
Abstract
Aim:
Type 2 diabetes is a risk factor for coronary artery disease; however, a number of studies have shown that patients are asymptomatic for coronary artery disease. The presence of coronary artery disease in asymptomatic patients with type 2 diabetes was evaluated to determine its impact on management decision and prognosis.
Methods:
A total of 75 patients underwent single-photon emission computed tomography myocardial perfusion imaging for detection of suspected coronary artery disease. We used 17-segment model for perfusion and function analysis. Multislice computed tomography was performed in 45 patients to assess coronary artery calcium. Complete laboratory analyses with lipid values and standard risk factors were analysed. Forward logistic regression analysis was used to assess predictive parameters for myocardial ischaemia during the follow-up period of 20 ± 4 months.
Results and Conclusion:
Silent myocardial ischaemia and subclinical coronary artery disease can be detected in a significant proportion of asymptomatic patients with type 2 diabetes. Diabetic patients with normal myocardial perfusion imaging had an excellent 2-year prognosis with optimal medical therapy and intensive risk factor control. In comparison, an abnormal myocardial perfusion imaging led to an increased risk of cardiovascular events. Myocardial perfusion imaging and coronary artery calcium are valuable tools for risk stratification and optimal treatment decision in this asymptomatic diabetic cohort of Macedonian patients.
Keywords
Introduction
The risk of type 2 diabetes increases with age, especially over the age of 50. Coronary artery disease (CAD) is the leading cause in morbidity, mortality and cost of management of patients with type 2 diabetes. Acute myocardial infarction or sudden cardiac deaths are often the first clinical presentations in asymptomatic diabetic patients due to the insufficient screening for CAD. 1 These events are linked to increased morbidity, mortality and socioeconomic burden. The dilemma on the cost-effectiveness of screening for myocardial ischaemia in asymptomatic diabetic patients in relation to the optimal therapeutic approach is still ongoing. There is controversy whether noninvasive imaging such as myocardial perfusion imaging (MPI) improves type 2 diabetic patient management and prognosis. Proposed strategies that may favourably affect CAD risk and outcomes in high-risk asymptomatic population include identifying patients with subclinical disease at high risk of future cardiac events. Current risk score models (SCORE, FRAMINGHAM, PROCAM) show inferiority for individual risk stratification and ability to predict the presence of ischaemia.2–4 MPI with gated single-photon emission computed tomography (SPECT) is a noninvasive imaging scan of the heart commonly used to diagnose and evaluate prognosis of patients with known or suspected CAD.1,2 There is increased interest in the use of coronary artery calcium (CAC) imaging to assess early subclinical atherosclerosis and total atherosclerosis burden in patients with intermediate cardiovascular risk.3–5 CAC is also a proven prognostic parameter in diabetic patients.6,7 While simple categorical risk factors, such as hypertension, hyperlipidaemia, obesity, smoking and age, cannot effectively discriminate which asymptomatic high-risk type 2 diabetic patients will or will not have ischaemia on stress testing. 5 It is still possible, however, that risk factor burden may predict risk of cardiovascular events in individual patients. Herein, we assessed the prognostic value of coronary atherosclerosis and myocardial ischaemia in asymptomatic diabetic patients of a Macedonian cohort. We also determined how noninvasive imaging could influence treatment strategies in these patients.
Methods
Study design and data source
A prospective cohort study was designed and 75 consecutive asymptomatic patients with type 2 diabetes (41 male, 34 female; age range: 63 ± 9 years), without previously known or established CAD, were included in the study. All patients completed the World Health Organization Rose Angina Questionnaire for confirmation of the asymptomatic status. Screening for myocardial ischaemia was performed using MPI SPECT imaging in the nuclear cardiology laboratory at our clinic in the period of October 2012–November 2013. Prospective follow-up was complete in all 75 patients (100%) with a median period of 20 months (16–24 months). CAC scores were performed and data evaluated using Agatston units (AU). Two-dimensional (2D) transthoracic echocardiography was used for assessment of systolic and diastolic left ventricular function with GE VIVID7 echo machine. We have screened 93 diabetic patients, from which 75 with preserved left ventricular systolic function and left ventricular ejection fraction (LVEF > 50%), assessed by echocardiography Simpson’s rule, were enrolled in the study and included in the final patient cohort. Distribution of study subjects is presented in Figure 1.
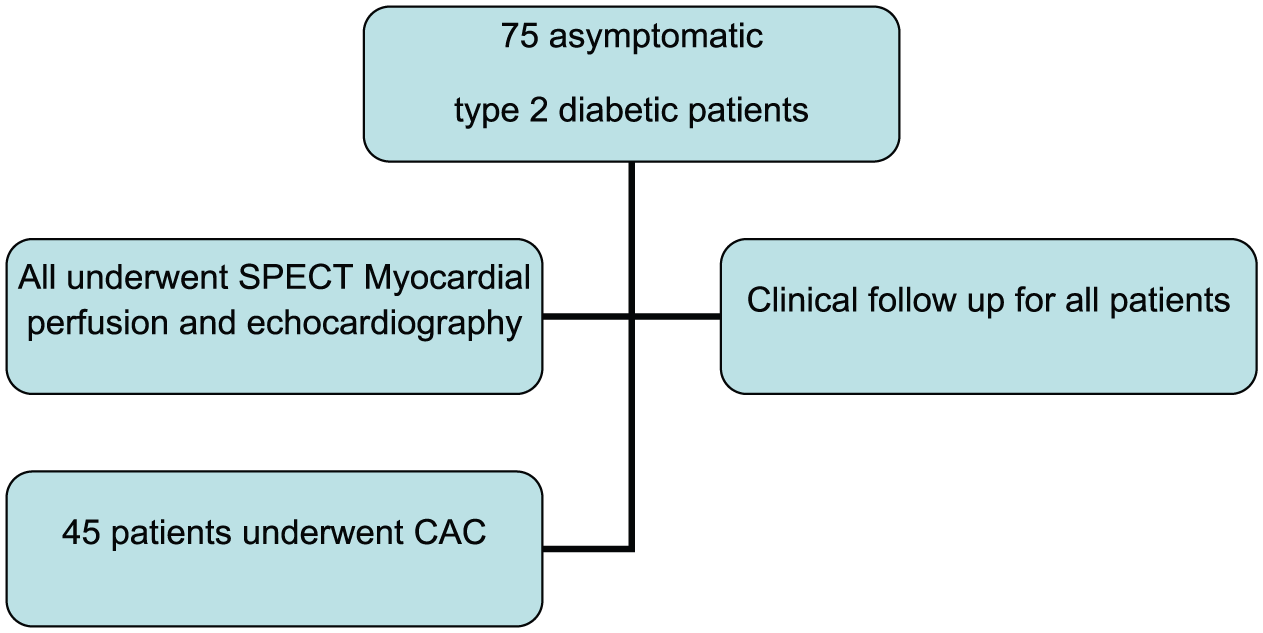
Distribution of study subjects.
All patients underwent a physical examination and included blood pressure measurements, weight, height, waist circumference, body mass index (BMI) and risk factor analysis. Full blood examination with high-density lipoprotein (HDL), low-density lipoprotein (LDL), non-HDL and triglyceride levels, fasting glucose levels, % glycated haemoglobin (HbA1c) and blood creatinine levels were performed within a maximum of 2 weeks prior to MPI. Medical history was evaluated and corrected according to target risk factor goals based on latest European Society of Cardiology (ESC) recommendations for cardiovascular prevention and hypertension treatment for all patients. Clinical and laboratory characteristics are shown in Table 1. The following inclusion criteria were used: asymptomatic patients with type 2 diabetes, normal rest left ventricular function with ejection fraction (EF) > 50%. Exclusion criteria were as follows: typical stable angina pectoris, previously known or established CAD (history of myocardial infarction, acute coronary syndromes (ACS), previous percutaneous intervention or coronary artery bypass surgery), LVEF < 50% at rest, severe valvular disease, atrial fibrillation, left bundle branch block, presence of pace maker and severe chronic pulmonary disease. The study was approved by the Human Ethics Committee of the Medical Faculty, University St. Ciril and Methodius in Skopje, Macedonia. All patients signed an informed consent.
Clinical characteristics of the study population.
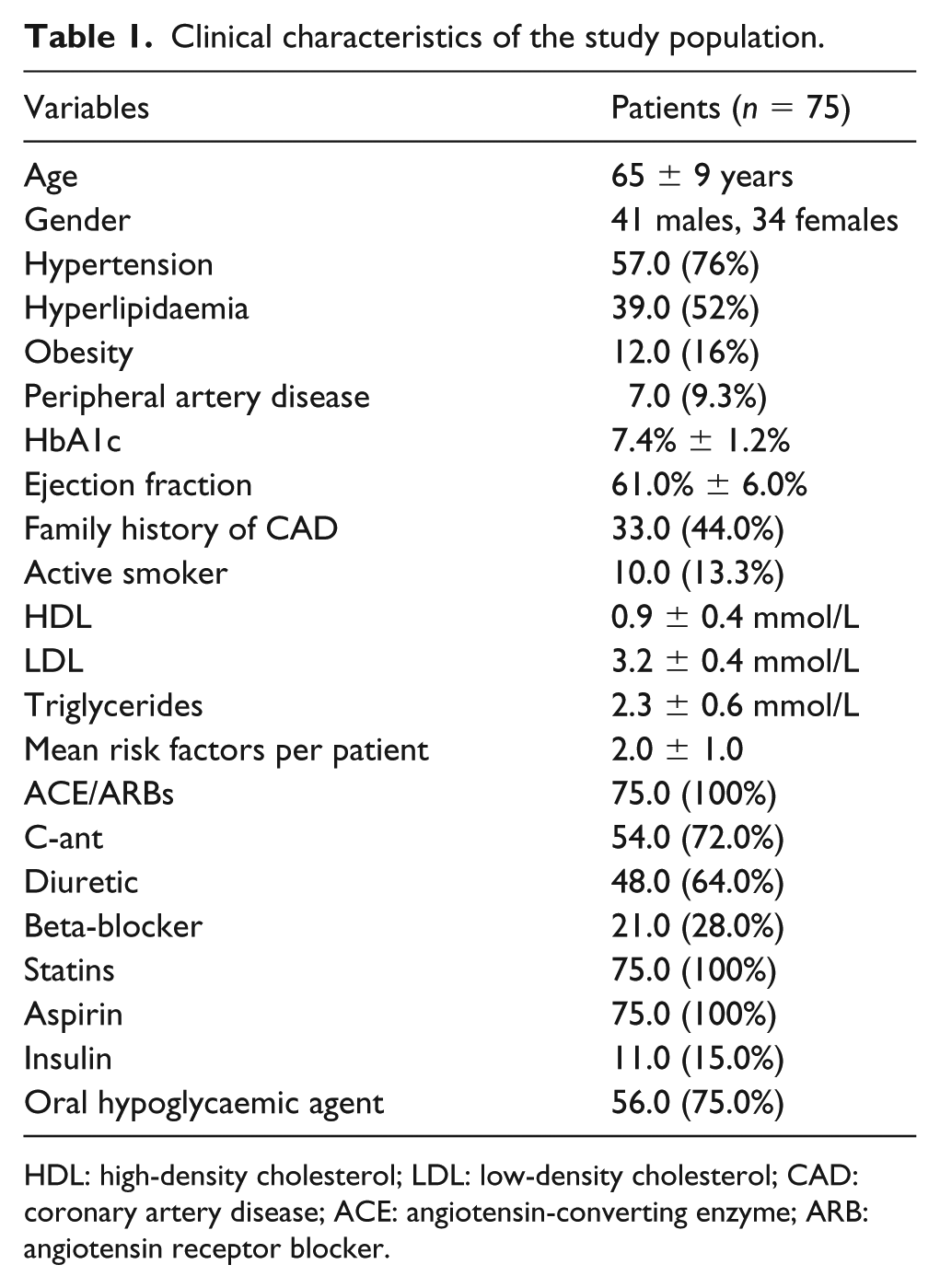
HDL: high-density cholesterol; LDL: low-density cholesterol; CAD: coronary artery disease; ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blocker.
Definition of study variables
Risk factor definitions were made according to the most recent ESC guidelines on hypertension, hyperlipidaemias and cardiovascular prevention: arterial hypertension [systolic blood pressure (SBP) > 140 bpm or diastolic blood pressure > 90 bpm], dyslipidaemia (LDL > 1.8 mmol/L; HDL < 1.1 and 1.0 mmol/L for females and males, respectively, and triglycerides >1.7 mmol/L), family history of myocardial infarction or sudden cardiac death in an immediate male relative <55 years or female <65 years and smoker (current smoker or those who quit in the past 6 months). BMI ⩾ 30 kg/m2 was used to define obese patients. Type 2 diabetes mellitus was defined as established disease in patients treated with oral anti-diabetic medication or insulin following initial treatment with oral anti-diabetic therapy. Newly diagnosed diabetes was defined as having either one of the following criteria, based on the ESC guidelines on pre-diabetes and diabetes: fasting glucose of 7.0 mmol/L or non-fasting glucose 11.0 mmol/L in two separate samples, HbA1c > 6.5% or pathologic oral glucose tolerance test in patients with fasting glucose over 6.5 without previously known or treated diabetes. Electrocardiography (ECG) abnormalities at rest were defined as the presence of ST-T abnormalities, Q-waves and T-wave inversion.
Myocardial perfusion SPECT imaging
MPI SPECT imaging was performed using 1-day rest stress protocol with radiotracer technetium (Tc-99m) sestamibi, using 15 mCi for the rest and 25 mCi for the stress study. We used single head gamma camera Siemens e-cam, with commercially available quantitative gated and perfusion SPECT software package (4DM-SPECT). Patients were instructed to refrain from caffeine-containing beverages for at least 12 h, nitrates for 24 h and beta-blockers for 48 h before the study. All patients underwent pharmacological stressing with dipyridamole. We used the 17-segment model for quantitative Bull’s eye analysis of regional myocardial perfusion and function. Myocardial perfusion was assessed by 5-point score system (0: normal radiotracer uptake; 1: mild; 2: moderate; 3: severe hypo perfusion; 4: absent uptake). Semi-quantitative analysis of regional perfusion at rest and stress was performed using summed stress score (SSS), summed rest score (SRS) and summed differential score (SDS), aimed to assess the presence and extent of myocardial ischaemia. Scan abnormalities were defined as follows: SSS < 4 normal perfusion, 4–8 mild, 9–13 moderate and >13 severely abnormal scan; SDS < 6 mild [<10% of left ventricle (LV)], SDS 7–10 moderate (10%–15% of LV) and SDS > 10 severe ischaemia (>15% of LV). Fixed defects were defined as SRS > 4. Any perfusion abnormality was defined as SDS > 4 and/or SRS > 4. LV volumes, LVEF at rest and stress, presence of transit ischaemic LV dilation (TID), visualization of right ventricle and lung uptake were also analysed. Regional wall motion analysis was assessed by a 6-point scoring system at rest and stress (0: normal wall motion; 1: mild; 2: moderate; 3: severe hypokinesia; 4: akinesia; 5: dyskinesia) using wall motion score index.
Results considered normal were those that showed a homogeneous distribution of the radiotracer throughout the LV myocardium at the stress and resting images and with normal systolic movement and thickening. The fixed perfusion defects, present in both images and with a segmental contractile deficit and systolic thickening were interpreted as fibrosis. Transient perfusion defects, present at the stress phase and absent at the resting phase, with normal range of movement and thickening, were considered to be ischaemia. When the recovery of these defects was only partial, with a contractile deficit, it configured the simultaneous existence of fibrosis and ischaemia.
CAC imaging
For CAC imaging, a non-enhanced, prospectively ECG-gated scan was obtained by use of a 128-slice CT scanner (Siemens Somatom Definition 128 AC+, single source). The estimated effective radiation dose for this protocol was bellow 1 mSv. Image reconstruction was performed at 55% of the R-R interval with prospective gating usage. The total calcium burden in the coronary arteries was measured according to the scoring algorithm of Agatston. On the basis of the total calcium score expressed in AU, patients were placed into five categories, as previously reported: 8 CAC 0 (no evidence of atherosclerosis), 1–10 AU (minimal or insignificant CAC), 11–100 (mild CAC), 101–400 (moderate CAC) and 401–1000 (severe CAC). Total CAC score and CAC score in each coronary artery was evaluated.
Coronary angiography
All patients with at least moderate myocardial ischaemia (SDS > 7) underwent coronary angiography. Invasive coronary angiograms were evaluated by consensus of two interventional cardiologists who were unaware of the SPECT and CAC imaging results. Segments were classified as normal, as having nonobstructive disease or as having significant stenosis (50% stenosis). Presence, localization, severity of coronary stenosis and number of vessels involved were analysed using Syntax score. Percutaneous coronary intervention (PCI) with stenting or coronary artery bypass surgery was performed according to the latest myocardial ESC revascularization guidelines, based on invasive cardiologist’s team decision.
Medical therapy and lifestyle advice
Medical therapy was reviewed in detail and all patients underwent an optimal medical treatment with lifestyle and risk factor control advice and targets based on the latest ESC guidelines for cardiovascular prevention and management of stable CAD.
Follow-up
Patients were prospectively followed for a median of 20 ± 4 months. The following were considered as cardiovascular events: sudden cardiac death, ACS with or without ST-segment elevation, myocardial revascularization with PCI or coronary artery bypass grafting (CABG) and cerebrovascular events (cerebrovascular insult, CVI). The follow-up of the sample was carried out by 6-month clinical visits until the end of the follow-up period, or in earlier periods in case of change in clinical symptoms or clinical event.
Statistical analysis
Statistical analysis was performed with the use of the SPSS statistical package (version 18.0). Categorical variables were compared using chi-square test and continuous variables using unpaired Student’s t test. Normality of variables distribution was performed. Categorical values were expressed in percentages, continued as mean value ± standard deviation (SD). Linear regression analysis was used to determine whether there was a correlation between the CAC score and perfusion abnormalities on SPECT. Multivariate forward stepwise logistic regression analysis was built in order to identify factors associated independently with the presence of silent myocardial ischaemia and prognosis. The analysis includes age, gender, hypertension, hyperlipidaemia, smoking, obesity, diabetes duration, myocardial perfusion imaging (MPS) perfusion scores, ECG ST segment depression during pharmacological stress and CAC. The criterion for entrance into the model was a univariate probability value of p < 0.05 and p > 0.10 for removal from the model. p < 0.05 was considered to be statistically significant for all statistical tests. Cumulative event-free survival rates as a function over time were obtained using the Kaplan–Meier method. Cardiac event-free survival curves were compared using the log-rank test. To identify the association between clinical and imaging variables and outcomes, Cox regression analysis was used.
Results
Follow-up was attained in all 75 patients. Study demographics consisted of 41 male (55%) and 34 female patients (45%), with mean age of 65 and 69 years, respectively, as shown in Table 1. The prevalence of metabolic risk factors, blood examination and medical therapy are presented in Table 1. All patients had on average two risk factors. The risk factors for the cardiovascular disease were distributed as follows: 76% of systemic arterial hypertension, 51.4% of dyslipidaemia, 14% of cigarette-smoking, 12% with obesity and 44% of family history for coronary history. Average duration of diabetes was 8 ± 3 years. A total of 11 patients (15%) used insulin therapy.
Myocardial SPECT findings
The stress phase was carried out through pharmacological stress with dipyridamole in all patients. A total of 1275 segments were analysed. All patients showed normal rest left ventricular function with EF > 55.0% assessed by gated SPECT. A total of 56 patients (74.6%) had normal MPI results. The scintigraphy results were abnormal in 19 patients (25.3%). Stress-inducible ischaemia was found in 18 patients (24.0%). Ischaemia plus fibrosis with fixed perfusion defects were found in three patients and fixed defects only in one patient, which could indicate the presence of previous silent myocardial infarction. Mild ischaemia was found in six patients – summed difference score (SDS) < 4, moderate ischaemia (SDS 7–10) in seven and severe ischaemia (SDS > 10) in five patients (Figures 2 and 3). Average wall motion index (WMI) in patients with ischaemia was 1.25.
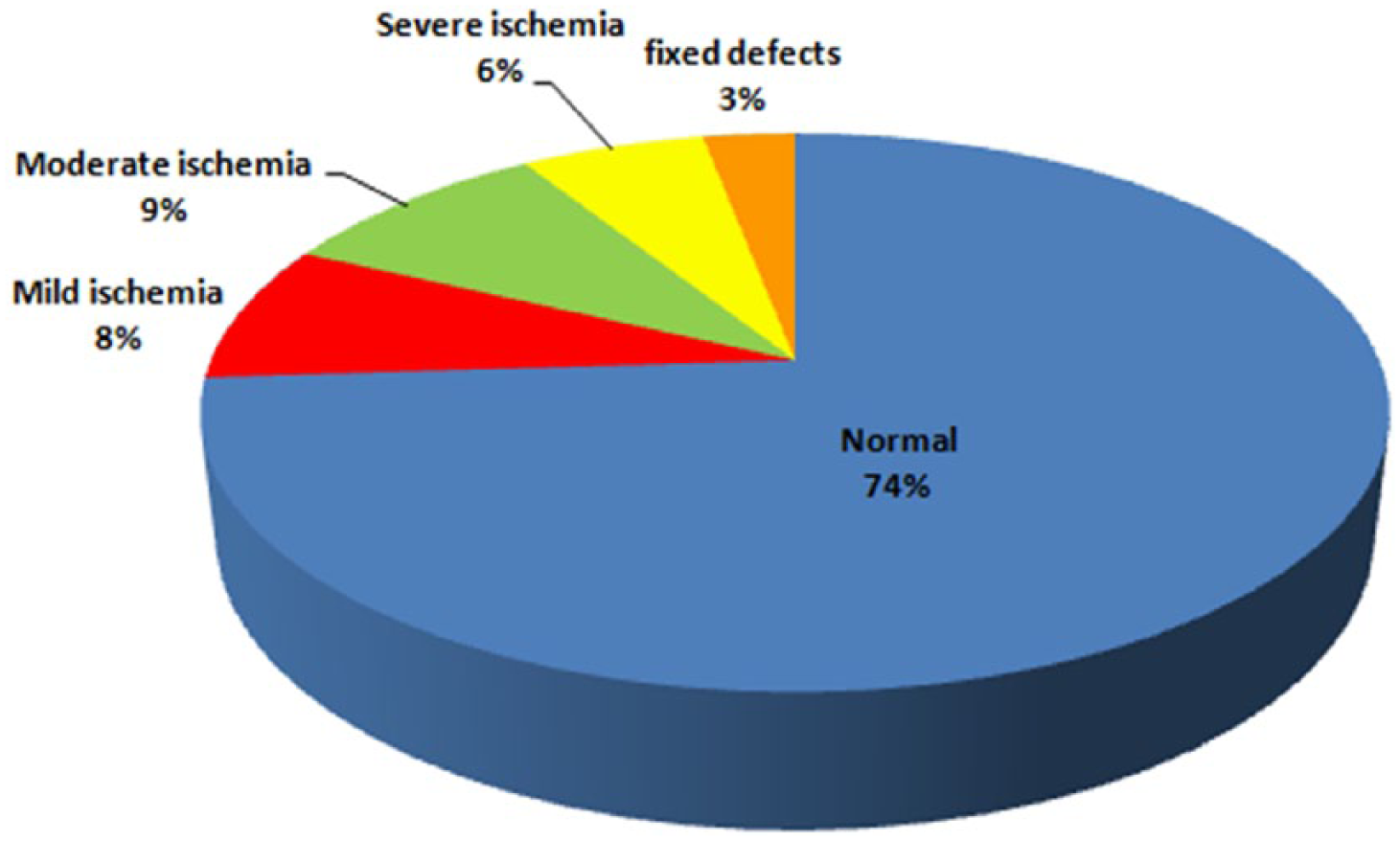
Severity of ischaemia in the studied population (n = 18).
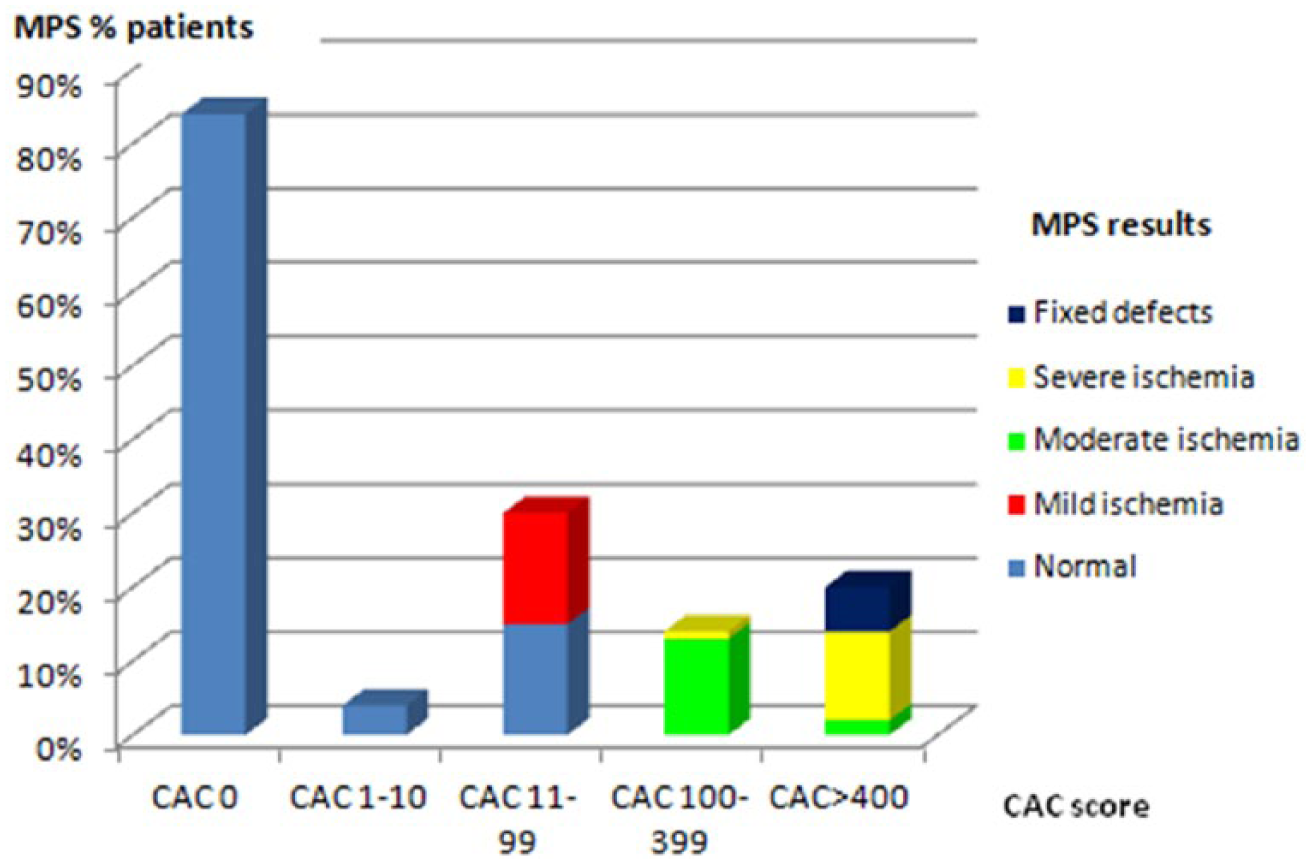
Relationship between percentage and severity of myocardial perfusion abnormalities and extent of coronary artery calcification.
Patients with severe ischaemia had a drop of LVEF during stress study by >5.0% and TID. There was a correlation with diabetes and stress ECG changes with the presence of myocardial ischaemia (r = 0.54 and r = 0.58, respectively). When the scintigraphy results were analysed, we noted that the patients with abnormal perfusion were significantly older male population (p = 0.01) when compared to the group with normal perfusion.
CAC findings
CAC score was assessed in total 135 coronary arteries. Subclinical atherosclerosis was present in 35 patients from 45 (77.7%) who had CAC score evaluated. A total of 10 patients had CAC score 0 AU, 4 patients had CAC score 1–10 AU, 15 patients had mild CAC score (11–99 AU), 7 patients had moderate CAC (100–399 AU) and 9 patients had severe CAC (401–1000 AU). No patients had extensive CAC > 1000 AU. Calcium was present in the left anterior descending coronary artery (LAD) in 17 patients, in the left circumflex artery (LCX) in 6 patients and right coronary artery (RCA) in 12 patients. The average calcium score in the LAD (289 ± 72) was significantly higher than those in the LCX (115 ± 56) and in the RCA (192 ± 68). Patients with moderate and severe ischaemia had CAC score 667 ± 112 AU. Patients with normal MPI scan had an average CAC score of 25 ± 18 AU.
The subclinical atherosclerosis group were older, predominantly male and 15 were smokers. Independent predictors of subclinical atherosclerosis were age (⩾65 years) [odds ratio (OR): 1.068, 95.0% confidence interval (CI): 1.05–1.92, p = 0.026], diabetes (OR: 1.89, 95% CI: 1.1–2.76, p = 0.052) and smoking (OR: 1.73, 95% CI: 1.2–2.21, p = 0.041) in multivariate forward logistic regression analysis.
Relationship between CAC imaging and gated SPECT
The relationship between the prevalence and severity of myocardial perfusion abnormalities and the extent of CAC is shown in Figure 4. Nine patients with normal SPECT results showed atherosclerosis with mild CAC score (11–99 AU). Contrarily, eight patients with moderate CAC and six patients with severe CAC had abnormal perfusion. The mean CAC score was significantly higher in subjects with at least moderate ischaemia than in those who had normal SPECT results (667 ± 112 vs 149 ± 45; p < 0.001).
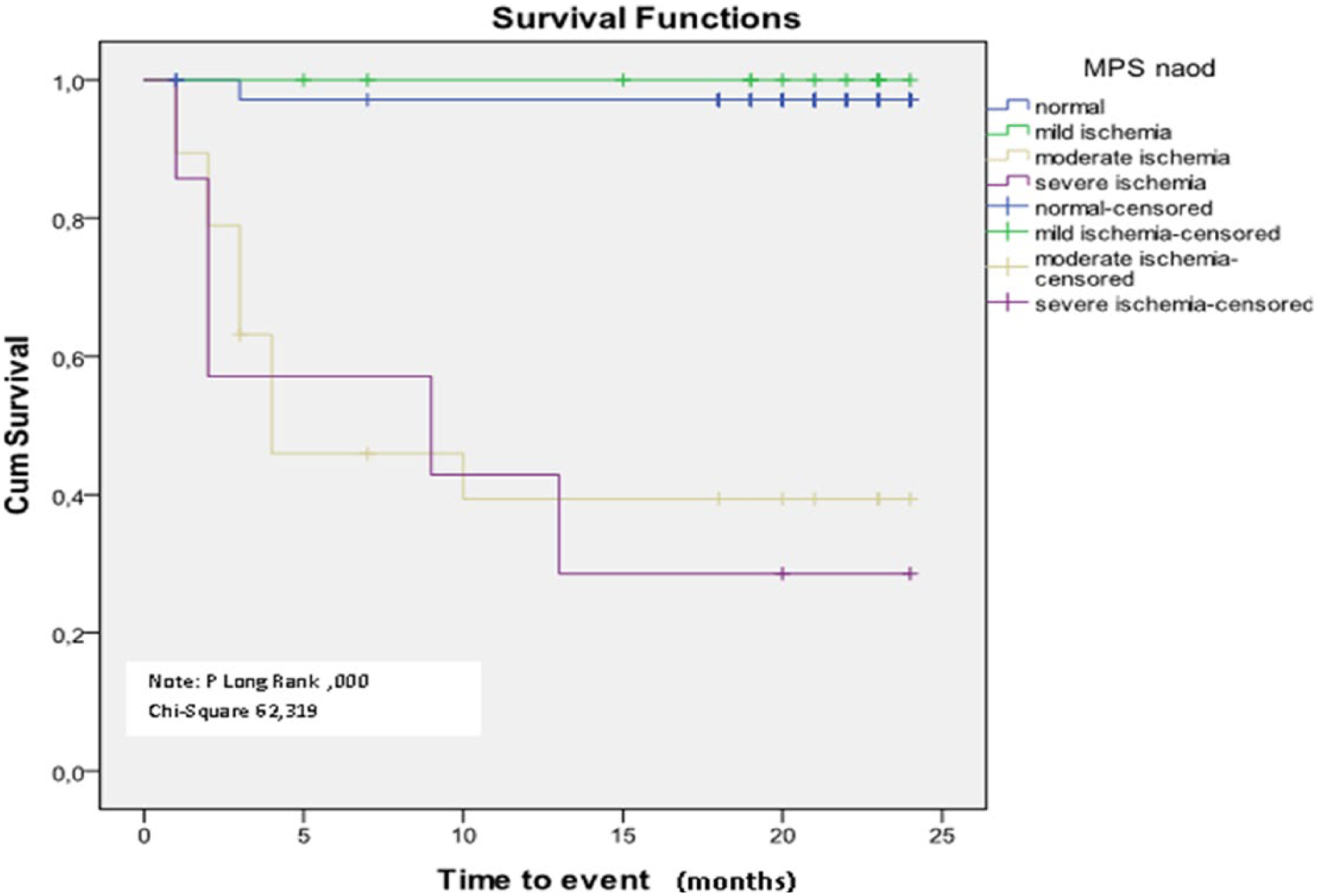
Kaplan–Meier survival curves as a function of myocardial perfusion scintigraphy results and severity of myocardial ischaemia.
Predictors of myocardial ischaemia
Stepwise forward logistic regression analysis for prediction of stress-induced ischaemia in the model that included CAC showed OR 2.4 (95% CI: 1.7−3.6) for stress-induced ECG changes, OR 2.8 for CAC > 400 (95% CI: 1.9–3.2) and OR 3.9 for the presence of type 2 diabetes over 10 years (95% CI: 2.3−6.6), as shown in Table 2. The second stepwise forward logistic regression model which did not include CAC showed OR 2.1 (95% CI: 1.3−3.4) for male gender, OR 2.4 for hyperlipidaemia (95% CI: 1.7–3.8) and OR 3.7 for presence of type 2 diabetes over 10 years (95% CI: 2.2−5.7), as shown in Tables 3 and 4. Relationship between percentage and severity of myocardial perfusion abnormalities and extent of CAC is presented in Figure 3.
Model 1: multivariate stepwise logistic regression analysis for predictors of stress-induced ischaemia (model includes CAC).
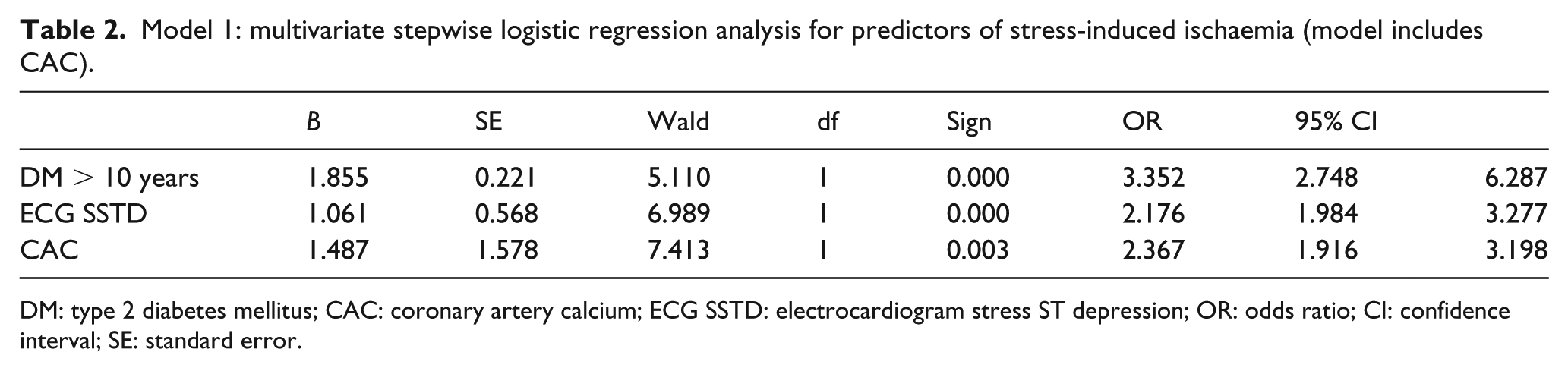
DM: type 2 diabetes mellitus; CAC: coronary artery calcium; ECG SSTD: electrocardiogram stress ST depression; OR: odds ratio; CI: confidence interval; SE: standard error.
Model 2: multivariate stepwise logistic regression analysis for predictors of stress-induced ischaemia (model excludes CAC).
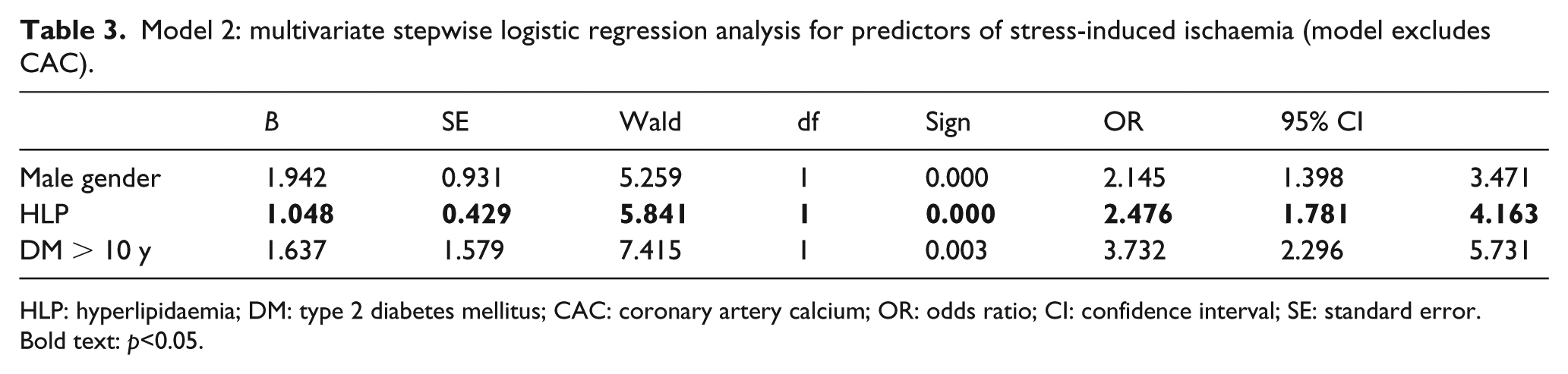
HLP: hyperlipidaemia; DM: type 2 diabetes mellitus; CAC: coronary artery calcium; OR: odds ratio; CI: confidence interval; SE: standard error.
Bold text: p<0.05.
Frequency of revascularization procedures and acute coronary syndromes during follow-up period.
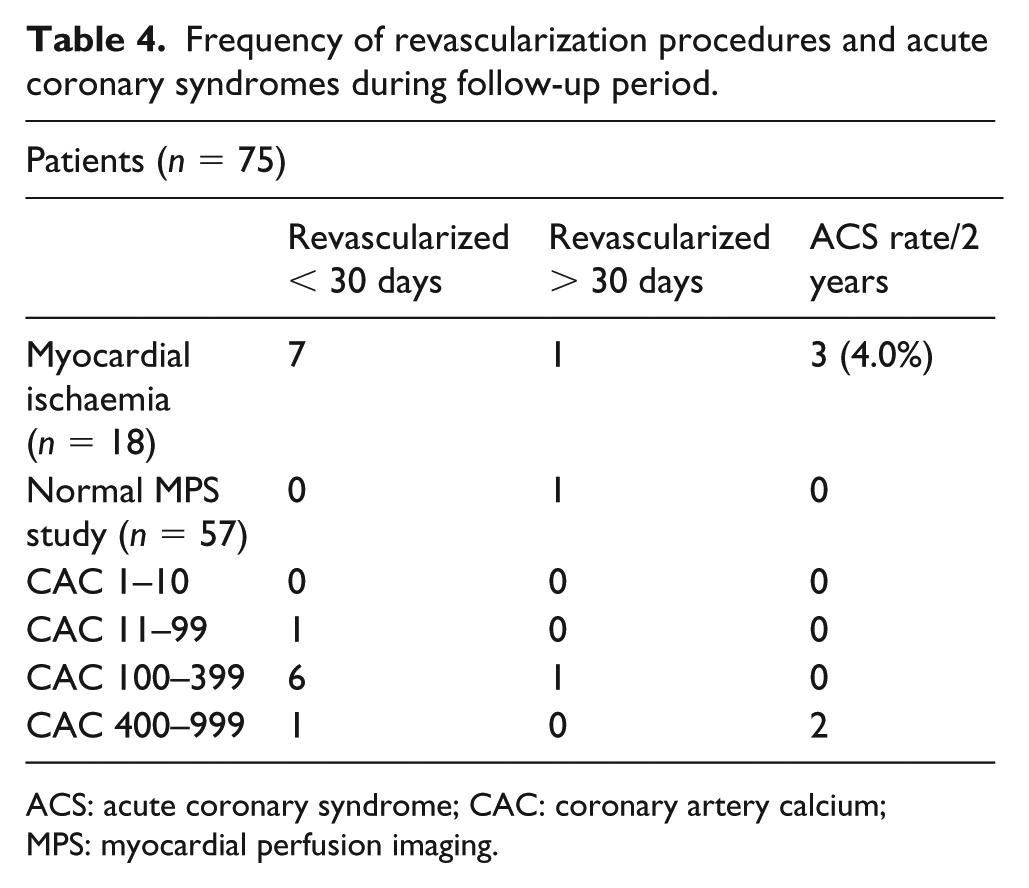
ACS: acute coronary syndrome; CAC: coronary artery calcium; MPS: myocardial perfusion imaging.
Cardiovascular events and frequency of revascularization procedures during follow-up
There were no cardiac deaths, myocardial infarctions or heart failure during the follow-up period. All patients with moderate severe ischaemia were referred for coronary angiography (n = 12). From 12 patients with at least moderate ischaemia, 8 patients had significant CAD and underwent PCI revascularization (66.6%; Tables 4 and 5). Two patients had PCI to RCA, 3 patients had PCI to LAD and 1 patient had PCI to LAD and LCx. Other four patients had angiographically nonsignificant CAD and received an advice for intensive medical treatment. Patients with mild ischaemia (SDS < 7) and normal MPI findings were put on intensive medical therapy and lifestyle modification. The average CAC score in these patients was 590 ± 145. Three patients were hospitalized due to non-stable angina, two with previous severe ischaemia and one with normal MPI study. Patients with normal MPI had a low revascularization rate of 1.3% during the follow-up period and no other cardiovascular events in the follow-up period. Revascularization rate in the studied cohort was 2.1% during the follow-up period of 20 ± 4 months. Univariate analysis of variables that influence future events presented with following predictive values: hyperlipidaemia (score = 2.275, p = 0.031), DMT2 duration over 10 years (score = 3.125, p = 0.021), CAC > 400 (score = 2.117, p = 0.018) and SDS > 7 (score = 4.173, p = 0.0012). Results of univariate analysis are summarized in Table 6. SDS > 7 (OR: 2.0371, p = 0.001) and diabetes duration over 10 years (OR: 1.9136, p = 0.002), stepped into the multivariate model, showed independent predictive values (Table 6). Kaplan–Meier curves (Figure 4) showed significant difference between event-free survival and degree of myocardial ischaemia (Log rank p = 0.000, chi-square = 62.319).
Cox regression analysis of predictors of cardiac events.
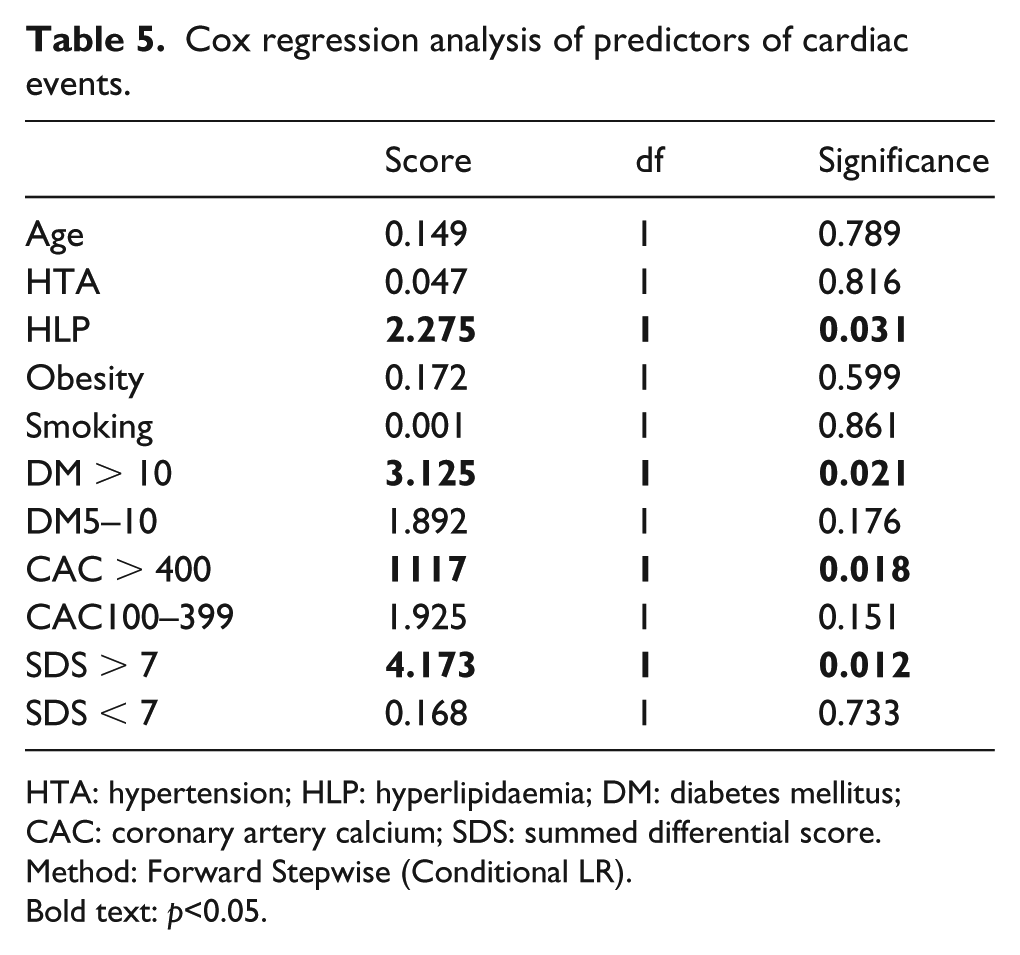
HTA: hypertension; HLP: hyperlipidaemia; DM: diabetes mellitus; CAC: coronary artery calcium; SDS: summed differential score.
Method: Forward Stepwise (Conditional LR).
Bold text: p<0.05.
Multivariate analysis for predictors of cardiac events.

SE: standard error; DM: type 2 diabetes mellitus; SDS: summed stress score.
Discussion
This study showed diabetes duration, stress ECG ST segment depression and coronary artery calcium >400 AU as predictors of at least moderate myocardial ischaemia in high-risk asymptomatic patients in logistic regression model which includes CAC. Male gender, hyperlipidaemia and diabetes duration over 10 years were predictors of silent ischaemia in the second model which excluded CAC. The aim of screening for silent CAD in high-risk patients is to detect disease in the early stage, taking into consideration up to 60.0% of male and 42.0% of female patients, and the first initial presentation of CAD is acute myocardial infarction and 40.0% with sudden cardiac death.1,2 There has been a long debate and conflicting opinions concerning the optimal screening approach in asymptomatic patients with high cardiovascular risk. The scientific data give arguments that atherosclerosis and myocardial ischaemia imaging in selected asymptomatic moderate and high-risk adults to be used, although prognostic implications of this approach are not clear. 3 The prevalence of silent ischaemia ranges between 22% and 63.0% in diabetic patients. We noted that 18 patients (24.0%) had stress-inducible ischaemia and 12 of them had at least moderate ischaemia. Our results showed high negative predictive value of the normal myocardial scintigraphy scan and good intermediate prognosis in diabetic patients. Four patients in our study (5.3%) had fixed perfusion defects alone and in combination with ischaemia, which indicate 5.3% had previous silent myocardial infarctions. This finding is in correlation with the previous studies data, which reports the incidence of silent myocardial infarction of 5% (18.20). The study reports the revascularization rate of 2.1% for 20 ± 4 months. Eight patients with at least moderate ischaemia (66.6%) underwent PCI revascularization. Three patients from our study were hospitalized for ACS (4.0%), two with previous incomplete revascularization and severe ischaemia and one patient with normal study. All patients with normal MPI study (74.6%) had good prognosis with no hard events and revascularization rate of 1.3% during the follow-up period of 20 ± 4 months. Multivariate Cox regression analysis showed SDS > 7 and diabetes duration over 10 years as independent predictor of cardiovascular (CV) events (OR: 2.0371, p < 0.001 and OR: 1.9136, p < 0.002), after adjustment for hyperlipidaemia and CAC > 400.
The concept of diabetes as CAD equivalent was introduced following the Finnish population-based study. 3 Based on several epidemiological studies, diabetic patients are considered as high-risk population. 5 However, it has been argued that CAD risk equivalence in diabetes is also influenced by additional risk factors, target organ damage and the presence of vascular disease. The use of vascular imaging may improve the individual risk assessment in diabetic patients. Acampa et al. 6 found significant risk reclassification after MPS use in diabetic patients with suspected or known CAD. The value of noninvasive imaging of diabetic vascular disease has been confirmed in several studies and also in our previous study.7,9
From a management and prognostic perspective, the important question is whether we are able to improve the overall state for diabetic patients? Will vascular damage and ischaemia assessment improve long-term prognosis? Recommended risk-stratification models have evident inferiorities, which do not include many additional risk factors such as diabetes, family history and obesity. These models do not predict the presence of myocardial ischaemia or atherosclerosis which has prognostic information. From the data we have thus far, patients with at least moderate myocardial ischaemia with 10% or more of the left ventricle involved are suitable candidates for invasive treatment, although the long-term benefits of this approach are still not confirmed in prospectively randomized ischaemia-based treatment studies. In fact, there was no significance in the BARI 2D trial in relation to survival. 10 Furthermore, there was no significance between major cardiovascular events in patients treated with medical therapy or revascularization. 10
The occurrence of ischaemia as detected by SPECT myocardial scintigraphy in asymptomatic type 2 diabetic patients demonstrated that myocardial ischaemia was highly prevalent in type 2 diabetic patients (34.0%) versus control subjects (17.0%). 11 The findings of reversible perfusion defects were only significantly associated with the presence of type 2 diabetes. The proof of CAD presence suggests the necessity to increase pharmacological therapy and risk factor control. In addition, the presence of atherosclerosis may also improve patient compliance and acceptance of lifestyle changes.
A number of studies involving CAD screening in type 2 diabetic patients did not show any correlation among the number of associated risk factors to inducible ischaemia as assessed by SPECT imaging.12,13 However, these studies did not evaluate severity, duration and treatment modalities of risk factors in patients with long-term type 2 diabetes. Furthermore, differences between the studies may also be a reflection of the differences between diabetes management, glucose and risk factor control and diabetes complications in different countries. European guidelines on cardiovascular prevention and treatment of stable CAD as well as American guidelines on screening for CAD in asymptomatic adults indicates that imaging of atherosclerosis and functional imaging of CAD have a place and can be used in this population.4,14 An important clinical question, however, is whether ischaemia should be screened in order to make a treatment decision. From a clinical point of view, the management dilemma should not be between medical versus invasive treatment, but rather which patient and when should invasive treatment be offered. In fact, the large ongoing ISCHEMIA Trial may answer many of these dilemmas and may provide the best initial treatment strategies for patients with stable CAD who have at least moderate ischaemia on noninvasive imaging tests.
In a meta-analysis study which evaluated type 2 diabetic patients who had normal MPI SPECT readings, it was noted that the rate of cardiac death or nonfatal myocardial infarction per annum was significantly lower (0.6%) in non-type 2 diabetic patients compared to type 2 diabetic patients. 15 The extent and severity of myocardial ischaemia is a strong risk predictor of coronary events.15–18 In fact, the annual rates for cardiac events in type 2 diabetic patients varied, with mild (1%–2%), moderate (3%–4%) and severe (7.0%) perfusion defects. 17 The only large prospective study for detection of asymptomatic ischaemia in non-selected type 2 diabetic patients with no prior CAD noted that 22% of patients presented with an abnormal MPI SPECT, and severe perfusion abnormalities were noted in 6.0% of the patients. 13 Of interest, males, duration of diabetes and the presence of cardiac autonomic dysfunction strongly correlated with ischaemia. 13 Herein, we noted abnormal MPS results in 25.3% of the patients. Stress-inducible ischaemia was found in 18 patients (24.0%), from which 12 patients had moderate and severe ischaemia. We had confirmed the impact of myocardial ischaemia detected by MPI on management decision in high-risk asymptomatic patients in our previous study. 19 The study showed that type 2 diabetic patients without a history of CAD and normal MPI have a relatively good 2-year prognosis. We found four false-positive results of MPI (4 of 12 had myocardial perfusion abnormalities with normal coronary angiography). These findings could be explained that microvascular dysfunction is often present in diabetic patients with multiple risk factors. This process could lead to heterogeneous myocardial perfusion and myocardial ischaemia, without the presence of significant CAD. The repetitive episodes of myocardial ischaemia due to microvascular dysfunction in larger myocardial regions could result in fibrosis, myocardial remodelling and development of diabetic cardiomyopathy.
A large observational study demonstrates that coronary calcium can be used as a prognostic marker even in patients with type 2 diabetes. Type 2 diabetic patients with zero CAC demonstrated an excellent 5-year survival rate but was not significantly different to control subjects (98.8% and 99.4%, respectively, p < 0.05). 8 However, several studies evaluating CAC in diabetic patients oppose the established opinion that DM type 2 is per se CAD equivalent. CV risk in diabetic patients actually is quite heterogenic and not all diabetic patients had the same risk. CAC 0 put the patient in lower risk group with expected good intermediate prognosis. The determinant factors to use coronary artery calcium as a screening method of atherosclerosis should be based on individual clinical approach and patient risk assessment. This test might be performed if the results are expected to influence the management decision. In fact, high-risk patients can be re-stratified into a lower risk category by the presence of zero calcium score, which also selects patients with good long-term prognosis.20–22 In our study, patients with moderate and severe ischaemia had Agatston CAC score of 667 ± 112. The presence of atherosclerosis is not necessarily the entity that leads to perfusion abnormalities. However, scintigraphic findings do not exclude the presence of obstructive CAD, but only indicates the absence of haemodynamically significant CAD. In a study using MPI, the prevalence of silent ischaemia was 18% in individuals with a CAC score of 100–400, with abnormal MPI findings in 45% of patients with a CAC score over 400. 23 Our results are in correlation with other studies underlying no absolute linearity of increasing CAC values and myocardial ischaemia findings, since these methods assess different aspects of CAD. We found that diabetic patients with normal MPI had good 2-year prognosis with optimal medical therapy. The risk for cardiovascular events increased as a function of perfusion scan abnormality. Larger prospective clinical trials with longer follow-up period are necessary to demonstrate the prognostic influence and ability of risk reclassification with SPECT imaging in asymptomatic diabetic patients.
Study limitations
The small sample we have evaluated could represent a limitation of our study. Nevertheless, our results could aid in improving our understanding of the relationship between functional and anatomic aspects of CAD in asymptomatic type 2 diabetic patients and their prognostic implications. CAC was performed in only 45 patients due to technical reasons.
Conclusion
The presence of silent myocardial ischaemia in asymptomatic type 2 diabetic patients is high and increases with diabetes duration. CAC imaging may be useful in identifying patients with extensive atherosclerosis without stress-induced ischaemia, who may be referred for risk factor modification and aggressive medical treatment. CAC over 400 AU, male gender and diabetes duration over 10 years predicted the risk of silent ischaemia in our study. Multivariate regression analysis showed SDS > 7 as MPI variable and diabetes duration over 10 years as predictors of CV events. These results indicate that MPI and CAC are valuable tools for risk stratification and optimal treatment decision in this asymptomatic diabetic cohort of Macedonian patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.