
Abstract
Aims:
A major proportion of patients with diabetic foot syndrome are older than 65 years. Little is known about outcomes of these elderly patients.
Methods:
We analysed 245 treatment cases in an observational single-centre study for comorbidities and outcomes over a 6-month period.
Results:
In all, 122 patients had peripheral arterial disease which was significantly increasing with age (n = 245, df = 1, χ2 = 23.06, p ⩽ 0.0001). Increasing age correlated positively with decreasing rate of revascularisations (n = 122, df = 1, χ2 = 4.23, p = 0.039). In total, 23 (9.3%) patients died in the observation period. In-hospital mortality was 2.8%, percentage of major amputations 2.8%. In the invasively treated subgroup, 13 out of 67 patients died within the observation period. Death after revascularisation was independent of age (n = 67, df = 1, χ2 = 2.05, p = 0.153). Mobility decreased in the whole study group with increasing age. The risk of decrease with age was not influenced by revascularisation status.
Conclusion:
With careful interdisciplinary evaluation, elderly patients with diabetic foot syndrome can be treated with favourable outcome. Mobility before and after treatment deserves more attention as a predictor of treatment success and outcome parameter.
Introduction
Average life expectancy is continuously increasing in developed countries. Prevalence of diabetes and the incidence of diabetic foot syndrome (DFS) are increasing with age. A major proportion of patients with DFS treated in hospital are older than 65 years. The impact of age on treatment and prognosis of DFS has been studied little. 1 In younger patients, the treatment strategy is aggressive revascularisation and infection control to prevent major amputations. In contrary, many older individuals are vulnerable to aggressive invasive procedures. They often decline functionally after hospitalisation even without bed rest. They can experience new and worsened functional impairment that improves at a much slower rate than the acute illness. 2 The aim of our study was therefore to analyse outcomes of elderly patients with DFS.
Methods
Study design and population
In a single-centre, observational study, we analysed outcomes of patients with DFS dependent on age. Retrospectively, we identified in our electronic patient records all treatment cases in 2007. In all, 245 patients could be followed up until death or for 6 month after first presentation. Data were pseudonymised and analysed for the diagnosis of peripheral arterial disease (PAD), demographic data, risk factors, comorbidities, extensive lower extremity arterial revascularisations, major amputations, mobility at discharge and mortality.
Diagnosis of PAD, peripheral neuropathy and management of diabetic foot ulcers
All patients were treated according to protocols based on the International Consensus on the Diabetic Foot. 3 A standardised questionnaire and examination was performed. PAD assessment included evaluation of pedal pulses and ankle-brachial pressure index (ABPI). PAD was considered to be present if ABPI was <0.9 or >1.3 and/or two foot pulses were absent. This led to further evaluation with magnetic resonance angiography or arteriography. Evaluation of peripheral neuropathy (PNP) included testing of sensation of 10 g monofilament, vibration sensation (128 Hz tuning fork) and cold/warm discrimination. PNP was diagnosed if two or more of the aforementioned tests were abnormal.
Decision about revascularisation procedures
All patients with PAD were evaluated for revascularisation in an interdisciplinary diabetic foot board. Decisions about revascularisation and the kind of procedure were made in consent.
Evaluation of mobility
Mobility was evaluated at discharge. Homebound or community bound mobility was interpreted as preservation of mobility, while bed rest or preserved transfer to chair resp. wheel chair was interpreted as immobile.
Statistical analysis
Data were analysed by logistic regression using SAS, version 9.1 (Cary, NC). All dependent variables were dichotomous, only the parameter ‘age’ was introduced in the statistic model as an independent continuous variable. p < 0.05 was interpreted as statistically significant.
Results
Age distribution of patients
The mean age of patients was 71 years: minimum 33 years and maximum 98 years. Approximately, 75% of 245 patients were older than 65 years, 40% even older than 74 years. Only 8% of patients were older than 84 years. In all, 88 (35.9%) were females and 157 (64.1%) were males.
PAD as one main cause of DFS
In our study group of 245 patients, 122 were identified to have PAD. The mean age of patients with PAD was 75 years, minimum 50 years and maximum 98 years, while the mean age of patients without PAD was 67 years ranging from 33 to 94 years. PAD is significantly increasing with increasing age (n = 245, df = 1, χ2 = 23.06, p ⩽ 0.0001). Demographic data, risk factors and comorbidities of the study population with PAD are shown in Table 1.
Demographic data, risk factors and comorbidities of the study population with PAD.
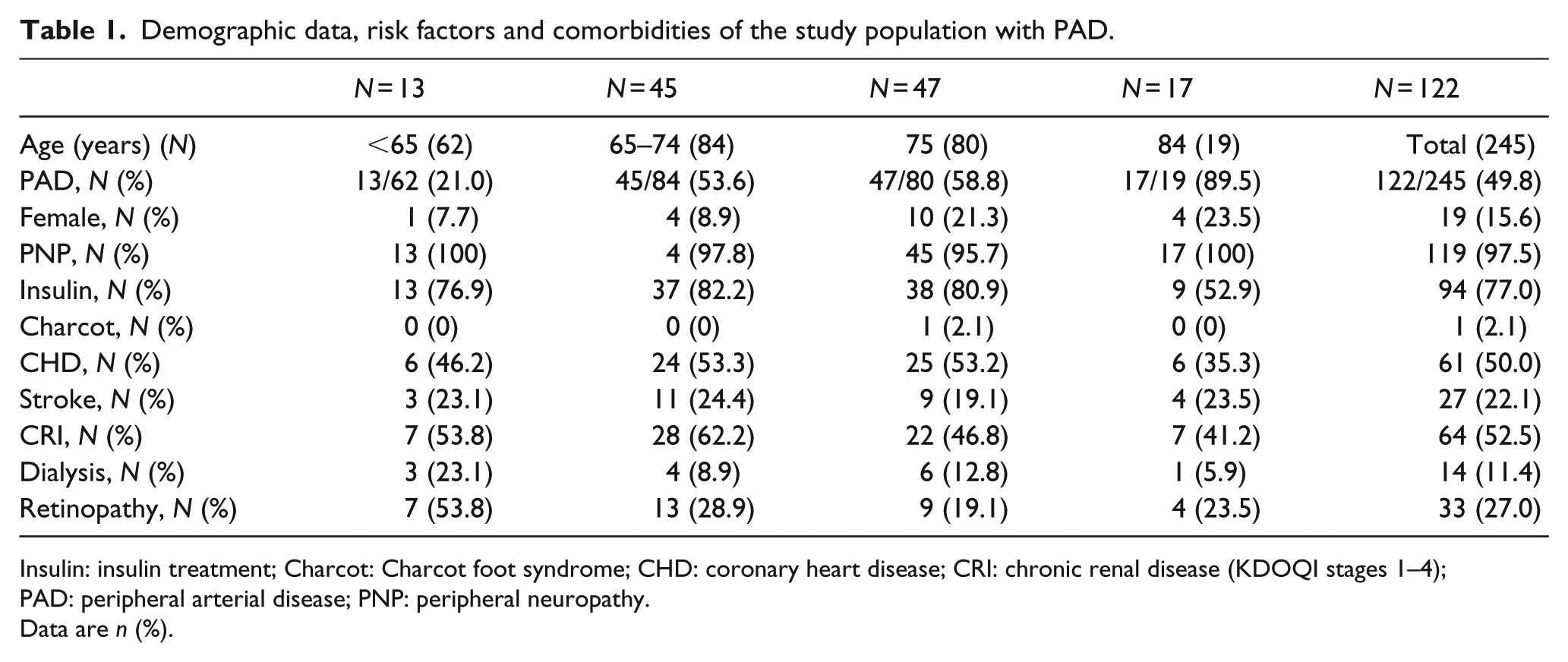
Insulin: insulin treatment; Charcot: Charcot foot syndrome; CHD: coronary heart disease; CRI: chronic renal disease (KDOQI stages 1–4); PAD: peripheral arterial disease; PNP: peripheral neuropathy.
Data are n (%).
Revascularisation decreases with older age
Increasing age correlated significantly positive with decreasing rate of revascularisations (n = 122, df = 1, χ2 = 4.23, p = 0.039). Patients under 65 years of age were revascularised most frequently (84.6% of patients), 55.6% in the age group between 65 and 74 years, 44.7% between 75 and 84 years and 47.1% in the group older than 84 years.
Outcome and benefit of revascularisation dependent on age group
Revascularisation was performed in 67 out of 122 patients with PAD, 22 were revascularised by angioplasty and 45 by bypass graft procedures. There were 7 (2.8%) major amputations in the intervention group, none in the group without intervention. Risk of major amputations was independent of age (N = 67, df = 1, χ2 = 0.526, p = 0.47). In the whole study group (n = 245), 23 (9.3%) patients died in the observation period of 6 months. In-hospital mortality was 2.8% (7 of 245), of whom the majority (5 of 7) died as a direct result of diabetic foot disease. In all, 16 patients died after discharge, 9 from cardiac diseases or stroke, 4 from malignancies, 1 from urinary tract infection and with only 2 as a direct consequence of DFS. Age correlated positively with the risk of death as expected (n = 245, df = 1, χ2 = 9.87, p = 0.002). In the invasively treated subgroup, 4 out of 67 patients died in hospital and 7 later on in the 6-month observation period. Death after revascularisation was independent of age (n = 67, df = 1, χ2 = 2.05, p = 0.153). In the different age groups, death rates were 9.1%, 8.0%, 27.3% and 22.0%.
Mobility decreased with increasing age in the whole study population (n = 245, p = 0.02). In the different age groups, percentages of mobile patients decreased from 80.6%, 71.4%, 57.5% to 52.6%. In the revascularisation subgroup, mobility decreased with age in patients with PAD: 72.7%, 80.0%, 42.9% to 37.5%.
Age has a significant effect on immobility (p = 0.0201). Revascularisation does not significantly affect mobility (p = 0.4940) and there is no difference in the relationship between mobility and age between the groups (p = 0.8701). In other words, revascularisation does not seem to affect mobility nor across age groups.
Discussion
To our knowledge, our study is the first one analysing outcomes of DFS dependent on age. It is limited by its retrospective and observational design with data from one single centre. It arises from our daily work in hospital with elderly patients and we wanted to know whether our routine strategies are advantageous for elderly patients. In our study population, the amputation rate (2.8%) is low and comparable to other studies reporting 8.7% or 5% major amputations after 1 year of observation.4,5 Rates of amputations were independent of age in contrast to other studies.
Our study might reflect the observation described by Benoit et al., that outcome of patients with chronic limb ischemia improved over the past 2 decades even if revascularisation was not an option.6,7
Our data indicate that the main burden of DFS in the elderly is not due to the rates of amputations but due to the loss of mobility. It is known that even short hospital stays lead to rapid functional decline in elderly patients.8,9 As a Swedish study showed, the subgroup of elderly patients is very heterogeneous. Health status varies from good functioning and no morbidity to multimorbidity and severe disability. 10 A Finnish study shows that independent living could be maintained in the majority of the patients after revascularisation for PAD in a population with median age of 92 years, predominantly in patients mobile before treatment. 11 Thus, mobile older individuals should be treated more aggressively following general principles of diabetic foot care. However, homebound ambulation, dementia and end-stage renal disease are risk factors for deterioration of ambulation among individuals with chronic limb ischemia. 12 That means that, in frail individuals with DFS, a more conservative management may be preferred.
Our findings changed our therapeutic strategies. We focus now on preservation of mobility from the first day in hospital. We started special training groups that exercise in sitting position with offloading of the foot wound to preserve muscular strength and coordination. With careful selecting patients for revascularisation, focussing on minimal invasive treatments, early mobilisation and special exercises, we hope to reach the important endpoints for elderly people with DFS: low risk of mortality and amputations and preservation of mobility with good quality of life.
Footnotes
Acknowledgements
We wish to acknowledge the impact of routine daily work of physicians and staff caring for our patients with diabetic foot syndrome. Without their continuous accurate work and documentation, our analysis would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.