
Abstract
Gender differences in cardiovascular outcomes were compared in asymptomatic men and women with type 2 diabetes (T2DM) in the Detection of Ischemia in Asymptomatic Diabetics (DIAD) study. Of 1123 participants, 290 men and 271 women were randomised to screening with stress myocardial perfusion imaging (MPI); 311 men and 251 women were randomised to no screening. Follow-up was 4.8±0.9 years for the occurrence of cardiac events (CE; cardiac death or non-fatal myocardial infarction). The frequency of abnormal screening was similar in men (24%) and women (19%), (p=0.2), although women trended to have smaller MPI abnormalities. CE rates were lower in women than men (1.7% vs. 3.8%, p=0.04). No CEs occurred in 17 high-risk (UKPDS risk engine) women, whereas 14 (11.2%) occurred in 125 high-risk men. Asymptomatic women with T2DM have significantly better cardiac outcomes than their male counterparts and represent a subgroup for which screening for coronary artery disease does not appear warranted.
Keywords
Introduction
The prospective randomised Detection of Ischemia in Asymptomatic Diabetics (DIAD) study 1 sought to assess the prevalence of inducible myocardial ischaemia in asymptomatic individuals with type 2 diabetes mellitus (T2DM) and to identify a profile of individuals at high risk for silent myocardial ischaemia and adverse cardiac outcomes. Despite a significant prevalence of inducible ischaemia (22%), the overall outcome in DIAD participants was unexpectedly favourable, with a cardiac event rate of only 2.9% over 4.8 years.1,2 Subsequent analysis showed that more than one-half of DIAD participants were considered at intermediate/high risk by the United Kingdom Prospective Diabetes Study (UKPDS) risk engine.3,4 However, the overall cardiac event rate in the high-risk groups was still relatively low. 3 Thus, a more precise identification of a subgroup of asymptomatic individuals at highest versus lowest risk remains highly relevant. One of the predictors of adverse outcome in DIAD was male gender. 1 To what extent outcomes in women were more favourable was heretofore not analysed. In the DIAD study an approximately equal number of men and women were enrolled. Accordingly, the aim of the present analysis was to compare in men and women the prevalence and severity of myocardial perfusion abnormalities and the subsequent occurrence of cardiac events, and to test the hypothesis that female gender protects asymptomatic women with diabetes against adverse outcomes.
Methods
Study design
Between the years 2000 and 2002, 1123 asymptomatic individuals with T2DM, from 14 diabetes clinics in the United States and Canada, were enrolled in the DIAD study.1,2 Patients were eligible if they were asymptomatic from a cardiovascular standpoint, 50–75 years of age, and had T2DM by the prevalent criteria of the World Health Organisation and the American Diabetes Association. Patients with angina pectoris or equivalent symptoms, coronary artery disease (CAD), heart failure or coronary revascularisation, or a stress test or coronary angiography within the prior 3 years were not eligible. In addition, patients with a resting electrocardiogram (ECG) indicating ischaemia or left bundle branch block, a clinical indication for stress testing, bronchospasm precluding the use of adenosine, or a limited life expectancy due to other co-morbidities were also excluded. 2 The DIAD protocol was approved by the institutional review boards at each participating centre. The participants in the study provided written informed consent.
At enrolment, all participants, 522 women and 601 men, underwent clinical and physical evaluation with assessment for diabetic neuropathy and cardiac autonomic dysfunction. In addition, they had baseline laboratory testing. Some 561 participants (290 men and 271 women) were randomised to screening for inducible ischaemia, and 562 (311 men and 251 women) to no screening (Figure 1).
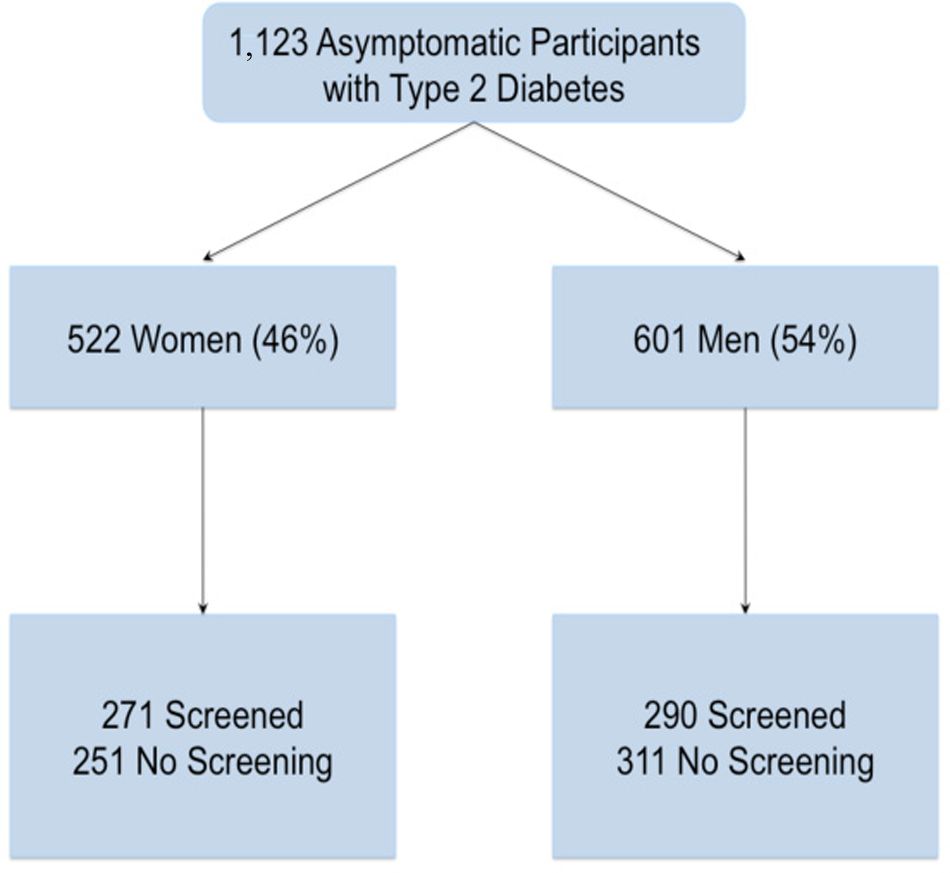
Flow of study participants.
In a post-hoc analysis, all DIAD men and women were stratified according to their baseline risk for developing CAD using the UKPDS risk engine, 4 which generates a score on the basis of age, gender, duration of diabetes, smoking, systolic blood pressure, total cholesterol, high density lipoprotein, ethnicity and haemoglobin A1c level. The UKPDS risk score allows for stratification into three risk categories for having non-fatal or fatal CAD within 10 years. Participants categorised as low risk were predicted to have a < 14% 10-year risk, those categorised as intermediate risk a 15–30% risk, and participants categorised as being at high risk have a > 30% 10-year risk. 4
After randomisation, medical treatment was at the discretion of the participants’ physicians, who were notified of the screening results. The DIAD protocol did not mandate any specific follow-up plan, such as angiography or revascularisation after screening. All participants underwent follow-up for 5 years, completed in September 2007.
Screening with myocardial perfusion imaging
At enrolment into the study, randomised participants were screened for inducible ischaemia with ECG-gated adenosine Tc-99m sestamibi myocardial perfusion imaging (MPI). MPI was performed in accordance with the standards published by the American Society of Nuclear Cardiology. 5 The screening MPI results were interpreted by consensus by an expert panel, blinded to clinical and outcomes data. MPI defects were categorised as small, moderate or large on the basis of quantitative analysis software. 2 Non-perfusion abnormalities were defined as ischaemic ECG changes during adenosine infusion, transient ischaemic dilation or left ventricular dysfunction.
Statistical analysis
Data are presented as mean ± standard deviation for continuous variables and as number and percentages for categorical variables. Statistical analysis was performed using Minitab 15 statistical software (Minitab, State College, PA, USA). The predefined primary outcomes were cardiac death and non-fatal myocardial infarction (MI). The predefined secondary outcomes were unstable angina, heart failure, stroke and coronary revascularisation. 1 A panel, blinded to randomisation status, adjudicated all cardiac events. The chi-square, two-tailed Fisher’s exact test and test of contingency were used to compare distributions of categorical variables, and t-test to compare the means of continuous variables. Kaplan–Meier curve analysis was used to compare primary cardiac events in men and women. The log-rank test was used to test survival distribution differences between groups. A p-value of < 0.05 was considered statistically significant.
Results
Baseline demographics
Table 1 shows the baseline characteristics of men and women. There were no differences in age, duration of diabetes, glycaemic control and treatment with insulin between genders. However, women had higher body mass index, more frequent hypertension and metabolic syndrome, higher total cholesterol and higher high-density lipoprotein than men. Only 50 (9.6%) of the women were pre-menopausal at enrolment into the study. The baseline predicted UKPDS cardiovascular risk was significantly lower in women compared with men (p < 0.0001), as could be anticipated since gender is a component of the assessment. Although 75% of men were at intermediate or high risk, 71% of women were at low UKPDS risk. Only 3.3% of women were at high risk, compared with 21% of men (Table 1).
Baseline characteristics of men and women participating in the DIAD study.
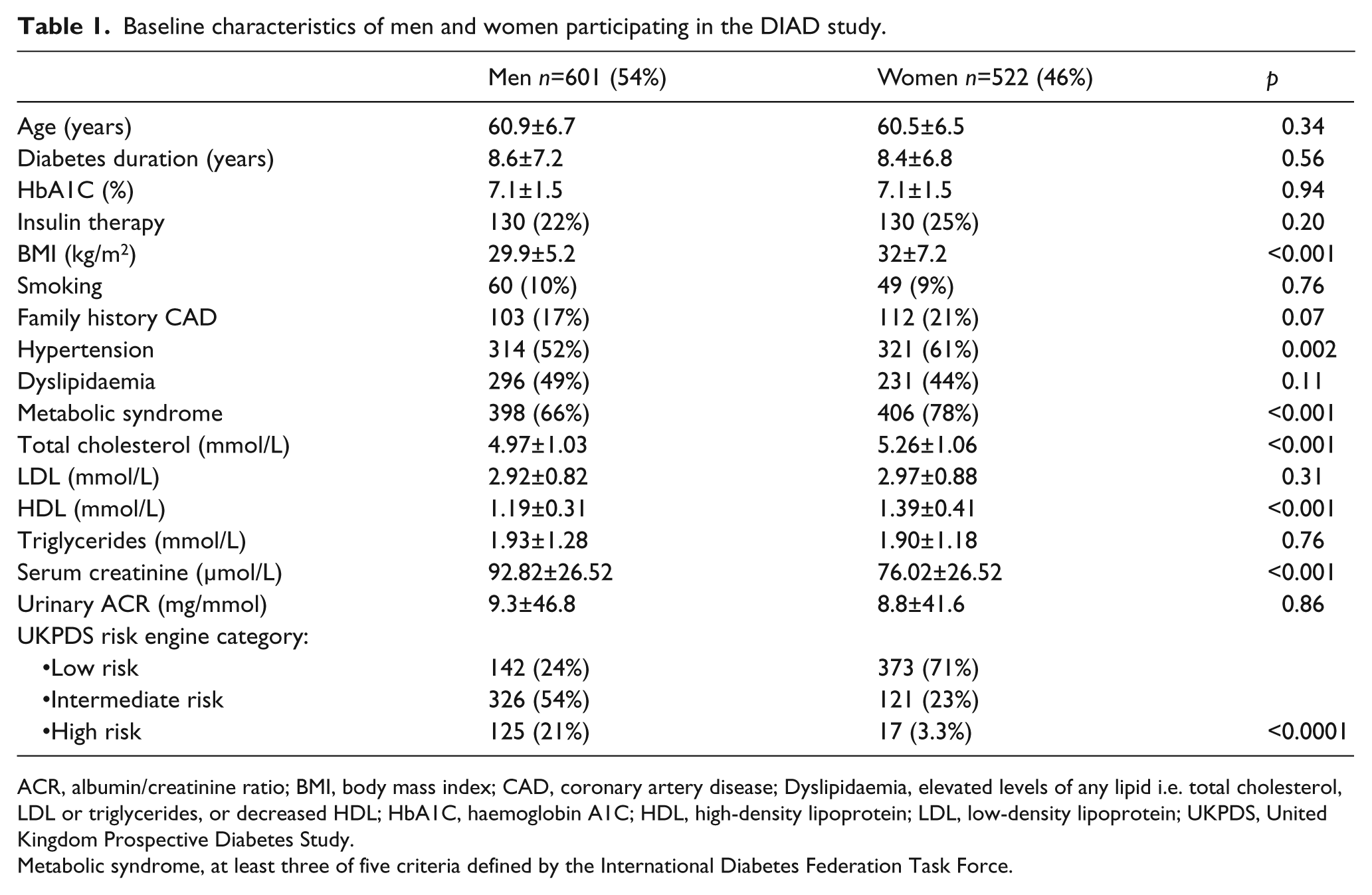
ACR, albumin/creatinine ratio; BMI, body mass index; CAD, coronary artery disease; Dyslipidaemia, elevated levels of any lipid i.e. total cholesterol, LDL or triglycerides, or decreased HDL; HbA1C, haemoglobin A1C; HDL, high-density lipoprotein; LDL, low-density lipoprotein; UKPDS, United Kingdom Prospective Diabetes Study.
Metabolic syndrome, at least three of five criteria defined by the International Diabetes Federation Task Force.
Myocardial perfusion imaging
Overall, the prevalence of abnormal screening MPI (Table 2) was not statistically different between genders: 47 (19%) women and 66 (24%) men had abnormal MPI (p = 0.2). However, women trended to have fewer moderate or large MPI abnormalities and more non-perfusion abnormalities compared with men (p = 0.053, Table 2). Of note, 18 (86%) of 21 participants with ischaemic ECG changes during adenosine infusion were observed in women (p < 0.001).
Results of adenosine SPECT myocardial perfusion imaging at initial screening in men and women.
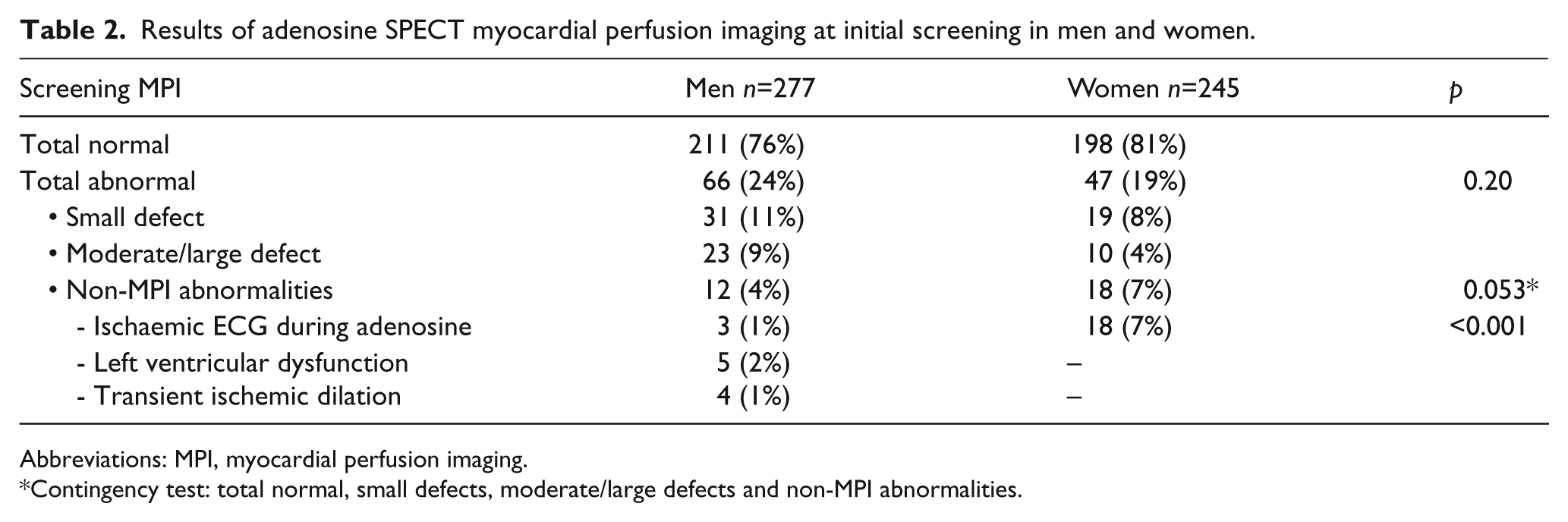
Abbreviations: MPI, myocardial perfusion imaging.
Contingency test: total normal, small defects, moderate/large defects and non-MPI abnormalities.
Cardiac event rates
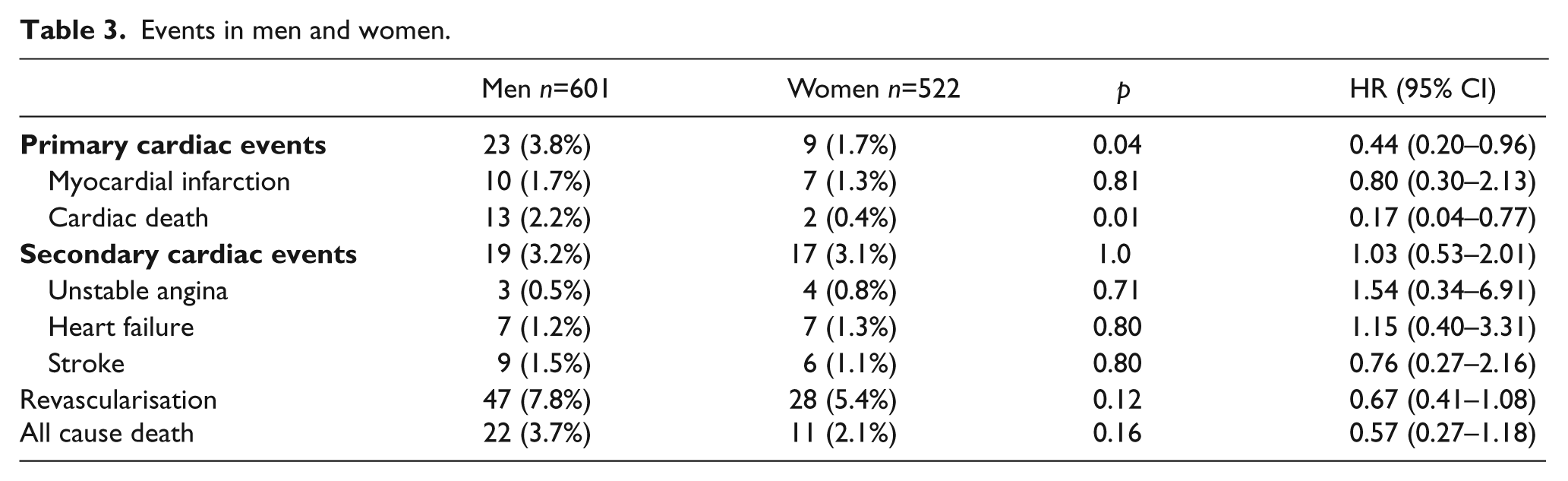
Overall, 32 (2.4%) primary cardiac events (cardiac death or MI) occurred during an average 4.8-year follow-up (Table 3). The primary cardiac event rate was significantly lower in women: women had nine (1.7%) events compared with 23 (3.8%) in men (p = 0.047). There was no difference in the occurrence of non-fatal MI; seven (1.3%) in women and 10 (1.7%) in men (p = 0.81). However, cardiac death occurred significantly more frequently in men (13 (2.2%)) than in women (two (0.38%)), (p = 0.01). Fourteen of these deaths were sudden deaths. Figure 2 shows the cumulative primary cardiac event rate in men vs. women (log rank p = 0.042).
Events in men and women.
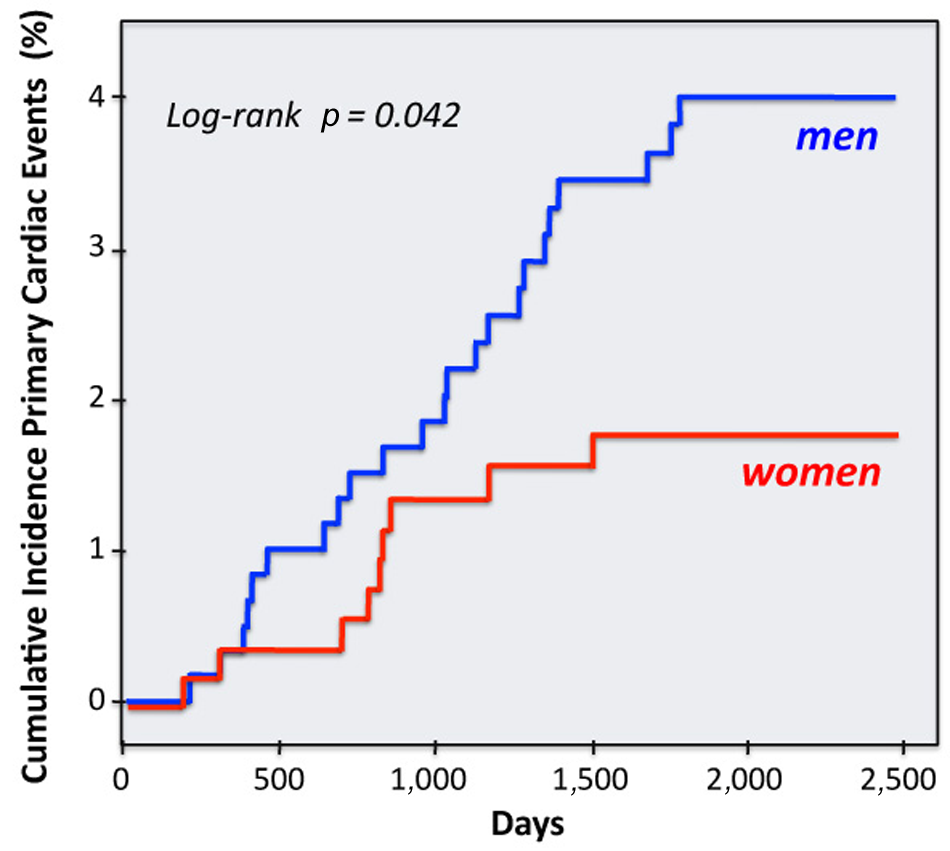
Cumulative incidence of primary cardiac events in men and women.
Secondary cardiac events, including unstable angina, heart failure, stroke and revascularisation were not significantly different between the genders (Table 3).
UKPDS risk score and cardiac events
Primary cardiac event rates are shown in Figure 3 in relation to risk predicted by the patients’ UKPDS score. High-risk men had 14 (11.2%) primary cardiac events, whereas only six (1.8%) and three (2.1%) primary events occurred in intermediate and low-risk men (p < 0.001). Primary cardiac events were very few in women, possibly precluding meaningful statistical analysis. However, low-risk women had three (0.8%) and intermediate-risk women had five (4.1%) primary cardiac events, while no primary cardiac event occurred in the 17 women classified as high risk (p = 0.03).
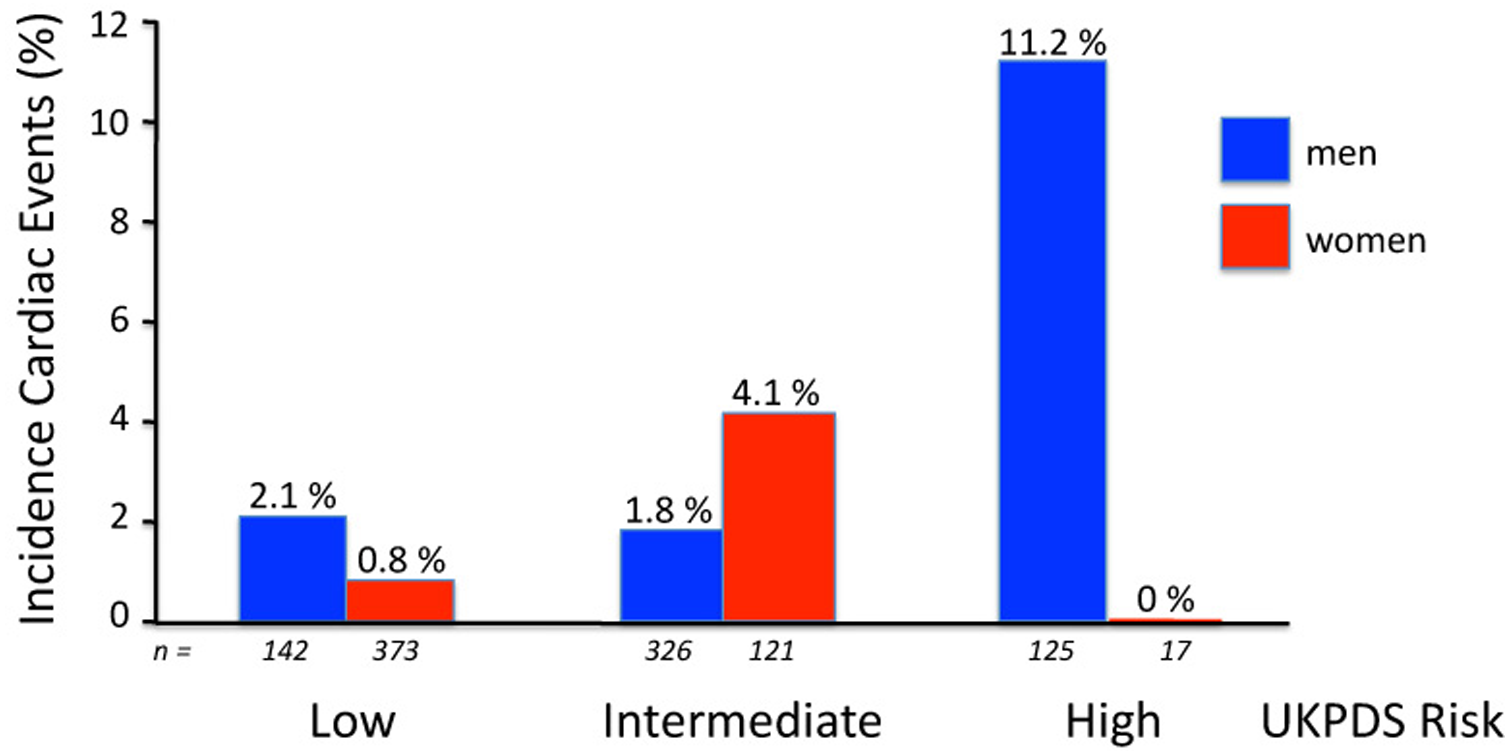
Incidence of primary cardiac events in men and women, categorised into low, intermediate or high cardiovascular risk by the United Kingdom Prospective Diabetes Study (UKPDS) risk engine.
Screening MPI results and cardiac events
The association between results of screening MPI and outcomes in the overall DIAD population has been published previously. 1 Of 66 men with abnormal MPI, six (9%) had cardiac events (six deaths). Of 211 men with normal screening MPI, five (2.3%) had cardiac events (one death and four non-fatal MIs) (p = 0.02 vs. abnormal MPI). In contrast, of 47 women with abnormal screening MPI, only one (2%) had a non-fatal MI, whereas of 198 women with normal screening MPI, three (1.5%) had cardiac events (one death and two non-fatal MIs) (p = 0.57 vs. abnormal MPI).
Of 23 men with moderate or large MPI abnormalities, four (17%) had cardiac death, whereas none of the 10 women with moderate or large MPI defects had any cardiac event.
Of three men with ischaemic ECG changes, one experienced cardiac death, whereas of 18 women with ischaemic ECG changes, one sustained a non-fatal MI. Because of the small number of events in women, meaningful comparative statistical analysis between genders is not feasible.
Screening status and cardiac events
Consistent with the results reported previously for the overall DIAD study group, 1 we found that screening did not affect primary outcomes in either women or men (Table 4). The primary cardiac event rate was not different in 271 women randomised to screening compared with 251 women randomised to no-screening (four (1.5%) vs. five (2.0%), p = 0.74), and also not different in 290 men randomised to screening and 311 men randomised to no screening (11 (3.8%) vs. 12 (3.9%), p = 1.0). Secondary cardiac event rates were also not different in either men or women, randomised to screening vs. no screening (Table 4).
Discussion
The prospective randomised DIAD study is the first to show that asymptomatic women with T2DM have significantly better cardiovascular outcomes than asymptomatic men. These results are of interest because of epidemiological observations that cardiovascular mortality in T2DM over the last two decades has decreased in men, but not to the same extent in women.6–8 Indeed, one survey suggested that cardiovascular mortality may actually be increasing in diabetic women. 9 Moreover, a meta-analysis of 37 cohort studies, comprising 447,064 patients, revealed that the relative risk for fatal coronary heart disease associated with diabetes was 50% higher in female than male participants. 10 In those with symptomatic CAD, numerous studies have shown that diabetic women have significantly worse outcomes than men after acute MI, percutaneous coronary interventions and coronary artery bypass grafting.11–13 Finally, in a retrospective study, women with diabetes and abnormal stress MPI also had worse outcomes than men, despite comparable MPI abnormalities. 14 Professional societies therefore consider women with diabetes to be at high risk for cardiovascular disease, and have focused their efforts on the prevention and early detection of CAD in this group. 15 Although the literature highlights the important impact of diabetes in symptomatic women, it should not be misconstrued to indicate that therefore asymptomatic diabetic women are therefore also at higher cardiovascular risk compared with men.
Overall, there was no difference between genders in the prevalence of inducible ischaemia in the DIAD study. However, women tended to have fewer moderate or large MPI abnormalities than men, consistent with their observed more favourable outcomes. In the whole DIAD analysis, moderate or large MPI abnormalities were associated with a six-fold higher cardiac event rate than participants with no or small MPI abnormalities. 1 Interestingly, however, while moderate or large MPI defects were predictive of cardiac events in men, they were not in women.
In the context of growing concerns about cardiovascular complications in the increasing number of diabetic women, the results of our study are somewhat reassuring: asymptomatic women with diabetes, but without known CAD, appear to be at a very low risk for cardiac events. Yet, it should be appreciated that the DIAD participants generally had good glycaemic control at baseline (HbA1c ~ 7%), and a large majority were receiving optimal contemporary medical care to reduce cardiovascular risk factors, with 67% taking statins, 75% on anti-hypertensive therapy and 74% on prophylactic anti-platelet therapy at study conclusion. 1 Thus, these results may be viewed as bolstering the need for aggressive preventive strategies to ensure such favourable outcomes.
Although baseline clinical characteristics of women and men in the DIAD study were otherwise similar, the UKPDS risk engine predicted lower cardiovascular risk in women by virtue of their gender, and this was borne out in our analysis. Specifically, the UKPDS calculator designated more than three out of four women at low risk, while, in contrast, a similar proportion of men were at intermediate-to-high risk. The highest actual cardiac event rate (11.2%, or ~ 2% per year) was observed in the 125 men with high UKPDS risk scores, which constituted 21% of the male cohort. In contrast, there were no events in the few women (n = 17) with high UKPDS risk scores, which constituted 3.3% of the female group.
In the DIAD study other statistical predictors of adverse outcome were male gender, duration of diabetes, the presence of microalbuminuria, peripheral vascular disease, serum creatinine and low-density lipoprotein levels, and cardiac autonomic dysfunction. 1 However, in spite of statistically significant hazard ratios, the positive predictive value of each of these predictors was very low (ranging from 6–9%), indicating their limited practical value for identifying individual patients at risk. Furthermore, except for gender, the number of participants with these predictors was small, precluding further meaningful statistical sub-analysis to define the interaction of these factors on risk.
Consistent with the previously published overall analysis of the DIAD study, screening with adenosine MPI did not affect outcome in either men or women. The appropriateness and the effectiveness of screening asymptomatic patients with diabetes remains controversial. However, the results of our prospective randomised investigation challenge the notion that general screening is of any benefit. Certainly, screening should no longer be recommended broadly in an asymptomatic diabetic patient population meeting the DIAD eligibility criteria. The analysis of the DIAD study reported herein extends these observations to suggest that screening asymptomatic women may be a particularly ineffectual strategy. The clinician might instead focus on diabetic patients who have high-risk characteristics, such as those identified in the present analysis – males with a high-risk UKPDS score. However, it still remains to be proven that early detection of sub-clinical CAD in this cohort and its subsequent contemporary management would actually improve clinical outcomes versus simple clinical observation with interventions when and if symptoms of CAD emerge.
Strengths and limitations
The DIAD study focused on silent CAD and subsequent cardiac outcomes. Therefore, we selected the composite primary endpoint of cardiac death or non-fatal MI. Other trials in diabetic patients have included stroke in addition as a primary endpoint.16,17 If stroke (Tables 3 and 4) were to be included in the composite primary endpoint of the DIAD study, the 5-year event rate still would be low at 4.2% (0.8% per year) and remain significantly lower in women than in men (2.9% vs. 5.3%, p=0.04).
The DIAD study is the first large prospective randomised trial to investigate the effects of screening of asymptomatic patients with T2DM on cardiovascular outcomes. However, the DIAD study was not powered to evaluate differences in outcomes between men and women randomised to screening and no screening. Nevertheless, it seems doubtful that even with larger numbers of male and female participants, clinically significant outcome differences would be realised.
Conclusions
Asymptomatic women with T2DM have a much more favourable 5-year cardiovascular outcome than asymptomatic men. Screening for silent myocardial ischaemia by adenosine MPI did not affect outcomes in either gender. Although the appropriateness of screening remains a contentious topic, the current results clearly indicate that there is no role for the screening of asymptomatic women with T2DM because of their very low risk of cardiac event rate under contemporary care. Whether early detection of sub-clinical CAD is warranted in the subgroup of high-risk asymptomatic men cannot be addressed in the DIAD study because of lack of statistical power, and so the hypothesis that screening might actually improve clinical outcomes in high-risk individuals remains unproven.
Footnotes
Appendix
Funding
This work was performed with the support of the General Clinical Research Centers at Yale University (National Institutes of Health M01-RR-00125), University of Rochester (NIH 5M01-RR-00847), and Tulane University (NIH 6M01-RR-05096). The DIAD was supported by grants from Bristol Myers-Squibb Medical Imaging (North Billerica, Massachusetts, USA) and Astellas Pharma (Deerfield, Michigan, USA), who also provided Technetium-99m Sestamibi (Cardiolite®) and Adenosine (Adenoscan®) for study patients. DIAD is an investigator-initiated study. The industrial sponsors had no role in the design or conduct of the study, in the collection, analysis or interpretation of data, or in the preparation of the manuscript.
Conflict of interest
None
Study concept and design: Drs Wackers, Young, Chyun, Inzucchi.
Recruitment of patients, acquisition of data: The DIAD Investigators (see above under Clinical Centres).
Analysis and interpretation of data: Drs Wackers, Tandon, Bansal, Young, Chyun, Inzucchi, and Staib.
Drafting of the manuscript: Drs Wackers, Tandon, Inzucchi, and Young.
Critical revision of the manuscript for important intellectual content and final approval: Drs Wackers, Tandon, Bansal, Inzucchi, Young, Staib, Chyun, Ms Davey.
Statistical analysis: Dr Staib.
Adjudication cardiac events: Drs Young, Wackers, Chyun.
Administrative, technical or material support: Dr Wackers, Ms Davey, Natale.
Study supervision: Dr Wackers, Ms Davey.