
Abstract
Diabetic nephropathy (DN) affects an estimated 20%–40% of patients with type 2 diabetes mellitus (T2DM). Key modifiable risk factors for DN are albuminuria, anaemia, dyslipidaemia, hyperglycaemia and hypertension, together with lifestyle factors, such as smoking and obesity. Early detection and treatment of these risk factors can prevent DN or slow its progression, and may even induce remission in some patients. DN is generally preceded by albuminuria, which frequently remains elevated despite treatment in patients with T2DM. Optimal treatment and prevention of DN may require an early, intensive, multifactorial approach, tailored to simultaneously target all modifiable risk factors. Regular monitoring of renal function, including urinary albumin excretion, creatinine clearance and glomerular filtration rate, is critical for following any disease progression and making treatment adjustments. Dipeptidyl peptidase (DPP)-4 inhibitors and sodium-glucose cotransporter 2 (SGLT2) inhibitors lower blood glucose levels without additional risk of hypoglycaemia, and may also reduce albuminuria. Further investigation of the potential renal benefits of DPP-4 and SGLT2 inhibitors is underway.
Introduction
The overall prevalence of diabetes mellitus, of which the vast majority of cases are type 2 diabetes mellitus (T2DM), is expected to increase worldwide from an estimated 382 million in 2013 (8.3% of the adult population) to 592 million by 2035 (10.0%). 1 Diabetic nephropathy (DN), which carries a heavy clinical and economic burden, is present in up to 40% of patients with T2DM. 2
Key modifiable risk factors for DN include hypertension, hyperglycaemia, dyslipidaemia, anaemia, albuminuria and lifestyle factors such as obesity and smoking. 3 The early identification of key risk factors and prompt therapeutic intervention can potentially prevent or slow the decline in renal function in patients with T2DM. 4
The primary aim of this review article is to discuss the current understanding of the association between T2DM and renal impairment (RI), and to review the management of risk factors for DN. A further aim is to examine the potential for improved prevention and treatment of DN, including the use of drugs that provide direct protection from diabetes-related end-organ damage in addition to risk factor control.
Association of DN and T2DM
Chronic kidney disease (CKD) is associated with various risk factors, including cardiovascular disease, obesity and diabetes. Between 1999 and 2004, the prevalence of CKD within the general US population was estimated to be 16.8% (Figure 1); 5 the most recent prevalence estimate for 2007–2012 is 15.0%. 6 CKD is more prevalent in those with diabetes and older patients (Figure 1). 5 Worldwide, the reported prevalence rates vary widely from 2.5% in China to 35.8% in Finland (Table 1). 33
Prevalence of CKD among US adults by disease stage – National Health and Nutrition Examination Survey (NHANES), United States, 1999–2004.
Prevalence of chronic kidney disease (CKD) in population-based studies in Northern/Central America, Europe and Australia/Asia.
MDRD: simplified equation of the Modification of Diet in Renal Disease Study; CG/BSA: Cockcroft–Gault formula adjusted by body surface area; NR: not reported.
©2008 Zhang and Rothenbacher; 33 licensee BioMed Central Ltd.
In the United States, an estimated 40% of adults living with T2DM experience some degree of CKD, 34 and 20%–40% of this population presents with DN characterised by macroalbuminuria and a low glomerular filtration rate (GFR). 2 Microalbuminuria precedes DN and has an estimated global prevalence of 39% among those with T2DM. 35 In the Western world, diabetes is the most common cause of end-stage renal disease (ESRD), accounting for 44% of all ESRD patients in the United States. 34
The pathophysiological mechanisms of DN in T2DM are multiple and complex. 36 Early haemodynamic changes are followed by albumin leakage from the glomerular capillaries and structural changes in the kidney. 3 Risk factors such as hyperglycaemia and hypertension activate inflammatory pathways, and patients with a genetic predisposition can progress to advanced-stage nephropathy. 3
There are important distinctions between DN and other renal complications of diabetes. DN is defined as the presence of both persistent macroalbuminuria (albumin ≥300 mg/dL) and reduced GFR. In patients with diabetes, microalbuminuria (albumin = 30–299 mg/dL) alone does not indicate DN, but is associated with endothelial dysfunction, vascular inflammation, coagulation abnormalities, a high rate of non-dipping of nocturnal blood pressure (BP) and increased cardiovascular risk.3,37,38 In contrast, there are many patients with T2DM who have a low GFR in the presence of normal albuminuria levels. 39
Key risk factors for DN in patients with T2DM
Non-modifiable risk factors of decreased renal function include longer diabetes duration, older age and genetic factors. Modifiable risk factors include anaemia, hypertension, hyperglycaemia, dyslipidaemia and albuminuria, as well as lifestyle factors, such as obesity and smoking.4,40 The early detection and treatment of modifiable renal risk factors can prevent or slow the progression of DN, and may even produce remission. 41
Hypertension
Hypertension is a common comorbidity of patients with T2DM,42,43 with elevated BP playing a major role in the development and progression of DN. 4 It is well established that intensive BP control slows the progression of kidney disease in patients with T2DM,4,44 and may even induce remission of renal structural and functional impairment. 4
Hyperglycaemia
Observational studies have established a relationship between hyperglycaemia and the development of microvascular complications. 36 Increasing levels of glycated haemoglobin (HbA1c) are associated with an increased incidence of kidney disease, even in the absence of a diagnosis of diabetes.45,46 Compared with standard glycaemic control, intensive lowering of HbA1c may prevent or slow the progression of kidney disease in patients with T2DM. 47
Dyslipidaemia
Diabetic dyslipidaemia is characterised by high levels of triglycerides and low-density lipoprotein cholesterol, and low levels of high-density lipoprotein cholesterol. In some studies, treatment targeting dyslipidaemia reduced the progression of CKD, 48 improved estimated GFR (eGFR) in patients with T2DM 49 and stabilised kidney function in patients with cardiovascular disease. 50 However, other studies have shown mixed findings regarding whether diabetic dyslipidaemia contributes to kidney disease. 4
Albuminuria
The development of albuminuria is closely associated with the progression of kidney disease in patients with T2DM, even within the range of normoalbuminuria. 4 Zoppini et al. 40 demonstrated that albuminuria was the strongest predictor of annual eGFR decline, with the reduction of albuminuria having emerged as a novel therapeutic goal for renoprotection. 4
A reduction in albuminuria can decrease the risk of renal endpoints in patients with T2DM. 51 For example, it has been shown that for every 50% reduction in proteinuria during the first year, the risk for kidney failure was reduced by 56%. 51 Thus, albuminuria can be effectively lowered with antihypertensive drugs that inhibit the renin–angiotensin–aldosterone system (RAAS), with these renoprotective effects observed at normoalbuminuric, microalbuminuric and overt albuminuria levels.
Anaemia
Reduced haemoglobin levels predict adverse renal outcomes, as was shown in a post hoc analysis of the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) trial. 52 Anaemia frequently occurs early in the course of diabetic kidney disease, even before GFR is severely reduced, perhaps because renal interstitial damage and autonomic neuropathy lead to decreased erythropoietin production from peritubular fibroblasts. 4 Early treatment of anaemia with erythropoietin may delay the onset and slow the progression of microvascular complications, including nephropathy. 53
Obesity
Although the mechanisms are not fully understood, adverse haemodynamic, structural and functional changes have been observed in the kidneys of obese individuals; 54 in those patients with T2DM, obesity contributes to the progression of CKD. 54 Conversely, weight loss reduces macro- and microalbuminuria, and stabilises renal function in various populations, including patients with T2DM. 55 This benefit may in part be due to reduced BP.
Smoking
Smokers with T2DM have an elevated risk of micro- and macroalbuminuria and reduced GFR. 56 Heavy smoking increased the rate of GFR decline by 1.3 mL/min/year after adjusting for other risk factors. 4 Continued smoking exacerbates, whereas cessation ameliorates, the progression of DN. 56
Current management of risk factors for DN
Lifestyle modifications such as dietary changes and weight loss both improve BP, dyslipidaemia and obesity, whereas protein restriction may slow the progression of albuminuria and decline in GFR.42,43
Pharmacotherapy is increasingly important for controlling key risk factors for DN, including hyperglycaemia, hypertension and dyslipidaemia. Although guidelines exist,42,43 goals and treatments should be tailored to the individual patient, taking into consideration demographics, duration of T2DM, life expectancy, degree of CKD, comorbidities, body weight and the presence of other risk factors.
BP control
Aggressive antihypertensive treatment has dramatically improved renal outcomes and survival in patients with T2DM. A BP goal of <140/80 mm Hg is recommended in patients with T2DM, irrespective of kidney disease. 42 Furthermore, BP lowering below these targets may provide additional renoprotection in patients with T2DM.
RAAS inhibitors, such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), have direct renoprotective effects in addition to lowering BP 4 and are recommended as first-line treatments in hypertensive patients with T2DM, regardless of kidney disease.42,43 RAAS inhibition can reduce the early transition to renal complications, 57 and can also protect in later stages, reducing the incidence of ESRD. However, RAAS inhibitors also reduce haemoglobin levels and may, therefore, aggravate anaemia. During RAAS inhibitor treatment, serum creatinine and potassium levels should be monitored to detect the development of acute kidney disease and hyperkalaemia. 42
Glycaemic control
The primary target in glycaemic control is HbA1c, for which treatment goals have been established.42,43,58 Currently available glucose-lowering drug classes include the biguanides (metformin), sulphonylureas, thiazolidinediones, meglitinides, α-glucosidase inhibitors, pramlintide, incretin-based therapy (glucagon-like peptide-1 (GLP-1) analogues, dipeptidyl peptidase (DPP)-4 inhibitors) and sodium-glucose cotransporter 2 (SGLT2) inhibitors. The choice of glucose-lowering therapy is important to balance the benefits of antihyperglycaemic treatment with adverse effects, such as hypoglycaemia and weight gain. Oral glucose-lowering drugs that are eliminated by the kidneys are also a concern in patients with T2DM and CKD. 43
Treatment of diabetic dyslipidaemia
Early treatment of dyslipidaemia may be important because lowering cholesterol has been shown to have little effect in patients with diabetes once DN has reached an advanced stage. 49 Although it is unclear whether dyslipidaemia is a risk factor for the development and/or progression of DN, because of the established cardiovascular benefits of cholesterol lowering, all patients with DN should receive lipid-lowering treatment, 4 with statins recommended as first-line treatment.42,58
Reduction of albuminuria
Several drug strategies decrease the level of urinary albumin excretion in patients with T2DM, with the data being most extensive for RAAS inhibitors. DPP-4 inhibitors may also reduce albuminuria in addition to lowering blood glucose. Evidence suggests that the thiazolidinediones and fenofibrate decrease albuminuria and may therefore have potential renal benefits in DN.59–61
The potential for improved prevention and treatment of DN
Early, intensive and multifactorial management of DN risk and progression
The early identification of modifiable risk factors for DN is important for prompt therapeutic intervention. Early achievement of multiple risk factor targets has been shown to delay DN. Thus, patients should receive early, intensive and multifactorial management, targeting all risk factors simultaneously, to prevent or slow the progression of kidney disease.42,43,58
Direct protection from DN
New drug interventions should also offer direct protection from DN and other diabetes-related end-organ damage. This has been partly achieved with RAAS inhibitors, which have renoprotective effects that are independent of their BP-lowering effects.42,43 However, albuminuria frequently remains elevated, and DN remains a major health problem, with many patients with T2DM still progressing to ESRD. 34 Because current efforts to prevent and treat DN have limited success, more effective treatment strategies are urgently needed.
GLP-1 analogues and DPP-4 inhibitors
Incretin-based therapies for the treatment of hyperglycaemia include the injectable GLP-1 receptor agonists and the orally active DPP-4 inhibitors, both of which stimulate insulin secretion and inhibit glucagon secretion in a glucose-dependent manner. Among the substrates of DPP-4 are peptide hormones such as B-type natriuretic peptides, neuropeptide Y, peptide YY and stromal cell-derived factor-1α (Figure 2),62,63 which are thought to be responsible for the cardio-renal effects potentially beneficial for patients with T2DM.63,64
DPP-4 effects beyond glucose lowering.
The secretion of native GLP-1 is impaired in patients with T2DM. 65 Injectable GLP-1 analogues, including exenatide and liraglutide, improve glycaemic control and are associated with weight loss. 66 Exenatide is predominantly excreted via the kidney, but has an acceptable tolerability profile in patients with mild CKD and requires no dose adjustment in this patient group. Dose escalation of exenatide in patients with moderate RI should proceed with caution, and its use in patients with severe kidney disease is not recommended. 67 Liraglutide is not exclusively metabolised by the kidney and can be used in patients with mild RI without dose adjustment. 67 However, studies assessing GLP-1 efficacy in patients with T2DM and moderate-to-severe RI are lacking.
Because of the favourable tolerability profile of DPP-4 inhibitors (weight neutral and a low incidence of hypoglycaemia) and their potential to preserve β-cell function, these drugs present a unique option in oral glucose-lowering therapy. Currently available DPP-4 inhibitors include sitagliptin, vildagliptin, saxagliptin, alogliptin and linagliptin, and preclinical studies have reported effects on myocardial infarction, and acute and chronic renal failure. 63 One of the key differentiators of the available DPP-4 inhibitors is the route of elimination, with sitagliptin, vildagliptin, saxagliptin and alogliptin displaying a variable renal elimination route ranging from 75% for saxagliptin to 87% for sitagliptin. 67 In comparison, less than 6% of linagliptin is excreted renally at an oral dosage of 5 mg/day. 68 In clinical studies, all DPP-4 inhibitors were well tolerated in patients with CKD, 67 with no dose adjustment needed in patients with mild RI. However, dose adjustments are needed in patients with moderate or severe RI for all DPP-4 inhibitors with the exception of linagliptin (Figure 3).
Antidiabetes therapy in patients with CKD.
Clinical evidence regarding the renal benefits of incretin-based therapies is limited. Liraglutide was not associated with any changes in renal function after 24 weeks in patients with DN (eGFR <60 mL/min). 70 Sitagliptin, saxagliptin and linagliptin may have the potential for beneficial renal effects. Sitagliptin (50 mg/day) reduced urinary albumin-to-creatinine ratio (UACR: −20.6 mg/g creatinine) after 24 weeks in patients with T2DM; the effect was observed in patients with normo-, micro- and macroalbuminuria. 71 In the recently completed Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus–Thrombolysis in Myocardial Infarction (SAVOR-TIMI) 53 trial, saxagliptin reduced the development and progression of microalbuminuria compared with placebo. 72 In a pooled analysis of four 24-week, randomised, placebo-controlled trials of patients with T2DM and prevalent albuminuria (UACR: 30–3000 mg/g creatinine) while receiving stable doses of RAAS inhibitors, linagliptin reduced UACR by 32% versus 6% with placebo, with a between-group difference versus placebo of 28%. 73 Finally, in a recent meta-analysis of 5466 patients with T2DM, treatment with linagliptin was not associated with an increase in renal risk and was associated with a significant reduction of clinically relevant renal safety events. 74 The renal effects of linagliptin are currently being investigated in the MARLINA-T2D™ (Efficacy, Safety & Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with LINAgliptin) trial (ClinicalTrials.gov Identifier: NCT01792518). The CARMELINA® (CArdiovascular Safety & Renal Microvascular outcomE study with LINAgliptin) trial (NCT01897532) has also recently been initiated, and is enrolling patients with T2DM and renal dysfunction.
SGLT2 inhibitors
SGLT2 inhibitors, a new class of oral antidiabetes therapy, selectively target the SGLT2 protein and prevent renal sodium and glucose reabsorption in the kidney, a process known to be involved in the development of DN. 75 Blocking the activity of SGLT2, which is almost exclusively expressed in the S1 segment of the renal proximal tubule, 76 leads to substantial glucosuria and a reduction in plasma glucose levels. 77 Since SGLT2 inhibitors do not stimulate insulin secretion, improvements in glycaemic control are seen without increasing the risk for hypoglycaemia. 77 Nonglycaemic benefits of SGLT2 inhibitors include reductions in body weight and BP.77,78 Recently, two head-to-head studies have demonstrated some benefits of SGLT2 inhibitors versus the DPP-4 inhibitor sitagliptin.79,80 When canagliflozin (300 mg daily) or sitagliptin (100 mg daily) were administered to patients with T2DM inadequately controlled with metformin plus sulphonylurea, 80 greater reductions in HbA1c (difference after 1 year, 0.37%), fasting plasma glucose (FPG; difference, 26.5 mg/dL), body weight (difference, 2.4 kg) and systolic BP (difference, 6 mm Hg) were observed with canagliflozin compared with sitagliptin (p < 0.001). A comparison of monotherapy 79 with either empagliflozin (10 or 25 mg daily) and sitagliptin (100 mg daily) showed slightly better glucose control with empagliflozin 25 mg versus sitagliptin at 24 weeks (reduction in HbA1c: −0.85% vs −0.73%; p < 0.0001), and reductions in body weight (difference, 2.67 kg) and systolic BP (difference, 4.2 mm Hg). Head-to-head long-term studies are needed to evaluate whether these differences will have an impact on cardiovascular and renal endpoints.
The primary route of elimination of the SGLT2 inhibitor canagliflozin is in faeces (approximately 50%), whereas dapagliflozin is primarily excreted in urine (75%).81,82 Approximately 20% of empagliflozin is excreted unchanged in urine. 83 The glucose-lowering efficacy of SGLT2 inhibitors is dependent on renal function and for the drugs approved at the time of writing, use is currently contraindicated in patients with severely impaired kidney function (eGFR <30 mL/min) or ESRD.81,82 In addition, renal function monitoring is recommended prior to initiating treatment with canagliflozin and dapagliflozin, and periodically thereafter.81,82
Given their mechanism of action, SGLT2 inhibitors may have significant renal effects beyond their glucose-lowering properties.84,85 In patients with T2DM and moderate RI, treatment with canagliflozin (100 or 300 mg for 26 weeks) 86 or dapagliflozin (5 or 10 mg for 104 weeks) 87 showed an initial transient decrease in eGFR which remained relatively stable for the duration of treatment (Figure 4). The effect of treatment with SGLT2 inhibitors in 6 different studies on renal function are summarised in Table 2.
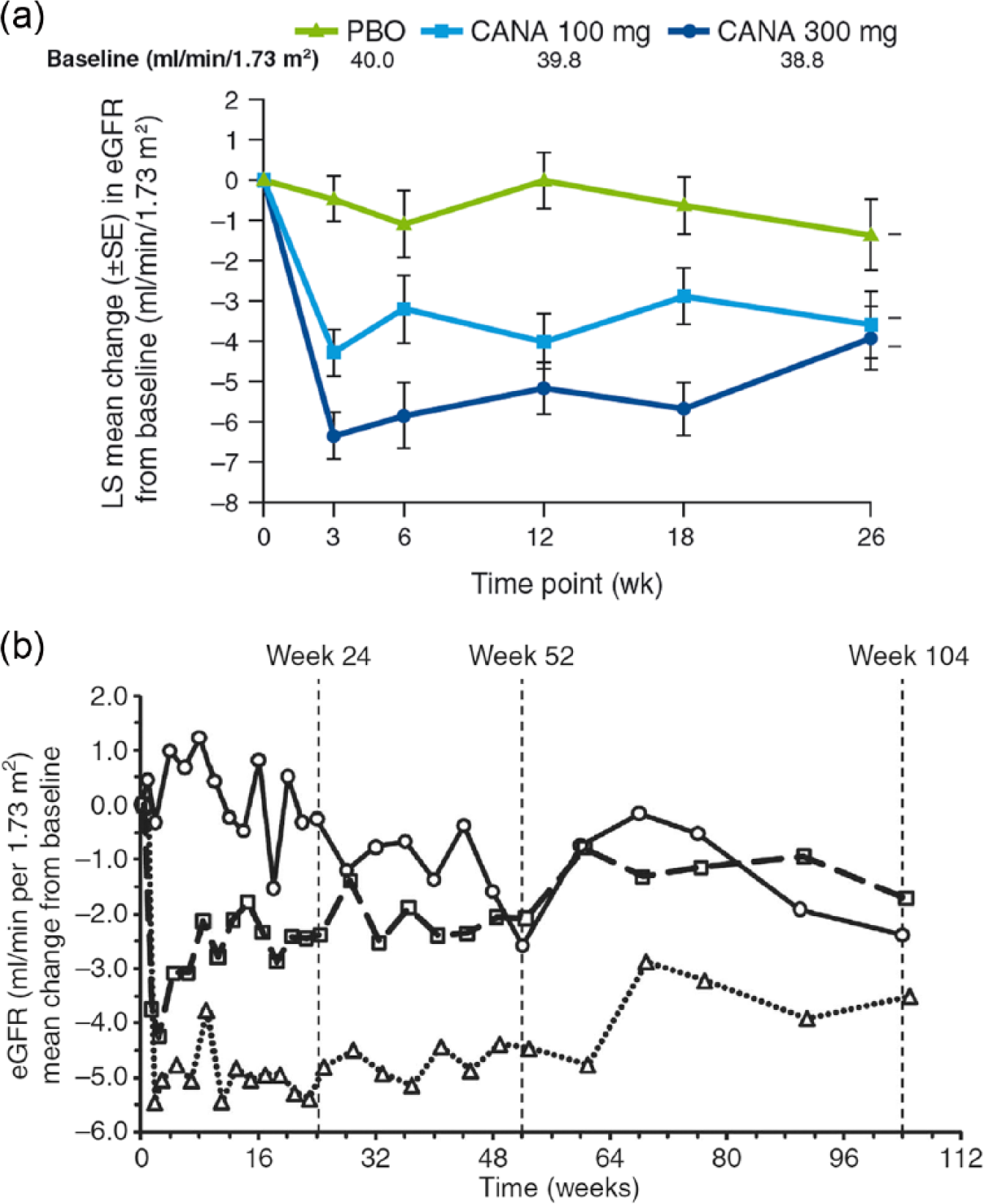
Changes in eGFR over time in T2DM patients with moderate RI treated with (a) canagliflozin and (b) dapagliflozin. Moderate RI = baseline eGFR ≥30 and <50 mL/min/1.73 m2; Moderate RI = baseline eGFR ≥30 and <60 mL/min/1.73 m2. Placebo (circles, solid line), dapagliflozin 5 mg (squares, dashed line) and dapagliflozin 10 mg (triangles, dotted line).
Effects of SGLT2 inhibitors on renal function.
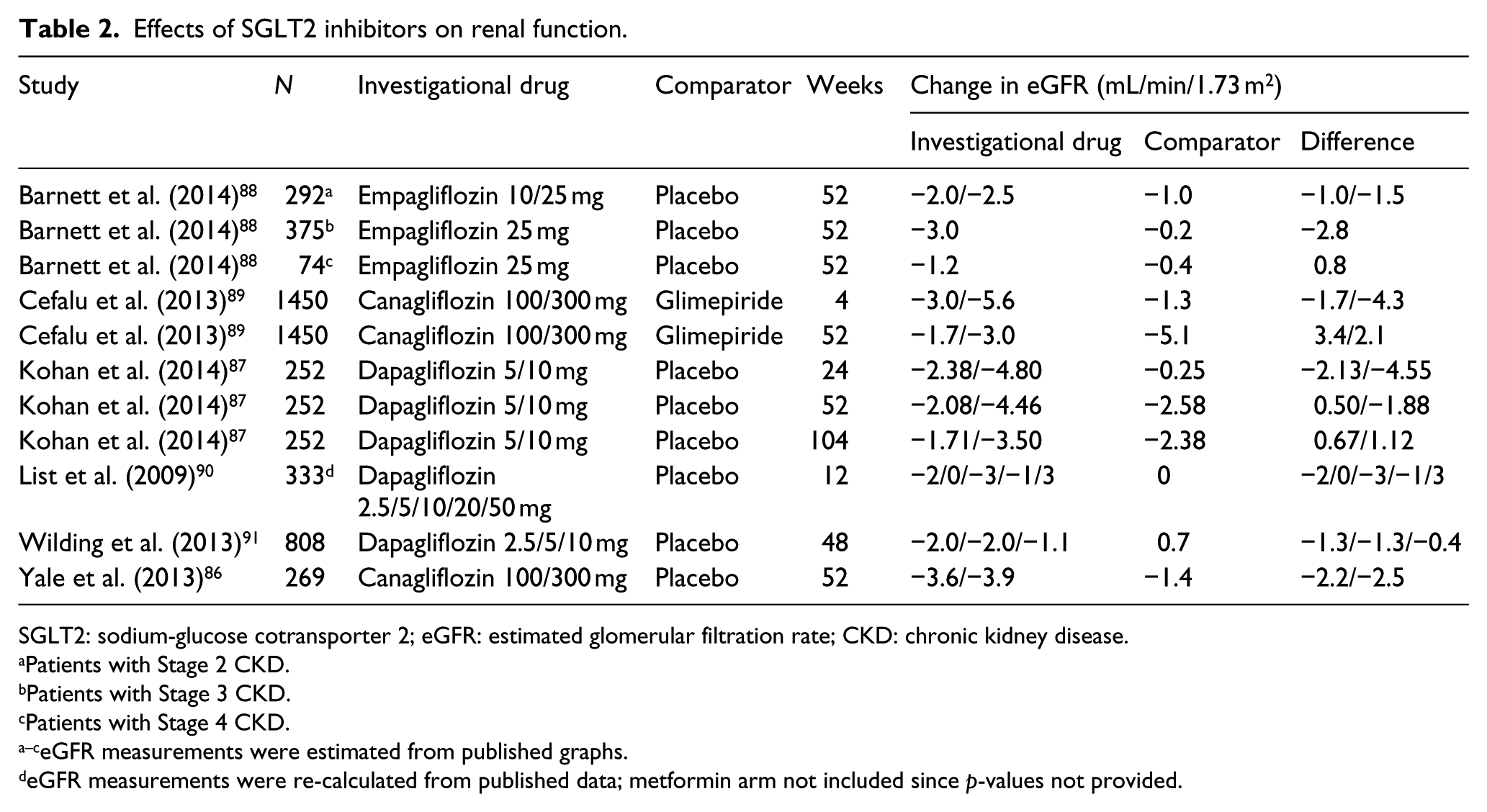
SGLT2: sodium-glucose cotransporter 2; eGFR: estimated glomerular filtration rate; CKD: chronic kidney disease.
Patients with Stage 2 CKD.
Patients with Stage 3 CKD.
Patients with Stage 4 CKD.
eGFR measurements were estimated from published graphs.
eGFR measurements were re-calculated from published data; metformin arm not included since p-values not provided.
In addition to GFR, impact on albuminuria has also been investigated in several SGLT2 studies (Table 3). Canagliflozin 100 and 300 mg were associated with greater decreases in UACR compared with placebo, with median percent reductions of −29.9%, −20.9% and −7.5%. 86 When these data were analysed with regard to their effects on albuminuria progression (normo- to micro-/macroalbuminuria or micro- to macroalbuminuria), the proportion of patients that progressed were 5.1%, 8.3% and 11.8% in the canagliflozin 100 mg, 300 mg and placebo groups, respectively, with odds ratios (95% confidence interval (CI)) of 0.33 (0.08, 1.48) and 0.51 (0.14, 1.91) for the pairwise comparisons of canagliflozin 100 and 300 mg to placebo, respectively. 86 Additional studies analysing UACR changes and progression as part of a cardiovascular safety report for the Food and Drug Administration, showed similar changes (Figure 5) in a larger group of more than 3000 individuals. 92
Effects of SGLT2 inhibitors on albumin excretion rate.
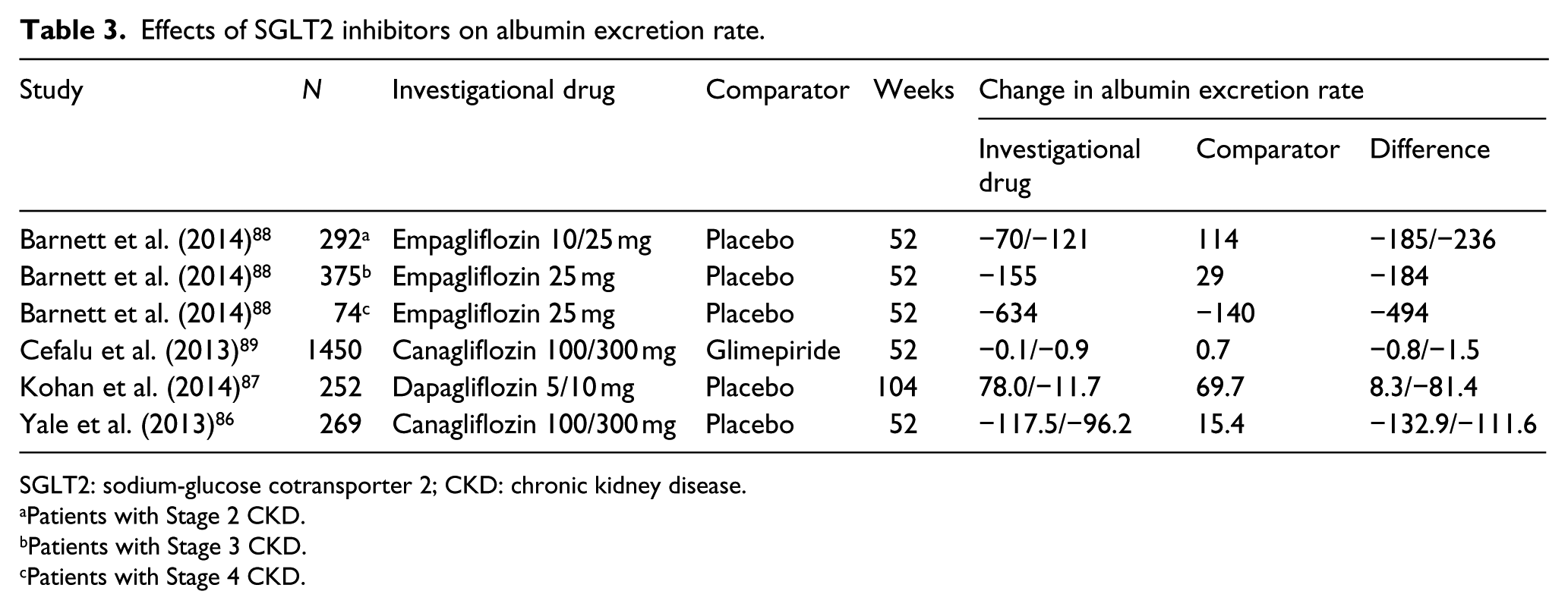
SGLT2: sodium-glucose cotransporter 2; CKD: chronic kidney disease.
Patients with Stage 2 CKD.
Patients with Stage 3 CKD.
Patients with Stage 4 CKD.
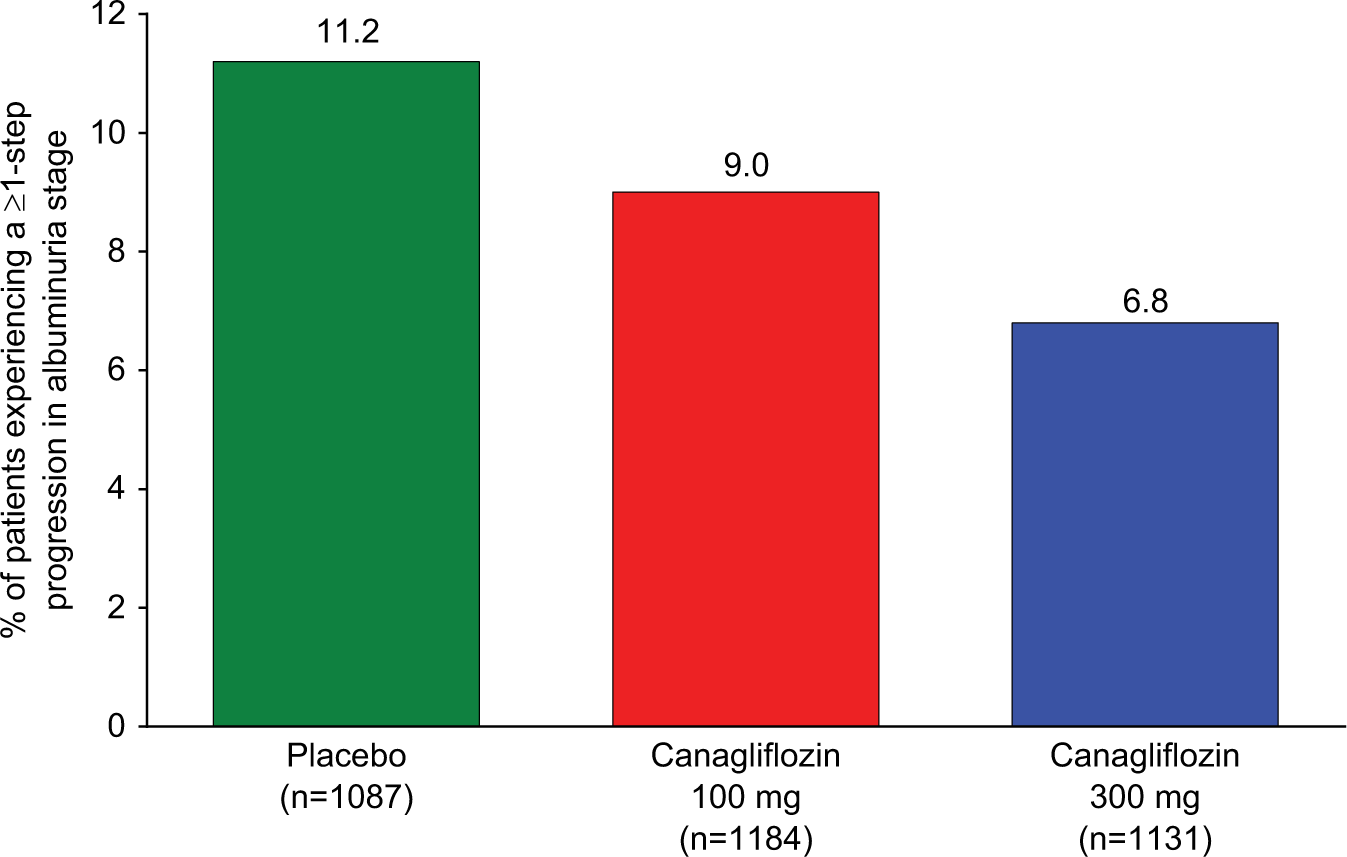
Proportion of participants in canagliflozin cardiovascular safety study in patients with T2DM experiencing a ≥1-step progression in albuminuria stage.
Very recently, similar findings were reported for dapagliflozin in a 104-week study of patients with CKD. 87 Of the 139 patients who completed the study, 96 were treated with dapagliflozin and 43 received placebo. Values of UACR >1800 mg/g during the 104-week treatment period were reported in a higher proportion of patients receiving placebo (13.3%) than in patients receiving dapagliflozin 5 or 10 mg (10.8% and 9.5%, respectively). In shift analyses, UACR was characterised according to one of three pre-specified categories: 0 to <30 mg/g (normoalbuminuria), 30 to <300 mg/g (microalbuminuria), or ≥300 mg/g (macroalbuminuria). Among dapagliflozin-treated patients, albuminuria shifted to a lower category in 38 patients (18 from microalbuminuria to normoalbuminuria, 19 from macroalbuminuria to microalbuminuria, and 1 from macroalbuminuria to normoalbuminuria) and shifted to a higher category in 18 patients; in patients receiving placebo, 9 shifted to a lower category and 12 to a higher one. 87
In a recent clinical trial of empagliflozin (10 or 25 mg for 52 weeks), small decreases in eGFR and albuminuria were also shown in T2DM patients with mild or moderate RI. 88 UACR improved with empagliflozin compared with placebo at Week 52 in patients with Stage 2 CKD (empagliflozin 25 mg: adjusted mean difference, −235.86 (95% CI: −442.85, −28.86), p = 0.0257) and Stage 3 CKD (−183.78 (95% CI: −305.18, −62.38), p = 0.0031). In patients with Stage 3 CKD, fewer patients on empagliflozin 25 mg than placebo shifted from no albuminuria to microalbuminuria, or from microalbuminuria to macroalbuminuria, at end of treatment (12.2% with empagliflozin vs 22.2% with placebo, and 2.0% with empagliflozin vs 11.4% with placebo, respectively). Remarkably, more patients with Stage 3 CKD on empagliflozin 25 mg improved from macroalbuminuria to microalbuminuria, or from microalbuminuria to no albuminuria, at end of treatment (32.6% with empagliflozin vs 8.6% with placebo, and 27.5% with empagliflozin vs 21.4% with placebo, respectively). These changes reversed (with levels returning to baseline values) 3 weeks after the end of treatment, indicating no long-term damage. In nonclinical studies, empagliflozin decreased the renal expression of molecular markers of kidney growth, fibrosis and inflammation,93,94 and intriguingly, in a small study of patients with type 1 diabetes, empagliflozin attenuated hyperfiltration, suggesting the potential to reduce the risk of DN. 95 Further studies are clearly needed to determine if these effects translate into renal benefits in clinical practice. For example, the renal effects of empagliflozin are being assessed as a pre-specified secondary endpoint in the EMPA-REG OUTCOME™ (Empagliflozin Cardiovascular Outcome) trial (NCT01131676).
Monitoring of renal risk factors and kidney function in patients with T2DM
CKD attributed to diabetes benefits from early intervention and thus warrants a screening program. 96 Urinary albumin excretion should be assessed in all adults at diagnosis of T2DM, and at least annually thereafter. In addition, for the estimation of GFR, serum creatinine should be measured at least annually regardless of the degree of urinary albumin excretion. 96 Albuminuria and eGFR are useful biomarkers for predicting the risk of renal and cardiovascular events, and treatment-induced reductions in albuminuria or changes in eGFR are associated with long-term renal and cardiovascular protection. 97 Continual monitoring of risk factors and renal function together with adjustment of the treatment regimen is important to maintain long-term glycaemic, BP and dyslipidaemia control. 98 Hypoglycaemia is a particular concern because increasing RI is associated with increasing hypoglycaemia risk. 43 Thus, certain oral glucose-lowering drugs that are eliminated by the kidneys are contraindicated in patients with T2DM and CKD. 43
Conclusion
Despite the use of lifestyle and pharmacologic interventions to reduce renal risk factors such as hypertension and hyperglycaemia, albuminuria frequently remains elevated in many patients with T2DM. As a consequence, DN persists as a major health problem, with many patients progressing to ESRD, and new strategies are needed to mitigate this burden.
The optimal treatment and prevention of DN calls for an early, intensive and multifactorial approach that targets all major renal risk factors at the same time. With regard to glucose-lowering pharmacotherapy, treatment should be carefully selected to balance adverse effects, such as hypoglycaemia and weight gain, with the benefits of lowering glucose. In particular, patients with CKD have an increased risk of hypoglycaemia, and many glucose-lowering drugs are either contraindicated or require dose adjustment in this high-risk population.
In addition to controlling risk factors, treatments should offer direct protection from DN and other end-organ damage, and the efficacy of new treatment modalities should be evaluated by their antiproteinuric effects and renal benefits. The improvement in albuminuria seen with DPP-4 and SGLT2 inhibitors suggests that these antidiabetes drugs may potentially provide renal benefits beyond their glucose-lowering effects. If beneficial renal effects are confirmed in future studies, a single DPP-4 and SGLT2 inhibitor combination pill may offer a promising therapeutic option for T2DM patients with CKD.
Due to the progressive nature of T2DM, regular assessment of risk factors and adjustment of treatment regimens are important management steps to maintain long-term glycaemic and BP control. Continual monitoring of renal function, including urinary albumin excretion, creatinine clearance and GFR, is critical to follow the progression of kidney disease in patients with T2DM. However, currently available data on the treatment and prevention of DN are mainly from observational studies, and large-scale intervention studies are required.
Key messages
Optimal treatment and prevention of diabetic nephropathy may require an early, intensive and multifactorial approach.
Anti-hyperglycaemic therapy should be carefully selected to balance adverse effects, such as hypoglycaemia and weight gain, with the benefits of lowering glucose.
Any therapy should also offer direct protection from diabetic nephropathy and provide renal benefits.
Newer classes of antidiabetes drugs may provide renal benefits in addition to their glucose-lowering effects.
Due to the progressive nature of T2DM, regular assessment of risk factors and adjustment of treatment regimens are important management steps to maintain long-term glycaemic and BP control.
Footnotes
Acknowledgements
The authors were fully responsible for all content and editorial decisions, were involved at all stages of article development and have approved the final version of the review that reflects the authors’ interpretation and conclusion. Medical writing assistance, supported financially by Boehringer Ingelheim, was provided by Howard Christian of Envision Scientific Solutions during the preparation of this review. Boehringer Ingelheim was given the opportunity to check the data used in the article for factual accuracy only.
Declaration of conflicting interests
Guntram Schernthaner has received lecture fees from Amgen, AstraZeneca/Bristol-Myers Squibb, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline (GSK), Merck Sharp & Dohme (MSD), Novartis, Novo Nordisk, Sanofi-Aventis, Servier and Takeda. Carl Erik Mogensen has declared no conflicts of interest. Gerit-Holger Schernthaner has received scientific grants and/or educational grants and/or travel grants and/or slide honoraria, and/or lecture honoraria, and/or advisory board honoraria, and/or contract research and/or partner research from/with Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Eli Lilly, Medtronic, Menarini, Merck, MSD, Novo Nordisk, Novartis, Pfizer, Sanofi, Sanofi-Aventis, Servier and Takeda in the past 10 years.
Funding
This article was supported financially by Boehringer Ingelheim.