
Abstract
Diabetes is associated with an increased cardiovascular risk. The role for aspirin in diabetes is of high clinical interest. Guidelines recommend that primary prevention of cardiovascular disease (CVD) in diabetes with aspirin should be based on the individual risk for CVD. New mechanistic studies suggest that enhanced platelet turnover may partly contribute to the fact the primary prevention studies found unequivocal results in diabetes. There is initial evidence that a potential future modification of dosages in diabetes may counteract the enhancement in platelet turnover in diabetes. The use of aspirin in diabetic patients for secondary prevention of CVD is supported by key evidence. The aim of the review is to present recent studies on aspirin for prevention of CVD in diabetes and to highlight its role also in view of new mechanistic and clinical studies with aspirin. Novel aspects of aspirin, e.g. its potential role for the prevention of cancer, are also presented.
Introduction
Diabetes mellitus is associated with an increased risk of cardiovascular events. In cardiovascular disease, all components of the ‘gluco-triade’, i.e. glycosylated hemoglobinA1c (HbA1c), fasting plasma glucose, and postprandial or postload plasma glucose are independently related with excessive morbidity and mortality. 1 A meta-analysis of 102 prospective studies including nearly 700,000 people found about a two-fold excess risk for vascular diseases in patients with diabetes (Figure 1). 2 Diabetic patients without a previous myocardial infarction have been shown to present with a comparable risk for cardiac mortality (20% over 7 years) as nondiabetic patients after myocardial infarction. 3
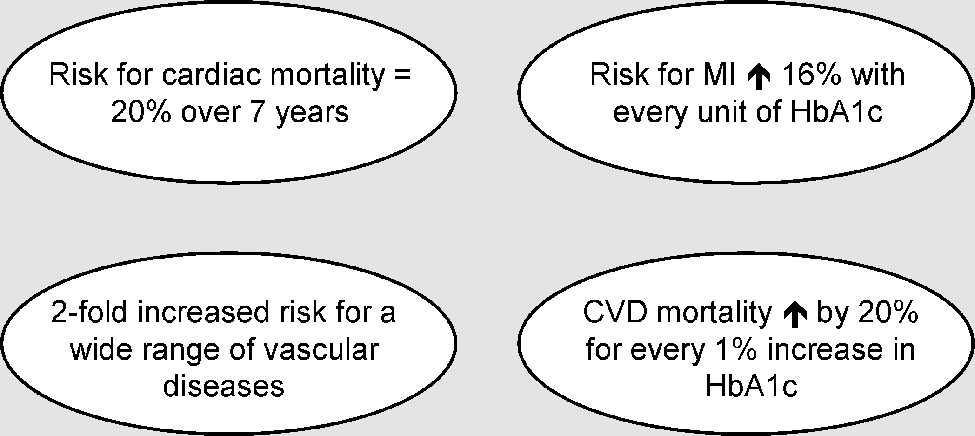
A graded association between the initial fasting and postprandial blood glucose level in nondiabetic people and the subsequent 12-year occurrence of cardiovascular (CV) events has been reported in a metaregression analysis of data from 20 studies including nearly 100,000 people. 4 In a large population study in Norway, cardiovascular disease (CVD) mortality was demonstrated to increase by 20% for every 1% increase in HbA1c. 5 In a post-trial monitoring of the United Kingdom Prospective Diabetes Study (UKPDS) the risk for myocardial infarction increased by 16% with every unit (%) increase of HbA1c (Figure 1). 6
The overall risk of CVD for people with diabetes is reported to be increased two- to threefold in men, and three- to fivefold in women. 1 A meta-analysis of epidemiological data for mortality from ischemic heart disease in relation to fasting plasma glucose (FPG) has demonstrated an overall increase of 20% for every 1 mmol/L increase of FPG above the optimum level. 7
Both for the short-term prognosis during a hospital stay, and also long-term over several years, the concentration of one single random blood glucose measurement in the acute condition of macrovascular complications was reported to be highly predictive.8–10
In diabetes the coagulation system is altered due to changes in clotting factor levels and/or activity. Plasma levels of procoagulant factors are reported to be increased while fibrinolytic capacity is decreased. 11 Insulin resistance and hyperglycaemia are reported to contribute to these alterations. 11 Hyperinsulinemia results in increased hepatic synthesis of prothrombotic factors such as fibrinogen and plasminogen activator inhibitor (PAI)-1, thereby creating a thrombotic milieu. Furthermore, diabetes causes quantitative modifications in clotting factors, including glycation and oxidation which also increase thrombosis risk. 11 In patients with type 2 diabetes decreased levels of adiponectin and increased levels of leptin, 12 both contributing to an accelerated atherogenic state, 13 are also found.
In diabetes, both the accelerated atherosclerosis and inflammation promote vascular complications. 14 Strategies to inhibit platelet activation and aggregation, therefore, are a pillar of key therapeutic strategies aimed at reducing the ischemic risk. 14
The aim of the current review is to highlight and summarize the role of aspirin for primary and secondary cardiovascular prevention in diabetes. New experimental and clinical study results on aspirin and diabetes as well as guideline recommendations are discussed. In view of the increased risk of colorectal carcinomas in people with type 2 diabetes,15–17 the potential role of aspirin to reduce the incidence of colorectal cancer is also highlighted.
Mechanisms of action and dosage of aspirin
Aspirin is considered to induce a permanent inactivation of cyclooxygenase (COX)-1 and -2 18 which play a key role in the catalysation of the biosynthesis of prostanoids like thromboxane A2 (TXA2) and prostacyclin. 19 Synthesis of TXA2 is largely derived from COX-1, 20 and is reported to induce vasoconstriction and irreversible platelet aggregation. 19 Prostacyclin, however, primarily derives from COX-2. 21 To inhibit COX-2 and, therefore, achieve analgesic and anti-inflammatory effects, higher doses of aspirin are needed than for inhibition of COX-1. 19 Due to this observation, a relative COX-1 selectivity is attributed to low-dose aspirin administration. 19 Therefore, low-dose aspirin achieves a consistent inactivation of platelets without inducing hypertensive effects or renal damage. 19
Due to the rapid inactivation of prostanoids, prostacyclin and thromboxane, their plasma concentrations and the levels of their primary metabolites, thromboxane B2 (TXB2) and 6-Keto Prostaglandin F1 alfa (6-Keto-PGF1 alfa) are reported to be no reliable indicators of their formation. 22 However, urinary excretion of TXA2’s major enzymatic metabolites (2,3-dinor-TXB2) such as 11-dehydro-TXB2 has been shown to reliably reflect the formation rates of prostanoids by various dosages and formulations of aspirin.22,23
The antiplatelet effect of low dose aspirin is not directly linked to the true systemic plasma concentrations of acetylsalicylic acid. 19 The acetylation of the target enzyme, COX-1, in platelets takes place in the mesenteric vessels before the first liver passage. Due to the irreversible blockade of the enzyme, the pharmacodynamic effect is maintained much longer than the short pharmacokinetic half-life of acetylsalicylic acid. 24 In healthy volunteers, a single-dose administration of 100 mg acetylsalicylic acid as immediate release (IR) and enteric-coated (EC) formulation provided a serum thromboxane inhibition of 90.1% and 86.5%. With both formulations serum thromboxane is almost completely (>95%) reduced when measured 7 days (100 mg/day). 22 Due to the cumulative presystemic acetylation of COX-1 in platelets, complete inhibition of serum thromboxane formation can be expected after only the first few doses (<7 days) of 100 mg acetylsalicylic acid either as IR or EC formulation. 24 The available evidence is reported to support daily doses of 75–100 mg for long-term prevention in patients at high risk of serious vascular effects. 25
Antithrombotic effects of aspirin, which do not include COX-dependent actions, need to be considered. 26 A reduction of thrombin generation with a subsequent attenuation of thrombin-mediated coagulant reactions such as factor XIII activation has been described.27–29 Aspirin has also been shown to acetylate lysine residues in fibrinogen, and thereby increases fibrin clot permeability and promotes clot lysis and fibrinolysis. 26
Gastrointestinal intolerability and/or side-effects have been reported in aspirin regimens using doses between 75 and 300 mg daily.22,30 As a consequence, lower doses (e.g. 40 mg daily) as well as EC formulations of aspirin have been introduced to prevent potential gastrointestinal side effects. 22 The 40 mg regimen was observed to cause a less complete inhibition of platelet aggregation and TXA2 formation, with a notable inter-individual variability. 22 In contrast, EC aspirin formulation (100 mg daily) was shown to inhibit platelet aggregation and platelet TXA2 formation to a degree which is comparable with the plain formulation (100 mg daily). 22 EC formulations of aspirin (100–300 mg) are, however, to be considered advantageous due to an improvement of gastroduodenal tolerance.22,31,32
Decreased responsiveness to aspirin administration in diabetes
The response to preventive aspirin administration can be assessed by different methods, e.g. bleeding time measurement, platelet aggregation testing, platelet function analyser, or expression of platelet surface receptors. 33 In studies, 5–57 % of patients are reported to have no optimal antiplatelet effects during aspirin treatment. 34 This observation is suggested to be related to an increased platelet turnover. 35 Normally, the administration of a low dose of aspirin once daily causes an almost complete deregulation of TXA2 formation and platelet aggregation throughout the entire platelet lifespan of 7–10 days. 36 Platelet function is restored by new, unacetylated platelets which are produced by megakaryocytes. 37 Accelerated platelet function recovery is suggested to play an important role in the variable response to aspirin. 36 In many people, a substantial recovery of COX-dependent platelet aggregation occurs within 24 hours after administration of aspirin. 35 Once daily administration of aspirin, therefore, might be insufficient in patients with enhanced platelet turnover. 35
Recovery of COX-1 activity in patients with type 2 diabetes treated with low-dose aspirin (100 mg once daily) has been demonstrated to be characterized by a large inter-individual variability. 38 Incomplete TXA2 inhibition during the 24-hour dosing interval has not been associated with poor glycaemic control. 38
Increased fractions of immature platelets or enhanced platelet turnover were also detected in diabetes.39–42 This phenomenon has been suggested to be present also in disease states characterized by inflammation and atherosclerosis.39–42 Recently, platelet dysfunction as well as increased platelet aggregation and aspirin insensitivity were reported to be more common in patients with type 2 diabetes and no clinical vascular disease, compared to nondiabetic people. 43 In addition, platelet dysfunction was found to be more pronounced in diabetic patients with poor glycaemic control. 43
To further optimize treatment with aspirin in patients with enhanced platelet turnover, a higher frequency of aspirin administration and possibly a higher daily dosage are currently being discussed.35,44–49 In diabetic patients, the enhancement of platelet turnover can be significantly counteracted by a twice daily aspirin regimen.44,48–50 Recently, a study of patients with type 2 diabetes and stable coronary artery disease demonstrated that doubling the frequency of aspirin administration but not doubling the once daily dose enhances platelet inhibition. 48 Improved laboratory responses on twice daily dosing have also been reported by other investigators.38,44,49
A lack of adherence, however, is also to be considered to be a very frequent cause of inadequate benefit from aspirin prescription.51–53 A large proportion of patients may not take the prescribed dosages of aspirin as required.54–56 Therefore, non-adherence has been assumed to be a key element, which needs to be considered. 53
Finally, a relation between decreased responsiveness to aspirin and the above mentioned COX-independent antithrombotic effects has been suggested. 26
Primary prevention of CVD in diabetes with aspirin
Studies
Numerous studies have assessed the effects of aspirin on primary prevention of CVD (Table 1). The Fremantle Diabetes Study observed that the administration of aspirin (≥ 75 mg/day) was independently associated with a decreased all-cause and cardiovascular mortality in a primary prevention setting in people with type 2 diabetes. 57 Within the follow-up period of a total of 7537 patient-years 160 patients (24.6%) died, including 70 (43.8%) due to CVD. 57 After adjustment for other significant variables, regular administration of aspirin in patients with type 2 diabetes and no prior history of CVD was associated with a reduction of CVD and all-cause mortality of at least 50%. 57 The strongest preventive effect was detected in men and patients older than 64. 57
Important studies on primary prevention with aspirin being discussed in this paper.
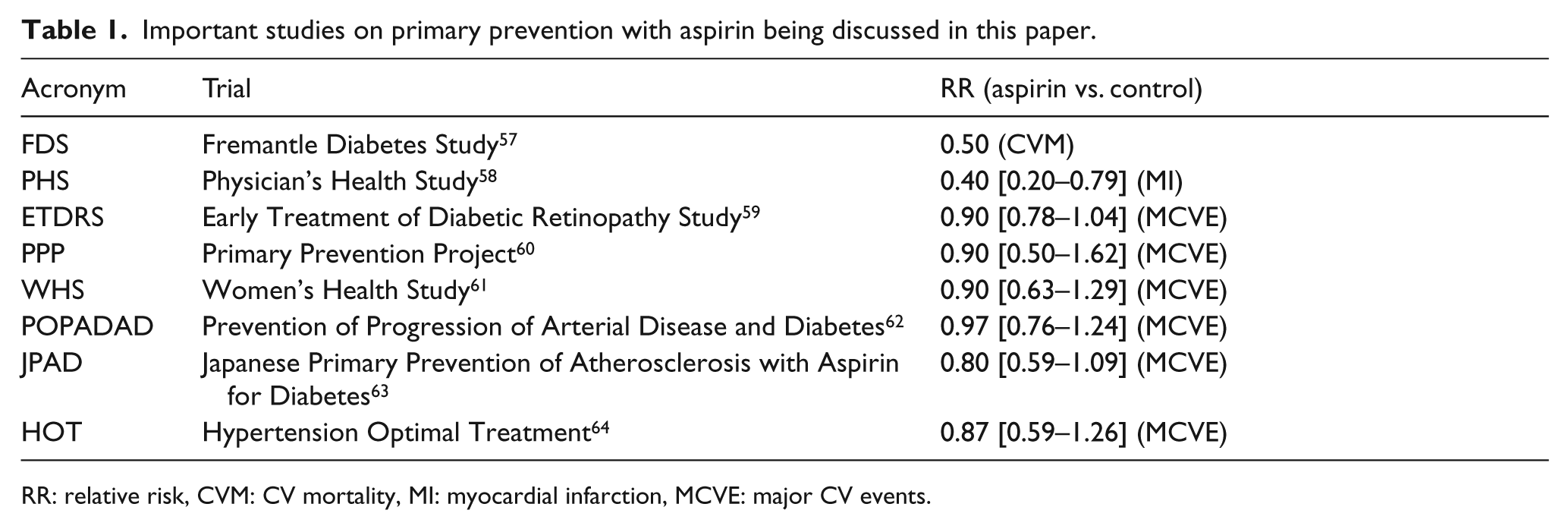
RR: relative risk, CVM: CV mortality, MI: myocardial infarction, MCVE: major CV events.
Three studies further assessed primary prevention of CVD in diabetes: the Early Treatment of Diabetic Retinopathy Study (ETDRS), 59 the Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) trial, 63 and the Prevention of Progression of Arterial Disease and Diabetes (POPADAD) trial. 62
ETDRS enrolled 3711 patients between the ages of 18 and 70 years with diabetes (30% type 1, 31% type 2, 39% unclassified), which were randomly assigned to aspirin (650 mg daily) or a placebo. 59 Of 446 incident myocardial infarctions in the entire group, 204 occured in the aspirin and 242 in the placebo group. 59 In the aspirin group, the relative risk for a first fatal or nonfatal myocardial infarction was reduced by 17% (99% confidence interval, 0.66 to 1.04). 59 The relative risk of total mortality was shown to be reduced non-significantly by 9%. 59 The ETDRS authors suggested that the use of aspirin in diabetic patients at increased CV risk is supported by their results. 59
The randomised controlled JPAD trial including 2539 patients with type 2 diabetes and no previous CVD was conducted to examine the efficacy of low-dose aspirin (81 or 100 mg daily) for the primary prevention of vascular events. 63 The combined primary end point included any atherosclerotic event, which was a composite of sudden death; death from coronary, cerebrovascular, and aortic causes; nonfatal acute myocardial infarction; unstable angina; newly developed exertional angina; nonfatal ischemic and haemorrhagic stroke; transient ischemic attack; or nonfatal aortic and peripheral vascular disease (arteriosclerosis obliterans, aortic dissection, mesenteric arterial thrombosis). 63 The fact that the primary end point also included atherogenic events, which are not expected to be modified by aspirin per se (e.g. angina), has been criticized and may have somewhat counteracted the value of the study.65,66
In the study, a total of 154 atherosclerotic events occurred: 68 in the aspirin group and 86 in the placebo group (hazard ratio (HR), 0.80; 95% confidence interval (CI), 0.58–1.10). 63 The combined end point of fatal coronary events and fatal cerebrovascular events occurred in 1 patient (stroke) in the aspirin and 10 patients (5 fatal myocardial infarctions and 5 fatal strokes) in the placebo group (HR, 0.10; 95% CI, 0.01–0.79; P = .0037). 63 Overall, the investigators concluded the risk of cardiovascular events not to be significantly reduced by low-dose aspirin. 63 The study design, however, was also criticized for low statistical power, since the predicted primary cardiovascular event rate was not met. In the study, 17 events /1000 patient years occurred compared to the prediction of 52 events /1000 patient years.65,67 The observed trend of a 20% risk reduction would have been significant if only harder end points had been included. 65
A subanalysis of JPAD of 2523 patients looked at the efficacy of low-dose aspirin on primary prevention in people with type 2 diabetes and coexisting renal dysfunction. 68 Aspirin reduced the incidence of atherosclerotic events in diabetic patients with estimated glomerular filtration rate (eGFR) 60–89 mL/min/1.73m2, but not in those with eGFR < 60 mL/min/1.73m2 and > 89 mL/min/1.73m2. It was hypothesized that eGFR may be applicable to identify patients who may benefit from primary prevention with aspirin. 68 The results were based on a post hoc subgroup analysis and need to be validated by additional studies. Furthermore, GFR is reported to be lower in the Japanese population compared to Caucasian people. 68
The POPADAD trial included 1276 patients aged 40 or over with type 1 or type 2 diabetes. 62 Patients with an ankle brachial pressure index less than 1.00 and no symptomatic cardiovascular disease were included. Following a randomised, double blind, 2×2 factorial, placebo controlled design, patients received either 100 mg aspirin tablet plus antioxidant capsule (n = 320), aspirin tablet plus placebo capsule (n = 318), placebo tablet plus antioxidant capsule (n = 320), or placebo tablet plus placebo capsule (n = 318). 62
No evidence was found of any interaction between aspirin and antioxidant. After an average of about 6 years of treatment and follow-up, 116 of 638 primary events occurred in the aspirin groups compared with 117 of 638 in the placebo groups (18.2% vs 18.3%): hazard ratio 0.98 (95% confidence interval 0.76 to 1.26). 62 Therefore, the authors concluded that POPADAD did not provide evidence to support the administration of aspirin as well as antioxidants in order to prevent cardiovascular events and mortality in diabetic patients. 62
POPADAD, however, was also criticized for a lack of statistical power.65,67 In the study, the annual CV event rate observed was 2.9%, compared to an event rate of 8%, which had been expected. 62 The 95% confidence limits for the effect of aspirin (0.76 to 1.26) include a possible 24% reduction in vascular events. 67 In addition, the reported cumulative withdrawal rate from trial medication of about 50% in 5 years 62 may also have impaired the statistical power. 65 In view of the limitations of the study, it has been suggested that primary prevention in diabetes with aspirin should not lead to a discontinuation of aspirin administration in diabetic patients. 69
Ongoing studies
ASCEND (A Study of Cardiovascular Events in Diabetes) is an ongoing trial involving 15,000 diabetic patients, which analyses whether low-dose, EC aspirin (with or without omega-3 fatty acids) is able to reduce the risk of CVD events. In the study, diabetic patients without peripheral artery disease are included. ASCEND and other ongoing studies such as ACCEPT-D (Aspirin and Simvastatin Combination for Cardiovascular Events Prevention Trial in Diabetes) or ASPREE (ASPirin in Reducing Events in the Elderly) will create further evidence. 69
Meta-analyses
Several meta-analyses have focussed on primary prevention of CV events with aspirin in diabetic people. A meta-analysis of 195 randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients conducted by the Antithrombotic Trialists’ Collaboration (ATC) incorporated 9 trials. 70 In 71,912 high risk patients assigned to antiplatelet therapy 7705 (10.7%) serious vascular events occurred in the aspirin group compared to 9502 events (13.2%) in the control group (n = 72,139; P < 0.0001). 70 In the subgroup of diabetic patients with antiplatelet therapy (n = 2568) 403 (15.7%) serious vascular events occurred compared to 426 (16.7%) events in diabetic patients without antiplatelet therapy (n = 2558). 70 It was concluded that the risk reduction in patients with diabetes (7%) was smaller as compared to the entire group (22%). 70 Aspirin, however, was suggested to be effective for primary prevention of vascular events in diabetic patients. 70
Six more recent meta-analyses on primary prevention of CV events with aspirin in diabetic people included data of 10 trials (Table 2).
Studies included in the six more recent meta-analyses.
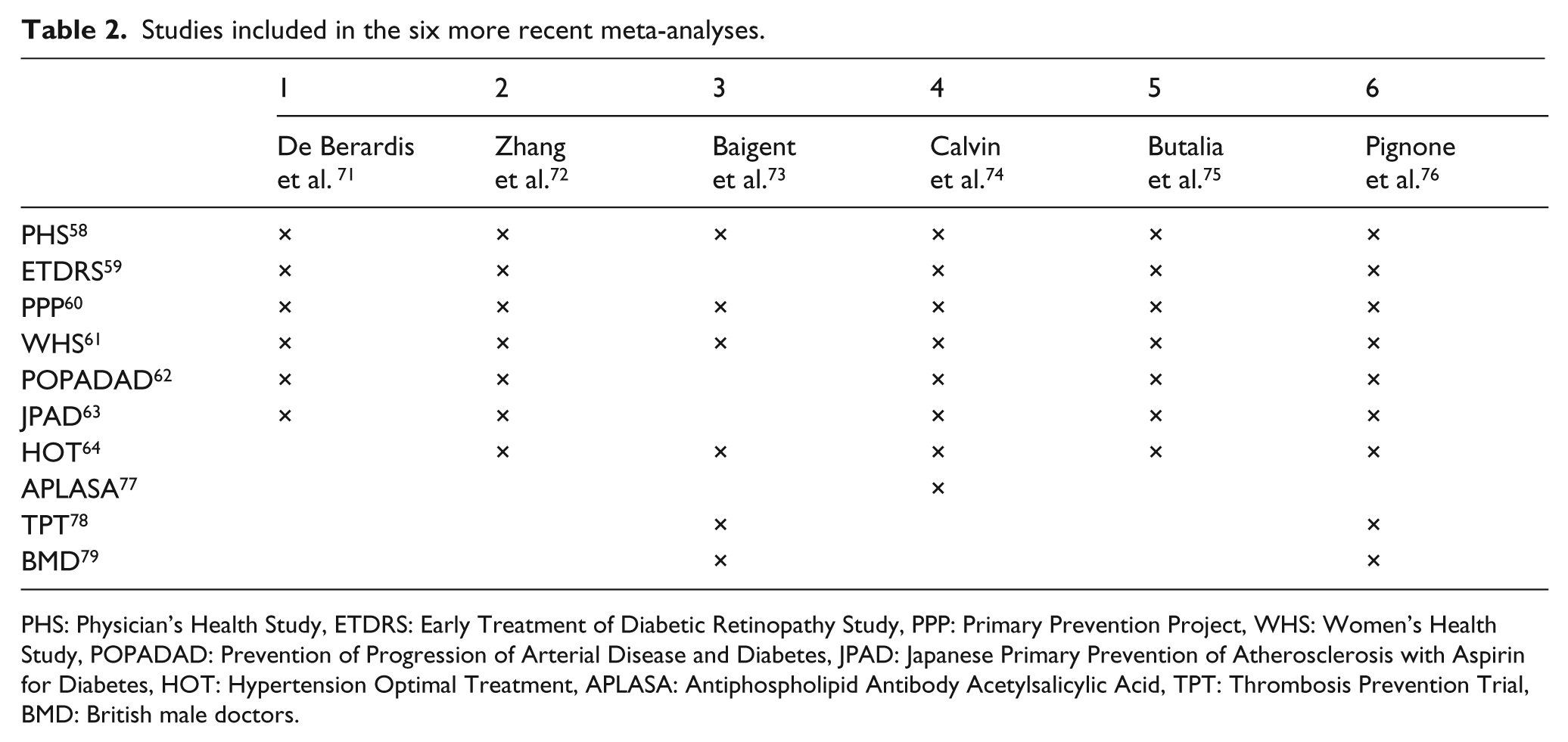
PHS: Physician’s Health Study, ETDRS: Early Treatment of Diabetic Retinopathy Study, PPP: Primary Prevention Project, WHS: Women’s Health Study, POPADAD: Prevention of Progression of Arterial Disease and Diabetes, JPAD: Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes, HOT: Hypertension Optimal Treatment, APLASA: Antiphospholipid Antibody Acetylsalicylic Acid, TPT: Thrombosis Prevention Trial, BMD: British male doctors.
A meta-analysis of 6 studies (Table 2) with 10,117 diabetic patients did not find a clear benefit of aspirin in the primary prevention of major CV events (RR 0.90; 95% CI 0.81–1.00) or CV mortality (0.94; 0.72–1.23) in people with diabetes. 71 Similarly, no significant reduction of all-cause mortality (0.93; 0.82–1.05) could be demonstrated. 71 A subgroup analysis by sex, however, found the risk of myocardial infarction was reduced by 43% in men as compared to no benefit in women. 71
11,618 patients with diabetes were included in a meta-analysis of 7 trials (Table 2). 72 The study found aspirin therapy to be associated with a non-significant reduction (RR 0.92) in major cardiovascular events (MACE). 72 The risks for all-cause mortality (RR 0.95), cardiovascular mortality (RR 0.95), stroke (RR 0.83), and myocardial infarction (RR 0.85) were shown to be reduced non-significantly. 72 The risk of major bleeding was not found to be significantly increased. 72 The risk of MI was reduced in men but not in women, and the risk of stroke in women but not in men. 72
The ATC’s meta-analysis included 6 primary prevention studies (Table 2) representing 95,000 individuals. 73 Aspirin administration was associated with an 18% proportional reduction in major coronary events (0.28 vs 0.34% per year) which mainly derived from a 23% proportional reduction (0.18 vs 0.23% per year). 73 The outcome did not depend significantly on CV risk factors such as sex, hypertension, smoking or diabetes. 73 There was no clear reduction in mortality from coronary heart disease (0.11 vs 0.12% per year). 73 Due to no significant effects on fatal stroke, fatal coronary heart disease, and other vascular causes of death, no significant reduction in overall-mortality (RR 0.97) could be demonstrated. 73 On the other hand, usage of aspirin is reported to increase the rate of major gastrointestinal and extracranial bleedings (0.10 vs 0.07% per year). 73
Another meta-analysis included 8 primary prevention trials (Table 2). 74 Overall, the included trials were reported to be of high methodological quality. 74 The pooled relative risk levels in diabetic patients treated with aspirin compared to patients without diabetes were 0.97 vs 0.87 (mortality), 0.86 vs 0.72 (myocardial infarction), and 0.62 vs 0.89 (ischemic stroke). 74 The risk reduction in patients with diabetes, therefore, is reported to remain non-significant. A treatment benefit with regard to mortality (13%), myocardial infarction (33%), and ischemic stroke (69%) was, however, not excluded. 74 The authors found the effect of aspirin among patients with diabetes not to be significantly different from patients without diabetes and interpret their findings as providing imprecise evidence for administration of aspirin in diabetic patients without a history of CV events. 74
A recently published systematic review and meta-analysis included 11,618 patients from 7 studies (Table 2). 75 According to other meta-analyses addressing the same clinical studies, the authors found the relative risk of major cardiovascular effects to be reduced by 9% in diabetic patients treated with aspirin; rates of haemorrhagic and gastrointestinal events were shown to be enhanced. All these findings did not meet statistical significance. 75 They reported a 1.09% absolute risk reduction of major cardiovascular effects by aspirin with a required number to treat of 92 to prevent one major cardiovascular event. The risk/benefit balance was estimated to be 6 (2–8) with a trend towards a more favourable balance with increasing baseline risk. Thus, for every 10,000 patients using aspirin, circa 109 major cardiovascular effects may be prevented at the expense of 19 major bleedings. 75
In view of questions raised by recent publications, an expert consensus document convened by the American Diabetes Association (ADA), the American Heart Association (AHA), and the American College of Cardiology Foundation (ACCF) reviewed the available evidence in order to reconcile the results and to draft updated recommendations (see also ‘Guidelines and expert recommendations’). 76 The group performed new meta-analysis with updated data from 9 studies (Table 2) including data relating to 11,787 people with diabetes. 76 Aspirin use was analysed to be associated with a non-significant decrease (RR 0.91) in risk of non-fatal and fatal myocardial infarction, and a non-significant decrease (RR 0.90) in risk of stroke. 76 The key findings show aspirin to produce a modest-sized reduction in stroke and myocardial infarction. 76 Current evidence, however, is reported to be not conclusive due to too few events in the available trials. 76
It needs to be considered that data on the potential benefit of aspirin in primary prevention trials might be counteracted by the fact that diabetes may be associated with decreased rates of responsiveness to aspirin.39–42,80
In general, methodological limitations, e.g. in JPAD and POPADAD, might also have blurred the results to some extent. Ongoing studies like ASCEND, ACCEPT-D and ASPREE will further contribute to defining the role of aspirin in primary prevention of CVD. 14
Guidelines and expert recommendations
The recommendations of the United States (US) Preventive Services Task Force for aspirin use in primary prevention were updated in 2009. It is recommended to encourage aspirin use for primary prevention in men aged 45 to 79 years and women aged 55 to 79 years, but not in younger adults.81,82 The recommendations do not differ for diabetic and nondiabetic patients.81,82
An expert group convened by the ADA, the American Heart Association (AHA), and the American College of Cardiology Foundation (ACCF) recommended: 76
– Low-dose aspirin use (75–162 mg daily) for primary prevention is reasonable in adult patients at a CVD risk above 10% over 10 years who are not at increased risk for bleeding. This recommendation should particularly apply to most men over 50 years and women over 60 years who have at least one of the following major risk factors: smoking, hypertension, dyslipidemia, family history of premature CVD, or albuminuria.
– Aspirin use for CVD prevention is not advisable in diabetic adults at low CVD risk: men < 50 years, women < 60 years, no major additional risk factor, 10-year CVD risk < 5%.
– In diabetic patients at intermediate CVD risk, low-dose aspirin might be considered until further research is performed.
The expert group postulates an accurate CV risk assessment to be a substantial part of the considerations concerning aspirin use for primary prevention in patients with diabetes. 76 The authors give as useful examples the UKPDS Risk Engine, 83 the Atherosclerosis Risk in Communities (ARIC) CHD Risk Calculator, 84 and the ADA Risk Assessment Tool Diabetes Personal Health Decisions (PHD). 85 Due to the fact that many patients acquire additional risk factors over time, regular re-assessment is advisable. 76
Secondary prevention of CVD in diabetes with aspirin
In secondary prevention of CV events in patients with coronary or cerebrovascular disease the use of aspirin is well established and supported by solid evidence.70,86 Aspirin is reported to decrease significantly the risk of future events in patients with previous myocardial infarction, stroke or transient cerebral ischemia.70,86
Aspirin has been shown to be protective in patients at high risk for cardiovascular disease, including those with diabetes, in two large meta-analyses of major secondary prevention trials by the ATC.70,86
The first analysis published in 1994 included 145 trials involving 70,000 participants at high CV risk that were available in 1990. A highly significant (2P < 0.000001) proportional reduction in vascular events of about 25% is reported in each of the four high risk categories: prior history of myocardial infarction, suspected or definite acute myocardial infarction, prior history of stroke or transient ischemic attack, and other evidence of vascular disease or some condition associated with an increased risk of occlusive disease. 86
The meta-analysis included 29 trials with about 47,000 patients which provided additional data concerning age, sex, blood pressure, and glycaemic status of the high risk patients. 86 Antiplatelet therapy showed significant benefits in middle age and old age, in men and women, in hypertensive and normotensive patients, and in diabetic and nondiabetic patients. In more than 4500 diabetic patients antiplatelet therapy proved to reduce the incidence of vascular events from 23.5% (control group) to 19.3% (P < 0.01). 86 In the approximately 42,000 nondiabetic patients, the incidence was reduced from 17.2 to 13.7% (P < 0.00001). Data is consistent with an overall risk reduction of 38 ± 12 vascular events per 1000 diabetic patients treated (P < 0.02). 87
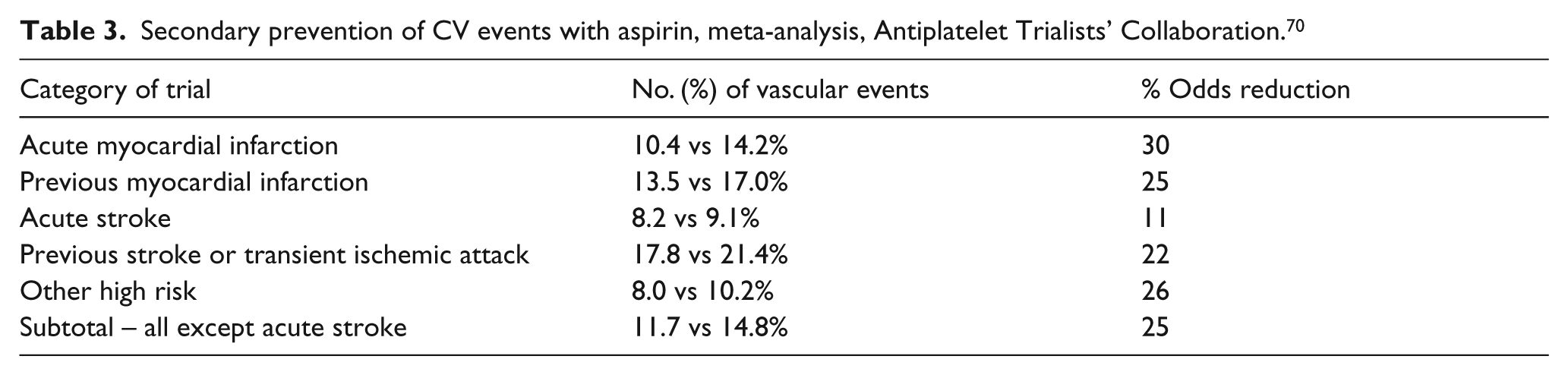
The ATC meta-analysis published in 2002 included 287 studies with 212,000 patients at high CV risk. 70 Antiplatelet therapy was shown to reduce the incidence of vascular events in the major high-risk groups by 23%. 70 Lower doses of aspirin (75–150 mg/day) were at least as effective as higher ones for long term use (however, in acute settings an initial loading dose of at least 150 mg may be required). Patients allocated to antiplatelet therapy presented a significant reduction of CV events as compared to the control groups (Table 3). 70
Secondary prevention of CV events with aspirin, meta-analysis, Antiplatelet Trialists’ Collaboration. 70
In general, the use of aspirin for secondary prevention of CV events is well established and supported by solid evidence. 14 In high-risk patients with previous myocardial infarction, stroke or transient cerebral ischemia, aspirin is reported to decrease the risk of future events by more than 20 %. 14
Guidelines and expert recommendations
The ADA recommends the use of aspirin therapy (75–162 mg/day) as a secondary prevention strategy in diabetic men and women with a history of myocardial infarction, vascular bypass procedure, stroke or transient ischemic attack, peripheral vascular disease, claudication, and/or angina. 88
People with aspirin allergy, bleeding tendency, anticoagulant therapy, recent gastrointestinal bleeding, or clinically active hepatic disease are not classified as candidates for aspirin therapy by the ADA.
The use of aspirin as a secondary cardiovascular prevention strategy in patients with diabetes is also recommended by associations (e.g. European Society of Cardiology, European Association for the Study of Diabetes). According to the ‘European guidelines on cardiovascular disease prevention in clinical practice’ lifelong treatment with low dose aspirin (75–150 mg daily) is recommended in all patients with established CVD – including patients with diabetes. 89
Referring to the available evidence the ‘Expert Consensus Document on the Use of Antiplatelet Agents’ suggests daily doses of aspirin (75–100 mg) for the long term prevention of serious vascular events in high-risk patients. 90
Referring to the ATC’s meta-analysis of 1994, the ‘Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary’ recommend aspirin to be given for the same indications and in similar dosages to diabetic and nondiabetic patients. 91
The ‘Global Guideline for Type 2 diabetes’, published by the International Diabetes Federation (IDF), recommends aspirin 75–100 mg daily in people with evidence of CVD or at high risk, based on cardiovascular risk assessment. 92
Perspectives and outlook
The prevention of cardiovascular events, however, is not the only benefit attributed to aspirin use in people with diabetes. There is increasing evidence for aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) to potentially reduce the incidence of colorectal cancer in the general population. This is particularly of interest for type 2 diabetes, which per se is associated with an increased risk of colorectal carcinomas.15–17 This increased risk is suggested to be related also to obesity, physical inactivity, nutrition, and hyperinsulinemia.93–100 Recently, a 20-year follow-up of 5 randomised trials demonstrated that aspirin may have remarkable preventive potential. 101 The follow-up involved four randomised trials of aspirin versus control in primary (Thrombosis Prevention Trial, 102 British Doctors Aspirin Trial 79 ) and secondary prevention (Swedish Aspirin Low Dose Trial, 103 United Kingdom Transient Ischaemic Attack (TIA) Aspirin Trial 104 ) of vascular events and the Dutch TIA Aspirin Trial 105 which examined different doses of aspirin.
In the 4 trials exploring aspirin versus control 391 of 14,033 patients (2.8%) presented with colorectal cancer during a median follow-up of 18.3 years. 101 Administration of aspirin reduced the 20-year risk of colon cancer (HR 0.76 / mortality HR 0.65), but not the rectal cancer risk (0.90 / 0.80).
Conclusion
The role of aspirin in the prevention of CVD in diabetes is increasing and currently being redefined in view of interesting new results. The phenomenon of enhanced platelet turnover in diabetic patients suggests the potential need to adapt the dosage for primary prevention in the future. Results of ongoing studies will further contribute to the role of aspirin in primary prevention of CVD, which is currently based on the individual risk for CVD, as suggested in the guidelines. Studies on primary prevention of CVD with aspirin have been somewhat limited with regard to their study designs.
In a secondary prevention setting, the use of aspirin in diabetic patients in order to prevent cerebrovascular and cardiovascular events is recommended throughout the key guidelines. Results on potential prevention of cancer with aspirin are of growing interest also in view of the per se elevated cancer risk in the diabetic population.
Footnotes
Funding
This work was supported by an unrestricted educational grant from Bayer Pharma AG.
Conflicts of interest
No conflicts of interest have been declared.