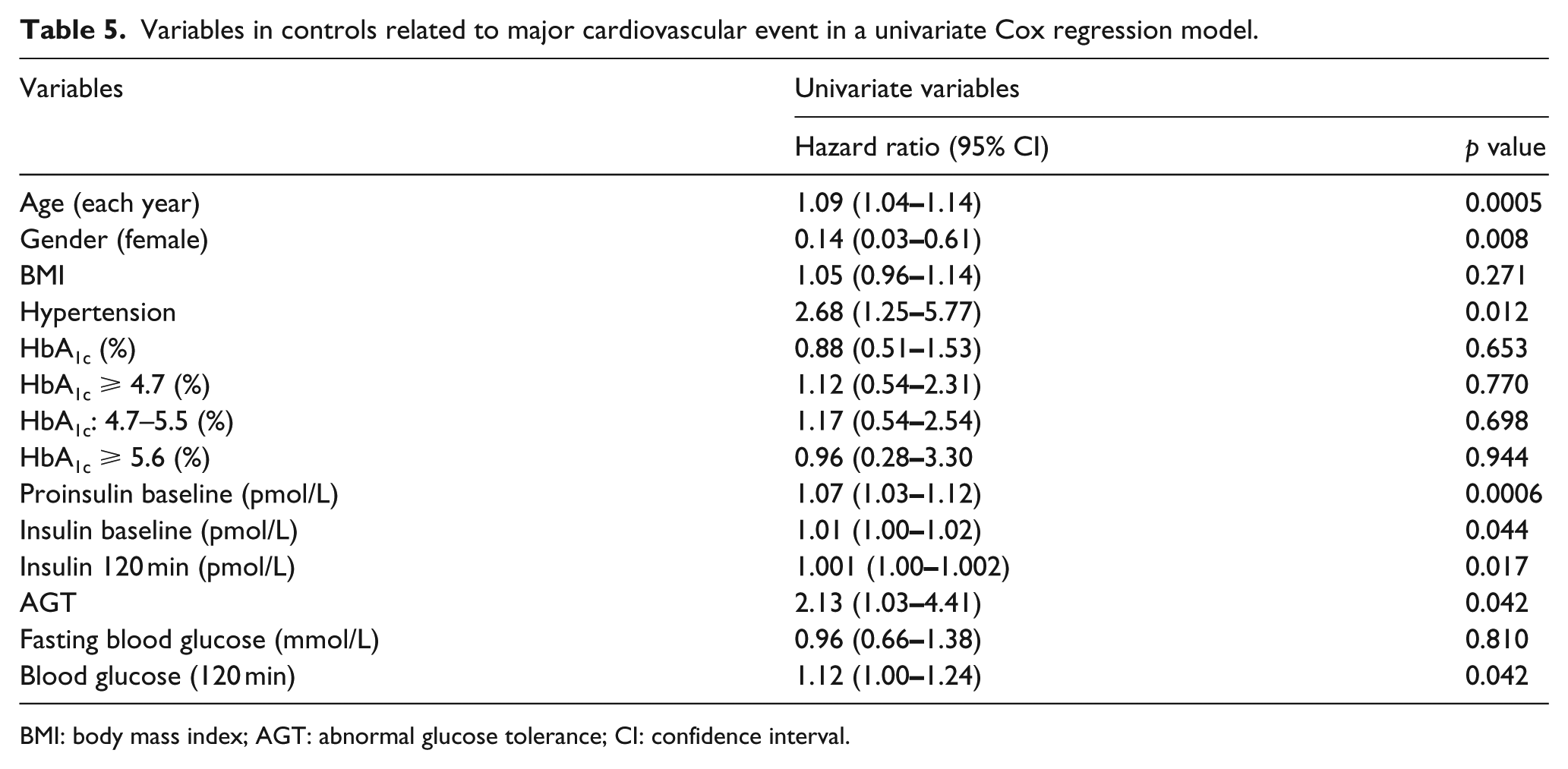
BMI: body mass index; AGT: abnormal glucose tolerance; CI: confidence interval.
Kaplan–Meier curves for patients and controls
Kaplan–Meier curves for the time to a first major cardiovascular event in patients and controls are presented together in Figure 1. The event rate was higher in patients with AGT than in those with NGT (log-rank p = 0.0018) and in controls with AGT versus those with NGT (log-rank p = 0.037). Separating patients with AGT into those with IGT and those with diabetes revealed only a negligible difference in event-free survival between these two groups (Figure 2).
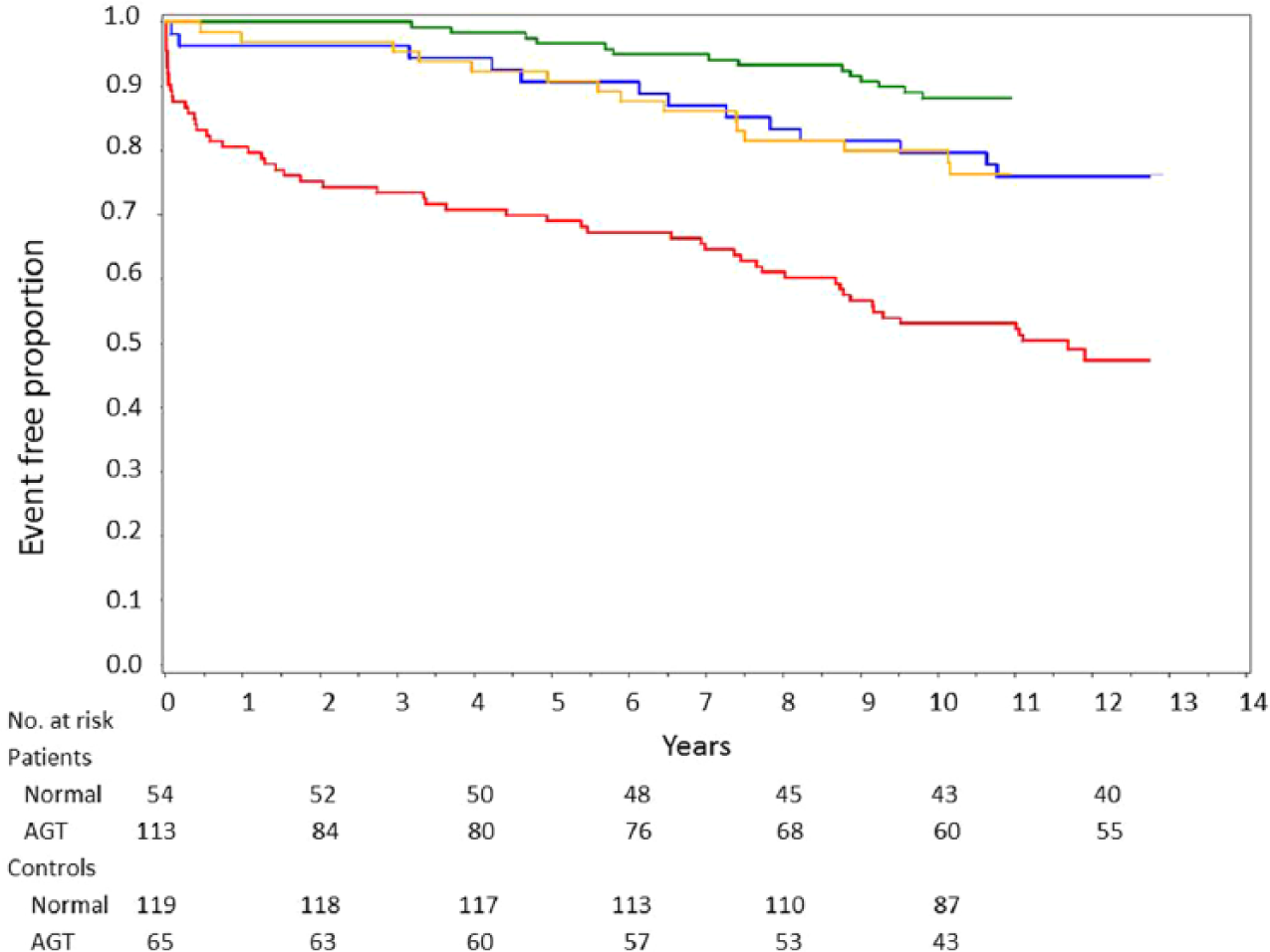
Kaplan–Meier curves showing time to a first major cardiovascular event in patients and controls.
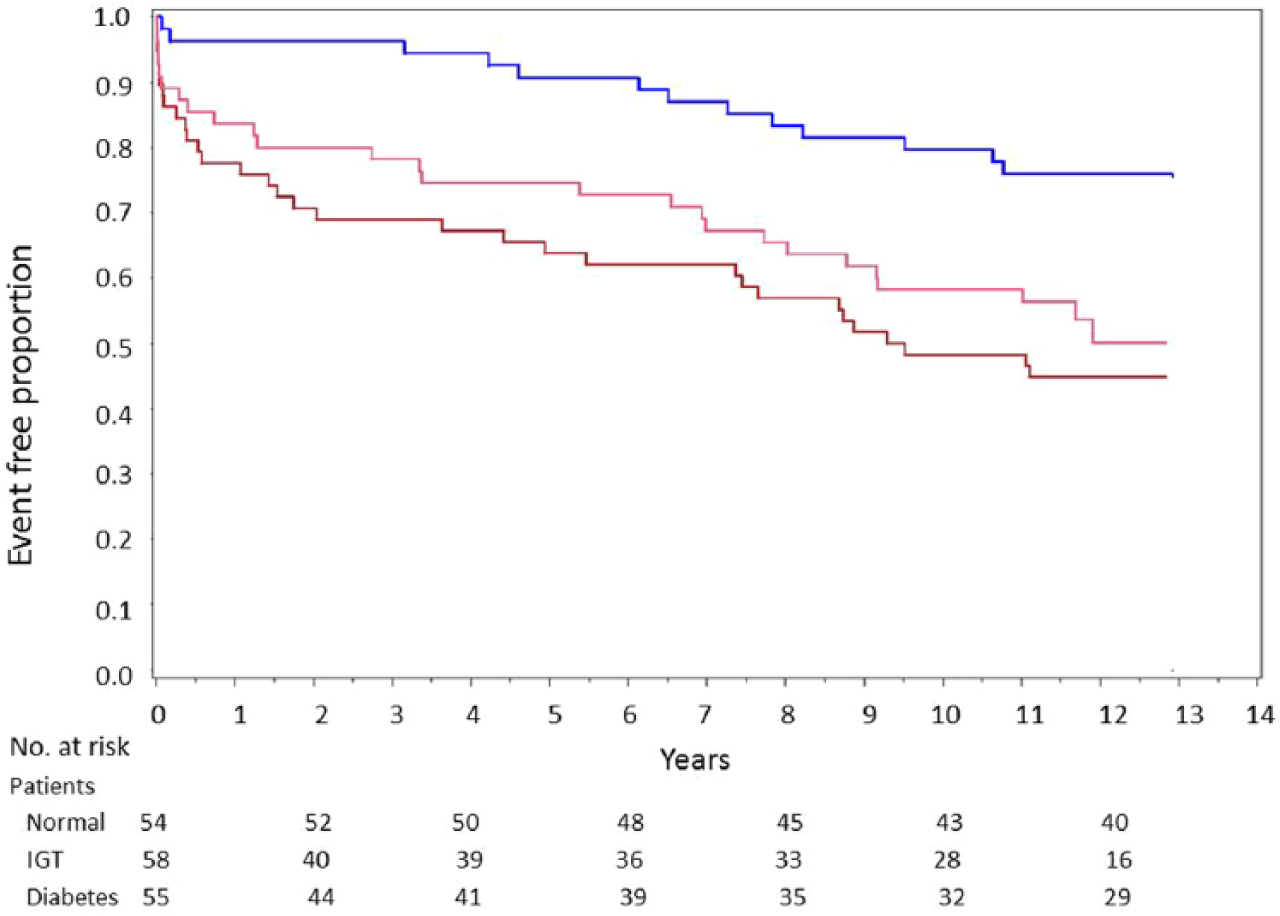
Kaplan–Meier curves showing time to a first major cardiovascular event in patients by glucose tolerance group (NGT, IGT, DM; log-rank overall p = 0.0046).
Conclusion
The most important finding in this long-term follow-up of the GAMI cohort is that an OGTT performed at the time for hospital discharge after an AMI identifies patients at continuously increased risk for major cardiovascular event during the following decade. In contrast, neither fasting glucose nor HbA1c had a similar predictive power.
Newly identified AGT, either in the form of IGT or diabetes, was an important predictor of cardiovascular event in patients with AMI remaining even after adjusting for age and other conventional risk factors. Interestingly, there was no major difference between IGT and diabetes favouring the assumption that it is more important to identify AMI patients with AGT rather than to classify them into IGT or diabetes, since hyperglycaemia seems to be a successively increasing risk factor starting already well below the level presently accepted as diagnostic for diabetes. Classification by means of OGTT in IGT and diabetes will then by definition be arbitrary by dichotomising a risk factor that is continuous.21,22 Recent guidelines from the ADA and the WHO recommend HbA1c rather than OGTT as diagnostic tool for diabetes.5,23 The present findings confirm that post-load glucose is a significantly more important risk marker than fasting glucose especially in early stages of dysglycaemic conditions in which the former and HbA1c still may be normal. 24 Importantly, HbA1c did not fall out as an independent predictor even above the cut-off of 4.7% (MonoS) corresponding to 5.7% (DCCT) advocated by ADA as indicating enhanced risk of diabetes. Thus, the present findings underline the importance of investigating patients with acute coronary syndromes with an OGTT as recommended in the most recently issued European management guidelines. 25
The original finding in the GAMI study that as many as two-thirds of patients with AMI have previously unknown, AGT has subsequently been confirmed by several studies in people with unstable as well as stable coronary artery disease.8–10,26 An OGTT performed earlier than 4–5 days after an acute coronary syndrome may give erroneous results due to a stress-induced increased adrenergic tone 27 and since discharge from hospital today frequently are within a few days, the best option may be to prescribe the test at the first follow-up. To not delay the diagnosis of diabetes, HbA1c and fasting glucose should be analysed during hospital stay but both will probably underestimate the true prevalence of glucose perturbations. The correlation between an OGTT performed before hospital discharge and 3 months thereafter is high. 28 Beta-cell dysfunction, with loss of early insulin response, was a major explanation for the glucose disturbances. 29 Thus, the influence of stress cannot explain the high prevalence of AGT revealed when the test is appropriately timed supporting the notion that the glucometabolic disturbance is an important contributor to the coronary arterial disease in itself and part of pathophysiological factors of importance for disease progression. Cardiovascular death was more common among individuals with AGT, while cancer mortality was more common in those with NGT. This indicates that the relation between AGT and cardiovascular complications is considerably stronger than that to mortality from other causes. AGT was indeed related to cardiovascular but not all cause mortality. This supports the inclusion of OGTT as a screening tool not only for diagnosing diabetes but even more for identifying individuals at high cardiovascular risk.
The present results support previous reports on an immediate dismal influence of newly detected AGT on cardiovascular event after a MI.12,13 Since follow-up times of the present duration are infrequent, another new and important information is that the dismal influence of an early detected AGT remains over time. As revealed by the Kaplan–Meier curves, the prognostic disadvantage of having newly detected AGT is an independent risk marker of importance during at least the following decade. Importantly, the GAMI cohort truly mirrors the prognostic implication of newly detected AGT, since it, in contrast to other reports, did not include patients with previously known diabetes.
Strengths and limitations
Strengths with the GAMI study are the inclusion of consecutive patients with AMI, the exclusion of those with known diabetes or an admission glucose levels of >11 mmol/L, thereby identifying a cohort free from previously known AGT. The collection of age- and gender-matched controls allows a true comparison of people with and without AMI demonstrating the much higher prevalence of AGT in the former group. 14 Finally, the careful ascertainment of cardiovascular event based on direct information from the patients, hospital records and national registries with only one patient lost to follow-up during a very long time provided a reliable base for the present observations. The major limitation is the small sample size and limited numbers of events in both patients and controls despite a decade of follow-up. This will limit the statistical modelling as well as the statistical power for both groups but especially for controls that have fewer cardiovascular events than patients. Lack of power due to few events may be one reason why AGT did not remain as an independent predictor for future cardiovascular events in controls. However, the limited number of patients and controls provided an opportunity to get complete information on each individual during an unusual long period of follow-up. It could have been an advantage to apply recently constructed prognostic algorithms, for example, the Global Registry of Acute Coronary Events (GRACE) score. 30 This was, however, not possible due to lack of full information on important variables in this score.
To conclude, an OGTT performed before hospital discharge after an AMI discloses a high prevalence of glucose abnormalities and identifies individuals at a substantially increased risk for future major cardiovascular event during the following decade. In contrast, patients with NGT have a considerably more benign prognosis. The results strongly support the inclusion of an OGTT as a screening tool in coronary care to add important and independent prognostic information in patients without previously known glucose abnormalities.
Footnotes
Acknowledgements
The authors would like to thank Christina Edman Jönsson, RN, at the Cardiology Unit at Karolinska University Hospital Solna for valuable assistance in collecting patient records and events by interviewing patients and controls. All authors have made substantial contribution to this article. All authors took part in the interpretation of the results. L.R., K.M., Å.T. and A.N. developed the study design and collected all the patients. V.R. analysed the death certificates together with A.N. and E.T. V.R. managed the database and performed the statistical analyses. P.N. provided supervision and support within the frames of statistical analyses. V.R. and A.N. finalised this article after adjustments from all authors.
Declaration of conflicting interests
The authors have no conflicts of interest to declare in relation to this article. L.R. has received research grants from The Swedish Heart-Lung Foundation, AFA Insurance and Swedish Diabetes Foundation and honorariums from expert group participation arranged by some pharmaceutical companies and have received personal occasional fees for delivering educational lectures organised by pharma and societal organisations, although none of the aforementioned was directly related to this publication. K.M. is currently employed by F. Hoffman-La Roche to 80% and works 20% as an adjunct professor at Karolinska Institutet, however fully paid by Roche. A.N., Å.T., E.T., P.N. and V.R. have nothing to declare.
Funding
This work was supported by The Swedish Heart-Lung Foundation, The Kronoberg County Council and Västerås Hospital.