
Abstract
Glucose-lowering treatment options are limited for uncontrolled type 2 diabetes mellitus (T2DM) patients with advanced stages of renal impairment (RI). This retrospective analysis evaluated glycaemic efficacy and tolerability of the dipeptidyl peptidase-4 inhibitor linagliptin added to sulphonylurea. Three randomized phase 3 studies (n = 619) including T2DM subjects with moderate or severe RI [estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2] were analysed; only sulphonylurea-treated subjects who received additional linagliptin (n = 58) or placebo (n = 33) were evaluated. Linagliptin provided meaningful placebo-adjusted HbA1c reductions of −0.68% (95% confidence interval: −1.19, −0.17), −1.08% (−2.02, −0.14) and −0.62% (−1.25, 0.01) after 24, 18 and 12 weeks, respectively. There was a similar incidence of overall adverse events (linagliptin: 79.3%, placebo: 75.8%) and hypoglycaemia (linagliptin: 37.9%, placebo: 39.4%). Severe hypoglycaemia was more common with placebo (linagliptin: 1.7%, placebo: 6.1%). These data suggest that linagliptin is a safe and effective glucose-lowering treatment in T2DM patients with moderate-to-severe RI for whom sulphonylurea treatment is no longer sufficient.
Introduction
Moderate-to-severe renal impairment (RI), defined as an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m2, is a frequent complication of type 2 diabetes mellitus (T2DM), occurring in 20%−30% of patients.1,2 Subjects at this advanced stage of RI comprise a difficult-to-treat population for several reasons: chronic kidney disease is frequently accompanied by additional vascular co-morbidities; it is associated with increased risk of hypoglycaemia; 3 and progressive renal dysfunction reduces drug elimination and prolongs exposure to higher drug levels. 4 The increased risk of hypoglycaemia is caused by impaired renal gluconeogenesis and decreased clearance of both insulin and non-insulin hypoglycaemic agents. 5 The prolonged half-life of insulin (endogenous and exogenous) reduces the dose requirement and necessitates adequate monitoring of glucose control.4,6 Furthermore, as most oral hypoglycaemic agents, including metformin, undergo renal excretion and elimination, many such agents are not recommended or are contraindicated in patients with RI.6–8 Thus, only a few agents can be used, often at a reduced dose, and with careful evaluation of renal function. Because of these restrictions, sulphonylureas are often prescribed in those who cannot use metformin, 9 despite the associated disadvantages (e.g. weight gain, 9 risk of hypoglycaemia 10 ). The low treatment cost of sulphonylureas is also likely to influence treatment selection. If glycaemic goals are not achieved or maintained, insulin may be considered the next logical treatment option. However, concerns about weight gain, hypoglycaemia and use of injections may be barriers to its prescription.11,12 Consequently, additional oral treatment alternatives for patients with T2DM and RI are clearly needed.
Linagliptin is an oral, once-daily dipeptidyl peptidase (DPP)-4 inhibitor that, unlike other DPP-4 inhibitors, has a primarily non-renal elimination route, 13 and does not require dose adjustment for any level of impaired renal function. 14 Phase 3 studies have demonstrated the efficacy and safety of linagliptin as monotherapy and in combination with other oral anti-diabetes drugs and/or insulin,15–23 including in patients with severe RI. 23 Comparable study designs and capture of data in the linagliptin phase 3 programme allow the pooling of all data for safety assessments, although differing treatment durations have to be taken into consideration.
The aim of this retrospective analysis was to evaluate the efficacy and safety of linagliptin as an add-on therapy to sulphonylurea in patients with uncontrolled T2DM and moderate or severe RI.
Methods
Study design
This was a post hoc analysis of data for subjects with moderate or severe RI (eGFR < 60 mL/min/1.73 m2) receiving linagliptin or placebo added to existing sulphonylurea treatment, taken from the wider study populations of three phase 3, randomized, double-blind, placebo-controlled trials of linagliptin 5 mg once daily for the treatment of T2DM (ClinicalTrials.gov identifiers for Studies 1, 2 and 3: NCT01084005, NCT00819091, and NCT00800683, respectively), details of which have been published previously.21–23 Treatment regimens were as follows: Study 1, 24 weeks of linagliptin or placebo added to current glucose-lowering medication(s) in elderly patients with T2DM; 21 Study 2, 18 weeks of linagliptin or placebo added to current sulphonylurea therapy; 22 and Study 3, 52 weeks of linagliptin or placebo added to current glucose-lowering medication(s) in patients with T2DM and severe RI. 23 These three studies were selected for analysis as these trials from the linagliptin phase 3 programme had included participants with moderate-to-severe RI and allowed a treatment regimen of linagliptin added to a stable background of sulphonylurea.
Efficacy analyses were based on the primary endpoint of the three parent studies, defined as the mean change from baseline in glycated haemoglobin (HbA1c) after the respective treatment periods (Study 1, 24 weeks; Study 2, 18 weeks; and Study 3, 12 weeks). Fasting plasma glucose (FPG) was assessed as a secondary endpoint. Safety and tolerability were assessed by the incidence of recorded adverse events (AEs).
Statistical analysis
Efficacy was analysed per study, rather than pooled, due to the differences in when the primary endpoint was measured. Analysis of covariance was used, applying a last observation carried forward imputation in the full analysis set (defined as all randomized participants who received at least one dose of study drug and had baseline and at least one post-baseline HbA1c measurement). Safety data were pooled and summarized descriptively in the treated set (defined as all randomized participants who received ≥ 1 dose of study drug).
Results
Ninety-one participants were included in this analysis: of these, 58 received linagliptin and 33 received placebo. Demographics and clinical characteristics of participants at baseline were generally comparable between the two groups (Table 1).
Demographics and clinical characteristics of participants at baseline.
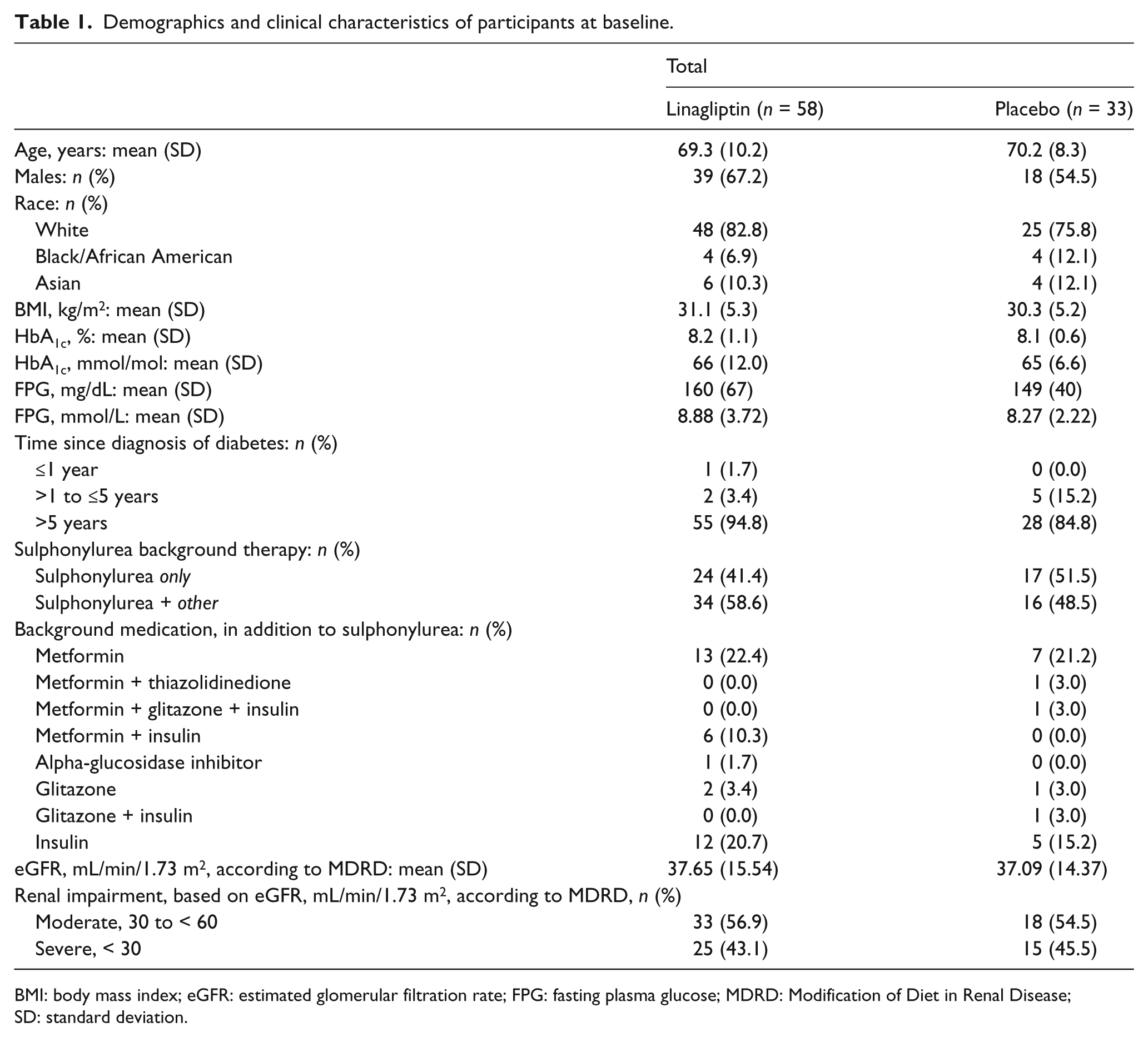
BMI: body mass index; eGFR: estimated glomerular filtration rate; FPG: fasting plasma glucose; MDRD: Modification of Diet in Renal Disease; SD: standard deviation.
Linagliptin treatment resulted in significantly greater adjusted mean decreases in HbA1c compared with placebo in Study 1 [−0.68%; 95% confidence interval (CI): −1.19, −0.17; p = 0.0102] and Study 2 (−1.08%; 95% CI: –2.02, −0.14; p = 0.0271), and a numerically greater decrease in HbA1c in Study 3 (−0.62%; 95% CI: −1.25, 0.01; p = 0.0551) (Figure 1). FPG was numerically decreased with linagliptin compared with placebo in Study 1 [adjusted mean (standard error, SE): −20.9 (14.3) mg/dL; p = 0.1545] and Study 2 [adjusted mean (SE): −16.3 (18.9) mg/dL; p = 0.4069] and was slightly increased versus placebo in Study 3 [adjusted mean (SE): 10.6 (18.6) mg/dL; p = 0.5745].
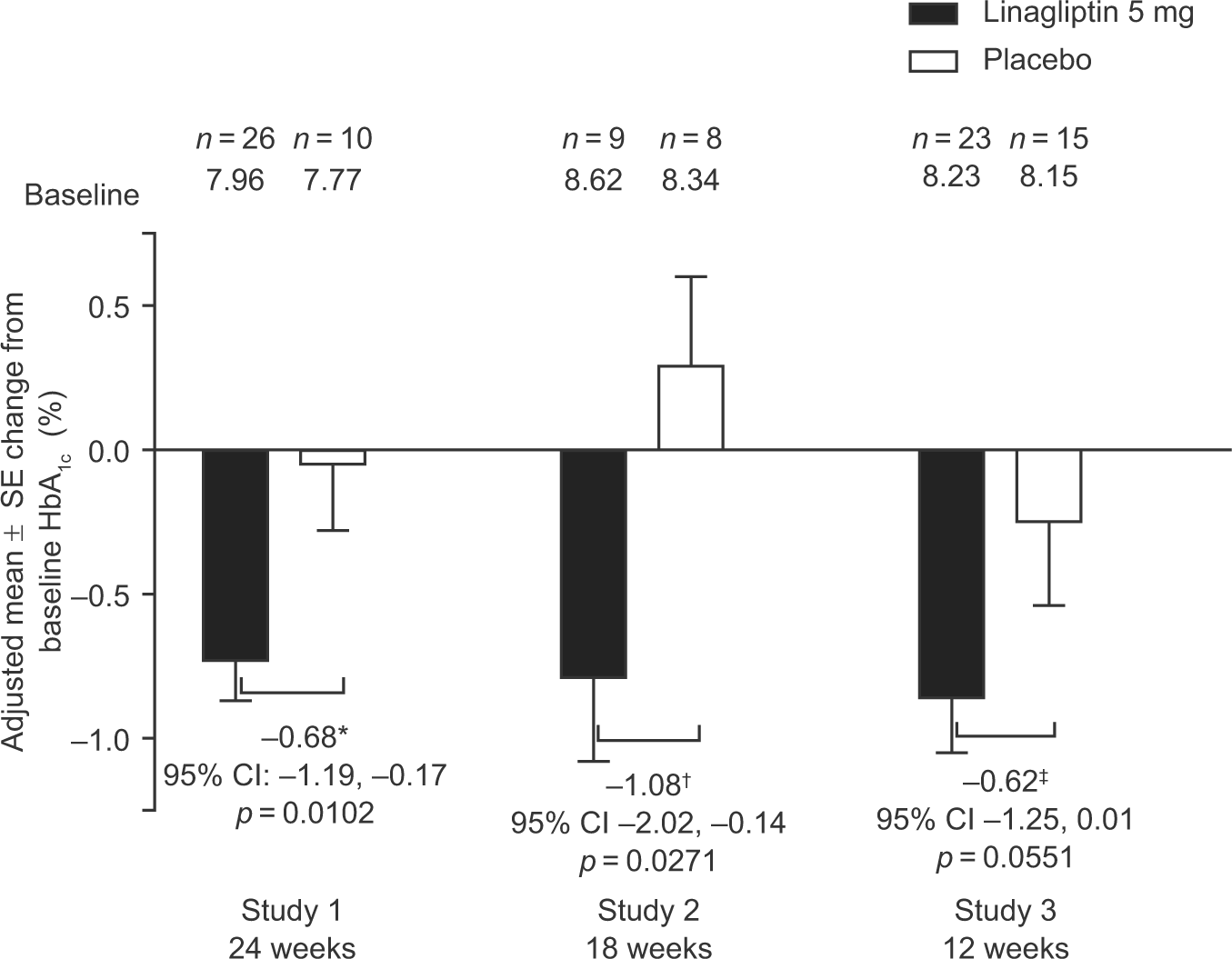
Adjusted mean change in HbA1c from baseline to visit of primary endpoint (full analysis set, last observation carried forward).
The overall incidence rates of participants reporting AEs, drug-related AEs and serious AEs were similar between linagliptin and placebo (Table 2). A similar proportion of participants reported hypoglycaemia with linagliptin (37.9%) and placebo (39.4%) (Figure 2), although fewer participants reported severe hypoglycaemia (requiring assistance) with linagliptin (1.7% vs 6.1% with placebo). Mean change in body weight did not differ significantly between linagliptin and placebo at the end of each study [placebo-adjusted mean change of 1.0 (95% CI: −0.7, 2.7; p = 0.2552), −1.0 (95% CI: −3.4, 1.3; p = 0.3551) and −0.2 kg (95% CI: −4.1, 3.8; p = 0.9319) in Studies 1, 2 and 3, respectively], and no clinically relevant changes were observed.
Incidence of adverse events.
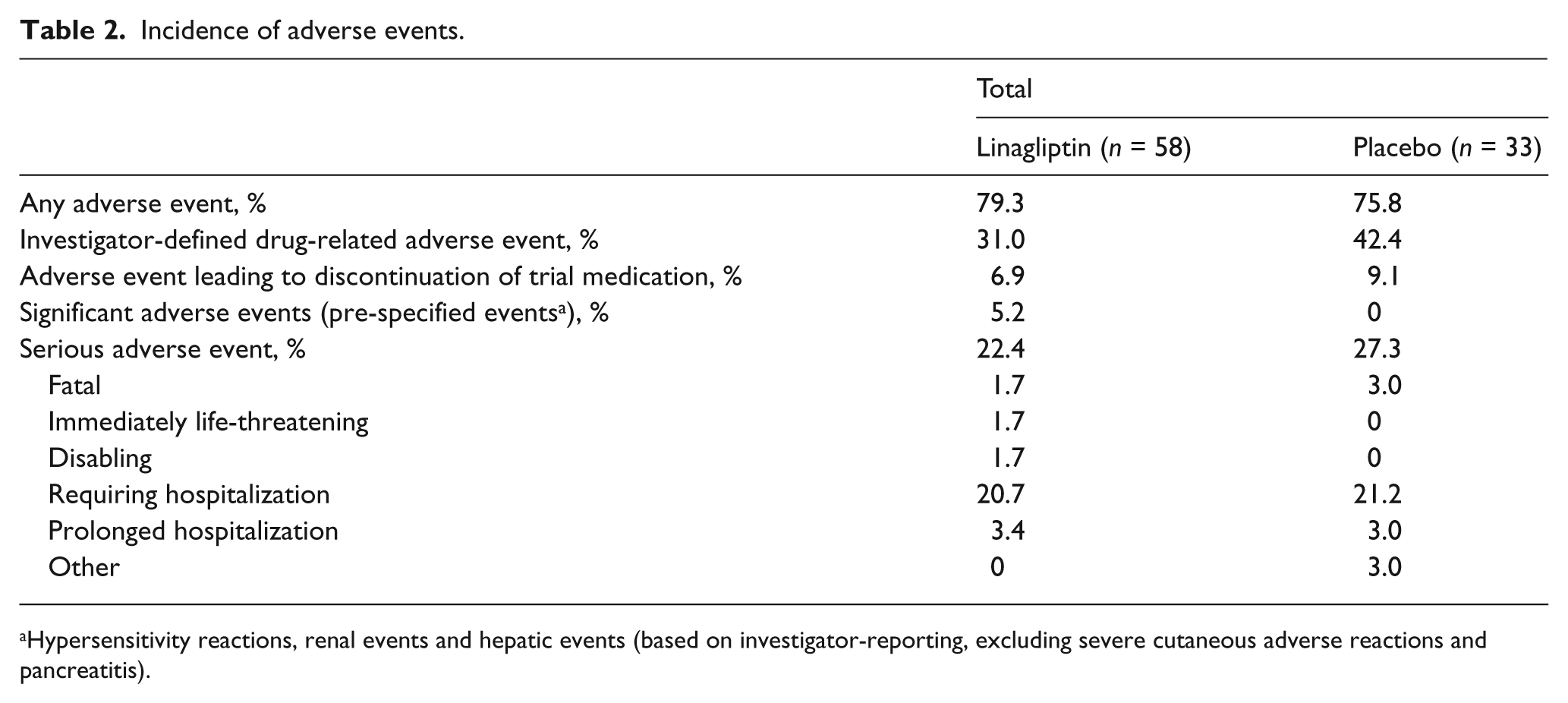
Hypersensitivity reactions, renal events and hepatic events (based on investigator-reporting, excluding severe cutaneous adverse reactions and pancreatitis).
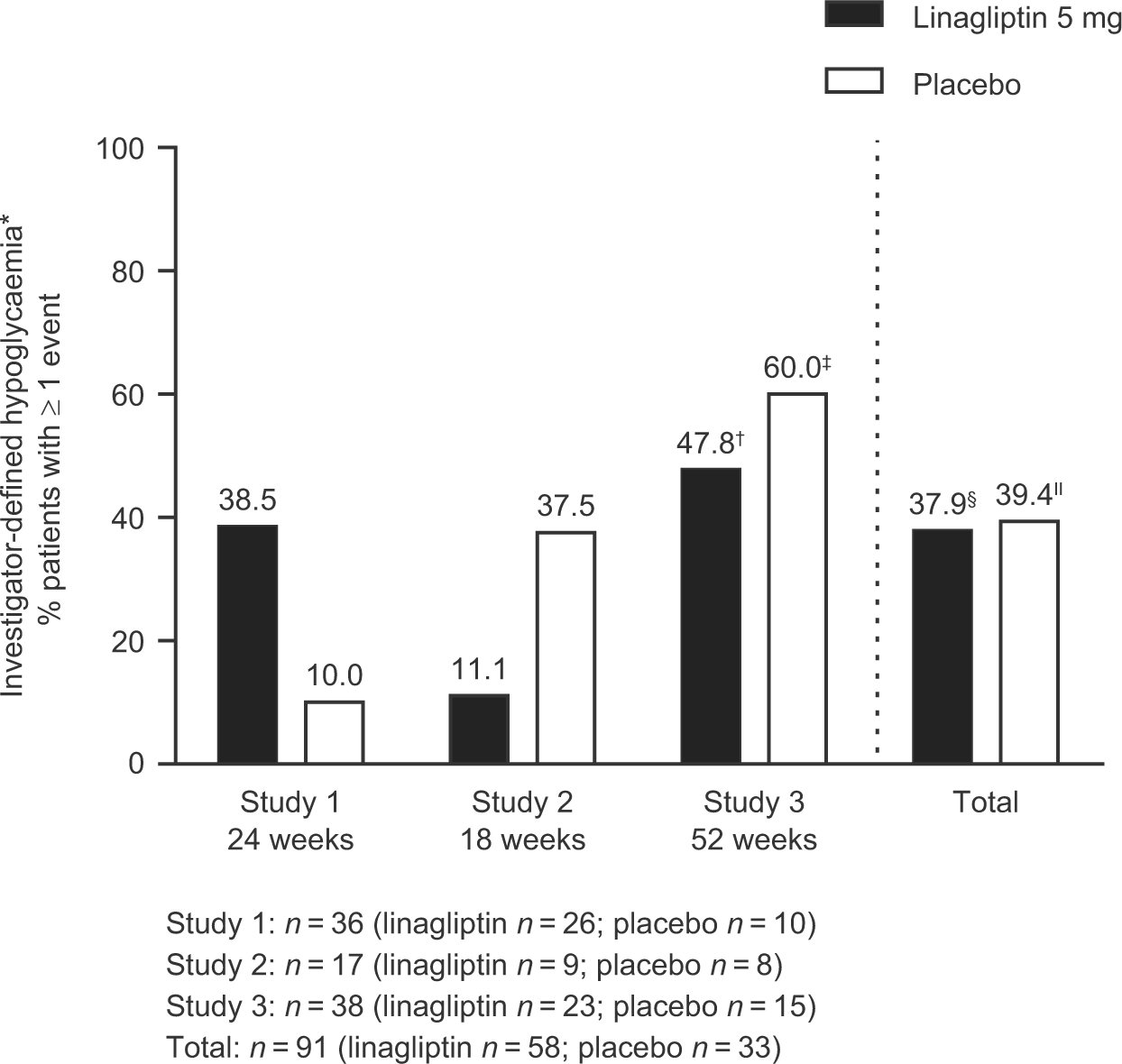
Hypoglycaemia.
Discussion
Linagliptin was well tolerated and provided clinically meaningful improvements in glycaemic control in study participants with T2DM and moderate or severe RI who were not achieving glycaemic control on a regimen including sulphonylurea therapy. Moreover, the incidence of overall hypoglycaemia and severe hypoglycaemia was not increased with linagliptin and body weight remained unchanged. This was observed although the sulphonylurea doses were kept stable in the current studies. From previous studies of DPP-4 inhibitors, it is, however, well known that the combination of this drug class with a sulphonylurea is likely to increase the risk of hypoglycaemia in general. Consequently, the US prescribing information for all available DPP-4 inhibitors indicates that dose reduction of a concomitant sulphonylurea should be considered to reduce the risk of hypoglycaemia.24–27 One possible mechanism for the lack of increased hypoglycaemia when linagliptin is added to sulphonylurea could be due to enhanced counter-regulatory responses to hypoglycaemia with DPP-4 inhibition, that is, improved glucose sensing and responsiveness in pancreatic islet cells, as reported for vildagliptin. 28 This is further supported by a recent analysis of elderly patients (aged > 70 years) receiving linagliptin on top of basal-insulin-based treatment regimens, in which linagliptin was associated with fewer hypoglycaemic events despite a significant improvement in glycaemic control. 29 The observed lack of increase in hypoglycaemia in the elderly and renally impaired population reported here is reassuring, although the relatively small sample size needs to be taken into consideration. Other limitations of this analysis include heterogeneity between the parent studies and the fact that the analysis was carried out post hoc. Consequently, these data should be considered as exploratory only.
The available options for glucose-lowering medication in RI were summarized in a review by Bailey and Day, 6 which states that moderate RI (GFR: 30–< 60 mL/min) may require dose reduction or treatment cessation for metformin, glucagon-like peptide-1 (GLP-1) receptor agonists, some sulphonylureas, and some DPP-4 inhibitors, while in severe RI (GFR: 15–< 30 mL/min), the use of a meglitinide, pioglitazone or certain sulphonylureas may be appropriate with careful consideration of dose and co-morbidities. 6 DPP-4 inhibitors can be used at reduced dose in patients with very low GFRs; 6 however, linagliptin can be used without dose reduction in patients with any degree of renal insufficiency. 24 Insulin can be used at any stage of RI but frequent blood glucose monitoring is needed to enable careful dose titration and prevention of hypoglycaemia. 6
There appears to be very few, if any, published data on the efficacy and tolerability of a DPP-4 inhibitor added to a sulphonylurea in patients with RI. It also seems that few or no dedicated studies are currently ongoing. In general, other treatment options for renally impaired patients not achieving glycaemic control with sulphonylurea monotherapy are restricted and, potentially, further complicated by the use of multiple medications to treat the frequent presence of cardiovascular and other co-morbidities, particularly in older patients. Although the sulphonylurea dose can be up-titrated to maximal levels, there is actually little evidence of dose–response for glycaemic efficacy beyond half of the recommended dose; however, there is a significant increase in side effects, mainly hypoglycaemia, particularly in association with RI. The reduced clearance of sulphonylureas in RI and a build-up of active metabolites (e.g. with glyburide) in some patients are additional reasons for not titrating the dose upwards. Furthermore, continuous exposure to higher plasma levels of sulphonylurea impairs therapeutic efficacy, apparently by down-regulating sulphonylurea-receptor activity. 30
The limited range of suitable treatments in RI means that physicians often choose to prescribe sulphonylureas. However, an alternative option is to use agents that are not associated with an increased risk of hypoglycaemia or weight gain. In a 2-year comparative study in T2DM patients inadequately controlled by metformin monotherapy, linagliptin elicited similar glycaemic improvement as the sulphonylurea glimepiride, but with significantly less hypoglycaemia, significantly fewer cardiovascular events and relative weight loss.18,31
In conclusion, the data reported here suggest that linagliptin could be considered as an additional treatment for T2DM patients with moderate-to-severe RI, whose glycaemic control is inadequate with sulphonylureas – a population in which treatment alternatives are scarce.
Footnotes
Declaration of conflicting interests
The authors were fully responsible for all content and editorial decisions, were involved at all stages of manuscript development and approved the final version. The authors have indicated that they have no other conflicts of interest with regard to the content of this article. S.P., D.N., M.v.E. and H.-J.W. are employees of Boehringer Ingelheim.
Funding
This work was initiated and supported by Boehringer Ingelheim, the manufacturer of linagliptin. Boehringer Ingelheim was given the opportunity to check the data used in the manuscript for factual accuracy only. J.B.M. has received consultancy and speaker fees from Boehringer Ingelheim. A.H.B. has received honoraria for lectures and advisory work from Boehringer Ingelheim. A.J.L. has received honoraria for attending meetings, consultancy fees, speaker fees and/or travel grants from Boehringer Ingelheim. Medical writing assistance, supported financially by Boehringer Ingelheim, was provided by Debra Brocksmith, MBChB, PhD, of Envision Scientific Solutions.