
Abstract
At the time of this study, guidelines recommended a primary goal of low-density lipoprotein cholesterol level less than 100 mg/dL for all patients, an optional goal of low-density lipoprotein cholesterol less than 70 mg/dL for patients with overt cardiovascular disease and statins for patients with diabetes and overt cardiovascular disease and patients 40 years and older with diabetes and at least one risk factor for cardiovascular disease. This study examined statin use and achievement of lipid goals among 111,730 Medicare fee-for-service beneficiaries 65 years and older in 2011. Three-quarters of patients met the low-density lipoprotein cholesterol goal of less than 100 mg/dL. Patients with cardiovascular disease were more likely to meet the goal than those without, not controlling for other differences. Patients on a statin were more likely to meet the goal. There is considerable opportunity for improvement in cholesterol management in high-risk patients with diabetes mellitus.
Keywords
Introduction
To mitigate risks of cardiovascular events in patients with diabetes mellitus, guidelines in place at the time of this study recommended a primary goal of low-density lipoprotein cholesterol (LDL-C) level less than 100 mg/dL for all patients and an optional goal of LDL-C less than 70 mg/dL for patients with overt cardiovascular disease.1,2 These guidelines further recommended statins for patients with diabetes and overt cardiovascular disease and patients 40 years and older with diabetes and at least one risk factor for cardiovascular disease. 2 We investigated statin use and achievement of lipid goals among Medicare fee-for-service beneficiaries in 2011 to identify gaps in adherence to treatment guidelines and opportunities for improvement. Although the 2013 American College of Cardiology (ACC)/American Heart Association (AHA) cholesterol guidelines effectively reversed course and removed LDL-C targets from cholesterol management, we believe the clinical community would value more information about the utility of LDL-C targets and how frequently these targets were achieved, especially because other professional societies in Canada and Europe continue to recommend LDL-C targets.
Methods
We obtained Medicare fee-for-service standard analytic files from the Centers for Medicare & Medicaid Services and a supplemental file containing outpatient laboratory test orders and results processed by a national laboratory vendor in 10 eastern states. We identified beneficiaries who were 65 years or older, had type 1 or type 2 diabetes mellitus as of 31 December 2010 and were living in one of the 10 states on 31 December 2011. We linked the laboratory and Medicare data using each patient’s Medicare health insurance identifier, Social Security number, date of birth and sex. 3 To ascertain medical history and medication exposure, we required continuous enrolment in Medicare Parts A and B from 2009 through 2011 and Medicare Part D from 1 October 2010 through 31 December 2011. We restricted the population to patients with at least one outpatient lipid panel test result in the laboratory file, thereby excluding patients who were not tested or whose test was processed by another laboratory vendor or hospital-based laboratory. The institutional review board of the Duke University Health System approved this study.
We identified history of myocardial infarction, diabetes, heart failure, hypertension, hyperlipidaemia, ischaemic heart disease, and stroke or transient ischaemic attack using Chronic Condition Data Warehouse indicators and peripheral artery disease using International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis codes (one or more inpatient, outpatient or carrier claim with code 440.0, 440.2x, 440.3x, 440.4, 440.9, 443.9, 444.2x, 444.8x, 445.02 or 447.1 during 2010). We defined cardiovascular disease as a history of myocardial infarction, stroke, ischaemic heart disease or peripheral artery disease.
We identified statins in the 2011 Medicare Part D drug event file by searching the generic drug name for atorvastatin, fluvastatin, lovastatin, rosuvastatin, simvastatin, pitavastatin or pravastatin. We used prescription fill dates and days’ supply to ascertain medication exposure on 1 January 2011 and on the date of each patient’s LDL-C test result (i.e. the most recent fill date plus days’ supply covers the date of interest). For statins, having coverage as of a specific date is associated with chronic use the large majority of the time. Among patients determined to be on a statin as of a specified date, approximately 95% were on a statin both 30 days before and 30 days later and over 85% of them were on a statin both 90 days before and 90 days later. We identified LDL-C test results using Logical Observation Identifiers Names and Codes 13457-7 and 18262-6. If a patient had more than one test result, we selected the result closest to the LDL-C goal. We tested for differences between patients with or without cardiovascular disease and included in or excluded from the study population using χ2 tests for categorical variables and Wilcoxon tests for continuous variables.
The eligible population included 922,318 beneficiaries; 111,730 had LDL-C results available. Most patients had a history of hypertension, hyperlipidaemia and/or cardiovascular disease (Table 1). Approximately half were on a statin, and statin use was higher among patients with cardiovascular disease. Three-quarters of patients met the LDL-C goal of less than 100 mg/dL. Patients with cardiovascular disease were more likely to meet the goal than those without, not controlling for other differences. Patients on a statin were more likely to meet the goal. The study population was younger, more likely to have hyperlipidaemia and less likely to have cardiovascular disease than patients who were excluded from the study (Supplementary Table 1). Patients who were on a statin were less likely to be Black or Hispanic and more likely to have cardiovascular disease or cardiovascular risk factors than those who were not on a statin (Supplemental Table 2).
Characteristics of the study population, use of statins and LDL cholesterol levels among eligible Medicare fee-for-service beneficiaries with laboratory results in 2011.
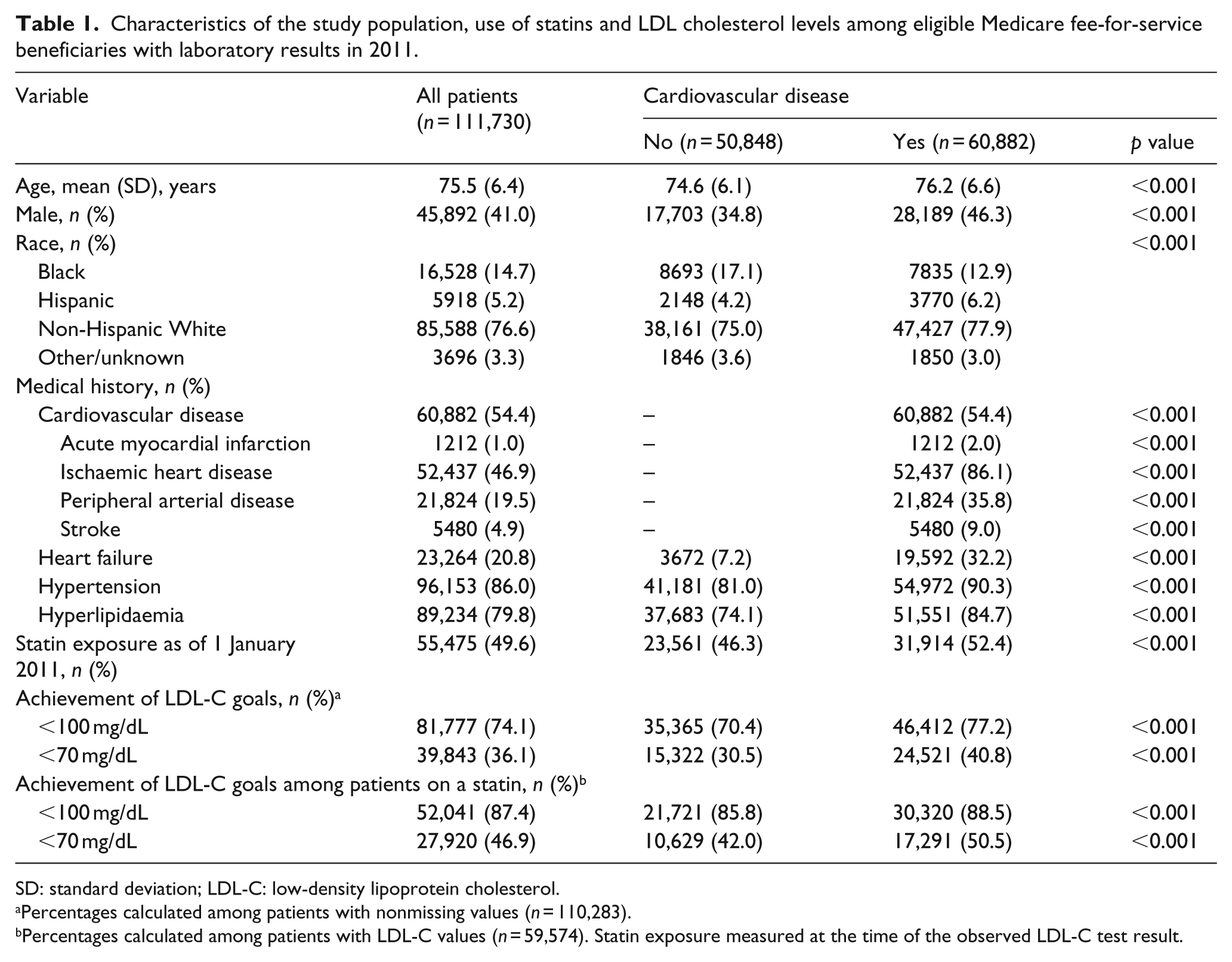
SD: standard deviation; LDL-C: low-density lipoprotein cholesterol.
Percentages calculated among patients with nonmissing values (n = 110,283).
Percentages calculated among patients with LDL-C values (n = 59,574). Statin exposure measured at the time of the observed LDL-C test result.
Comment
Only half of the study population received a statin, despite a high prevalence of cardiovascular disease and risk factors including age, hypertension and hyperlipidaemia. Lack of statin treatment may be explained either by physicians not prescribing statins or by patients not filling prescribed medications. While nearly three-quarters of the population had LDL-C less than 100 mg/dL, only 40% of patients with prevalent cardiovascular disease had LDL-C less than 70 mg/dL. These findings are similar to previous results from multinational registry data and cohort studies in Europe.4,5
Evidence is mounting that progression of atherosclerosis occurs more frequently in high-risk patients not treated with a statin and in statin-treated patients lacking adequate reduction in LDL-C.6,7 Furthermore, there is clear evidence that statins reduce cardiovascular morbidity and mortality across the cardiovascular disease risk spectrum. 8 Reasons why more patients are not treated with statins and treatment goals are not met likely include lack of physician awareness of potential benefits and patient noncompliance. While the ACC/AHA cholesterol guidelines may provide greater focus on cholesterol management for high-risk patients, they admittedly represent a ‘significant departure from current strategies’ 9 and may confuse doctors and patients and increase inertia regarding the application of clinical guidelines. 10 Furthermore, guidelines from the Canadian Cardiovascular Society and European Society of Cardiology continue to emphasize the use of LDL-C targets. Hence, there remains considerable opportunity for improvement in cholesterol management in high-risk patients with diabetes mellitus.
Footnotes
Acknowledgements
Damon M. Seils, MA, Duke University, provided editorial assistance and formatted the manuscript for submission.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Curtis reported receiving research support from Boston Scientific, Gilead, GlaxoSmithKline and Novartis. Dr Jones reported receiving research grants from the American Heart Association, AstraZeneca and Boston Scientific. Dr Maciejewski reported receiving research grants from the Agency for Healthcare Research and Quality. No other disclosures were reported. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the Department of Health and Human Services or any of its agencies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by Cooperative Agreement Number 1C1CMS331018-01-00 from the Department of Health and Human Services, Centers for Medicare & Medicaid Services, and a grant from the Robert Wood Johnson Foundation’s Health Care Financing and Organization Initiative (#70922). Dr Maciejewski was supported by a Research Career Scientist award from the Department of Veterans Affairs (RCS 10-391).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.