
Abstract
Recently, copeptin was found associated with cardiovascular disease (CVD) and all-cause mortality in type 2 diabetes mellitus (T2DM) patients treated in primary care. This study aimed to evaluate whether plasma copeptin correlated to CVD in asymptomatic T2DM patients intensively investigated for sub-clinical CVD. A total of 302 T2DM patients referred to the Diabetes Clinic at Odense University Hospital, Denmark, entered the study. None of the patients had known or suspected CVD. As a control group, 30 healthy adults were recruited from the DanRisk study – a random sample of middle-aged Danes. A variety of clinical investigations were performed, including blood pressure measurements, carotid intima media thickness evaluation and myocardial perfusion scintigraphy. Blood sample analyses included copeptin measurements. Median plasma copeptin concentrations were similar in the T2DM group and the control group. However, men had significantly higher copeptin concentrations than women in the T2DM group (p < 0.001), and also, T2DM men had significantly higher copeptin concentrations than men without T2DM (p = 0.038). Copeptin correlated significantly with a number of variables, but the strongest correlation was with creatinine (R = 0.432, p < 0.001), and in multiple regression analysis, only this correlation remained significant. When association with clinical scores were investigated, plasma copeptin remained significantly associated with peripheral arterial disease (PAD) (p = 0.01). We found correlations between creatinine, copeptin levels and PAD in T2DM patients, and if confirmed, plasma copeptin combined with plasma creatinine could be a candidate for PAD screening in T2DM patients.
In the search for valid biomarkers for asymptomatic cardiovascular disease (CVD) in type 2 diabetes mellitus (T2DM), patients arginine vasopressin (AVP), also known as antidiuretic hormone, has been investigated. It plays a central role in cardiovascular homeostasis, but due to a very short half-life, it is difficult to measure in plasma. 1 Copeptin shares the same precursor as AVP (prepro-vasopressin) and is released at a 1:1 molar ratio with AVP, 2 but unlike AVP, copeptin is stable in plasma at room temperature and has a longer half-life. Copeptin concentrations are therefore considerably higher than AVP in plasma samples, which enable valid measurements. Copeptin measurement adds to the diagnostic value of troponin in the diagnosis of acute myocardial infarction, 3 and copeptin is also a prognostic biomarker in patients with chronic heart failure. 4 Recently, copeptin was found associated with CVD and all-cause mortality in T2DM patients treated in primary care, 5 and we therefore conducted a study to evaluate whether copeptin correlated to CVD in asymptomatic T2DM patients intensively investigated for sub-clinical CVD.
From a population of 753 T2DM patients referred to the Diabetes Clinic at Odense University Hospital, Denmark, 302 patients with copeptin measurements met the inclusion criteria as previously reported. 6 None of the patients had known or suspected CVD. As a control group, 30 healthy adults were recruited from the DanRisk study, which includes a random sample of middle-aged Danes. 7 Our study followed the Helsinki II Declaration and is registered at http://www.clinicaltrials.gov . Clinical investigations were performed as previously described, 6 including arm, ankle brachial index (ABI) and toe systolic pressure index (TSPI) blood pressure measurements, carotid intima-media thickness (CIMT) evaluation and myocardial perfusion scintigraphy. Three different scores were used to evaluate CVD: peripheral arterial disease (PAD), carotid arterial disease (CAD) and summed stress score (SSS), also defined as previously described. 6 The copeptin analysis was performed using a Kryptor device (Thermo Fisher, Germany). HbA1c was measured by cation-exchange chromatography (Tosoh G7, Medinor, Denmark), while glucose, lipids and high-sensitive C-reactive protein (CRP) were analysed on a Modular Analytics P (Roche Diagnostics, Switzerland). Variables were tested for Gaussian distribution, and as copeptin was not normally distributed, data are reported as median (interquartile ranges). The Mann–Whitney test was used for non-Gaussian distributed variables, and Spearman’s test was applied for correlation analysis. Multiple regression analysis was conducted with forward entry of parameters positively correlated in the former analyses.
As shown in Table 1, median plasma copeptin concentration in the T2DM group was the same as in the control group. T2DM men had significantly higher copeptin concentrations than men without T2DM (p = 0.038), while women did not differ. Within each group, men had significantly higher copeptin concentrations than women in the T2DM group (p < 0.001), while there were no differences in the control group. Copeptin correlated significantly with age, duration of diabetes, systolic blood pressure, haemoglobin, insulin, C-peptide and creatinine, the latter with an R = 0.432 (p < 0.001). Copeptin also correlated with CIMT (p = 0.018), but there were no correlations with SSS, ABI or TSPI. In multiple regression analysis, only the correlation between copeptin and creatinine remained significant, as stepwise entry revealed that the other correlations were due to a confounding effect from creatinine. When association with clinical scores (PAD, CAD and SSS) were investigated with backward stepwise entry, copeptin was significantly associated with PAD (p = 0.01) but not with the other clinical scores.
Copeptin concentrations (pmol/L) in the two groups and divided by gender.
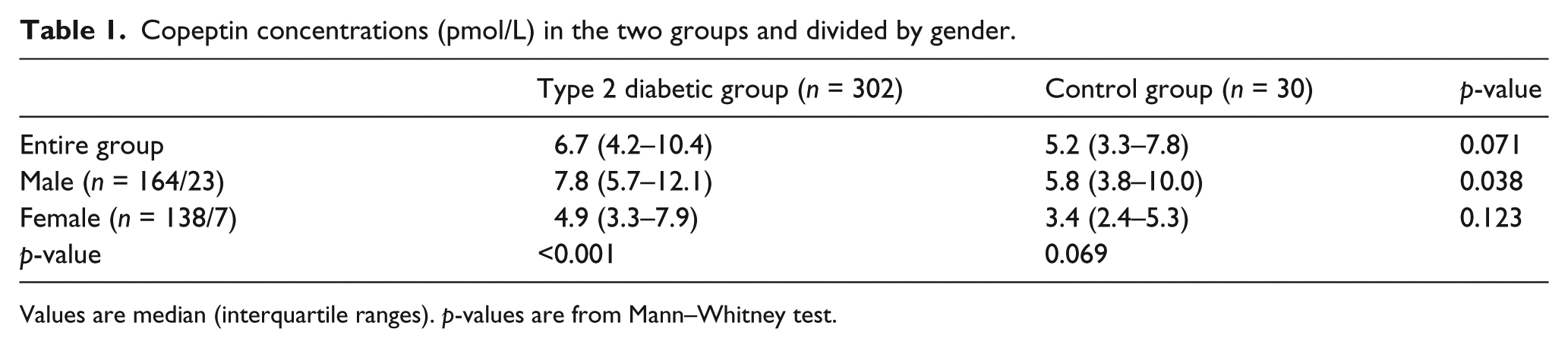
Values are median (interquartile ranges). p-values are from Mann–Whitney test.
Our study discloses several aspects concerning plasma copeptin concentrations in T2DM patients: first, men had higher concentrations than women, and diabetes men had significantly higher levels than non-diabetes men. Second, plasma copeptin correlated strongly with plasma creatinine, and copeptin remained significantly associated with PAD after adjustment for other variables. The gender difference in copeptin concentrations is compatible with earlier reports,1,8 while the difference between men with and without diabetes is novel. Whether it reflects a true increased CVD risk cannot be deduced from these data, but it is suggestive that plasma copeptin levels follow the well-known CVD risk categories, namely women < men < T2DM men. Of note, Abbasi et al. 8 also found higher concentrations in men in a general population, but in women only, copeptin predicted diabetes at a later time point, which contradicts the idea that copeptin in itself should be a risk marker in a general population. The strong correlation we found between copeptin and plasma creatinine is compatible with previous studies, 9 and a recent study also found copeptin concentrations associated with decline in glomerular filtration in T2DM patients. 10 The association between plasma copeptin and PAD is also novel, and relevant information on asymptomatic CVD in T2DM could potentially be obtained measuring copeptin. However, further studies, including the effect of inhibitors on the renin–angiotensin–aldosterone system, are necessary before a more qualified judgement can be made on the relations between copeptin and the degree of atherosclerotic disease.
Altogether, we find correlations between creatinine, copeptin levels and PAD in T2DM patients, but further research is necessary to confirm these findings and to elucidate whether they are also present in non-diabetic subjects. If confirmed, plasma copeptin combined with plasma creatinine could be a candidate for PAD screening in T2DM patients.
Footnotes
Acknowledgements
We kindly thank Thermo Fisher for generous donation of the Copeptin kits used in this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was partly funded by the Danish Cardiovascular Research Academy (DaCRA), The Danish Diabetes Association and The Danish Heart Foundation.