
Abstract
Aims:
Recent studies have raised concerns regarding increased heart failure in patients on dipeptidyl peptidase-4 inhibitors. We examined whether dipeptidyl peptidase-4 inhibitors, compared to non-incretin–based therapies, have differential effects on left ventricular and endothelial function in patients with type 2 diabetes mellitus.
Methods:
A total of 25 type 2 diabetes mellitus patients commenced on a dipeptidyl peptidase-4 inhibitor were compared with 50 matched controls. Left ventricular systolic and diastolic function and flow-mediated dilatation were compared before and 12 months after treatment.
Results:
At baseline, both dipeptidyl peptidase-4 inhibitor and control groups had elevated HbA1c and comparable subclinical left ventricular dysfunction (left ventricular global longitudinal strain: −15.4% vs −15.9%, p = 0.538; e′ velocities: 6 vs 6 cm/s, p = 0.151, where e′ is the peak mitral annular early diastolic tissue velocity). After 12 months, both groups had similar improvement in HbA1c. However, patients on dipeptidyl peptidase-4 inhibitors had greater improvement in systolic (ΔGLS: 3.6% vs 1.3%, p < 0.001), despite no significant differences in weight, blood pressure or lipid parameters in both groups. Diastolic (Δe′: 38% vs 17%, p = 0.001) and endothelial function improved in the dipeptidyl peptidase-4 inhibitor group but not the control group (ΔFMD: 5% vs −1%, p = 0.029).
Conclusion:
We demonstrated significant improvements in LV systolic, diastolic and endothelial function in patients treated with a dipeptidyl peptidase-4 inhibitor over 12 months. These beneficial effects may provide some reassurance regarding the cardiovascular safety of dipeptidyl peptidase-4 inhibitors.
Introduction
Type 2 diabetes mellitus (T2DM) is an important risk factor for the development of cardiovascular disease and heart failure.1,2 Diabetic heart disease, manifest as left ventricular (LV) dysfunction that cannot be ascribed to hypertension, coronary artery disease (CAD) or significant valvular disease, is well described. Subclinical LV dysfunction is widely prevalent in apparently healthy, asymptomatic patients with T2DM. 3
Incretin-based therapies, including treatment with glucagon-like peptide-1 (GLP-1) receptor agonists and dipeptidyl peptidase-4 inhibitor (DPP4i), have become widely used as a new class of anti-hyperglycaemic drugs with different mechanisms of action from those of conventional agents. Multiple potentially beneficial effects have been demonstrated in patients with T2DM. These include reduction of cardiovascular risk, 4 blood pressure 5 and cholesterol lowering, 6 protective effects on endothelial function, 7 improvements in LV contractile performance and reduction in ischaemic/reperfusion injury in the setting of myocardial infarction in animals 8 and humans, 9 as well as anti-inflammatory 10 and anti-fibrotic effects. 11 A recent study by Nogueira et al. 12 demonstrated improvements in LV diastolic function in patients with T2DM randomized to sitagliptin versus insulin as add-on therapy to metformin and glyburide. 12 DPP4i demonstrated beneficial effects on LV remodelling in preclinical and early clinical studies, and may delay the progression to symptomatic heart failure. 13 However, several large trials of DPP4i designed to evaluate cardiovascular outcomes in patients with T2DM and cardiovascular diseases have raised concerns regarding increased hospitalization for heart failure.14–16
Echocardiographic 2D speckle tracking strain imaging allows a very sensitive, angle-independent and site-specific assessment of LV systolic function. 17 Endothelium-dependent flow-mediated dilatation (FMD) of the brachial artery using high-resolution ultrasound is a reliable non-invasive estimate of endothelial function in the coronary and systemic circulations. 18
Little is known about the effects of DPP4i on myocardial and endothelial function in patients with T2DM without CAD. This observational pilot study examined whether DPP4i, compared to non-incretin-based anti-hyperglycaemic therapies, have any differential effects on LV systolic and diastolic function, and endothelial function in patients with T2DM without significant CAD.
Materials and methods
In 2010, a cardio-diabetology service was established at our institution as a multi-disciplinary clinic where patients with poorly controlled T2DM were managed by an endocrinologist and a cardiologist for 12 months. The patients were referred predominantly by primary care physicians. In this clinic, the patients were treated according to local guidelines in an attempt to optimize their glycaemic control, blood pressure and lipid profile, 19 and they were reviewed every 3 months. All patients had significant CAD excluded by exercise echocardiography when they first attended the clinic. Repeat echocardiography was performed 12 months later to assess for any improvement in cardiac function before they were discharged back to their primary care physician.
A total of 181 patients with T2DM were managed in this clinic over a period of 3 years. A review of our database showed that 25 were commenced on a DPP4i (19 on sitagliptin, 5 on vildagliptin and 1 on saxagliptin) for management of their T2DM during the first clinic visit, and they remained on the medication after 12 months. Fifty patients who were matched for age, gender, baseline glycated haemoglobin (HbA1c) and body mass index (BMI) but who did not receive DPP4i or GLP-1 agonists during the 12 months were selected as controls. In this study, we compared the LV systolic, diastolic and endothelial function of patients who were started on DPP4i with that of the control group at baseline as well as at 12 months with echocardiographic strain imaging and FMD of the brachial arteries. The study was approved by the Hospital Human Research Ethics Committee.
Clinical data
Anthropometric data, cardiac risk factors, duration of diabetes, medications and presence of macrovascular and microvascular complications were recorded at the first clinic visit. All patients ranked their degree of breathlessness from 1 to 5 using the Medical Research Council (MRC) dyspnoea scale. 20
Echocardiogram
Two-dimensional and Doppler echocardiography
All transthoracic echocardiograms (TTEs) were performed with Vivid E9 (GE Healthcare). All standard echo and Doppler parameters of LV systolic and diastolic function including pulse-wave tissue Doppler (TDI) were measured. Offline analysis was performed using EchoPAC BT13.
Strain imaging
Mean peak global longitudinal strain (GLS) of the left ventricle was obtained with two-dimensional (2D) speckle tracking analyses in apical 4-, 2- and 3-chamber axis views using highest possible frame rates. Analyses were performed by experienced observers blinded to the clinical history and metabolic profiles. The GLS was calculated as the average of the three mean peak longitudinal strains of the three apical views (Figure 1). All Doppler and 2D speckle tracking echocardiographic measurements were taken as averages of three representative cycles. Our inter- and intra-observer variability in measurement of LV GLS has been reported. 21
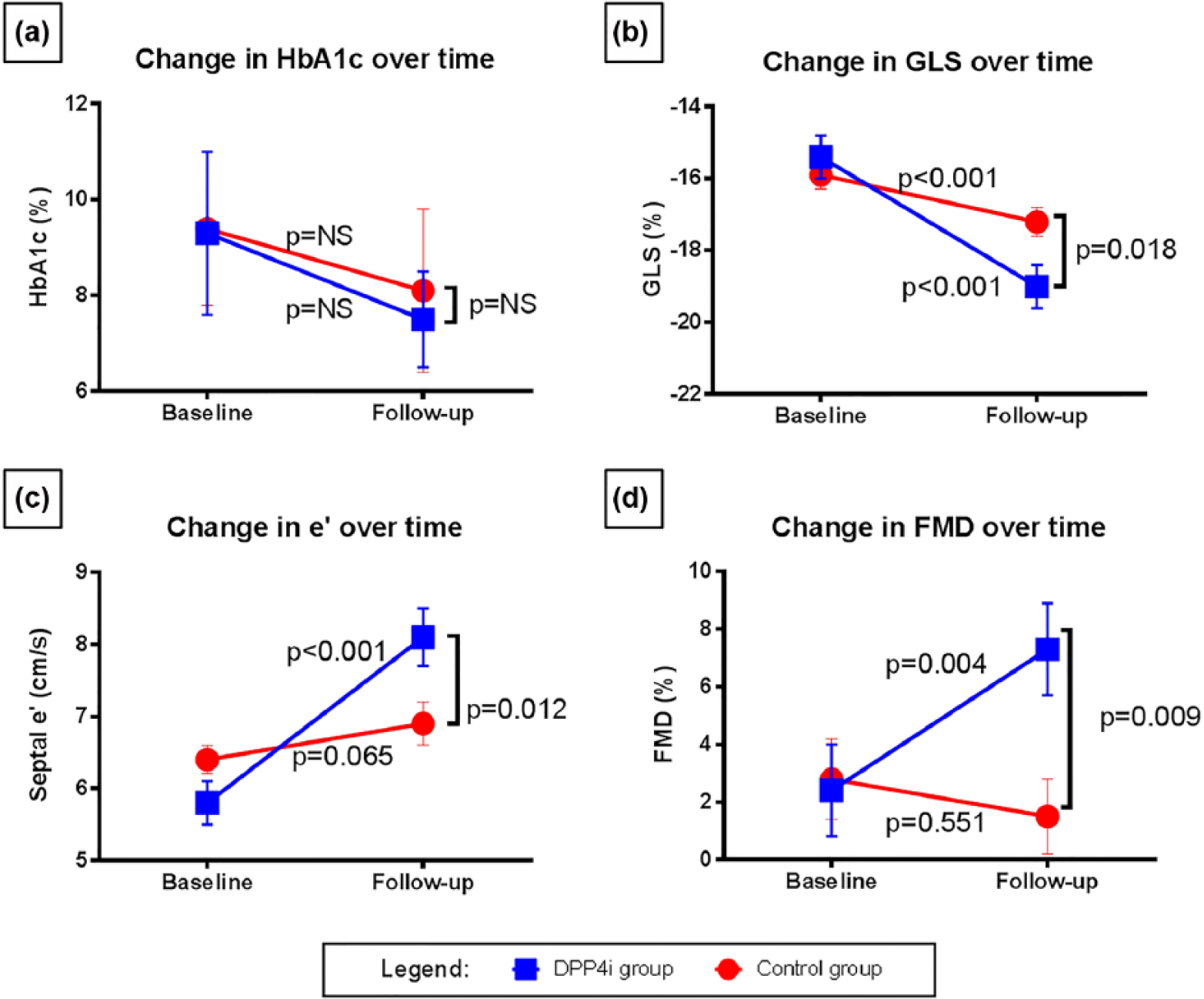
Changes over time in HbA1c: (a) left ventricular systolic, (b) diastolic function and (c) flow-mediated dilatation and (d) in DPP4i-treated group compared to controls.
Assessment of endothelial function by brachial artery reactivity
Brachial artery reactivity testing was performed at baseline and follow-up in a subset of our patients to evaluate endothelial function according to standard protocols. 22 The preparation and protocol for this has been previously described.21,23
The brachial artery diameter was measured from the intima–lumen interface of the opposing vessel walls at rest and during hyperaemia. FMD was defined as the percentage dilatation of the vessel, measured as the difference in diameters between the hyperaemic and resting phases divided by the resting diameter. Flow rate was measured as the product of cross-sectional area of the vessel assuming a circular geometry and the time velocity integral of the antegrade flow velocities. The averages of at least three cardiac cycles were used.
Statistical analysis
Results are expressed as mean ± standard deviation (SD) for continuous, normally distributed variables, median and interquartile ranges (IQR) for continuous, non-normally distributed variables and percentages for categorical variables. Baseline differences between treatment groups were analyzed using the student’s t-test for normally distributed variables, Wilcoxon test for nonparametric continuous variables and χ2 for categorical variables. Comparison between DPP4i and control groups pre- and post-treatment was achieved using a linear mixed model using Bonferroni correction for multiple comparisons. The treatment group and timing of ultrasound measurement (baseline or follow-up) were incorporated into the model as fixed variables as well as the interaction between these two variables. An unstructured covariance matrix was applied. The estimated marginal means ± standard error of the means were presented. A two-sided p-value < 0.05 was considered significant. Statistical analyses were performed using STATA v12 (STATA Corporation, Texas).
Results
Clinical profile of patients at baseline
The clinical characteristics of patients who were on DPP4i and those in the control group are shown in Table 1. The patients in the two treatment groups were well matched, except that more patients in the control group were on insulin. The patients were obese and had poor glycaemic control with a mean HbA1c above 9.3% (78 mmol/mol) and mean BMI above 32 kg/m2. Most of them suffered from hypertension and hyperlipidaemia but did not have significant macrovascular complications. None of the patients had congenital heart disease, significant valvular disease, CAD, severe hypertension (>200/120 mmHg at rest) or left bundle branch block.
Baseline clinical and metabolic characteristics of patients.
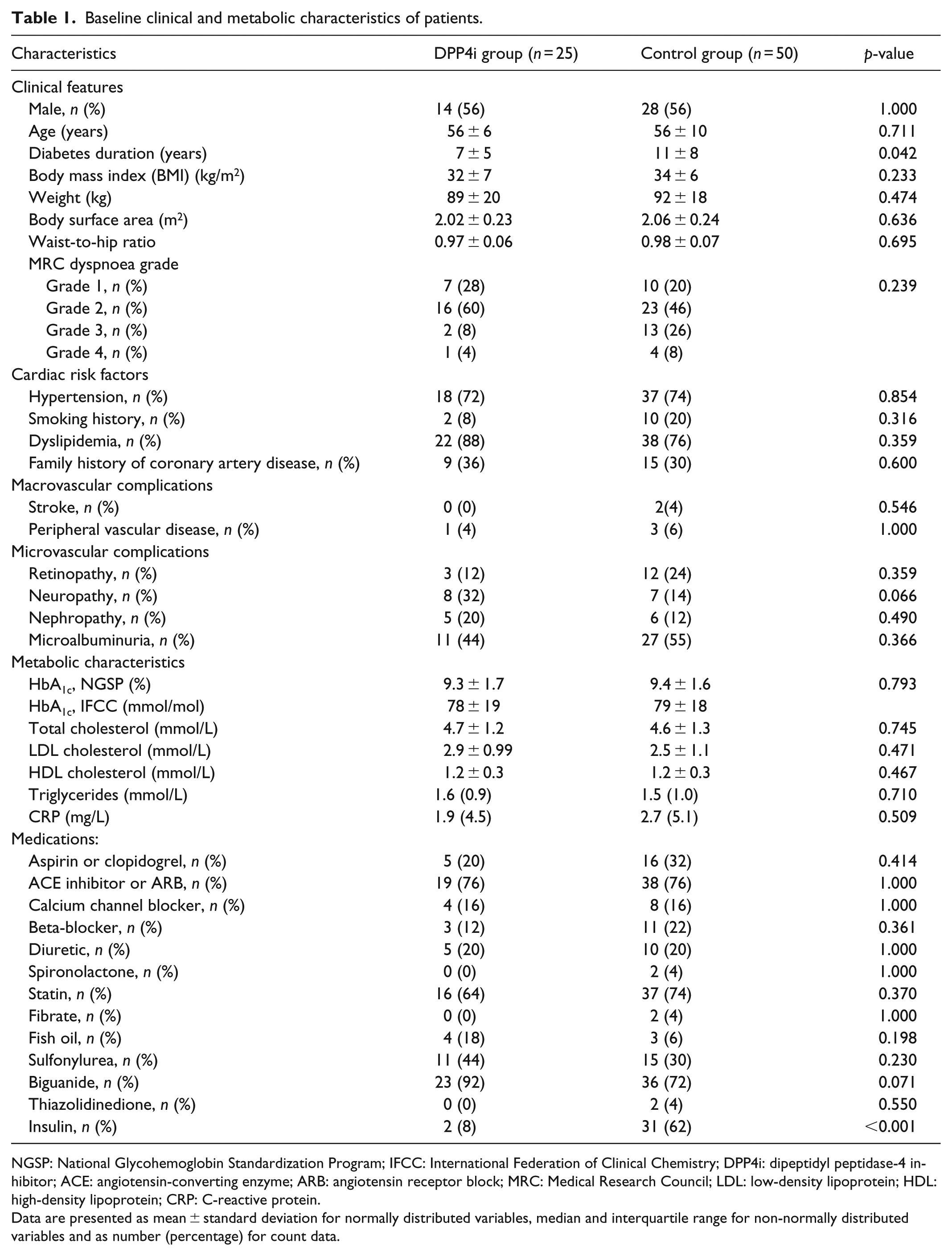
NGSP: National Glycohemoglobin Standardization Program; IFCC: International Federation of Clinical Chemistry; DPP4i: dipeptidyl peptidase-4 inhibitor; ACE: angiotensin-converting enzyme; ARB: angiotensin receptor block; MRC: Medical Research Council; LDL: low-density lipoprotein; HDL: high-density lipoprotein; CRP: C-reactive protein.
Data are presented as mean ± standard deviation for normally distributed variables, median and interquartile range for non-normally distributed variables and as number (percentage) for count data.
Echocardiography and FMD at baseline
Patients in the DPP4i group and the control group were comparable in all echocardiographic variables as well as FMD at baseline (Table 2).
Change in ultrasound characteristics of patients after 1-year treatment in DPP4i and control groups, correcting for corresponding baseline variable.
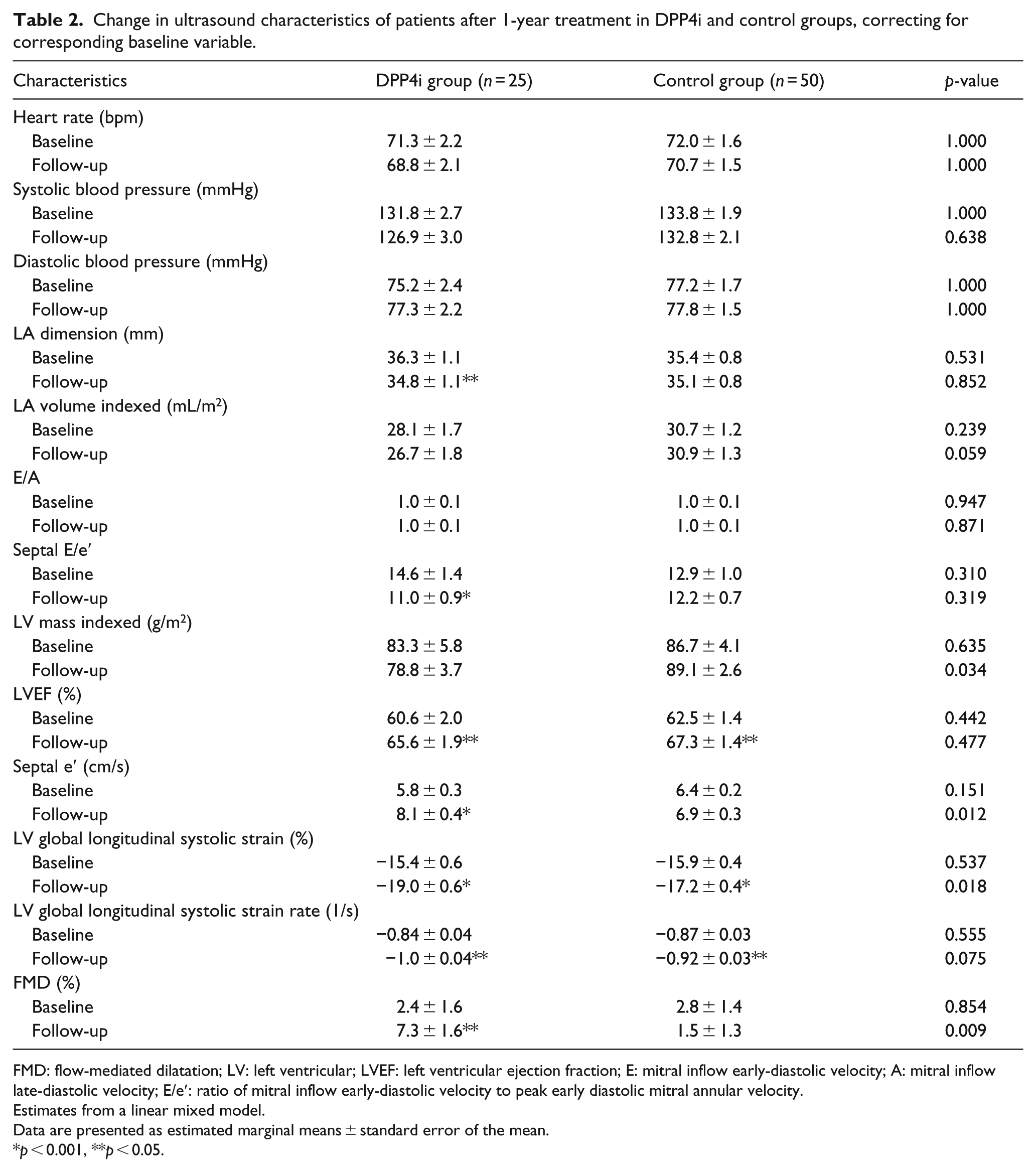
FMD: flow-mediated dilatation; LV: left ventricular; LVEF: left ventricular ejection fraction; E: mitral inflow early-diastolic velocity; A: mitral inflow late-diastolic velocity; E/e′: ratio of mitral inflow early-diastolic velocity to peak early diastolic mitral annular velocity.
Estimates from a linear mixed model.
Data are presented as estimated marginal means ± standard error of the mean.
p < 0.001, **p < 0.05.
At 12 months follow-up
Patients in both groups had better glycaemic control compared to that at baseline, but there was no difference in the degree of reduction in HbA1c between the two groups (1.8% vs 1.3%, p = 0.260). There was no significant change in their weight at the end of study (−0.79 kg in DPP4i group vs 1.3 kg in controls, p = 0.189). The patients’ lipid profile (total cholesterol −0.63 mmol/L vs −0.5 mmol/L, p = 0.691; low-density lipoprotein −0.1 mmol/L vs −0.5 mmol/L, p = 0.342; triglycerides −0.4 mmol/L vs 0 mmol/L, p = 0.241), systolic blood pressure (−4 mmHg vs −1 mmHg, p = 0.443) and C-reactive protein (−0.1 ml/L vs −0.2 mg/L, p = 0.964; in DPP4i and control groups, respectively) did not differ from baseline in either group. The use of angiotensin-converting enzyme inhibitors, angiotensin 2 receptor antagonists and beta-blockers at baseline and at follow-up did not differ between the two groups. None of the patients in our cohort suffered any cardiovascular event during the 12-month follow-up period.
There were improvements in LV GLS and LV ejection fraction in both groups, and this GLS improvement was significantly greater among patients in the DPP4i group (Table 2, Figure 1). The use of DPP4i remained an independent determinant of GLS improvement when controlling for the duration of T2DM in the linear mixed model (β = −1.73, p = 0.019). Furthermore, LV mass was lower in the DPP4i group.
As for diastolic function, there was a significant drop in septal E/e′ and an increase in septal e′ in patients in the DPP4i group but not in the control group after 12 months. Furthermore, 40% of patients in the DPP4i group compared with 18% of controls had normal diastolic function at follow-up.
FMD improved significantly in patients in DPP4i group between baseline and 12-month follow-up (Figure 1). However, there was no change in FMD among patients in the control group at follow-up compared to baseline.
Discussion
In this case-control study, we demonstrated that patients with T2DM who were commenced on DPP4i had better LV systolic and diastolic function at 12 months, as indicated by greater improvement in LV GLS, septal E/e′ and septal e′ on echocardiography, compared to patients who were not on DPP4i or GLP-1 agonists. Furthermore, patients on DPP4i had better endothelial function as shown by higher FMD at 12 months. This was despite the fact that patients in both groups had comparable age, BMI, blood pressure, lipid profiles and glycaemic control at baseline as well as at follow-up.
In recent years, DPP4i have been widely used as an anti-hyperglycaemic agent in the management of T2DM. Its glucose-lowering effect is mediated through inhibition of dipeptidyl peptidase-4 (DPP4), thereby increasing the availability of incretins including GLP-1. While GLP-1 has direct signalling effects on the cardiovascular system, DPP4 has a multitude of non-incretin substrates, and the activity of some of these substrates, such as bradykinin, SDF-1α and IP-10, may also impact on vascular function. 24 Animal studies showed that DPP4i improved LV function and reduced ischaemic reperfusion injury in the setting of acute coronary syndrome. 8 In an obese diabetic mice model, inhibition of DPP4 decreased LV stiffness and improved global LV performance. 25
However, concerns regarding the safety of DPP4i were raised following the Saxagliptin and Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus (SAVOR-TIMI) study, which found that the rate of hospitalization for heart failure was greater in patients receiving saxagliptin. 14 A meta-analysis of nine data sets also suggested an increase in heart failure among patients on DPP4i. 26 On the other hand, the recently published Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS) showed that hospitalization for heart failure was not higher in subjects on sitagliptin after a median follow-up of 3 years. 27 Subjects recruited in TECOS had high background cardiovascular risk, with three quarters of the cohort having previous cardiovascular events, and treatment with sitagliptin did not increase the development of any other cardiovascular endpoints.
To date, there have been few clinical studies that evaluated the effects of DPP4i on LV function by echocardiography. Nogueira et al. 12 recently demonstrated improvements in LV diastolic function in patients with T2DM randomized to sitagliptin versus insulin as add-on therapy to metformin and glyburide. However, although the authors reported no changes in LV systolic function, details of how LV systolic function was assessed were not discussed. Ussher and Drucker 13 also demonstrated beneficial effects of DPP4i on LV remodelling in preclinical and early clinical studies, and suggested that DPP4i may delay the progression to symptomatic heart failure.
Despite the fact that our patient group is distinct from those in the TECOS, 27 SAVOR-TIMI 14 and the EXamination of cArdiovascular outcoMes with alogliptIN versus standard of carE in patients with T2DM and acute coronary syndrome (EXAMINE) studies 15 by way of the absence of significant CAD, they were at significantly increased risk of heart failure and diabetic cardiomyopathy. 28 Our study is novel in demonstrating improvements in LV systolic as well as diastolic function in patients on DPP4i using advanced echocardiographic imaging techniques. This effect on LV function went beyond the impact of better glycaemic control, as the degree of change in GLS, septal E/e′ and septal e′ was greater than that of patients in the control group with similar improvement in HbA1c. Although there was no difference in LV ejection fraction, strain imaging is superior to ejection fraction in the detection of early diabetic heart disease. 17
Micro-angiography and vascular endothelial dysfunction have been identified as possible mechanisms for the pathogenesis of diabetic cardiomyopathy. 29 DPP4i affect endothelial function and have been shown to be associated with an increase in biological activity of nitric oxide. Mason et al. 30 demonstrated that saxagliptin improved endothelium-dependent vasodilatation of renal arteries, re-normalized renal blood flow and reduced systolic blood pressure in rats. In this study, we assessed endothelial function in patients who were commenced on DPP4i using FMD. The finding that FMD was higher in patients on DPP4i could provide a mechanism to explain how this class of medication may improve cardiac function. Our results are similar to another clinical study where sitagliptin significantly improved endothelial function as assessed by reactive hyperaemia peripheral arterial tonometry index in patients with CAD and uncontrolled T2DM. 7
There were some limitations in this study. Although we tried to match the clinical characteristics of patients on DPP4i with those in control group, the decision to add DPP4i as part of anti-hyperglycaemic therapy in the clinic was made by clinicians based on patient factors, and thus subjected to various biases. Nevertheless, even if the two groups were not completely equal with regards to diabetes duration and therapy, we demonstrated that subjects taking DPP4i had improvement, rather than worsening of cardiac function after 12 months. Because this was a small pilot study, it was not feasible to perform sub-analyses on the contributions of other factors such as anti-hypertensive medications, tightening of glycaemic control and changes in weight on LV function. Regarding the choice of DPP4i, the great majority of the 25 patients were on sitagliptin. It is possible that there are differences between the various DPP4i in their effect on LV function. We also could not extrapolate these effects to GLP-1 agonists, and separate echocardiographic studies would need to be performed for this class of medication. Finally, we did not assess B-type natriuretic peptide (BNP) in our patients, and that could be interesting as heart failure occurred almost exclusively in subjects with high baseline BNP levels in the SAVOR-TIMI study.
Conclusion
This small pilot study demonstrated improvement in LV systolic and diastolic function following 12 months’ treatment with DPP4i. Following reports of increased heart failure admissions as shown in the SAVOR-TIMI study, our findings provide some reassurance regarding the safety and possible beneficial effects of DPP4i, and are in line with the results of TECOS. A larger, randomized study that assesses cardiac function prospectively with advanced imaging modalities is being planned to validate these effects of DPP4i on the diabetic myocardium.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.