
Abstract
Objective:
To evaluate additional role of left atrial two-dimensional speckle tracking echocardiography in patients with diabetes mellitus type 2, 218 patients with heart failure with preserved left ventricular ejection fraction divided according to the presence of diabetes mellitus (108 with and 110 without) were enrolled in the study.
Methods:
Traditional parameters using two-dimensional echocardiography and Doppler imaging were measured as expressions of left ventricular diastolic function as well as peak atrial longitudinal strain and peak atrial contraction strain were measured using two-dimensional speckle tracking echocardiography.
Results:
Global average peak atrial longitudinal strain and peak atrial contraction strain were significantly lower in patients with diabetes mellitus (p = 0.002 and p = 0.001, respectively) and its reduced values were significantly associated with higher prevalence of diabetes mellitus (p = 0.002 and p = 0.001, respectively), its greater severity (p = 0.002 and p = 0.016, respectively) and longer duration only for global average peak atrial longitudinal strain (p = 0.030). Multiple linear regression analysis demonstrated that the presence of diabetes mellitus appeared as independent predictor of reduced global peak atrial longitudinal strain [B = −2.173; 95% confidence interval: −3.870 to (−0.477); p = 0.012] as well of reduced global peak atrial contraction strain [B = −1.30; 95% confidence interval: −2.234 to (−0.366); p = 0.007].
Conclusion:
Two-dimensional speckle tracking echocardiography appeared as a useful additional tool for detection of left atrial dysfunction in patients with heart failure who have preserved left ventricular ejection fraction and diabetes mellitus who are especially prone to develop cardiovascular complications.
Keywords
Introduction
Numerous epidemiological and clinical studies have shown a high prevalence of diabetes mellitus (DM) in patients with heart failure who have preserved left ventricular ejection fraction (HFpEF). This rate, which varies from approximately 30%–40%, most likely contributes to the increased morbidity and mortality in the DM population.1–7 Observational and clinical studies in asymptomatic patients with DM type 1 and/or type 2 have shown a prevalence of left ventricular (LV) diastolic dysfunction (DD) from 20% to 75%, mainly depending on patient selection and the echocardiographic markers used for diagnosing DD.7–13 Most of the current noninvasive methods for diagnosis of DD 14 and/or HFpEF 15 rely on determining the increase in left atrial (LA) volume and/or LV filling pressures as markers of its severity and duration. However, several recent studies suggest that the degree of elevated LV filling pressures may not fully explain LA failure and that LA myocardial fibrosis and LA remodelling may play a role in the LA dysfunction in patients with HFpEF.16–20 Additionally, the ability of two-dimensional (2D) speckle tracking echocardiography (STE) to provide a quantitative assessment of the longitudinal myocardial LA deformation mechanics further enables the characterization of LA impairment in patients with HFpEF,21–23 especially those with DM.20,24,25 All these findings suggest that the use of LA deformation mechanics can help detect LA dysfunction earlier than standard measurements, thus mediating the cardiovascular risk in patients with diabetes. To this end, our study aimed to evaluate the role of LA longitudinal strain using 2D speckle tracking in standard echocardiographic measurements of DD in patients with DM and HFpEF.
Methods
Study population
This was a prospective, cross-sectional study examining 218 consecutive patients who presented with multiple atherosclerotic risk factors and were referred for cardiology assessment to either an academic cardiology clinic or a private specialist clinic in Skopje. Patients with unexplained dyspnoea and/or exercise intolerance who fulfilled clinical and/or echocardiographic criteria of HFpEF presence – dyspnoea, preserved left ventricular ejection fraction [LVEF > 50% or left ventricular end diastolic volume index (LVEDVI) < 97 mL/m2] and DD along with elevated LV filling pressure (E/E′ > 15) – were enrolled in the study. 15 In patients with an intermediate E/E′ average ratio between 8 and 15, the additional parameters of DD were implemented. These included an E/A ratio <0.5 and/or deceleration half-time (DT) >280 ms in patients over 50 years (7.3% and 8.6% of patients with E/E′ < 15, respectively), and/or a duration difference of atrial reverse pulmonary vain flow and atrial mitral valve flow (Ar-A) >30 ms (8.6% of patients with E/E′ < 15), and/or a left atrial volume index (LAVI) >40 mL/m2 (41.1% of patients with E/E′ < 15) and/or increased LV mass index (LVMI: men > 149 g/m2, women > 122 g/m2) (91.4% of patients with E/E′ < 15).14,15
Data on the presence of DM or pre-diabetes state were confirmed by chart review (blood tests and/or use of anti-diabetic medications) and medical history intake at the time of echocardiography. The severity of DM was assessed using the principal treatment regimen for DM, highlighting the use of insulin as greater severity of DM.
To be eligible for the study, patients had to have a sinus rhythm, normal lung function tests and normal blood counts. Patients with a history of recent (⩽6 months) acute coronary syndrome, coronary artery bypass grafting, more than moderate mitral regurgitation or more than mild disease of the other valves, hypertrophic obstructive cardiomyopathy, atrial fibrillation, pulmonary disease or anaemia were excluded. Patients with a history of coronary artery disease (CAD), post-percutaneous coronary intervention (>6 months) or post-myocardial infarction (>6 months) were not excluded if they showed preserved LV ejection fractions and had no significant coronary artery stenosis. Patients were included if they were on chronic medications, including beta-blockers or nondihydropyridines calcium blockers.
The Medical Ethics Committee of involved institutions approved the study protocol, and signed informed consent was obtained from all enrolled patients.
Echocardiography study
Standard assessments of LV dimensions, wall thickness and mass were performed in standard views on commercially available equipment (Vivid 7; GE, USA) according to the professional association recommendations. 26 LV volumes and ejection fraction were calculated using the biplane method of discs (modified Simpson’s rule) 26 Relative wall thickness (RWT) was measured as RWT = 2×(PWTd/LVIDd), where d was the end-diastole. LAVI was derived using the biapical area-length method and indexed to body surface area (BSA). 26 Mitral flow using pulsed-wave Doppler was recorded as recommended and early (E) and late (A) transmitral inflow velocities, deceleration time (DT) as well using continuous-wave Doppler isovolumetric relaxation time (IVRT) were measured. 14 Pulmonary venous flow using pulsed-wave Doppler was recorded and peak systolic (S), early diastolic (D), S/D ratio and atrial reversal flow (Ar) including Ar-A duration difference were measured and calculated as recommended. 14 The ratio of LV peak E-wave velocity to flow propagation velocity assessed by colour M-mode was calculated. 14 Pulsed-wave tissue Doppler imaging (TDI) was performed in the apical four-chamber view to assess annular early and late diastolic velocities. 14 The recording was performed at a sweep speed of 100 mm/s at end-expiratory apnoea. The septal, lateral and average early diastolic velocity (E′) and late diastolic velocity (A′) were recorded, and the ratio of mitral flow E-wave to E′ for each of these annular velocities was calculated. Tissue Doppler was not performed in patients with dense mitral annular calcification. The average of three consecutive cardiac cycles was taken for measurement of each echocardiographic index.
LA speckle tracking longitudinal strain analysis
LA speckle tracking longitudinal strain was assessed using conventional 2D grey scale echocardiography.22,27–29 During breath hold, three consecutive heart cycles were recorded and averaged. The frame rate was set between 55 and 80 frames per second. Recordings were processed using acoustic-tracking software (Echo Pac; GE), allowing off-line semi-automated analysis of speckle-based strain. LA endocardial border was first traced manually and subsequently the software automatically delineated this region of interest (ROI) into six segments in both four- and two-chamber views. After the segmental tracking quality was assessed and eventually manually adjusted again (Figure 1), the longitudinal strain curves were generated by the software for each atrial segment (Figure 2). In patients in whom some segments were excluded because of the impossibility of achieving adequate tracking, calculations were done by averaging the values measured in the remaining segments. Peak atrial longitudinal strain (PALS), measured at the end of the reservoir phase, and peak atrial contraction strain (PACS), measured just before the start of the active atrial contraction phase, were calculated by averaging the values observed in all accepted LA segments (global PALS and PACS) (Figures 1 and 2) in four- and two-chamber views.22,27–29
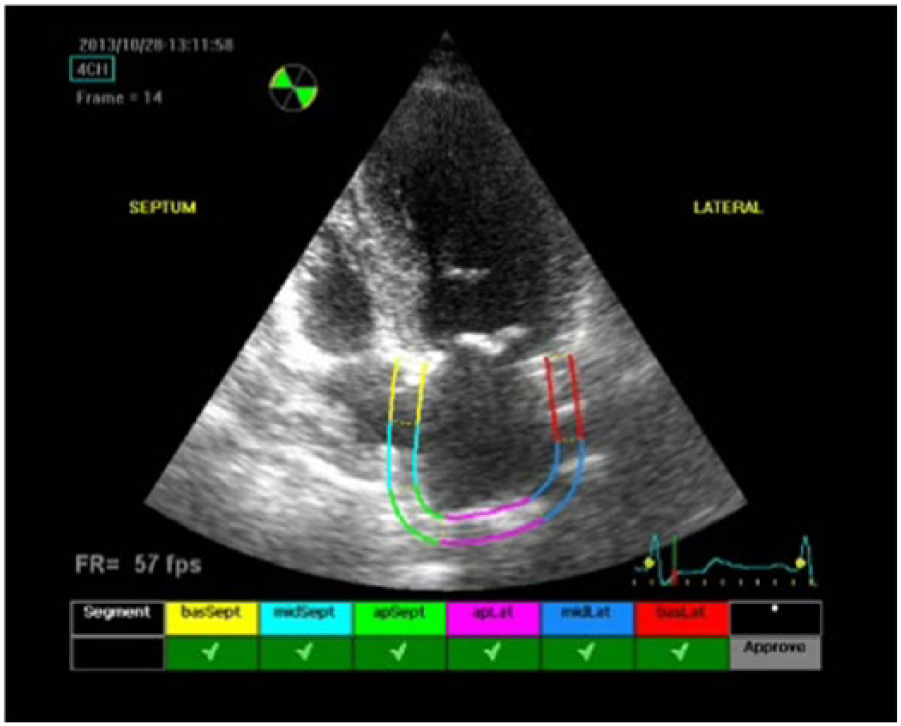
Tracing LA endocardia border and automatically delineating a region of interest (ROI) into six segments in four-chamber view.
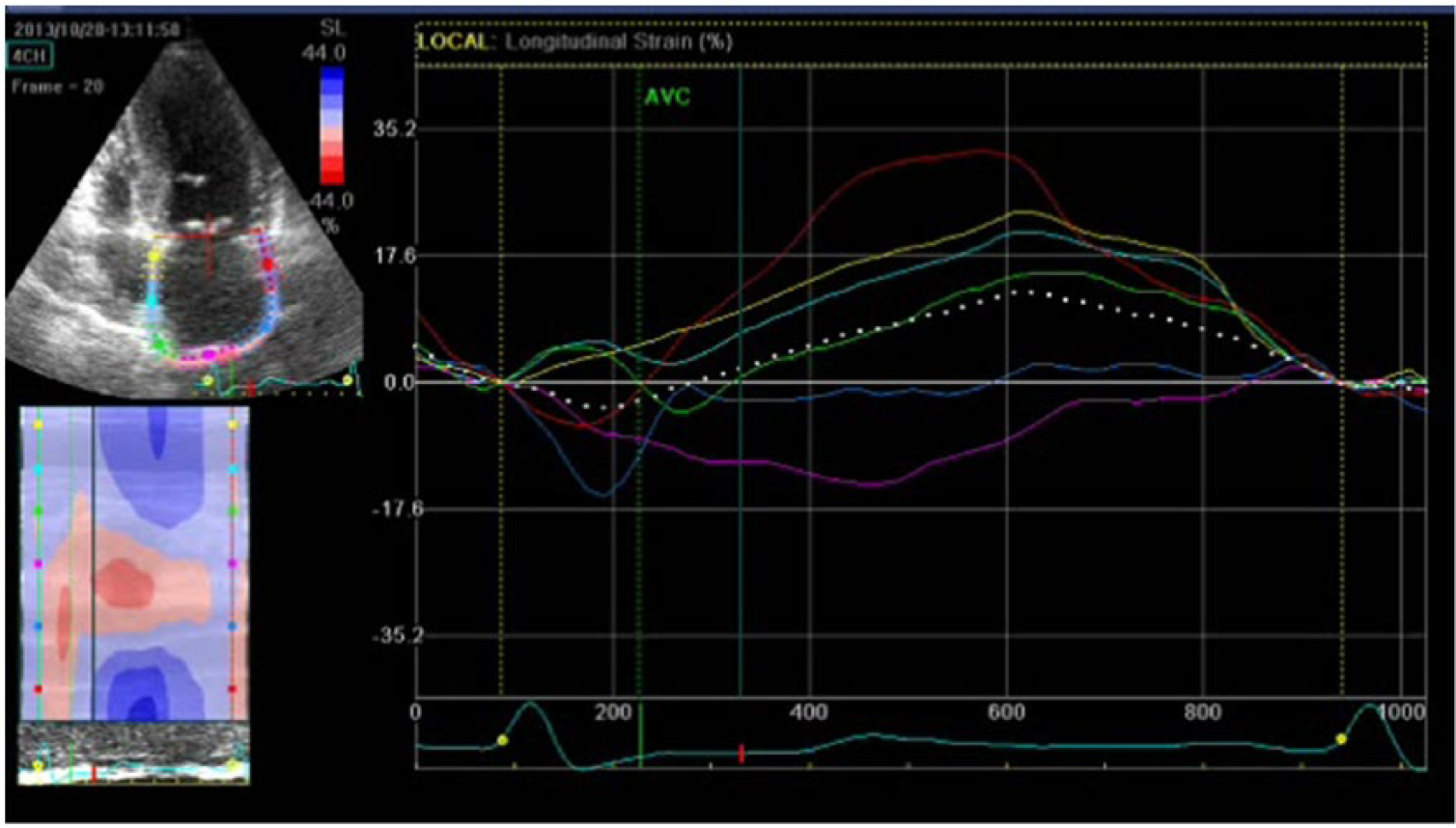
LA tracing in order to measure peak atrial longitudinal strain (PALS) and peak atrial contraction strain (PACS) in four-chamber view.
Reproducibility
In order to assess the reproducibility as well as reliability of the LA strain measurements, we calculated the intraclass correlation coefficient (ICC) by assessing 20 randomly selected images seen in two different occasions by the same investigator.
Statistical analysis
The categorical parameters were summarized as percentages and continuous parameters as mean ± standard deviation (SD). Comparisons between the two groups with and without DM were performed using Student’s t test for continuous parameters and Pearson’s chi-square test for categorical parameters. Assessment of correlation of global average PALS and PACS with various echocardiographic parameters was done using Pearson’s correlation analysis. Multiple linear regression analysis was performed to determine independent predictors of reduced global average PALS and/or PACS. The area under the receiver operating characteristics (ROC) curve (AUC) was performed in order to quantifying the added value of LA strain parameters over TDI parameters to discriminate patients with and without DM. All data analysis was performed using SPSS version 22.0 (IBM SPSS, Inc., Chicago, IL, USA) and p-value ⩽0.05 was considered significant.
Results
Baseline characteristics
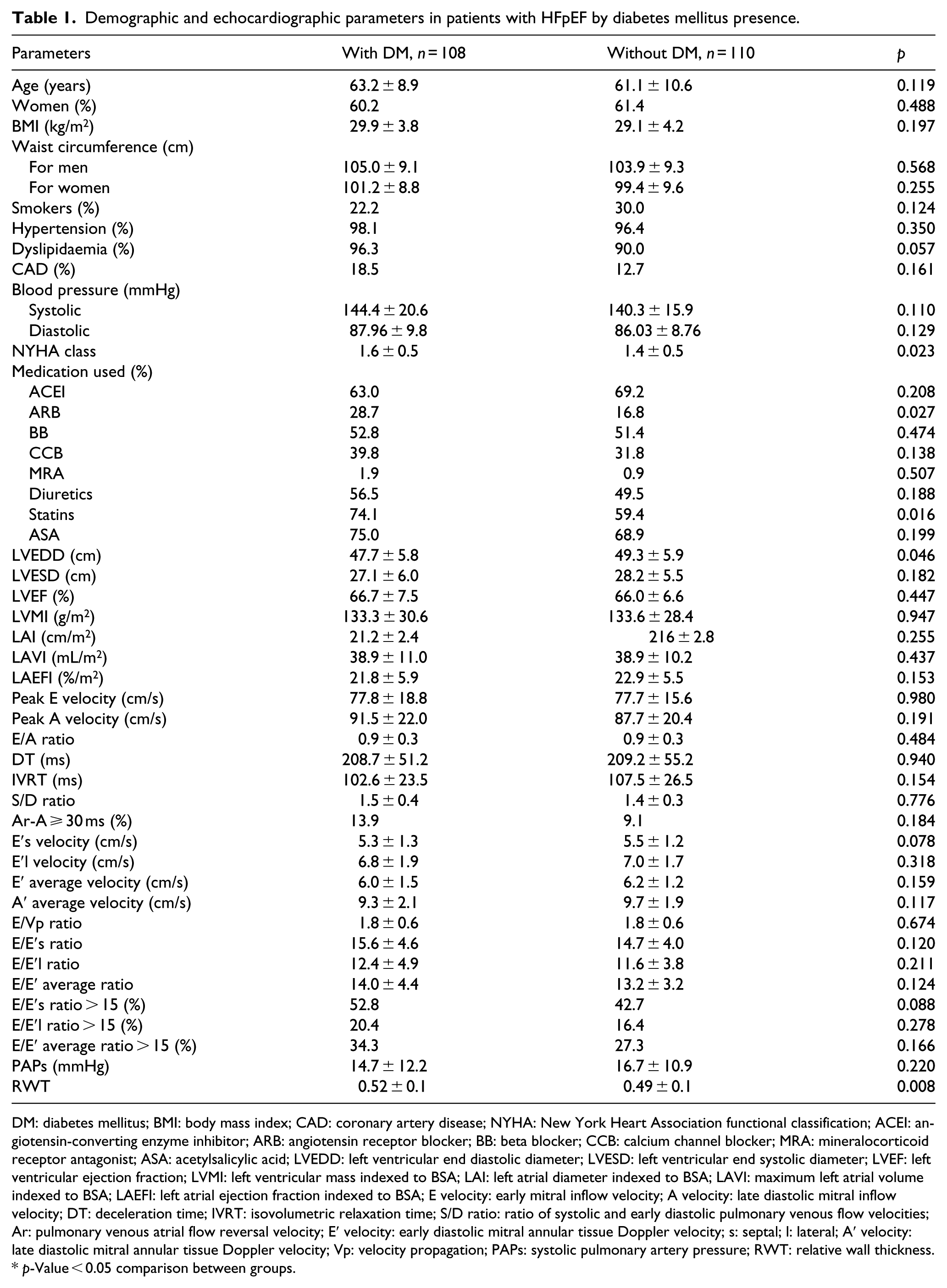
The baseline characteristics of the study cohort are listed in Table 1. Of all patients, 108 (49.5%) had DM type 2. The mean duration of DM was 5.0 ± 6.6 years. Of all patients with DM, 28.7% were on insulin therapy, 13.0% on combination of insulin and tablets, 44.4% on tablets while 13.9% were put only on a diet. Patients with DM were insignificantly older, had higher body mass index (BMI) and wider waist circumference. Additionally, the patients with DM had insignificantly higher incidence of hypertension as well higher values of systolic and diastolic blood pressure, dyslipidaemia and CAD, but were less likely to be smokers. Patients with DM had more pronounced symptoms during physical activity manifested by significantly higher New York Heart Association (NYHA) functional class (p = 0.023). Assessment of correlations showed existence of significant association between higher NYHA functional class and DM presence (r = 0.155, 0.023), its duration (r = 0.163, p = 0.017) and severity (r = 0.192, 0.005). Angiotensin receptor blocker (ARB) was significantly more frequently used in patients with DM (p = 0.027), along with more frequent use of other medications (Table 1).
Demographic and echocardiographic parameters in patients with HFpEF by diabetes mellitus presence.
DM: diabetes mellitus; BMI: body mass index; CAD: coronary artery disease; NYHA: New York Heart Association functional classification; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; BB: beta blocker; CCB: calcium channel blocker; MRA: mineralocorticoid receptor antagonist; ASA: acetylsalicylic acid; LVEDD: left ventricular end diastolic diameter; LVESD: left ventricular end systolic diameter; LVEF: left ventricular ejection fraction; LVMI: left ventricular mass indexed to BSA; LAI: left atrial diameter indexed to BSA; LAVI: maximum left atrial volume indexed to BSA; LAEFI: left atrial ejection fraction indexed to BSA; E velocity: early mitral inflow velocity; A velocity: late diastolic mitral inflow velocity; DT: deceleration time; IVRT: isovolumetric relaxation time; S/D ratio: ratio of systolic and early diastolic pulmonary venous flow velocities; Ar: pulmonary venous atrial flow reversal velocity; E′ velocity: early diastolic mitral annular tissue Doppler velocity; s: septal; l: lateral; A′ velocity: late diastolic mitral annular tissue Doppler velocity; Vp: velocity propagation; PAPs: systolic pulmonary artery pressure; RWT: relative wall thickness.
p-Value < 0.05 comparison between groups.
LV systolic and diastolic parameters
Table 1 illustrates the LV parameters for the entire cohort. All patients fulfilled criteria for HFpEF having preserved LVEF. Comparison of neither systolic nor diastolic parameters showed statistical difference between patients with and without DM. Patients with DM in comparison to those without had significantly higher values of RWT (p = 0.008), and as expected according to inclusion criteria, all patients had some degree of DD. Patients with DM were more likely to have an E/E′ septal, lateral and average ratio over 15, compared to those without (52.8% vs 42.7%, p = 0.088; 20.4% vs 16.4%, p = 0.278; 34.3% vs 27.3%; p = 0.166, respectively); however, this difference was not statistically significant. Lower E′ at either the septal or lateral level or taken as average along with higher E/E′ measured at the same levels did not show any significant association with DM presence. However, lower E′ at the septal level as well as higher E/E′ ratio at the septal level and taken as average showed significant association with DM duration (r = −0.168, p = 0.013; r = 0.215, p = 0.001; r = 0.181, p = 0.007, respectively) and with its greater severity (r = −0.174, p = 0.010; r = 0.159, p = 0.019; r = 0.123, p = 0.069, respectively).
LA volume and function
The LA dimension and maximum volume indexed to BSA were above the expected values for patients with HFpEF, but they were almost identical in groups of patients with and without DM (p = 0.437 and p = 0.437, respectively), just as were parameters of LA function (Table 1). There was a lack of significant association of DM presence, its longer duration and/or severity with any of parameters of LA volume and function.
LA strain measurements
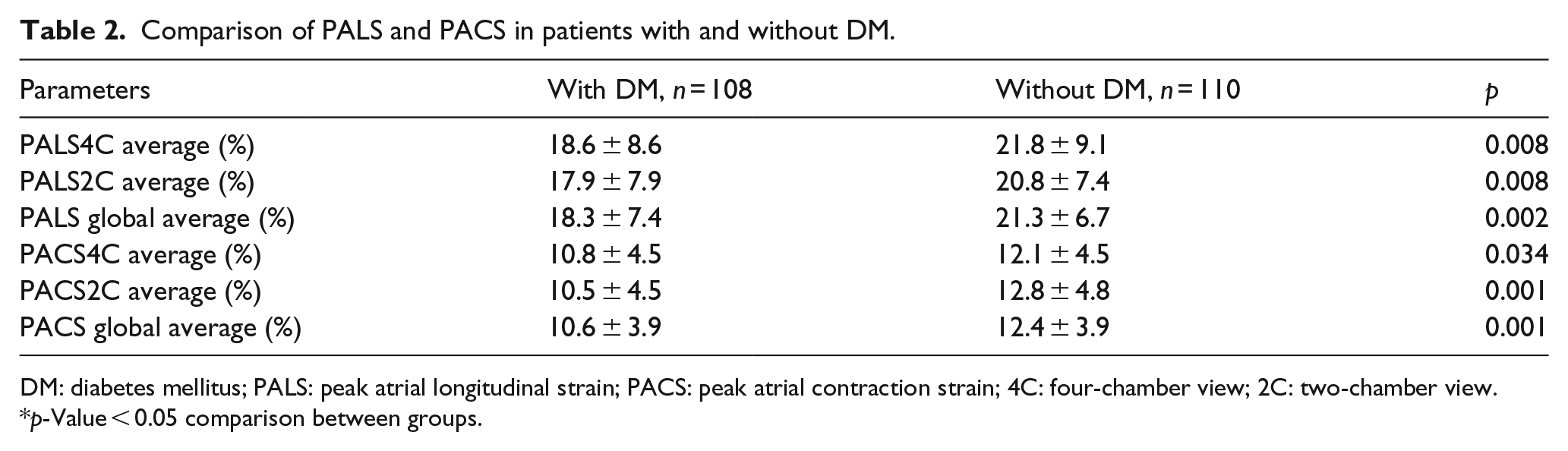
PALS and PACS in two- and four-chamber average as well as global strain (derived as an average) were reduced and significantly lower in the DM group in comparison to those without DM (Table 2). Reduced global average PALS and PACS were significantly associated with increased age (r = −0.213, p = 0.002; r = −0.149, p = 0.029, respectively), female gender (r = −0.192, p = 0.005; r = −0.197, p = 0.004, respectively), higher NYHA functional class (r = −0.138, p = 0.044; r = −0.152, p = 0.026, respectively) and more frequent use of diuretics (r = −0.190, p = 0.005; r = −0.180, p = 0.009, respectively) or only for global average PALS use of mineralocorticoid receptor antagonist (MRA) medications (r = −0.138, p = 0.045). There was significant association of reduced global average PALS and PACS with higher prevalence of DM (r = −0.205, p = 0.002; r = −0.217, p = 0.001, respectively), its longer duration only for global average PALS (r = −0.148, p = 0.030) and its greater severity (r = −0.210, p = 0.002; r = −0.1649, p = 0.016, respectively). As for echocardiographic parameters, reduced global PALS was significantly associated with most of the echocardiographic measures of reduced diastolic function, as well as decreasing values of LA functional parameters (Table 3). When we performed a correlation analysis only for patients with DM, the result was similar. Thus, reduced global PALS in patients with DM was significantly associated with increased age (r = −0.205, p = 0.033), and along with global PACS with echocardiographic parameters of impaired LA volume and/or reduced LA function as well impaired diastolic function (Table 4). The ICC for global PALS average was 0.985 [95% confidence interval (CI): 0.965–0.993] and for global PACS average was 0.932 (95% CI: 0.843–0.971).
Comparison of PALS and PACS in patients with and without DM.
DM: diabetes mellitus; PALS: peak atrial longitudinal strain; PACS: peak atrial contraction strain; 4C: four-chamber view; 2C: two-chamber view.
p-Value < 0.05 comparison between groups.
Significant correlations of global average PALS and PACS with echocardiographic parameters of LV diastolic and LA function in all patients (n = 218).
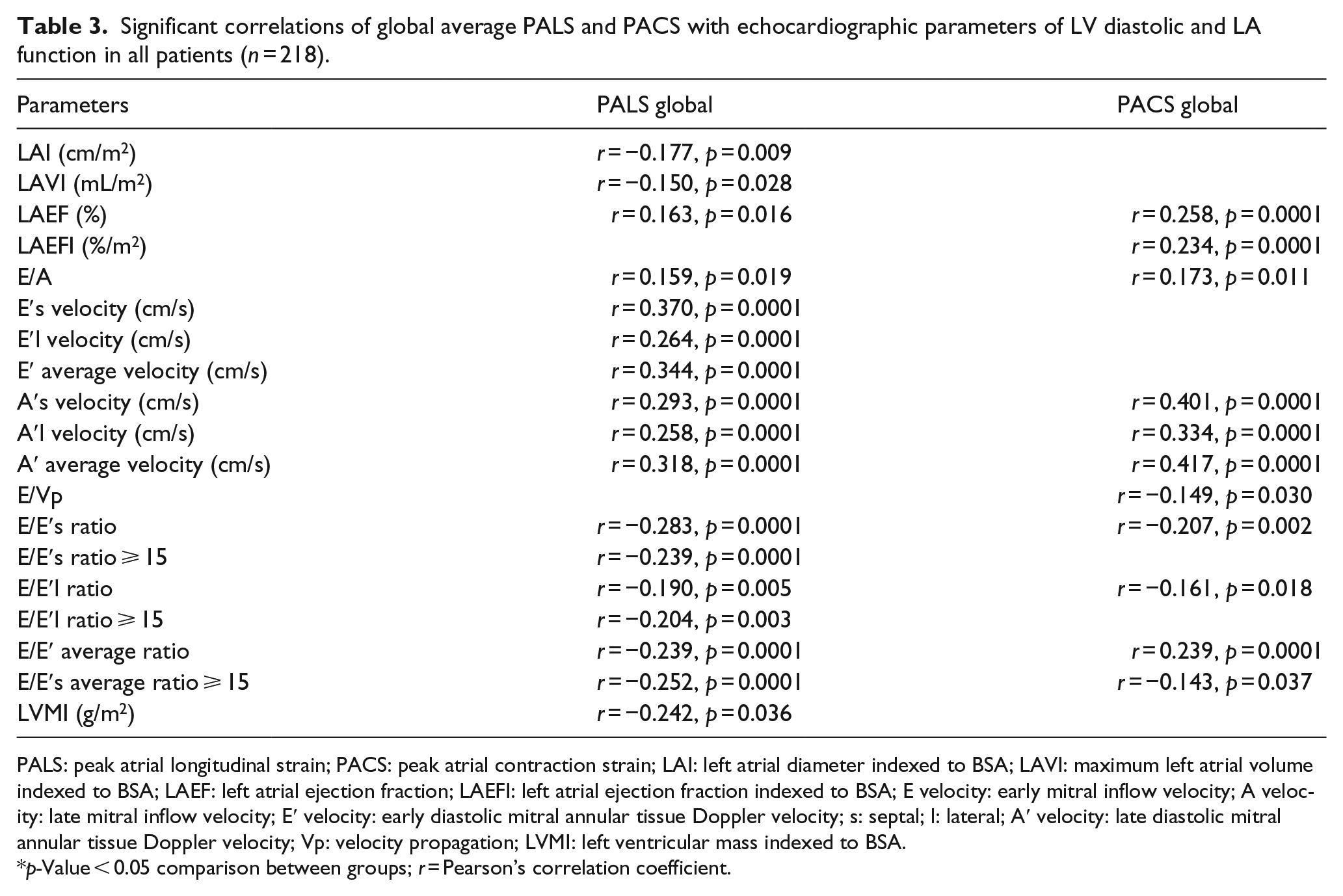
PALS: peak atrial longitudinal strain; PACS: peak atrial contraction strain; LAI: left atrial diameter indexed to BSA; LAVI: maximum left atrial volume indexed to BSA; LAEF: left atrial ejection fraction; LAEFI: left atrial ejection fraction indexed to BSA; E velocity: early mitral inflow velocity; A velocity: late mitral inflow velocity; E′ velocity: early diastolic mitral annular tissue Doppler velocity; s: septal; l: lateral; A′ velocity: late diastolic mitral annular tissue Doppler velocity; Vp: velocity propagation; LVMI: left ventricular mass indexed to BSA.
p-Value < 0.05 comparison between groups; r = Pearson’s correlation coefficient.
Significant correlations of global average PALS and PACS with echocardiographic parameters of LV diastolic and LA function in patients with diabetes mellitus (n = 108).
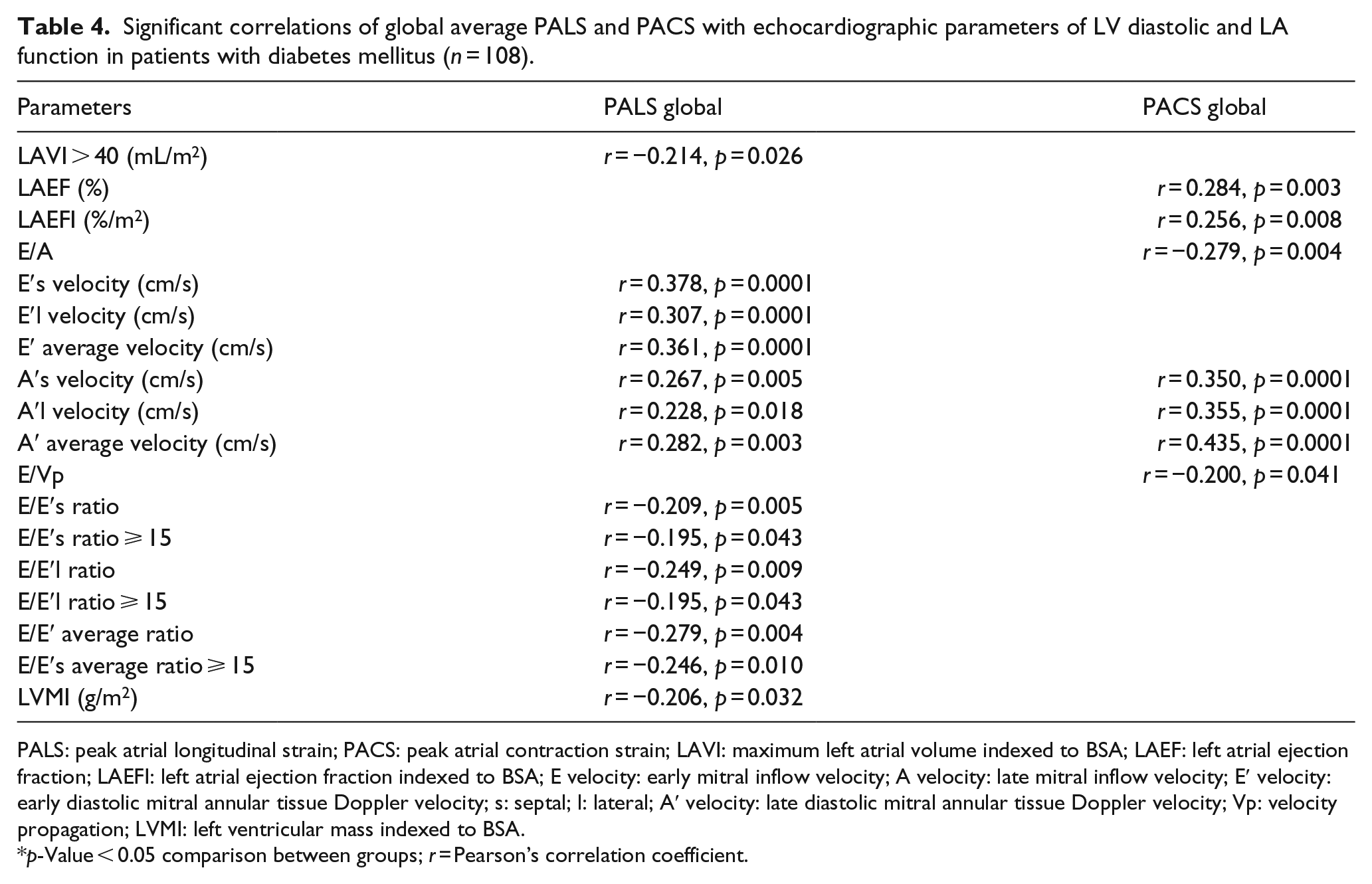
PALS: peak atrial longitudinal strain; PACS: peak atrial contraction strain; LAVI: maximum left atrial volume indexed to BSA; LAEF: left atrial ejection fraction; LAEFI: left atrial ejection fraction indexed to BSA; E velocity: early mitral inflow velocity; A velocity: late mitral inflow velocity; E′ velocity: early diastolic mitral annular tissue Doppler velocity; s: septal; l: lateral; A′ velocity: late diastolic mitral annular tissue Doppler velocity; Vp: velocity propagation; LVMI: left ventricular mass indexed to BSA.
p-Value < 0.05 comparison between groups; r = Pearson’s correlation coefficient.
Predictive variables of reduced global PALS
In order to determine the independent predictors of reduced global PALS and PACS among patients with HFpEF, we performed multiple stepwise linear regression analysis with demographic and echocardiographic covariates that showed significant relation to it. The results demonstrated that presence of DM, female gender, reduced E′septal and reduced A′ average velocity as well as increased LVMI appeared as independent predictors of reduced global PALS (Model 1, Table 5). Age (B = −0.100, p = 0.114), NYHA (B = −0.005, p = 0.994), diuretic use (−0.074, p = 0.243) and DM duration (B = 0.023, p = 0.738) were excluded as nonpredictive demographic variables in the regression analysis. When the predictive model was limited only to patients with DM, again reduced E′septal and A′ average velocity as well as presence of LAVI > 40 appeared as independent predictors of reduced global PALS (Model 2, Table 5). In order to confirm additional role of LA strain in discriminating patients with and without DM, ROC analysis revealed that addition of PALS to reduced E′septal (AUC = 0.576, 95% CI: 0.500–0.652, p = 0.053) and reduced A′ average (AUC = 0.553, 95% CI: 0.476-0.629, p = 0.178) assessed with TDI significantly improved the AUC (AUC = 0.638, 95% CI: 0.565–0.712, p = 0.0001). As for global PACS, the results showed that presence of DM, female gender, reduced A′ average velocity, increased maximal LAVI as well reduced left atrial ejection fraction (LAEF) appeared as independent predictors of its reduced value (Model 1, Table 6). Again, age (B = −0.056, p = 0.392), NYHA (B = −0.039, p = 0.558), diuretic use (−0.092, p = 0.142) and DM duration (B = 0.004, p = 0.950) were excluded as no predictive demographic variables in the regression analysis. As for those with DM, then again reduced A′ average velocity as well as increased E/Vp ratio appeared to be independent predictors of reduced global PACS (Model 2, Table 6). Similarly, in order to discriminate patients with and without DM, addition of PACS to reduced E′septal (AUC = 0.583, 95% CI: 0.507–0.659, p = 0.036) and reduced A′ average (AUC = 0.554, 95% CI: 0.477–0.631, p = 0.169) assessed with TDI significantly improved the AUC (AUC = 0.622, 95% CI: 0.547–0.696, p = 0.002).
Multiple linear regression model of global PALS as dependent parameter and demographic and echocardiographic variables of diastolic function as independent parameters.
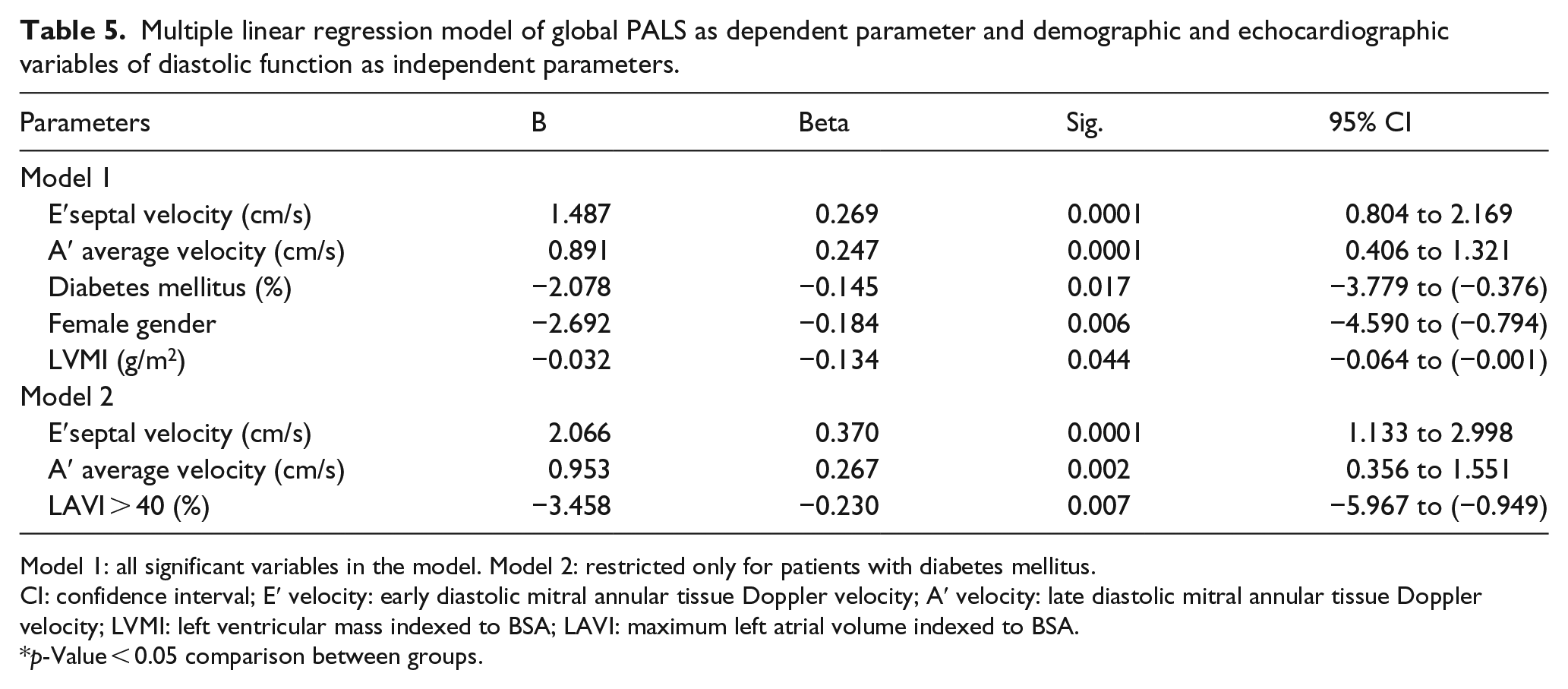
Model 1: all significant variables in the model. Model 2: restricted only for patients with diabetes mellitus.
CI: confidence interval; E′ velocity: early diastolic mitral annular tissue Doppler velocity; A′ velocity: late diastolic mitral annular tissue Doppler velocity; LVMI: left ventricular mass indexed to BSA; LAVI: maximum left atrial volume indexed to BSA.
p-Value < 0.05 comparison between groups.
Multiple linear regression model of global PACS as dependent parameter and demographic and echocardiographic variables of diastolic function as independent parameters.
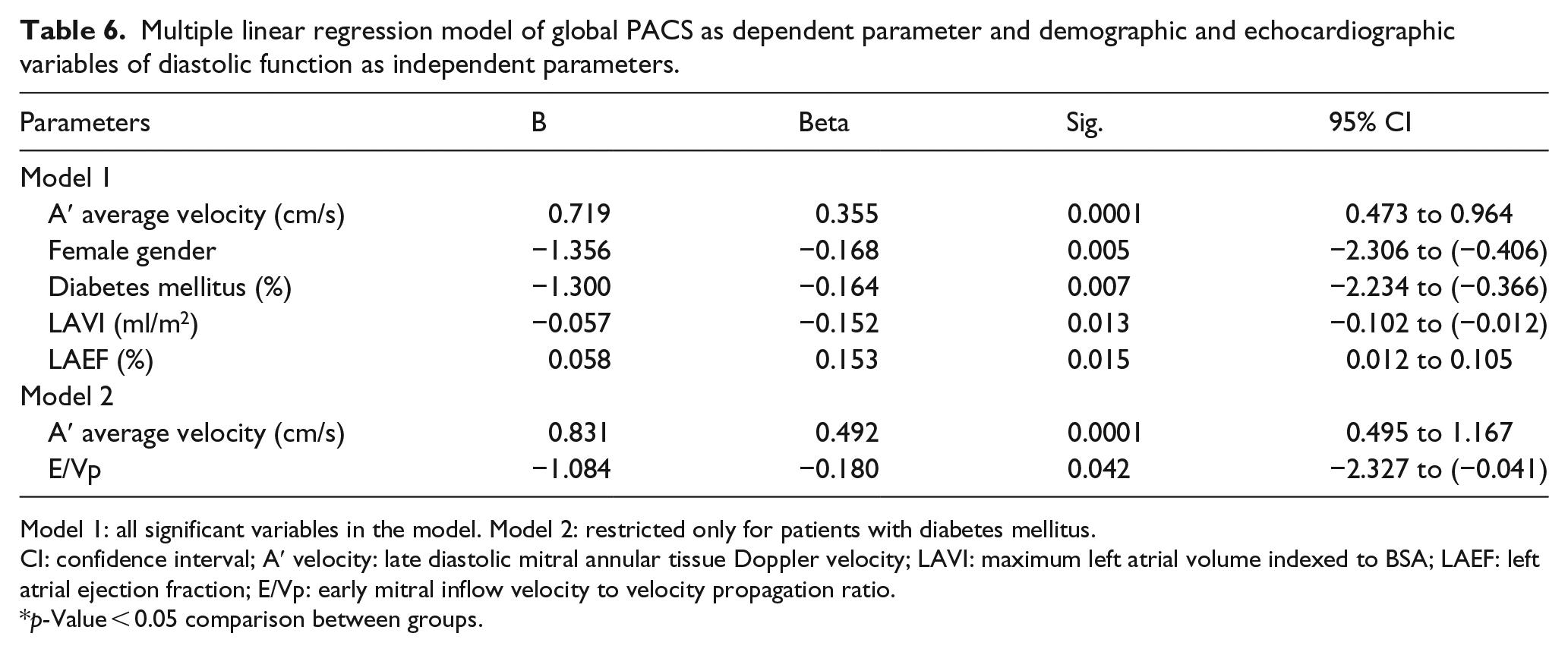
Model 1: all significant variables in the model. Model 2: restricted only for patients with diabetes mellitus.
CI: confidence interval; A′ velocity: late diastolic mitral annular tissue Doppler velocity; LAVI: maximum left atrial volume indexed to BSA; LAEF: left atrial ejection fraction; E/Vp: early mitral inflow velocity to velocity propagation ratio.
p-Value < 0.05 comparison between groups.
Discussion
Baseline characteristics
Analysis of baseline characteristics of 218 patients with HFpEF diagnosed using the widely accepted criteria published by Paulus et al., 15 divided according to the presence of DM, showed that our cohort was made up of mostly individuals over 60 years, overweight with wider waist circumference and with high prevalence of female gender, DM, hypertension and low prevalence of CAD, characteristics that are similar to the results from numerous published studies on patients with HFpEF and represent its distinctive phenotype in comparison to those with reduced LVEF.1,6,30,31 However, regarding these baseline characteristics, patients with DM did not show significant difference when compared to patients without DM (Table 1), except for the NYHA functional class that was significantly higher in patients with DM as well was significantly associated with its presence, longer duration and greater severity. DM is an important co-morbidity in patients with HFpEF, and in accordance with its increased prevalence in the general population and among community-based patients, numerous epidemiological and clinical studies have shown that the prevalence of DM in patients with HFpEF is high, approximately around 30%–40%.1–7 The higher prevalence of DM found in our study might be due to patient selection criteria, given that we involved patients with impaired fasting glucose and/or impaired glucose tolerance who were placed on medication.
DD
Regarding the criteria for diagnosing HFpEF, 15 all 218 patients in our study had preserved systolic function and some degree of DD. However, comparison of LVMI and traditional transmitral inflow and pulmonary flow parameters showed absence of significant differences between patients with and without DM (Table 1). In addition, patients with DM in comparison to those without had insignificantly lower early diastolic mitral annular tissue Doppler velocity (E′) and higher E/E′ ratio either at septal, lateral level or taken as an average, representing higher LV filling pressure, hence more extensive DD. Nonetheless, longer DM duration and its greater severity showed significant association with markers representing higher LV filling pressure or abnormality of relaxation. Our results were consistent with those from numerous observational and clinical studies in asymptomatic patients with DM type 1 and/or type 2 that have shown high prevalence of LV DD.3,7–13 Investigators from the Heart Strong Study 8 demonstrated that abnormalities of diastolic function are common and are independently associated with DM regardless of LV mass, systolic function, hypertension or other comorbidities, but they also demonstrated that DM very often jointly acts with hypertension, suggesting an additive deleterious effects on LV relaxation. Along with this finding, From et al. 32 found a significant association between duration of DM and DD after adjustment for CAD and hypertension, so they speculated that the aetiology of DD must, in part, be due to DM itself or to its consequences. Potential mechanisms contributing to increased DD in diabetic patients are still under investigation, but most frequently mentioned in the literature according to the systematic review of the pathophysiological features underlying HFpEF in DM done by Magri et al. 33 include enhanced interstitial accumulation of advanced-glycated end products (AGES), which include collagen, elastin and other connective tissue proteins, as well as myocardial fibrosis and myocite hypertrophy, abnormal myocardial metabolism, hyperglycaemia, abnormalities in cardiomyocyte calcium handling, increased arterial stiffness, worse endothelial function, myocardial ischaemia due to microvascular disease and presence of autonomic dysfunction. Taking into account all those mechanisms of DD in patients with HFpEF and DM, particular attention has been paid in recent years to the concept of ‘diabetic cardiomyopathy’ as a primary structural and functional myocardial disease, the existence which has been proposed in diabetic patients, that could be expressed subclinically for a long time before symptoms and/or signs of heart failure appear.34–36 In their review, Lam 36 stressed that DM is a risk factor for HFpEF and asymptomatic diabetic cardiomyopathy which represent unique phenotype with preserved ejection fraction and elevated diastolic stiffness as a manifestation of stage B HFpEF that should be targeted for risk management and preventive strategy.
LA volume, function and strain measurements
Most of the current noninvasive methods for diagnosis of DD 14 and/or HFpEF 15 rely on determining the increase in LA volume and/or LV filling pressures as markers of its severity and duration. However, we could not find any significant difference between patients with and without DM regarding LA dimension and LA maximum volume indexed to BSA which were above the normal values as expected for patients with HFpEF (Table 1) as well as for LA function (Table 1). There was a lack of significant association of DM presence, its longer duration and greater severity with any of the parameters of LA volume and function. Given that several recent studies in patients with HFpEF suggest that the degree of elevated LV filling pressures may not fully explain LA failure, thus LA myocardial fibrosis and LA remodelling could be responsible for LA dysfunction,16–20 use of 2D STE possesses a great potential for a quantitative assessment of longitudinal myocardial LA deformation mechanics in order to obtain further insights into impaired LA performance,21–23 especially for patients with DM.20,24,25 Therefore, we performed 2D STE in all patients with HFpEF and found that global PALS and PACS were reduced and significantly lower in the DM group in comparison to those without DM (Table 2). These results were consistent with previous studies done in patients with HFpEF showing that the same fibrotic changes that affect the subendocardial fibres of the LV secondary to comorbidities such as hypertension, DM, obesity and/or hystory of CAD could also affect the subendocardial layer of the LA and could be manifested as LA longitudinal systolic and DD.16,19–25 In addition, all those mechanisms of DD previously mentioned in this text regarding the patients with HFpEF and DM might also have an impact on LA function.24,32–38 Hence, Asbun and Villarreal 39 demonstrated that diabetic cardiomyopathy causes atrial fibrosis with a consequent reduction in LA compliance. Muranaka et al. 25 also suggested that the fibrotic change in LA in DM is responsible for the reduction in atrial phasic function as measured by strain rate parameters. Furthermore, Mondillo et al. 24 showed that LA deformation is impaired in patients with hypertension and/or DM with normal LA size and they suggest that early abnormalities in LA strain may precede changes in traditional 2D measures of LA function. Along with this finding, Kadappu et al. 20 emphasize that DM causes LA enlargement and LA dysfunction which are due to the combination of DD and a coexistent diabetic atrial myopathy. In this respect, Cameli et al., 40 in a population of patients with prevalent hypertension and DM, found that global longitudinal LA strain is a strong and independent predictor of cardiovascular events, even better than the conventional parameters of LA analysis.
The results of our study are consistent with such evidence, as we found that reduced global PALS and PACS in patients with HFpEF and DM was significantly associated with most of the echocardiographic measures of reduced diastolic function, as well as with decreasing values of LA functional parameters (Tables 3 and 4). Multiple regression analysis demonstrated that the presence of DM along with echocardiographic diastolic parameters appeared to be independent predictors of reduced global PALS and PACS (Model 1, Tables 5 and 6) with similar results when the analysis was restricted only to patients with DM. Given that assessment of atrial strain has significant association with conventional TDI measurements, especially that addition of atrial strain parameters to basic models containing TDI significantly improved the AUC in discrimination of patients with and without DM, as well as that inclusion of DM adds significant power in predicting PALS and/or PACS over transmitral velocities assessed with TDI, we could speculate that assessment of LA strain with 2D STE will have additional role in direct evaluation of LA function, especially in the subset of patients prone to cardiovascular complications. In addition, the findings suggest that DD is only partially responsible for the LA remodelling/dysfunction in diabetic patients, and that it is likely that independent atrial myopathy developed as a consequence of DM contributes to these changes.
Limitation of the study
Patients with DM were included in the study regardless of the duration of DM that can affect the inhomogeneity of diabetic effects on LA function. Due to ethical reasons, coronary angiography in asymptomatic patients was not done in our study, although it is the best way to exclude CAD; however, for its exclusion we used solely noninvasive tests. Considering the limitations of classical indices of LA function, assessment of LA strain by speckle tracking may represent a relatively rapid and easy-to-perform technique to explore LA function, due to its semi-automated nature and to its off-line processing, but we have to stress the existence of potential difficulty in accurately obtaining an ROI especially in the region of auricle and the outlet of the pulmonary veins that could be a source of incorrect measurements.
Conclusion
LA deformation mechanics are impaired in patients with DM and HFpEF and they demonstrated significant association with DM presence, its longer duration and greater severity. Assessment of LA strain using 2D STE appeared as a useful additional tool to conventional echocardiographic measurements for detection of LA dysfunction in patients with HFpEF and DM. We believe that the results of our study regarding LA impaired mechanics in patients with DM with HFpEF have significant clinical implications, because they demonstrate the importance of comprehensive assessment of LA function in everyday clinical practice, particularly in this group of patients prone to develop cardiovascular complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.