
Abstract
Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with LINAgliptin (MARLINA–T2D™), a multicentre, multinational, randomized, double-blind, placebo-controlled, parallel-group, phase 3b clinical trial, aims to further define the potential renal effects of dipeptidyl peptidase-4 inhibition beyond glycaemic control. A total of 350 eligible individuals with inadequately controlled type 2 diabetes and evidence of renal disease are planned to be randomized in a 1:1 ratio to receive either linagliptin 5 mg or placebo in addition to their stable glucose-lowering background therapy for 24 weeks. Two predefined main endpoints will be tested in a hierarchical manner: (1) change from baseline in glycated haemoglobin and (2) time-weighted average of percentage change from baseline in urinary albumin-to-creatinine ratio. Both endpoints are sufficiently powered to test for superiority versus placebo after 24 weeks with α = 0.05. MARLINA–T2D™ is the first of its class to prospectively explore both the glucose- and albuminuria-lowering potential of a dipeptidyl peptidase-4 inhibitor in patients with type 2 diabetes and evidence of renal disease.
Keywords
Introduction
Chronic kidney disease in type 2 diabetes
Chronic kidney disease (CKD) is a serious and common condition in patients with type 2 diabetes, occurring in approximately 30%–45% of patients. 1 Intensified glycaemic control and inhibition of the renin–angiotensin–aldosterone system (RAAS) are currently considered standard treatments for patients with type 2 diabetes and CKD.1,2 However, despite optimized glucose control and RAAS blockade, patients with type 2 diabetes and residual albuminuria are known to remain at an increased risk of cardio-renal morbidity and mortality. 3
Dipeptidyl peptidase-4 inhibition in patients with type 2 diabetes and CKD
Dipeptidyl peptidase-4 (DPP-4) inhibitors lower serum glucose levels mainly by a glucose-dependent mechanism that prevents the degradation of glucagon-like peptide-1 (GLP-1). DPP-4 inhibitors are known to have a very low risk for hypoglycaemia and are generally associated with a favourable safety and tolerability profile. 4 Placebo-controlled studies with linagliptin, vildagliptin, saxagliptin and sitagliptin, as well as a recent pooled analysis with linagliptin, have underscored the likely positive benefit-risk profile of DPP-4 inhibitors in patients with type 2 diabetes and mild-to-severe renal impairment.5–9
Potential renal pleiotropic effects of DPP-4 inhibitors
DPP-4 has a widespread organ distribution, and its expression level differs greatly among tissues, with the highest levels found in the kidneys. 10 In the healthy human kidney, DPP-4 is predominantly present in the apical brush border surface of kidney proximal tubular cells, 11 but only a very small amount of immunoreactivity was observed in glomerular podocytes. 12 However, under pathologic conditions such as diabetes, DPP-4 is expressed in human glomeruli.13,14 DPP-4 upregulation was also observed in human glomerular endothelial cells exposed to high glucose 15 or in renal tubular cells in high-fat fed and streptozotocin-treated rats. 16
Renal effects of DPP-4 inhibition: experimental evidence
Sitagliptin and vildagliptin reduced kidney injury and albuminuria in rat models of type 1 and type 2 diabetes.17,18 Similar effects of linagliptin given either alone or in combination with RAAS blockade therapy were also observed in animal models of diabetic nephropathy.13,19,20 Different mechanisms have been proposed to explain the potential renal effects of linagliptin. First, linagliptin ameliorates kidney fibrosis via the inhibition of transforming growth factor-beta 2 (TGF-β2)-induced endothelial-to-mesenchymal transition and the restoration of renal microRNA-29s expression levels. 21 Similar results were also obtained in a mouse model of type 2 diabetes and obesity where linagliptin inhibited myofibroblast transformation and reduced podocyte injury. 13 Second, linagliptin involves alleviation of renal oxidative stress and inflammation by blocking advanced glycation end product (AGE) signalling pathways.19,22,23 According to in vivo data, linagliptin significantly reduced the interaction of AGE with its receptor, RAGE, 24 leading to decreased nicotinamide adenine dinucleotide phosphate (NADPH) oxidase–dependent reactive oxygen species generation. 20 Furthermore, linagliptin was shown to reduce oxidative stress and inflammation by blocking the pathological crosstalk between the AGE–RAGE axis and DPP-4 via an interaction with the mannose-6-phosphate/insulin-like growth factor II receptor (M6P/IGF-IIR). 22 An overview of the GLP-1 independent mechanisms of DPP-4 inhibition in the diabetic kidney is summarized in Figure 1.
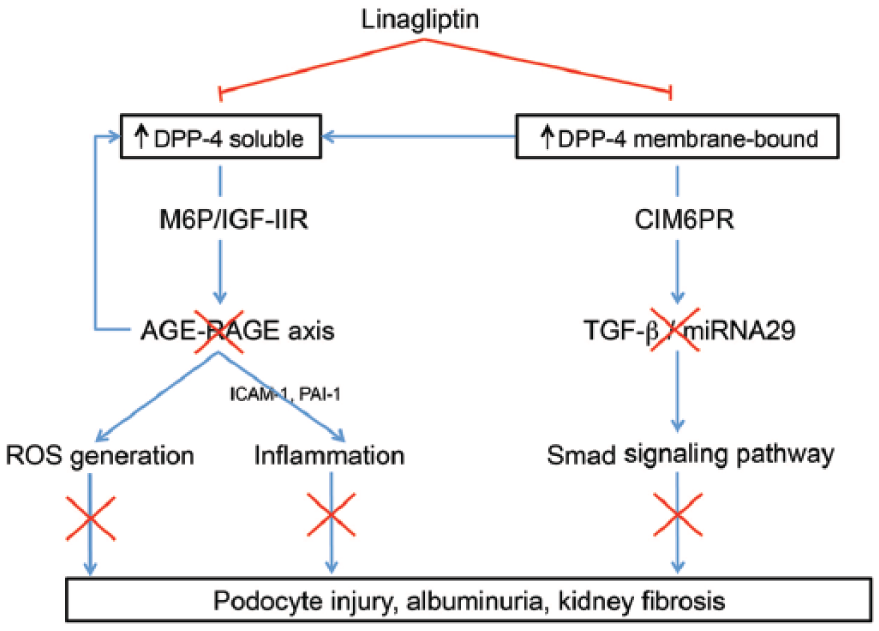
Potential GLP-1 independent mechanisms of DPP-4 inhibition with linagliptin in the diabetic kidney. Recent studies using endothelial cell or rodent models of diabetic nephropathy demonstrated that both soluble and membrane-bound forms of DPP-4 are upregulated in the diabetic milieu. Linagliptin may alleviate microvascular inflammation and filtration barrier injury by interrupting the protein–protein interaction between the circulating soluble form of DPP-4 and the mannose-6-phosphate/insulin-like growth factor II receptor (M6P/IGF-IIR) (left side of panel). In addition, linagliptin may reduce kidney fibrosis by interrupting the protein–protein interaction between the renal membrane-bound form of DPP-4 and the cation-independent mannose 6-phosphate receptor (CIM6PR) and thereby reducing the activation of the transforming growth factor-β (TGF-β)/Smad signalling pathway (right side of panel).
Renal effects of DPP-4 inhibition: clinical evidence
To date, only a few exploratory clinical studies have specifically examined the renal effects of DPP-4 inhibitors in patients with type 2 diabetes.25–27 However, this evidence has emerged from smaller, non-randomized, uncontrolled studies. A recent pooled analysis of four randomized, double-blind, placebo-controlled clinical trials has demonstrated that linagliptin administrated on top of RAAS inhibition significantly reduced albuminuria by 28% [95% confidence interval (CI) −47 to −2; p < 0.05] after 24 weeks of treatment. 28 In line with these findings, the risk of either development or progression of microalbuminuria was significantly reduced with saxagliptin at a median follow-up period of 2.1 years in the long-term SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus – Thrombolysis in Myocardial Infarction 53) phase 4 clinical trial. 29
In summary, experimental and clinical studies have supported the novel concept that DPP-4 inhibitors may have pleiotropic renal effects beyond their glucose-lowering properties. Thus, prospective, randomized and placebo-controlled clinical trials with appropriate design and adequate statistical power are now needed to further define the potential renal benefit afforded by DPP-4 inhibitors.
Methods
The MARLINA–T2D™ (Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with LINAgliptin) trial has been designed to specifically establish whether adding linagliptin to current glucose-lowering background therapy will result in superior reduction in both HbA1c and urinary albumin-to-creatinine ratio (UACR) as compared to placebo after 24 weeks of treatment in patients with insufficiently controlled type 2 diabetes and renal dysfunction.
Study population
Main inclusion and exclusion criteria are listed in Table 1. MARLINA–T2D aims to recruit patients with inadequately controlled type 2 diabetes and renal dysfunction. The latter is defined as residual albuminuria despite stable single-agent RAAS blockade, the recommended standard treatment for diabetic nephropathy. 2 In brief, eligible individuals with type 2 diabetes (aged 18–80 years at screening) must have HbA1c levels between 6.5% and 10.0% at screening, a body mass index ⩽40 kg/m2 at screening and are either treatment-naïve or concomitantly treated with one or two oral glucose-lowering therapies or basal insulin, either alone or in combination with a maximum of two oral glucose-lowering therapies. Importantly, study participants are required to fulfil the following criteria: UACR levels between 30 and 3000 mg/g Cr (further details are provided in Table 1) and estimated glomerular filtration rate (eGFR) ⩾30 mL/min/1.73 m2 based on the Modification of Diet in Renal Disease (MDRD) formula at screening, and ongoing pharmacotherapy with RAAS blockade, either an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin receptor blocker (ARB), at a stable dose for 10 weeks prior to informed consent.
Key inclusion and exclusion criteria of MARLINA–T2D™.
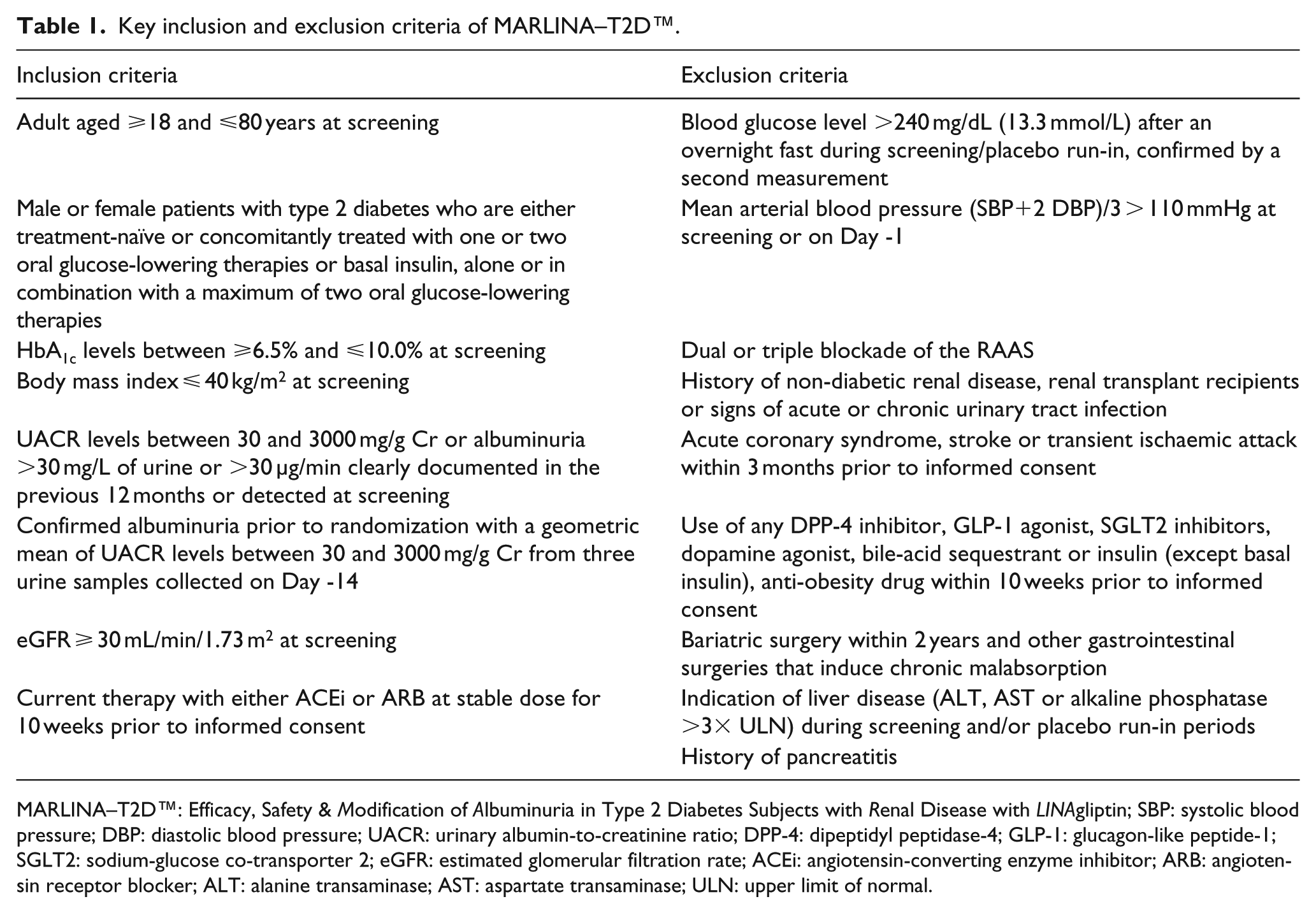
MARLINA–T2D™: Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with LINAgliptin; SBP: systolic blood pressure; DBP: diastolic blood pressure; UACR: urinary albumin-to-creatinine ratio; DPP-4: dipeptidyl peptidase-4; GLP-1: glucagon-like peptide-1; SGLT2: sodium-glucose co-transporter 2; eGFR: estimated glomerular filtration rate; ACEi: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; ALT: alanine transaminase; AST: aspartate transaminase; ULN: upper limit of normal.
Study design
MARLINA–T2D is a 24-week, multicentre, multinational, randomized, double-blind, placebo-controlled, parallel-group, phase 3b clinical trial. The overall study design is detailed in Figure 2. In brief, eligible participants undergo a 2-week, open-label, placebo run-in period to ensure compliance with study procedures and appropriate intake of study drug. Subjects who successfully complete this period and who still meet the inclusion/exclusion criteria are randomized in a 1:1 ratio to receive either linagliptin 5 mg or placebo in addition to their background therapy for 24 weeks. Randomization is stratified by HbA1c level (<8.5% vs ⩾8.5%) at screening and UACR level (<300 mg/g Cr vs ⩾300 mg/g Cr) at the start of the run-in period (Day -14).
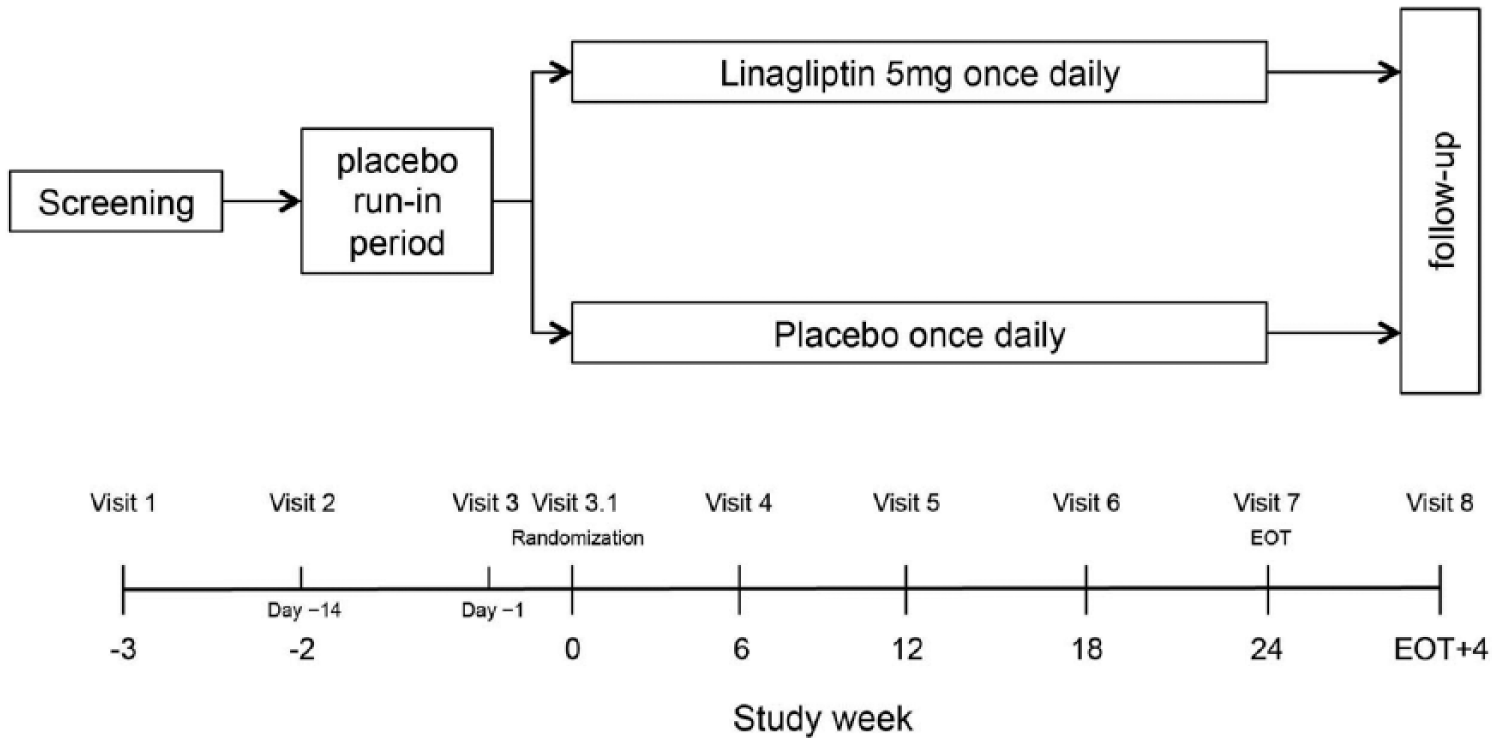
MARLINA–T2D™: flow chart of study design.
After completion of the 24-week randomized period, MARLINA–T2D will further assess changes in albuminuria after a 4-week follow-up period of study drug withdrawal in both arms. The aim of this off-treatment period is to explore whether the potential albuminuria-lowering effect of linagliptin is maintained after drug withdrawal. Previous studies have shown that short-term treatment effects related to haemodynamic mechanisms are mitigated after cessation of treatment. 30 However, linagliptin may improve renal function by structural rather than by haemodynamic effects in view of its previously reported antifibrotic and anti-inflammatory effects.19,20,24 The 4-week follow-up period of MARLINA–T2D will help to address this question.
MARLINA–T2D was initiated in March 2013, and approximately 80 centres in 12 countries (Canada, Denmark, Finland, France, Germany, Japan, Philippines, South Korea, Spain, Taiwan, the United States and Vietnam) are foreseen to recruit individuals for this trial. The study protocol has been approved by the Institutional Review Board/Ethics Review Committee affiliated with each centre and by appropriate authorities according to national and international regulations. The study is being conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants will provide written informed consent before participation. MARLINA–T2D has been registered on Clinicaltrials.gov, NCT01792518.
Endpoints
The primary glycaemic efficacy endpoint is the change in HbA1c from baseline to Week 24. The key secondary renal efficacy endpoint is the time-weighted average of percentage change from baseline UACR during the course of 24-week treatment. Predefined primary, key secondary and other efficacy endpoints are listed in Table 2.
Statistical approach of predefined efficacy endpoints in MARLINA–T2D™.
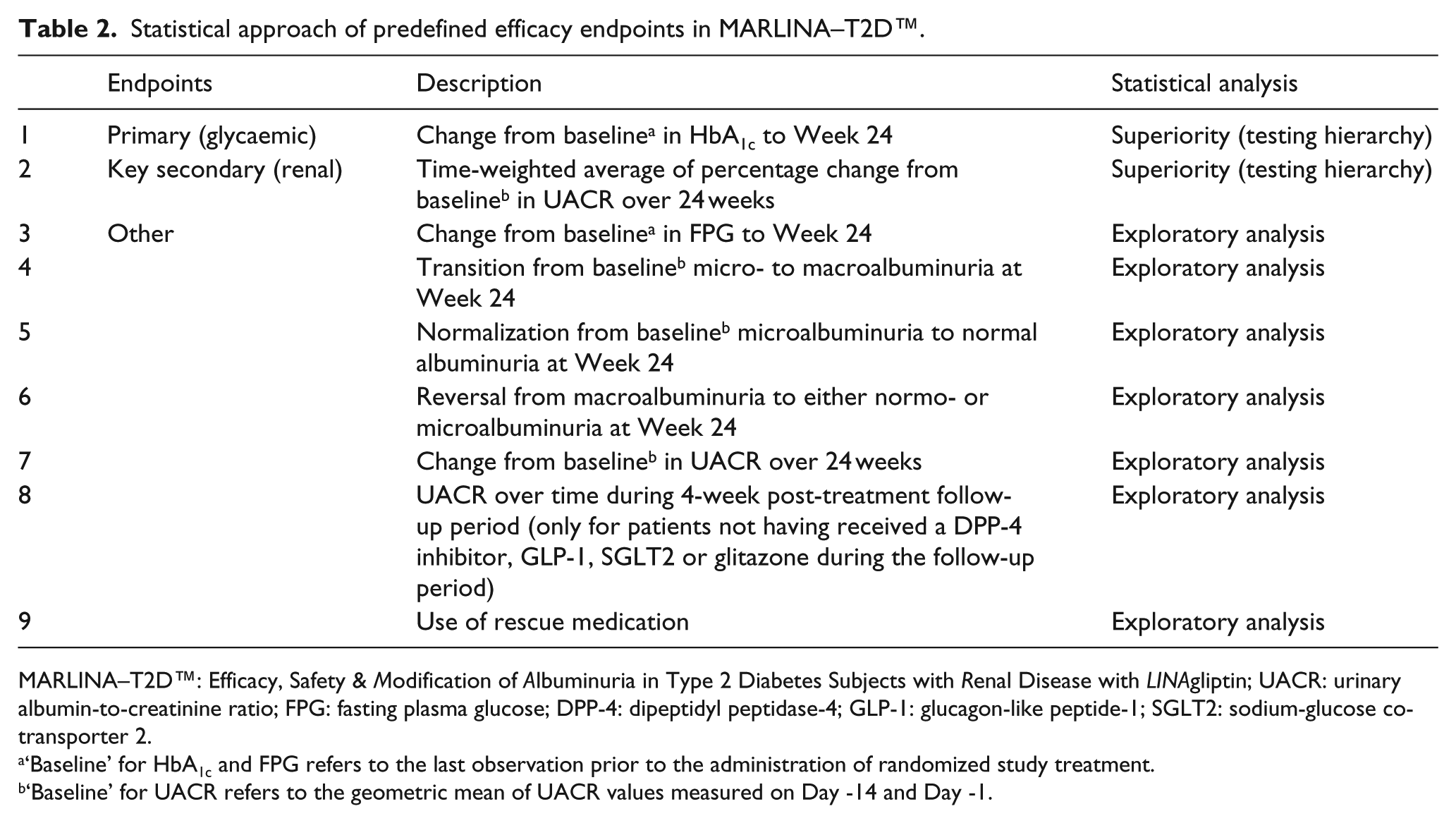
MARLINA–T2D™: Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with LINAgliptin; UACR: urinary albumin-to-creatinine ratio; FPG: fasting plasma glucose; DPP-4: dipeptidyl peptidase-4; GLP-1: glucagon-like peptide-1; SGLT2: sodium-glucose co-transporter 2.
‘Baseline’ for HbA1c and FPG refers to the last observation prior to the administration of randomized study treatment.
‘Baseline’ for UACR refers to the geometric mean of UACR values measured on Day -14 and Day -1.
Safety endpoints include incidence and intensity of adverse events; withdrawals because of adverse events; hypoglycaemia; and changes in renal function, vital signs and laboratory variables. On the basis of clinical experience with the DPP-4 inhibitor class, adverse events of special interest include hypersensitivity reactions (angio-oedema, angio-oedema-like event, anaphylaxis), renal events (kidney failure, two times or greater increase in serum Cr), increases in hepatic enzymes [alanine transaminase (ALT), aspartate transaminase (AST) or alkaline phosphatase above more than three times the upper limit of normal (ULN)], severe cutaneous adverse reactions and pancreatitis.
Study assessments
Key biochemical and clinical parameters assessed over the course of the study are listed in Table 3. Assessments of HbA1c, UACR and comprehensive safety laboratory parameters [including renal tubular biomarkers: kidney injury molecule-1 (KIM-1), neutrophil gelatinase-associated lipocalin (NGAL) and liver fatty acid binding protein (LFABP)] will be performed at a central laboratory (Quintiles Laboratories). Albuminuria will be determined by the geometric mean UACR value from three urine samples taken on 3 consecutive days at each visit (first void morning spot urine samples). To capture UACR adequately, at least two out of the requested three samples have to be available at each time point. Glomerular filtration rate will be estimated using either the MDRD or Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. In addition, estimated Cr clearance will be determined using the Cockcroft–Gault formula. In order to adequately capture potential haemodynamic treatment effects, a 24-h ambulatory blood pressure measurement (ABPM) will be conducted before first study drug intake (Day -1) and at the last day of active study drug treatment (Week 24). Additional predefined ancillary studies of MARLINA–T2D will explore the impact of linagliptin on a broad panel of circulating and urinary biomarkers. Moreover, urinary proteomic and metabolomic assessments will be conducted in partnership with academic institutions. A recent metabolomics study identified a signature for diabetic kidney disease, 31 and this study will address the role of this metabolomic signature in the MARLINA–T2D trial.
Time points of key biochemical and clinical parameters assessed over the course of MARLINA–T2D™.
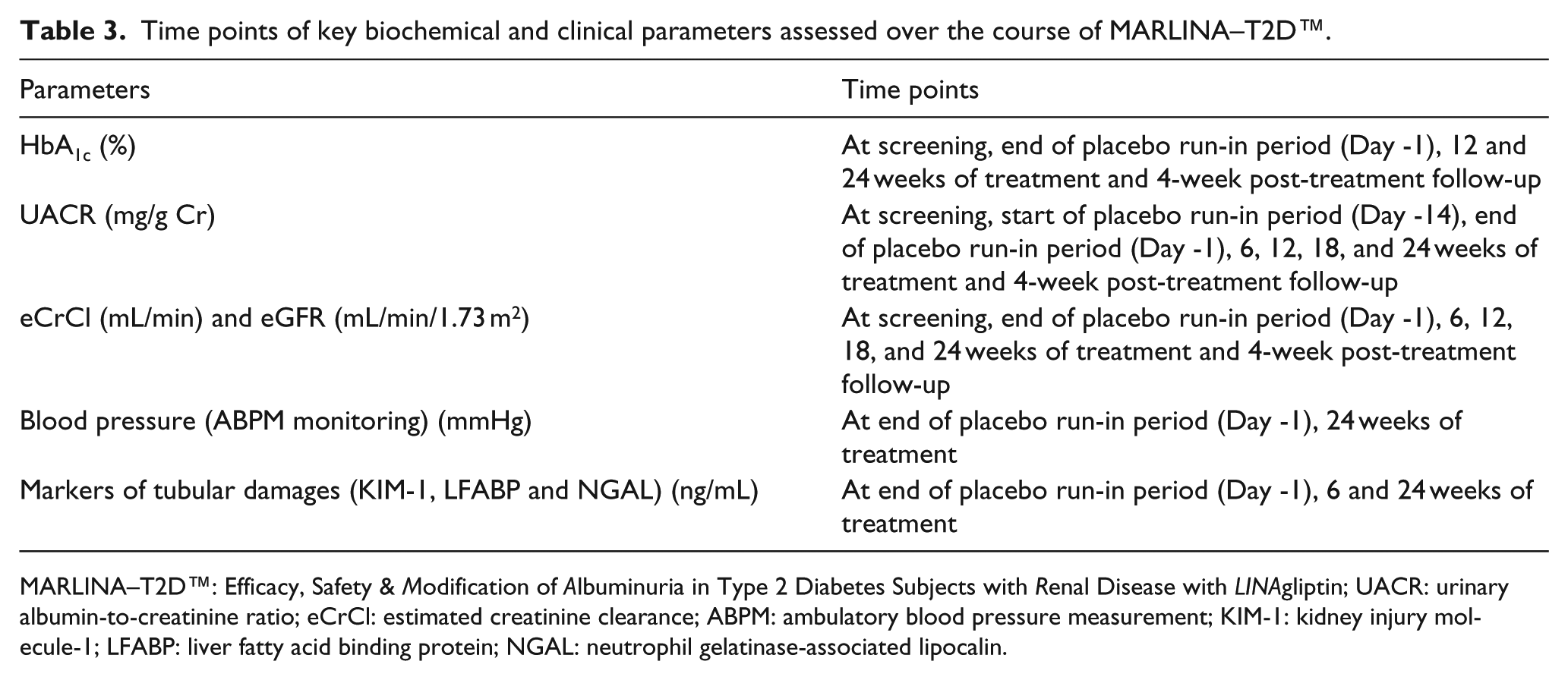
MARLINA–T2D™: Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with LINAgliptin; UACR: urinary albumin-to-creatinine ratio; eCrCl: estimated creatinine clearance; ABPM: ambulatory blood pressure measurement; KIM-1: kidney injury molecule-1; LFABP: liver fatty acid binding protein; NGAL: neutrophil gelatinase-associated lipocalin.
Sample size
Assuming a common standard deviation (SD) of 1.1% for the change in HbA1c from baseline for both treatment groups, a total of 166 subjects in each treatment group will be required to detect a significant difference (at α = 0.05, two-sided) between placebo and linagliptin groups with a power of more than 99%, assuming a 0.6% difference in HbA1c after 24 weeks of treatment. This sample size also ensures a power of 87% to detect a treatment ratio of 0.79 in the ratio of UACR change from baseline with a SD of 0.30 on the log10-scale. Assuming an overall dropout rate of 5%, MARLINA–T2D aims to recruit 350 individuals in a 1:1 randomization ratio for linagliptin 5 mg or placebo.
Statistical analysis plan
Primary and key secondary endpoints will be tested at the 5% significance level (two-sided) in a hierarchical manner in order to control for multiplicity (Table 2). Superiority of linagliptin over placebo for changes in HbA1c from baseline after 24 weeks of treatment will be first tested. If the null hypothesis concerning the primary glycaemic endpoint is rejected, then superiority of linagliptin over placebo for changes in UACR from baseline will be tested in a confirmatory way. Otherwise, the key secondary endpoint will be tested for exploratory purposes only. Based on previous trials with similar endpoints and because of their skewed distribution, UACR data will be log10-transformed before analysis in order to assume normality of residuals on the analysis scale.
The primary glycaemic endpoint will be analysed using a mixed-effects model for repeated measures (MMRM). The model will include treatment, visit and visit by treatment interaction as fixed classification effects, and baseline HbA1c, baseline log10 (UACR), baseline HbA1c by visit and baseline log10 (UACR) by visit as linear covariates. This analysis will be performed on the full analysis set (FAS) using observed cases (OC) (i.e. patients with available data). The FAS will consist of all randomized subjects who were treated with at least one dose of study drug and had a baseline HbA1c, a baseline UACR and at least one on-treatment HbA1c or UACR measurement. The key secondary renal endpoint will be analysed on the FAS using an analysis of covariance (ANCOVA), with treatment as a fixed classification effect and baseline HbA1c and baseline log10 (UACR) as linear covariates. An approach of last observation carried forward (LOCF) will be used to replace missing data. Sensitivity analyses of the primary and key secondary endpoints will be performed on the per-protocol set (PPS) (i.e. patients in the FAS without any important protocol violations) using the same models mentioned above. Analyses of other endpoints will be performed on the FAS in an exploratory manner. Safety data will be analysed using descriptive statistical methods. Results of MARLINA–T2D trial are expected to be reported in 2016.
Discussion
CKD is a common and complex disease with an increasing prevalence across the world. The primary unmet need to improve outcomes related to CKD in patients with type 2 diabetes is clearly evident. Therefore, well-designed trials are of paramount importance in this high-risk population. However, a recent systematic review of ClinicalTrials.gov revealed a critical underrepresentation of the numbers of clinical trials in nephrology as compared with other specialties, such as cardiology. 32 The MARLINA–T2D will contribute to further narrow the research-to-practice gap in the treatment of patients with type 2 diabetes and CKD. The study objectives of this trial combine established (glucose-lowering) and potential novel pleiotropic (albuminuria) targets of DPP-4 inhibition. The study should be considered as a proof-of-concept approach to explore the potential treatment effect of linagliptin on the renal surrogate parameter albuminuria. Conclusive evidence on the impact of altering the natural course of CKD in type 2 diabetes, however, will have to emerge from larger, long-term and adequately powered studies. Such research has to target and assess hard renal outcomes, such as progression to end-stage renal disease (ESRD), renal death or significant loss of renal function over time (historically expressed as doubling of serum Cr). Therefore, and complementary to the ongoing MARLINA–T2D study, the CARMELINA® (Cardiovascular and Renal Microvascular Outcome Study with Linagliptin; NCT01897532) trial has been recently initiated to determine whether linagliptin has the potential to improve long-term cardiovascular and/or renal outcomes. In brief, CARMELINA will enrol approximately 8300 subjects with type 2 diabetes at high-risk of cardiovascular and renal events defined by (1) albuminuria and previous macrovascular disease and/or (2) impaired renal function with and without residual albuminuria. It should be noted that participants in MARLINA–T2D are more likely to present with early stages of CKD, whereas CARMELINA aims to recruit a majority of patients at more advanced stages of CKD (often with concomitant macrovascular disease). Thus, these two trials will investigate a new treatment strategy with linagliptin aiming to not only prevent overt nephropathy but also slow progression of more advanced stages of diabetic kidney disease.
In addition to DPP-4 inhibition, further interventional and novel therapeutic strategies are currently being tested in late-stage development for patients with type 2 diabetes and CKD (Table 4). Given previous unsuccessful experiences in renal outcomes trials in type 2 diabetes, 33 embarking on renal outcomes studies in this population is still viewed as a challenging endeavour. However, it is important to consider that previous ‘failed’ studies and novel interventional strategies significantly vary in the underlying pathophysiological concepts and/or in the targeted mechanisms being examined (Table 4 and Supplementary Table 1). With the addition of novel proteomic and metabolomic strategies, it is hoped that novel markers of disease progression and treatment effects will be identified in upcoming clinical trials in patients with type 2 diabetes and CKD.
Major ongoing, phase 3, randomized, placebo-controlled clinical trials with renal outcomes in patients with type 2 diabetes and CKD.
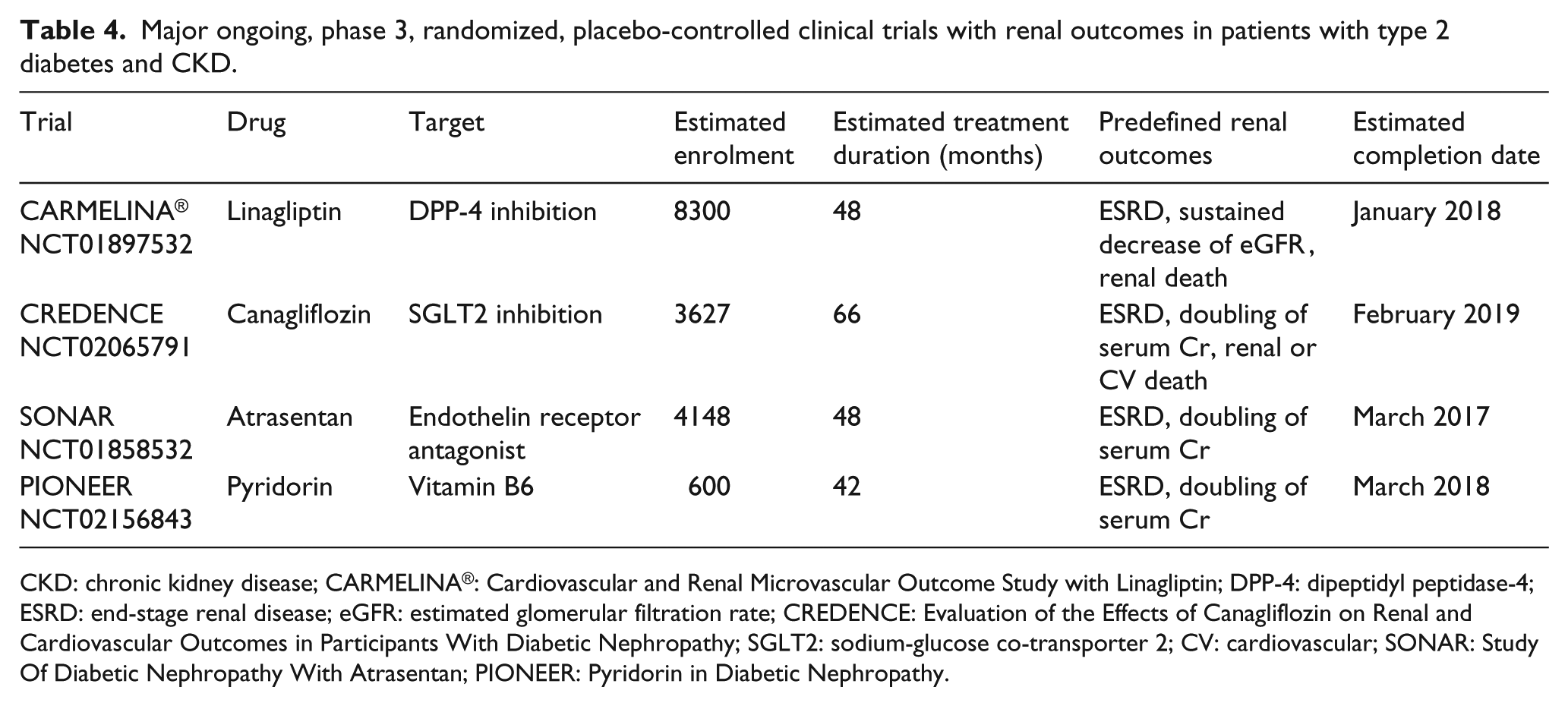
CKD: chronic kidney disease; CARMELINA®: Cardiovascular and Renal Microvascular Outcome Study with Linagliptin; DPP-4: dipeptidyl peptidase-4; ESRD: end-stage renal disease; eGFR: estimated glomerular filtration rate; CREDENCE: Evaluation of the Effects of Canagliflozin on Renal and Cardiovascular Outcomes in Participants With Diabetic Nephropathy; SGLT2: sodium-glucose co-transporter 2; CV: cardiovascular; SONAR: Study Of Diabetic Nephropathy With Atrasentan; PIONEER: Pyridorin in Diabetic Nephropathy.
In conclusion, growing clinical evidence supports the likelihood of renal effects of DPP-4 inhibitors building on a number of hypothesis-generating studies,28,34 which have reported an albuminuria-lowering effect of this drug class. In addition, a large body of experimental evidence has shown that DPP-4 inhibition may improve the progressive course of kidney disease due to these agents’ antifibrotic, anti-oxidative and anti-inflammatory properties. However, hard evidence defining the renal effects of DPP-4 inhibition is not yet available. Utilizing the DPP-4 inhibitor linagliptin, MARLINA–T2D and CARMELINA represent two randomized clinical trials, which have been adequately designed and powered to provide more robust and reliable clinical data on both surrogate and hard renal outcomes in the high-risk population of patients with type 2 diabetes and renal disease.
Footnotes
Acknowledgements
Members of the trial executive committee provided critical advice on study design and reviewed the study protocol in collaboration with clinical researchers employed by Boehringer Ingelheim. Members of the executive committee led the manuscript development, and all authors approved the final version of the present report. We thank Audrey Koïtka-Weber, PhD, for scientific consulting and medical writing services, supported financially by Boehringer Ingelheim. Trial registration: Clinicaltrials.gov NCT01792518.
Declaration of conflicting interests
P.-H.G., M.E.C., V.P., K.S., G.S., M.H. and B.H. have received fees for advisory services to Boehringer Ingelheim. V.P. has received honoraria from AbbVie, and his employer holds research contracts with AbbVie and Janssen. M.G., J.C., H.-J.W. and M.v.E. are full-time employees of Boehringer Ingelheim.
Funding
MARLINA–T2D™ is funded and conducted by Boehringer Ingelheim, the manufacturer of linagliptin.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.