
Abstract
We investigated whether mitochondrial (mtDNA) haplogroups and maternal family history of diabetes mellitus were associated with vascular diabetes mellitus complications in a population-based cohort of 299 Finnish diabetes mellitus patients with disease onset in young adult age. We found that haplogroup U was more prevalent among patients with no vascular diabetes mellitus complications than among those with at least one complication (p = 0.038). Haplogroup U was also more prevalent among the patients who reported maternal family history of diabetes mellitus than among those who did not (p = 0.0013). Furthermore, haplogroup U was more prevalent among patients with maternal family history of diabetes mellitus but no vascular diabetes mellitus complications than among those with at least one vascular diabetes mellitus complication but no maternal family history of diabetes mellitus (p = 0.0003 for difference). These findings suggest that different mtDNA-related factors may influence the risk of diabetes mellitus per se and the risk of vascular diabetes mellitus complications. Further studies are, however, warranted to replicate and elaborate on these results.
Keywords
Mitochondrial DNA (mtDNA) has a ~10–17 times higher mutation rate than the nuclear DNA. 1 This rapid mutation rate leads to mtDNA sequence variants that eventually result in population-specific, recognisable patterns represented as the mtDNA haplogroups. Interestingly, mitochondrial dysfunction is closely involved in the pathophysiology of diabetes mellitus (DM), 2 and mtDNA haplogroups have been reported to modulate the risk of vascular complications in people with DM. 3 We have previously found that mtDNA haplogroup U is associated with maternal family history of DM (MFH) among patients with DM onset in young adulthood. 4 We decided to investigate whether mtDNA haplogroups and MFH are associated with the risk of vascular DM complications.
The study setting, patient identification procedure and molecular methods have been reported previously. 4 All patients in the study (N = 299; women = 159) were asked to fill out a medical history questionnaire including family history of DM among their relatives (children, siblings, parents, both maternal and paternal grandparents) in order to identify those with MFH.
The electronic medical charts of the 299 patients at Turku University Hospital (TUH) were scrutinised to detect any vascular complications associated with DM. The manifestations of DM-associated vascular disease were ischaemic heart disease with or without a history of myocardial infarctions, ischaemic stroke or transient ischaemic attack (TIA), peripheral artery occlusive disease, nephropathy and retinopathy. It was required that the vascular DM complication had been confirmed at TUH by an internist or endocrinologist or, in the case of diabetic retinopathy, by an ophthalmologist or, in the case of ischaemic stroke or TIA, by a neurologist.
Two-tailed Fisher’s exact test was used to examine the association between vascular DM complications and mtDNA haplogroups. Unpaired t-test was used to detect differences in age or disease duration between groups of patients with DM. Exact test of population differentiation, as implemented in Arlequin (version 3.5.1.2), was applied to test possible non-random distribution of haplogroup clusters between patient groups.
Patients were analysed for mtDNA haplogroups (Table 1). The prevalence of haplogroup clusters (p = 0.54) or the prevalence of reported MFH (p = 0.24) did not differ between men and women. Haplogroup U was more prevalent among the patients who reported MFH than among those who did not (p = 0.0013). Patients with complications were, not surprisingly, somewhat older than patients with no DM complications: The difference in mean age was 6.3 years (p < 0.0001 for difference). Patients with complications also had longer history of DM than those without. The difference in mean disease duration was 5.1 years (p < 0.0001 for difference).
Vascular complications, maternal family history of diabetes mellitus (MFH) and mitochondrial DNA haplogroup clusters among patients with diabetes mellitus (DM).
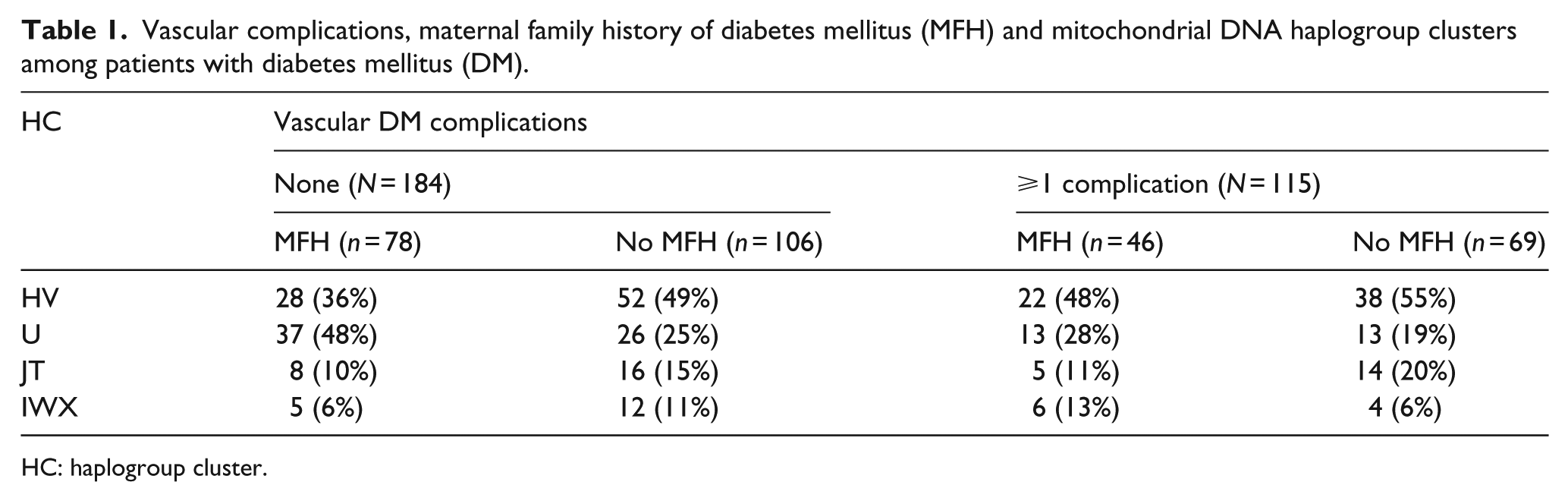
HC: haplogroup cluster.
Haplogroup U was more prevalent among patients with no vascular DM complications than among those with at least one complication (p = 0.038). Four groups were then defined on the basis of the presence or absence of vascular complications and the presence or absence of MFH. The frequency of haplogroup clusters differed among these groups (p = 0.017). Detailed analysis showed that haplogroup U was most prevalent among patients with MFH but no vascular DM complications (Table 1). The prevalence of haplogroup U was different from those observed in the three other groups, the most striking difference being in comparison to the group with at least one vascular DM complication but no MFH (p = 0.0003 for difference). The prevalence of haplogroup clusters did not differ between the other three groups. To further analyse whether age, duration of DM, gender, MFH and presence of complications were independently associated with haplogroup U, a multivariate logistic regression analysis was performed. Only the lack of complications (odds ratio (OR): 1.5; 95% confidence interval: 0.8–2.8) and MFH (OR: 2.3; 95% confidence interval: 1.3–3.9) were associated with haplogroup U.
We found mtDNA haplogroup U to be more frequent among patients without vascular DM complications than among patients with at least one complication. This effect was observed among patients who reported MFH, but not among those patients who reported no such family history. Thus, haplogroup U seems to be inversely associated with vascular complications of DM, and this association is related to MFH. Interestingly, a previous study found an association between MFH and a reduced risk of cardiovascular disease among women with type 2 DM. 5 MtDNA haplogroups affect both the assembly and the stability of the mitochondrial respiratory chain. 6 Therefore, haplogroups may differ in their propensity for the production of oxygen free radicals and, further, for the development of endothelial dysfunction, providing one putative mechanism of how the mtDNA haplogroups might modify the risk of vascular DM complications.
Unfortunately, the clinical data abstracted from the patient records did not allow us to control for the several conventional vascular risk factors in DM (such as cholesterol or HbA1c levels, hypertension or smoking) among subjects. However, we find it unlikely that the associations found between MFH, mtDNA haplogroups and vascular DM complications would be confounded by differences in the burden of such vascular risk factors among patients. In addition to the limitations of the available medical history data, a weakness of this study is the relatively small number of patients included. Further studies are, therefore, warranted to replicate and confirm these findings.
Our findings suggest that mtDNA haplogroup U is associated with MFH and inversely associated with vascular complications of DM. The complex association pattern suggests that different mitochondrial factors might influence the risk of DM per se and the risk of vascular DM complications.
Footnotes
Acknowledgements
The authors thank Ms Anja Heikkinen and Ms Pirjo Keränen for their expert technical assistance.
Declaration of conflicting interests
All authors declare that there are no conflicts of interest related to this article.
Funding
This work was supported by a grant from the Sigrid Jusélius Foundation.