
Abstract
Objective:
The aim of this study was to determine the impact of diabetes and diastolic dysfunction on exercise capacity in asymptomatic, normotensive patients with type 2 diabetes without coronary artery disease.
Methods:
A total of 43 type 2 diabetes patients (age: 50 ± 5 years) and 20 healthy controls (age: 48 ± 4 years) were enrolled. Diastolic function was investigated by conventional pulsed-wave (PW) Doppler and tissue Doppler imaging (TDI). Exercise capacity was evaluated with cardiopulmonary exercise testing (CPET).
Results:
In patients with type 2 diabetes, increase in resting heart rate (HR-rest) (p = 0.013), decrease in maximum heart rate during exercise (HR-max) (p < 0.001) and exercise time (p < 0.001) compared with controls were significant. Patients had significantly increased minute ventilation volume (VE)/maximum carbon dioxide discharge (VCO2) ratio (p < 0.001), decreased maximum oxygen consumption (VO2-max) (p < 0.001), oxygen consumption at anaerobic threshold (VO2-an) (p < 0.001) and maximum carbon dioxide discharge (VCO2) (p < 0.001) compared to controls indicating significantly reduced exercise capacity. HbA1c was inversely correlated with VO2-max (r = −0.456, p < 0.01) independent of the absence or presence of mild diastolic dysfunction.
Conclusion:
Exercise capacity was found to be significantly decreased in normotensive patients with type 2 diabetes without coronary artery disease, and this decrease was independent of diastolic dysfunction.
Introduction
Patients with type 2 diabetes often complain of fatigue and reduced exercise capacity which may be related to other disease conditions, such as hypertensive left ventricular hypertrophy and/or coronary artery disease, and the subsequent development of heart failure, but the presence of diabetes may independently contribute to the impaired exercise capacity.1–3 Several studies have revealed that exercise capacity decreases in patients with type 2 diabetes and is related with cardiac mortality. 3 The evidence indicates that in patients with type 2 diabetes, myocardial damage with fibrosis and apoptosis, failure in energy consumption, small vessel disease and autonomic neuropathies affect diastolic function before systolic function which is independent of hypertension and coronary artery disease and leads to diabetic cardiomyopathy.2,4
Echocardiography plays a central role in the evaluation of diastolic function, and conventional pulsed-wave (PW) Doppler is usually performed to obtain mitral inflow velocities to assess left ventricular filling. 5 Doppler pattern of impaired left ventricular relaxation, characterized by decreased early and increased late diastolic flow, is an early sign of diastolic dysfunction.5,6 More advanced grades consist of pseudonormal and restrictive left ventricular filling patterns manifested by predominant early diastolic filling and rapid velocity decceleration.5,6 Pseudonormal and normal patterns cannot be distinguished by PW transmitral inflow because of its preload dependence, and tissue Doppler imaging (TDI) is used to confirm the grade of diastolic dysfunction.5,6 For the assessment of global left ventricular diastolic function, it is recommended to acquire and measure mitral annular velocities with TDI signals at least at the septal and lateral sides of the mitral annulus and their average. 5
The objective of this study was to determine the impact of diastolic dysfunction with impaired relaxation on exercise capacity in asymptomatic, normotensive patients with moderately controlled type 2 diabetes without coronary artery disease.
Research design and methods
A total of 43 asymptomatic, which are free from angina, exertional dyspnoea, normotensive type 2 diabetes patients (mean age: 50 ± 5 years, male/female: 24/19) and 20 healthy subjects (mean age: 48 ± 4 years, male/female: 13/7) were enrolled after written informed consent had been obtained. Excluding criteria were hypertension, known or suspicious coronary artery disease, cardiac arrhythmias and/or bundle branch blocks, chronic renal and/or liver disease, chronic obstructive pulmonary disease and inappropriate physical condition which restricts the exercise capacity, pseudonormal and restrictive left ventricular filling patterns with PW Doppler echocardiography and TDI which indicates more severe diastolic dysfunction. Local Ethical Committee of Istanbul University, Istanbul Medical Faculty, approved the study (2010/328-54).
Detailed medical history was collected from each subject, and they underwent physical examination. In the patient group, diabetes was diagnosed by the ‘American Diabetes Association 2010 Guidelines’ 7 criteria. Patients with one of the following criteria was diagnosed as type 2 diabetes: HbA1c ⩾ 6.5% or fasting plasma glucose ⩾126 mg/dL or 2-h post-challenge glucose ⩾200 mg/dL or a random plasma glucose ⩾200 mg/dL or participants receiving hypoglycaemic medication. Duration of diabetes and drugs used were based on patient data. Patients with type 2 diabetes were using insulin and oral antidiabetic drug; none of these drugs impaired cardiac systolic and diastolic function. All the participants were normotensives, blood pressure was <140/90 mmHg on at least >2 measures and the patients and the control group were never on antihypertensive or statin treatment. After 12-h fast, a venous blood sample was collected for the following: plasma glucose level, glycated HbA1c, total serum cholesterol, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, serum triglycerides (TG), serum creatinine and whole blood count. Resting electrocardiogram (ECG) recordings were obtained.
Pro-brain natriuretic peptide (pro-BNP) levels were measured with electro-chemiluminescence immunoassay (ECLIA) in order to exclude the neurohormonal presence of heart failure, and <125 pg/mL was considered as normal value. 8 Morning spot urine samples were collected for microalbuminuria as a marker of diabetic nephropathy, and immunoturbidity method was used for the measurement; <30 mg/L was accepted as normal value. 9
Standard M-mode and two-dimensional echocardiography and Doppler blood flow measurements were performed in agreement with the American Society of Echocardiography guidelines. 10 Echocardiographic measurements were performed in participants of the study with VIVID 7 (General Electric (GE)) echocardiography machine with 3 MHz transthoracic transducer at left lateral decubitus position and all images were saved at digital media. Left ventricular end-diastolic internal diameter (LVEDD), Left ventricular end-systolic diameter (LVESD), septal (interventricular septal thickness (IVST)) and posterior wall thickness (PWT) were obtained from the parasternal long-axis view. The left ventricular end-systolic volume (LVESV) and left ventricular end-diastolic volume (LVEDV) were obtained from two-dimensional apical images, and left ventricular ejection fraction (LVEF%) was calculated from two-dimensional apical four-chamber images according to the Simpsons method. 10
Left ventricular mass (LVM) was calculated by the formula LVM (g) = 0.8 × 1.04 [(LVEDD + IVST + PWT) 3 − (LVEDD) 3 ] + 0.6, proposed by Devereux et al. 11 and indexed by body surface area.
Left ventricular diastolic function parameters were measured with conventional PW, continuous wave (CW) Doppler and TDI. PW Doppler was performed in the apical four-chamber view to obtain mitral inflow velocities to assess left ventricular filling. The sample volume was placed between the mitral leaflet tips at diastole; mitral velocity recordings were obtained at a sweep speed of 50 mm/s and averaged over three consecutive cardiac cycles. The measurements of mitral diastolic filling included the E-wave and A-wave velocities, the E/A ratio, and deceleration time (DT) of early filling velocity. The cursor of the CW Doppler was placed in the left ventricular outflow tract to simultaneously display the end of aortic ejection and the onset of mitral inflow in order to measure and record isovolumetric relaxation time (IVRT), which is the interval from the closure of the aortic valve to the opening of the mitral valve, and isovolumetric contraction time (IVCT), which is the interval from the closure of the mitral leaflets and aortic opening. The interval between the opening and closure of the aortic valve was measured which is called as the ejection time (ET). Then, myocardial performance index (MPI) was calculated by the formula MPI = (IVCT + IVRT)/ET. This is a simple, easily recordable, non-invasive Doppler index of myocardial performance and correlates well with invasive measurements of left ventricular systolic and diastolic function. 12
TDI was performed in the apical four-chamber views to acquire mitral annular velocities. The sample volume was positioned 1 cm within the septal and lateral insertion sites of the mitral leaflets, and annular velocities were obtained at a sweep speed of 50 mm/s at end-expiration. The measurements were maximum systolic mitral annular myocardial rate (Sm), early diastolic (e′) and late diastolic (a′) velocities and e′/a′ ratio. Septal and lateral e′ and a′ were averaged. After these measurements, the ratio of mitral inflow E velocity to tissue Doppler septal e′ (E/e′) was acquired which plays an important role in the estimation of left ventricular filling pressures. Using the septal E/e′ ratio, ratio <8 is usually associated with normal left ventricular filling pressures, whereas a ratio >15 is associated with increased filling pressures. 5
Symptom-limited cardiopulmonary exercise testing (CPET) with Bruce protocol was performed by ‘Quinton 65 treadmill’ walking band with ‘Quinton 5000’ exercise testing system and ‘Cortex Metalyzer 3B’ metabolic measurement apparatus by the help of ‘Metasoft 2.7’. In order to measure the metabolic parameters of the participants, ‘Rudolph Mask 2 way 7910’ was used. Standard 12-lead ECGs were obtained at rest, each minute during exercise and for at least 5 min during the recovery phase; blood pressure was measured using a standard cuff sphygmomanometer. Exercise parameters examined were resting heart rate (HR-rest; pulse/min), exercise period (min), maximum heart rate during exercise (HR-max; pulse/rate), maximum oxygen uptake (VO2-max) (mL/kg/min), amount of oxygen consumption at the anaerobic threshold (VO2-an) (mL/kg/min), maximum minute ventilation volume (VE) (L/min), maximum carbon dioxide discharge (VCO2) (L/min) and VE/VCO2 slope. 13
All the participants underwent echocardiography and CPET on the same day, that is, 3 days after the physical examination and biochemical investigation. Patients with type 2 diabetes were then divided into two subgroups according to the presence (type 2 diabetes with diastolic dysfunction (DD-DM)) or absence (type 2 diabetes with normal diastolic function (DFN-DM)) of diastolic dysfunction using the data of conventional and TDI measurements. In this study, criteria for normal left ventricular diastolic function were E/A ratio >1, E-wave DT ⩽220 msn, IVRT <100 msn and averaged e′/a′ >1; diastolic dysfunction with impaired left ventricular relaxation determining criteria were E/A ratio <1, DT ⩾220 msn, IVRT ⩾100 msn and e′/a′ ratio <1. 5
Statistical analysis
Statistical analysis was performed by Statistical Package for Social Sciences for Windows (SPSS, version 10.5). Values were presented as mean ± standard deviation (SD); χ2 test was used to compare the categorical values of patient and control groups, and parametrical continual values were compared with Student’s t-test. In the comparison of diabetic patients with and without diastolic dysfunction and control groups, single-sided variance analysis and Scheffe correction formula were used. Pearson correlation test was used for evaluation of the relationships between parametrical continuous variables, and value p < 0.05 was accepted statistical level of significance.
Results
A total of 43 normotensive subjects with type 2 diabetes on follow-up for 6.9 ± 4.2 years, without coronary artery disease, hypertension and/or heart failure and 20 healthy age- and sex-matched controls were included. A total of 21 patients (48%) were on oral antidiabetic and insulin treatment, the rest 22 (52%) only on oral antidiabetics, and none of the patients was receiving blood pressure lowering drugs or statins. The body mass index (BMI), smoking status, systolic and diastolic blood pressures, and biochemical indices were similar for both patients and controls. Diabetes group had significantly increased serum glucose and HbA1c levels (p < 0.001 for both) as expected. Pro-BNP levels were similar and within normal range in both groups. Microalbuminuria was slightly but non-significantly elevated in both patients and controls. Resting ECG was on sinus rhythm in each subject. Echocardiographic left ventricular dimensions and volumes, ejection fraction (EF)%, LVM and mass indexes were similar and within normal range in both controls and patients. No subject had echocardiographically detectable regional wall motion abnormalities; each subject had normal valvular structure and functions. Demographic, biochemical and echocardiographic characteristics of the controls and the patients with type 2 diabetes are shown in Table 1.
Demographic, biochemical and echocardiographic characteristics of the controls and the patients with type 2 diabetes.
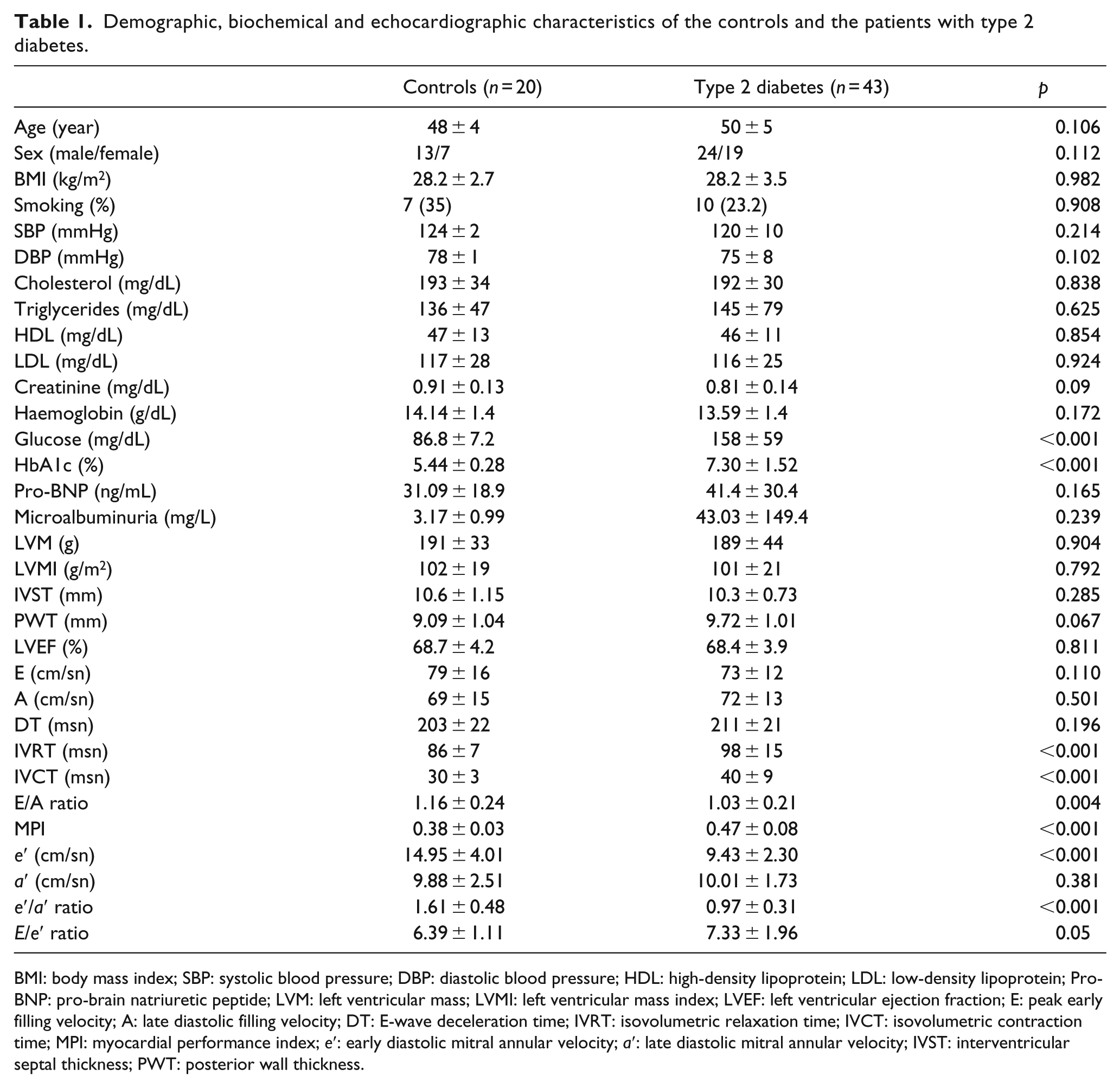
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; Pro-BNP: pro-brain natriuretic peptide; LVM: left ventricular mass; LVMI: left ventricular mass index; LVEF: left ventricular ejection fraction; E: peak early filling velocity; A: late diastolic filling velocity; DT: E-wave deceleration time; IVRT: isovolumetric relaxation time; IVCT: isovolumetric contraction time; MPI: myocardial performance index; e′: early diastolic mitral annular velocity; a′: late diastolic mitral annular velocity; IVST: interventricular septal thickness; PWT: posterior wall thickness.
In the control group, all the subjects (male/female: 13/7, 48.3 ± 5.8 years old) had normal diastolic function. In the diabetes group, E/A ratio was significantly decreased (p < 0.004) and IVRT and IVCT were significantly increased (p < 0.001 for all) as a marker of decreased left ventricular relaxation with diastolic dysfunction. In the patient group, TDI-derived e′ and e′/a′ were significantly reduced (p < 0.001 for each) indicating diastolic dysfunction, whereas a′ and E/e′ were similar. The MPI was within normal range in control group and slightly but significantly increased in diabetic group showing a non-invasive measurement of left ventricular systolic and diastolic function, which is expected to increase more in patients with heart failure (Table 1).
A symptom-limited CPET was performed in both diabetes and control groups. The resting HR was significantly increased, and maximum HR at maximum exercise was significantly decreased in diabetes group (p = 0.013 and p < 0.001, respectively). Exercise time was 10.2 ± 3.0 min in controls and 7.1 ± 2.2 min in diabetes group, which shows restricted exercise time in diabetes, and this result was found to be statistically significant (p < 0.001). The patients had significantly decreased VO2-max, VO2-an and VCO2 (p < 0.001 for all), indicating significantly decreased peak oxygen uptake during exercise, decreased amount of oxygen consumption at the anaerobic threshold and decreased maximum carbon dioxide discharge during exercise. Similarly, VE/VCO2 slope which is the index of ventilatory efficiency was significantly increased in the diabetes group (p < 0.001). The minute ventilation (VE) was found to be non-significant (p = 0.416) despite a slight increase in diabetes group. BMI was found to be inversely correlated with VO2-max (r = −0.26, p = 0.043), indicating decrease in maximum oxygen uptake as BMI increases. Another important and significant result was the correlation of HbA1c and oxygen consumption during exercise. The patient group of this study consisted of moderately controlled type 2 diabetes patients with HbA1c levels of 7.3% ± 1.52%. HbA1c levels were found to be inversely correlated with VO2-max (r = −0.456, p < 0.01), indicating significant decrease in maximum oxygen uptake as HbA1c levels increase (Figure 1). Table 2 summarizes the CPET-derived data.
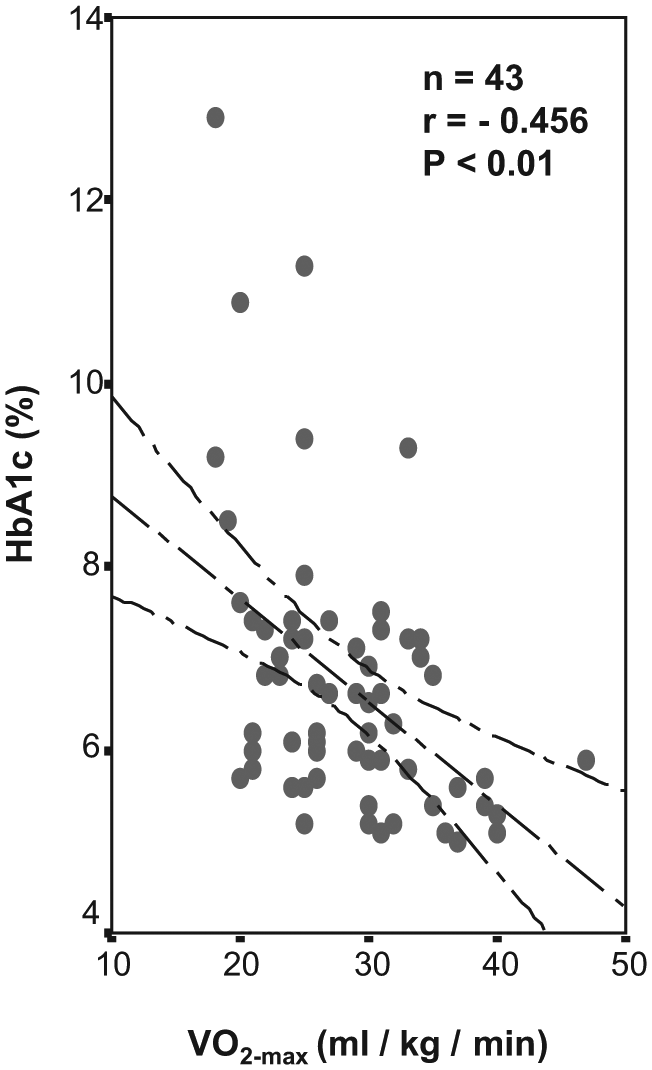
HbA1c levels were inversely correlated with maximum oxygen consumption (VO2-max) indicating significant decrease in VO2-max as HbA1c increases.
Cardiopulmonary exercise testing characteristics of the controls and the patients with type 2 diabetes.
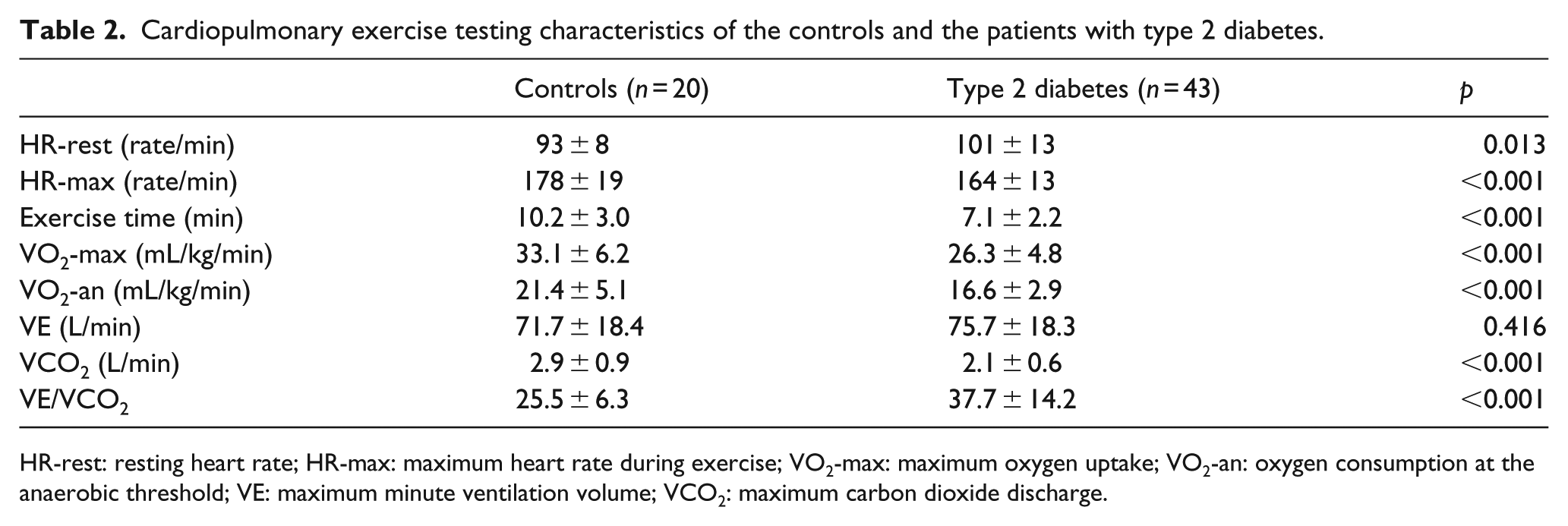
HR-rest: resting heart rate; HR-max: maximum heart rate during exercise; VO2-max: maximum oxygen uptake; VO2-an: oxygen consumption at the anaerobic threshold; VE: maximum minute ventilation volume; VCO2: maximum carbon dioxide discharge.
The patients with type 2 diabetes were divided into two subgroups according to the presence (DD-DM) or absence (DFN-DM) of diastolic dysfunction with impaired relaxation according to the PW and TDI variables mentioned above. The DFN-DM subgroup (24 patients, male/female: 12/12, 49 ± 1 years old) and DD-DM (19 patients, male/female: 12/7, 51 ± 1 years old) have similar demographic and biochemical variables summarized in Table 3.
Demographic, biochemical and echocardiographic characteristics of the controls and the subgroups of patients with type 2 diabetes with and without diastolic function.
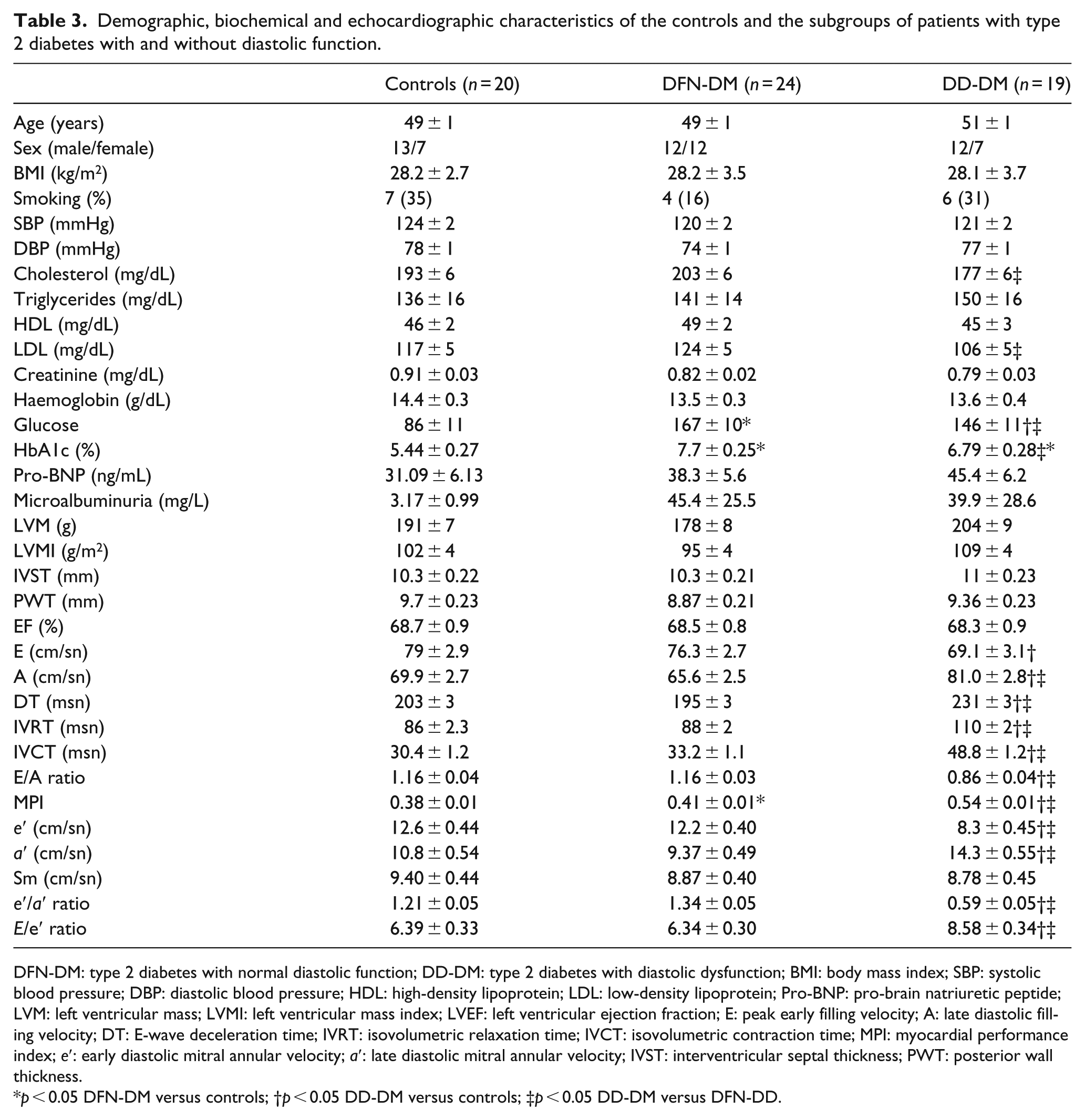
DFN-DM: type 2 diabetes with normal diastolic function; DD-DM: type 2 diabetes with diastolic dysfunction; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; Pro-BNP: pro-brain natriuretic peptide; LVM: left ventricular mass; LVMI: left ventricular mass index; LVEF: left ventricular ejection fraction; E: peak early filling velocity; A: late diastolic filling velocity; DT: E-wave deceleration time; IVRT: isovolumetric relaxation time; IVCT: isovolumetric contraction time; MPI: myocardial performance index; e′: early diastolic mitral annular velocity; a′: late diastolic mitral annular velocity; IVST: interventricular septal thickness; PWT: posterior wall thickness.
p < 0.05 DFN-DM versus controls; †p < 0.05 DD-DM versus controls; ‡p < 0.05 DD-DM versus DFN-DD.
The comparison of DFN-DM and DD-DM subgroups revealed a slight but significant increase in MPI, however not matching the criteria for heart failure in DD-DM group (p < 0.05), which shows that myocardial performance is more deteriorated in patients with concomitant diabetes and mild diastolic dysfunction. In the DD-DM group, there was a mild but significant increase in septal E/e′ ratio in DFN-DM group compared with DD-DM group (p < 0.05), which cannot be interpreted as an increase in left ventricular filling pressures. The two subgroups had similar HR-rest and HR-max, exercise time, VO2-max, VO2-an, VE, VCO2 and VE/VCO2 slope (Table 4). These results can be interpreted as the deterioration of exercise parameters measured during CPET in patients with type 2 diabetes is independent of the absence or presence of diastolic dysfunction.
Cardiopulmonary exercise testing characteristics of the controls and subgroups of patients with type 2 diabetes with and without diastolic dysfunction.
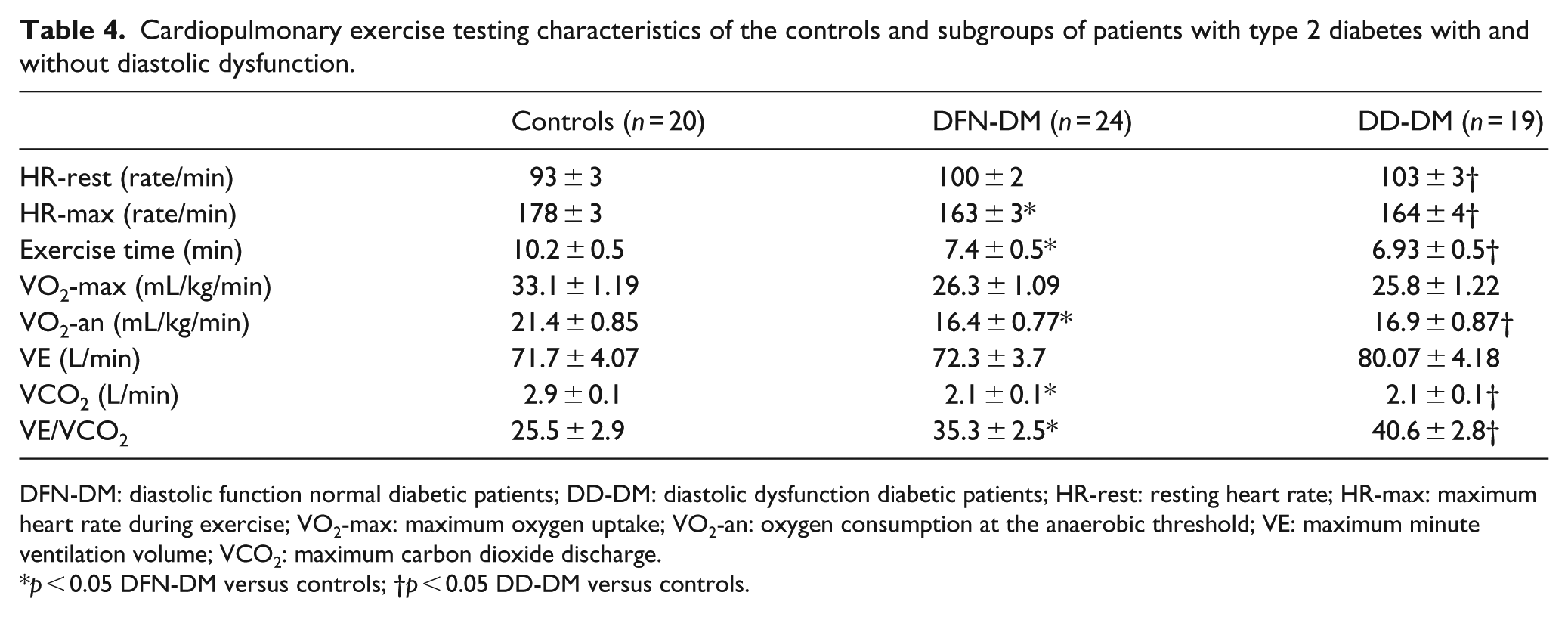
DFN-DM: diastolic function normal diabetic patients; DD-DM: diastolic dysfunction diabetic patients; HR-rest: resting heart rate; HR-max: maximum heart rate during exercise; VO2-max: maximum oxygen uptake; VO2-an: oxygen consumption at the anaerobic threshold; VE: maximum minute ventilation volume; VCO2: maximum carbon dioxide discharge.
p < 0.05 DFN-DM versus controls; †p < 0.05 DD-DM versus controls.
Discussion
The major finding of this study is exercise capacity is impaired in asymptomatic type 2 diabetes with moderately glycaemic control, despite the absence of hypertension and coronary artery disease, and this impairment is independent of the absence or presence of mild diastolic dysfunction. Patients with type 2 diabetes included in the study had normal EF% and blood pressures; coronary artery disease was ruled out; pro-BNP and MPI were within normal range indicating the absence of overt heart failure; and each subject had a normal value of LVM. Left ventricular diastolic function was evaluated with conventional PW Doppler echocardiography, and TDI was performed in order to rule out the pseudonormal filling patterns, and patients with impaired left ventricular relaxation which is the mild form of diastolic dysfunction were included.
Previous studies have shown that the exercise capacity is impaired in patients with type 2 diabetes. Reduced exercise capacity in patients with type 2 diabetes is associated with diabetes control, subclinical left ventricular dysfunction and impaired HR recovery in one study 14 and with poorly controlled diabetes in another. 15 A few studies have shown that maximum oxygen uptake, 16 work capacity 17 or exercise duration 18 are inversely correlated with HbA1c. Correspondingly, some studies have demonstrated that well-controlled glycaemia has favourable effects on cardiopulmonary function, 19 and exercise capacity increases 24% after improvement of hyperglycaemia with subcutaneous insulin infusions. 14 The patient group of this study included moderately controlled glycaemia with HbA1c levels of 7.3% ± 1.52%, and it was inversely correlated with VO2-max. The results of this study are consistent with the studies mentioned, but we have not investigated the values of CPET in the case of improvement or deterioration of the HbA1c values.
Another point of view is the detection of diastolic dysfunction in diabetic hearts without hypertrophy indicating that hypertrophy is not a requisite of diabetes-induced ventricular dysfunction. 20 Previous studies have observed left ventricular diastolic dysfunction in 47%–75% of asymptomatic normotensive patients with well-controlled type 2 diabetes from transmitral left ventricular filling patterns4,21 In this study, diastolic function was investigated both with transmitral left ventricular diastolic filling patterns and TDI annular velocities, and diastolic dysfunction was found to be 44%, which is rather less than the other studies, TDI may be the point of fact. TDI is a more sensitive method for detection of left ventricular dysfunction than conventional PW Doppler; it enables measurement of myocardial tissue velocities in the longitudinal direction, and the peak early diastolic myocardial velocity (e′) reflects the global left ventricular diastolic function. 20 Kosmala et al. 22 and Di Bonito et al. 23 have reported before that e′ was significantly lower in diabetic patients without hypertension than in normal subjects, encouraging our results.
Patients with type 2 diabetes often complain of fatigue and reduced exercise capacity which may be related to other disease conditions, such as hypertension, hypertensive left ventricular hypertrophy or coronary artery disease, but the presence of diabetes may independently contribute to the impaired exercise capacity. 2 The evidence indicates that myocardial damage in patients with type 2 diabetes affects diastolic function before systolic function. 4 In these patients, the existence of a pre-clinical diastolic dysfunction has been well defined, and estimates of prevalence vary from 20% to 60% depending on the Doppler echocardiographic critera and are associated with worse outcome. 1 Several lines of evidence indicate that left ventricular diastolic dysfunction may precede left ventricular systolic dysfunction. 4 This early restrictive disease seen in patients with type 2 diabetes is reported as likely due to microangiopathy, interstitial fibrosis, extracellular collagen deposition, cardiomyocyte loss, impaired energy usage, small vessel disease, autonomic neuropathy, calcium transport abnormalities and neurohormonal alterations, alone or in combination, independent from hypertension and coronary artery disease.1,24 The steps following this pathophysiology may be the development of diabetic cardiomyopathy and heart failure, which is a controversial subject of the debate and needs further investigation. The clinical significance of these results and their potency on prognosis and treatment remain to be determined. We believe that prospective studies with larger sample sizes investigating the pathophysiology of decreased exercise capacity in diabetes may lead to earlier diagnosis of pre-clinical left ventricular failure associated with diabetic cardiomyopathy, which will give opportunity to the development of new treatment modalities and prevent the progression of heart failure.
Study limitations
In this study, we tried to rule out coronary artery disease and ischaemia by non-invasive symptom-limited treadmill exercise test and wall motion assessment by transthoracic echocardiography. Although the patients had normal resting ECG, treadmill exercise test and wall motion, the methods used do not rule out the existence of atherosclerosis. Hypertension was excluded with clinical follow-up; ambulatory blood pressure recordings were not available because of financial problems. The study was limited to a small group of well characterized, moderately controlled type 2 diabetes patients without any manifest clinical evidence of major and/or minor diabetic complications. All the patients had normal EF% indicating normal systolic function and no signs of left ventricular hypertrophy on echocardiography. All the tests were performed only once for the patients and the control group; however, the assessment of the data was evaluated precisely.
Footnotes
Declaration of conflicting interests
No conflicts of interest have been declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.