
Abstract
Objective:
To evaluate the risk of cardiovascular events in diabetes defined by isolated post-challenge hyperglycaemia (IPH).
Methods:
We followed 3794 subjects aged ≥40 years without known history of diabetes or cardiovascular disease (CVD) at baseline for CVD events. Participants were categorized as subjects without diabetes [fasting plasma glucose (FPG) < 126 mg/dL and 2-h post-challenge plasma glucose (2-hPG) < 200 mg/dL], IPH (FPG < 126 mg/dL and 2-h PG ≥ 200 mg/dL) and fasting hyperglycaemia (fasting blood glucose (FBS) ≥ 126 mg/dL). Hazard ratios (HRs) were calculated with the use of Cox proportional-hazards regression models to evaluate the risk of CVD events.
Results:
At baseline, of 486 subjects with newly diagnosed diabetes, 190 (39%) had IPH. Over the next 8 years, age and sex-adjusted HR for incident CVD was 1.77 (95% confidence interval (CI): 1.19–2.64; p = 0.005) in subjects with IPH compared with subjects without diabetes. After further adjustment for potential confounders, the HR for CVD was not significant [1.32 (95% CI: 0.88–1.99; p = 0.2)].
Conclusions:
IPH in middle-aged adults adds nothing for identifying CVD risks when other risk factors are taken into account. Associated metabolic risk factors seem to be more important than hyperglycaemia per se.
Introduction
Isolated post-challenge hyperglycaemia (IPH), defined as fasting plasma glucose (FPG) < 126 mg/dL and 2-h post-challenge plasma glucose (2-hPG) ≥ 200mg/dL after oral glucose tolerance test (OGTT), is a phenotype of an early stage of overt type 2 diabetes mellitus (DM), 1 which is usually unrecognized and untreated. 2,3 Although 2-hPG (OGTT) is the only diagnostic tool available to identify subjects with IPH, its use is discouraged because of its inconvenience, less reproducibility and higher cost. According to a report from National Health and Nutrition Examination Survey (NHANES III), the prevalence of IPH was 3.3%, 4 which encompassed about 41% of all newly diagnosed DM. In an urban Iranian population, the prevalence of IPH was 3.1%, 5 being 40% of total new cases of DM, a prevalence that increases with age.
Diabetes confers about a twofold excess risk for a wide range of cardiovascular diseases (CVDs), independent of other conventional risk factors. 6,7 Recent studies have shown that, to reduce CVD mortality, interventions should be implemented in the early stage of diabetes, highlighting the importance of early diagnosis and hazards associated with delaying in treatment, especially in undiagnosed cases. 8,9 Considering the above concept, more attention to diagnosis of mild hyperglycaemia, such as IPH, would be prudent.
There is controversy over the choice of the most accurate predictor for CVD events, between impaired fasting blood glucose (FBS) and 2-hPG load. Most studies suggest that 2h-PG is superior to FBS in assessing the risk of future CVD. 10,11 However, other studies demonstrate that 2h-PG add nothing 12 or very little 13 to identifying CVD risk. Individuals with IPH, especially older adults, in the absence of clinically diagnosed diabetes, experience significant fasting and postprandial metabolic dysregulation, accompanied by a proatherosclerotic and prothrombotic vascular profile. 14 To the best of our knowledge, only a few longitudinal studies have evaluated possible association between IPH, as a phenotype of DM, and CVD outcome. 15 –20 Conducted within the framework of the Tehran Lipid and Glucose Study (TLGS), a large population-based cohort, we followed individuals with IPH for development of CVD events during a mean of 8.1 years.
Methods
Subjects and design
TLGS is a study conducted to determine the prevalence of non-communicable diseases and the risk factors of atherosclerosis among Tehran’s urban population and to develop population-based measures to decrease the prevalence of DM and dyslipidemia. 21 The baseline survey was performed from 1999 to 2001, including 15,005 residents of Tehran, aged ≥3 years. The details of sampling have been published elsewhere. 21 From participants of the cross-sectional phase, we used data of 3794 subjects aged ≥40 years without known history of DM or CVD and with full relevant clinical and biochemical data both at baseline and end of follow-up. The ethics committee of the Research Institute for Endocrine Sciences approved this study.
Measurements
At baseline, subjects were interviewed by trained interviewers using pre-tested questionnaires. Anthropometric measures included weight and waist circumference (WC). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured twice in a seated position after a 15-min rest period using a standard mercury sphygmomanometer, and the mean of the two measurements was considered as the participant’s blood pressure. Overall obesity was considered as body mass index (BMI) ≥ 25 kg/m2. With the ethnic-specific cut-off point for WC in Iranians, 22 central obesity was considered as WC ≥ 95 cm in both genders. Data on physical activity, reported previously, 23 were obtained using the Lipid Research Clinic (LRC) questionnaire. Subjects were classified into three groups as having light, moderate and severe physical activity based on their oral responses to the LRC questionnaire. Additional information on smoking habits was also collected.
A blood sample was taken after a 12- to 14-h overnight fast. All blood analyses were done at the TLGS research laboratory on the day of blood collection. Standard OGTTs were performed in participants without treated diabetes. Plasma glucose and serum lipids were determined as previously described. 21,24 The subjects underwent a standardized 25 75-g OGTT.
The collected data were then evaluated by an outcome committee consisting of an internist, an endocrinologist, a cardiologist, an epidemiologist and other experts, when needed, to assign a specific outcome for every event. In this study, our desired events were the first CVD events, including definite myocardial infarction (MI) [with diagnostic electrocardiogram (ECG) and biomarkers], probable MI (positive ECG findings plus cardiac symptoms or signs plus missing biomarkers or positive ECG findings plus equivocal biomarkers), unstable angina (new cardiac symptoms or changing symptom patterns and positive ECG findings with normal biomarkers), angiographic proven coronary heart disease (CHD), stroke (as defined by a new neurological deficit that lasted more than 24 h) and death from CVD.
Hypertension was defined as SBP/DBP ≥ 140/85 mm Hg. High triglyceride (TG) was defined according to the fasting triglycerides ≥ 150 mg/dL. Fasting high-density lipoprotein cholesterol (HDL-C) < 40 mg/dL in men or <50 mg/dL in women, and fasting total cholesterol (TC) ≥ 240 mg/dL were considered as low HDL-C and high TC, respectively. 26 Details of the biochemical measurements are published elsewhere. 24 We used three categories: subjects without diabetes as FPG < 126 mg/dL and 2-hPG < 200 mg/dL (reference group); IPH as FPG < 126 mg/dL and 2-hPG ≥ 200 mg/dL and fasting hyperglycaemia as FBS ≥ 126 mg/dL. Classification of pre-diabetes status [impaired fasting glucose (IFG) as FPG ≥ 100 and <126 mg/dL, and impaired glucose tolerance (IGT), as 2-hPG ≥ 140 and <200 mg/dL] was based on the American Diabetes Association criteria. 11
Statistical analyses
All continuous data are expressed as mean [standard deviation (SD)] and/or median [interquartile (IQ25–75)], and categorical variables are expressed as percentage. Categorical variables were compared using the chi-square test. Differences of continuous variables between three groups were analysed using analysis of variance (ANOVA; Tukey’s post hoc test) and Kruskal–Wallis test where appropriate. Man–Whitney test was used for pairwise comparisons of TG.
Participants, free of known history of DM or CVD at baseline, were followed up until the occurrence of a new ischaemic cardiovascular (CV) event (the exact date of which was considered as the date of the end-point event) or to death or loss to follow-up, in which case the date of the last patient visit or date of death due to a non-CVD event was considered as censoring. We tested for interaction between sex and different diabetes categories in development of CVD (p = 0.4). The Cox proportional-hazards model was used to predict the independent contribution of IPH to CVD after adjusting for age, sex and potential confounders. The proportional-hazards assumption in the Cox model was assessed graphically and with the Schoenfeld residual test. Proportionality assumptions were appropriate. Statistical analyses were all performed using SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA), and all probabilities are for two-tailed tests, with statistical significance defined as p < 0.05.
Results
After exclusion of subjects with known history of diabetes or CVD at baseline evaluation in 1999–2001, there were 4596 participants, aged ≥40 years; of these, clinical and biochemical data were available for 3794 (82.5%) at the end of follow-up (March 2009). However, those with missing data did not significantly differ from those with complete data regarding baseline characteristics (data not shown). During follow-up, of the 486 subjects who newly diagnosed with DM, 190 (39%) and 296 (61%) had IPH and fasting hyperglycaemia, respectively. In IPH group, 28% of the subjects had FPG level < 100 mg/dL. The remaining 3308 subjects, who were not diabetic, served as the referent groups for these analyses. Among them, 412 (12.5%) and 377 (11.4%) subjects had IFG and IGT, respectively.
As shown in Table 1, individuals with IPH were significantly older and compared to subjects without diabetes had higher fasting and 2h-PG levels and BMI, WC, SBP, DBP, TC and TG as well. Cigarette smoking and physical activity did not differ by IPH status.
Subject characteristics.
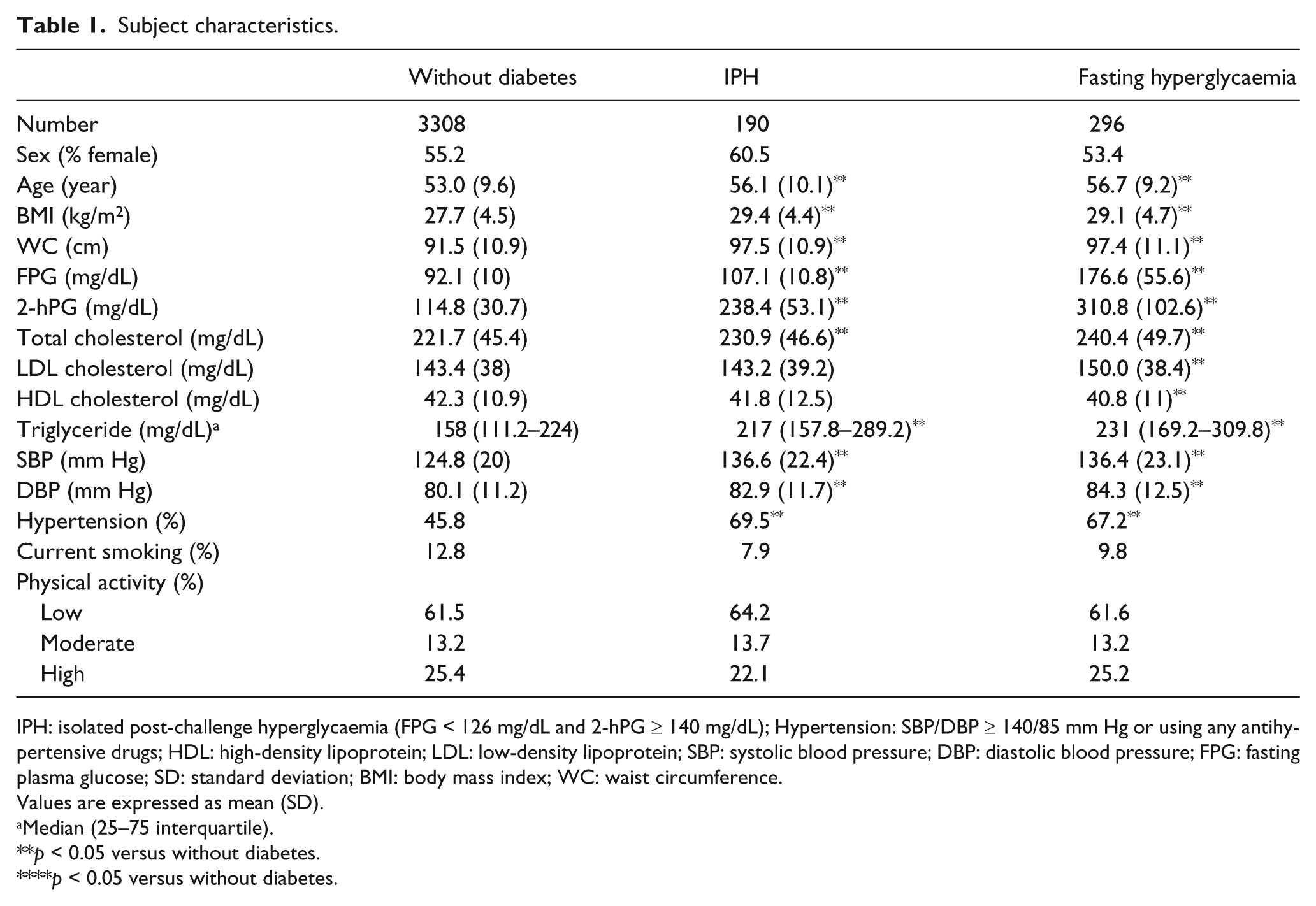
IPH: isolated post-challenge hyperglycaemia (FPG < 126 mg/dL and 2-hPG ≥ 140 mg/dL); Hypertension: SBP/DBP ≥ 140/85 mm Hg or using any antihypertensive drugs; HDL: high-density lipoprotein; LDL: low-density lipoprotein; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; SD: standard deviation; BMI: body mass index; WC: waist circumference.
Values are expressed as mean (SD).
Median (25–75 interquartile).
p < 0.05 versus without diabetes.
p < 0.05 versus without diabetes.
Over a mean of 8.1 years (SD = 1.6 years) of follow-up, 346 subjects developed a first CVD event. Among those with IPH and subjects without diabetes at baseline, there were 27 (14.2%) and 246 (7.4%) CVD events, respectively. Table 2 shows the CVD risk for the different glycaemic status as determined by the Cox proportional-hazards model. In the age- and sex-adjusted Cox model, IPH was associated with CVD [hazard ratio (HR) = 1.77; (95% CI: 1.19–2.64)]. HR was not statistically changed in Cox models adjusted for age, sex and hypertension. However, with further adjustment for central obesity, low HDL, high TC, high TG and current smoking, HR for CVD was not significant [HR = 1.32 (95% CI: 0.88–1.99)].
The hazards of cardiovascular events according to the different diabetes categories: Tehran Lipid and Glucose Study.
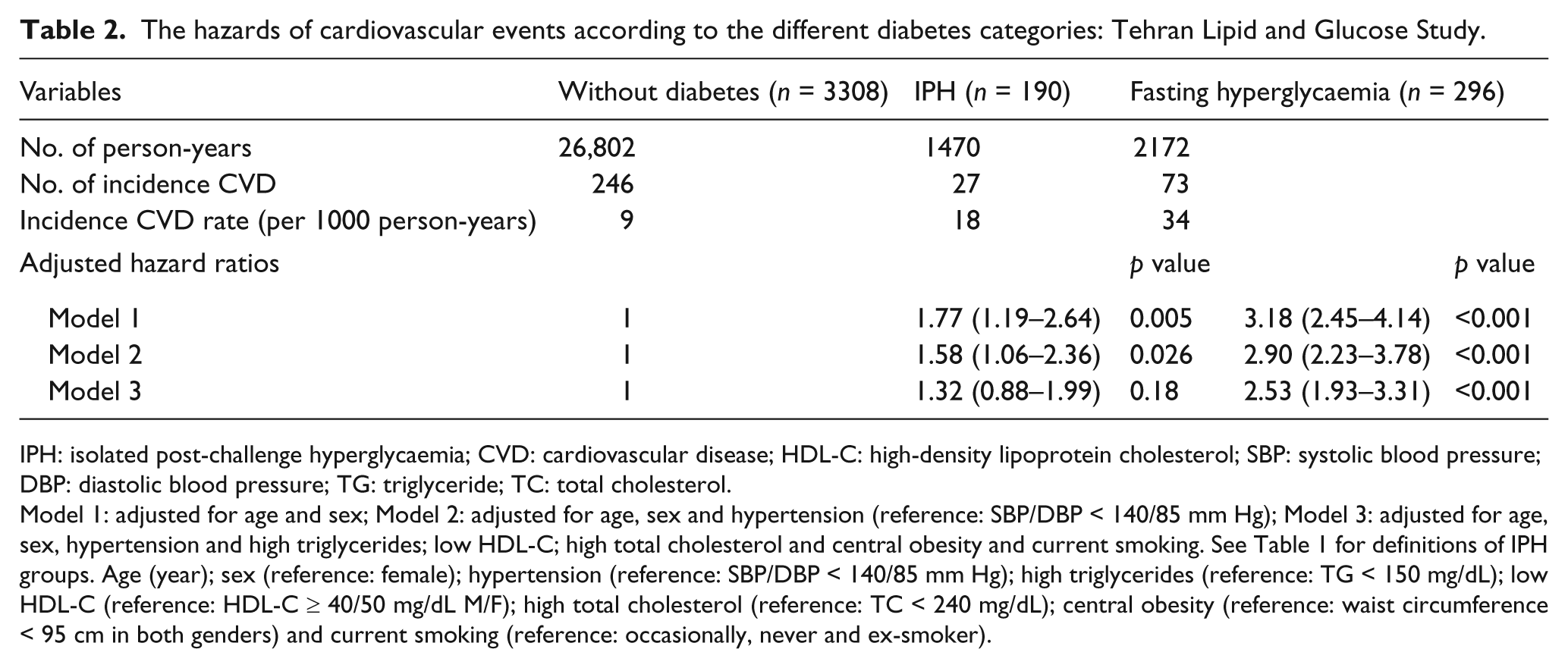
IPH: isolated post-challenge hyperglycaemia; CVD: cardiovascular disease; HDL-C: high-density lipoprotein cholesterol; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG: triglyceride; TC: total cholesterol.
Model 1: adjusted for age and sex; Model 2: adjusted for age, sex and hypertension (reference: SBP/DBP < 140/85 mm Hg); Model 3: adjusted for age, sex, hypertension and high triglycerides; low HDL-C; high total cholesterol and central obesity and current smoking. See Table 1 for definitions of IPH groups. Age (year); sex (reference: female); hypertension (reference: SBP/DBP < 140/85 mm Hg); high triglycerides (reference: TG < 150 mg/dL); low HDL-C (reference: HDL-C ≥ 40/50 mg/dL M/F); high total cholesterol (reference: TC < 240 mg/dL); central obesity (reference: waist circumference < 95 cm in both genders) and current smoking (reference: occasionally, never and ex-smoker).
Discussion
This is the first population-based cohort study in the Middle East region, showing that IPH as a phenotype of newly diagnosed DM, beyond conventional metabolic abnormalities, adds nothing for identifying diabetic patients who are at increased risk for CVD. From a clinical perspective, it seems that ignoring IPH phenotype does not confer significant risks if the other risk factors are taken into account. Based on our results and the difficulties encountered in OGTT, omitting of OGTT and more emphasis being placed on FPG measurement would be proposed as a reasonable strategy in routine clinical practice.
There are a lot of studies addressing differences between pre-diabetic stages (IGT and IFG) with diabetic subjects in developing CVD. 27,28 Previously, in framework of TLGS, it has been shown that newly diagnosed DM consisting of IPH and fasting hyperglycaemia was a strong risk factor for incident CVD compared with pre-diabetic and normal subjects. 29,30 An unanswered question relates to whether blood glucose levels per se, especially in pre-diabetes range, are a direct cause of CVD. 31,32 Recently, a systematic review reported that pre-diabetes can increase risk for CVD by 20%. 33 However, due to difficulty in separating effects of associated cardiometabolic risk factors, this does not prove that this range of glycaemia directly causes clinical CVD. However, there is little doubt regarding direct role of overt fasting hyperglycaemia on atherogenesis. In this study, we have focused on different phenotypes of diabetes and their comparisons with all subjects without diabetes (normal and pre-diabetic). Several studies have tried to clarify the IPH and CVD association; 15 –20 however, these studies differed from each other in the terms of varying types of study designs, lengths of follow-up, types of outcomes and ascertainment methods used, adjustment for confounders and statistical analysis leading to inconsistent results. Different to our findings, a few studies have been reported that IPH made a statistically significant contribution to predicting CVD, even after accounting for conventional CV risk factors. 15 –18 In the Rancho Bernardo Study, 16 IPH after adjusting for age, waist-to-hip ratio (WHR), TG, HDL-C, hypertension and current smoking in older women, but not in men, doubled the risk of fatal CVD and heart disease after a mean follow-up of 7 years. Moreover, Shaw et al. 17 evaluated 9179 subjects from three population-based longitudinal studies, followed for between 5 and 12 years, and they showed that subjects with IPH had increased all-cause mortality in both genders and at least twice the CVD mortality risk in contrast to subjects without diabetes, after adjustment for age, ethnicity, blood pressure and BMI. In contrast to above studies, we have included non-fatal outcomes to identify the composite end point (CVD outcomes); also, subjects included in our study were obviously younger than those of the Rancho Bernardo Study. However, similar to ours, other studies reported non-significant association between IPH and increased risk of CVD mortality. 19,20 The Strong Heart Study involved a cohort of 4304 American Indian aged 45 to 74 years who were followed for 9 years to describe the CVD, cancer and all-cause mortality by FPG, IPH and IGT. 19 Those with IPH had non-significant elevations in risk for CVD mortality compared with normal FPG (<110 mg/dL). Moreover, the NHANES II Mortality Study showed that in the 3092 adults aged 30–74 years, post-challenge hyperglycaemia was not associated with increased risk of CVD mortality compared with subjects who had FPG < 126 mg/dL and 2-hbG < 140 mg/dL. 20
Our findings, in line with previous studies, 12,13 demonstrate that 2h-PG in the context of mild fasting hyperglycaemia (100 < FPG < 126 mg/dL) has little impact on development of CVD. In addition, after adjustment for metabolic risk factors association between overt fasting hyperglycaemia and CVD remained statistically significant. Recent studies 34 –37 reported that addition of metabolic abnormalities to overt fasting hyperglycaemia did not alter the CVD risk, whereas addition of metabolic abnormalities to subjects without diabetes fasting hyperglycaemia did increase it. Consequently, it seems that treatment of cardiometabolic risk factors using statins and/or antihypertensive drugs, 38,39 irrespective of 2h-PG, should be given more consideration for individuals with this range of mild fasting hyperglycaemia. In any case, measurement and treatment of 2h-PG in subjects with mild fasting hyperglycaemia and metabolic abnormalities do not contribute any additional prognostic information. However, there are some conflicting intervention studies addressing lowering postprandial hyperglycaemia in reducing CVD. 40,41 In the STOP Non-Insulin-Dependent Diabetes Mellitus (STOP-NIDDM) trial the effects of acarbose in the prevention of type 2 DM in patients with IGT was tested. 40 The results of post hoc analysis indicated that during the 3.3 years, acarbose was associated with 49% reduction in CV events. However, NAVIGATOR (Nateglinide and Valsartan in Impaired Glucose Tolerance Outcomes Research) in a median of 5.0 years of follow-up showed that nateglinide did not reduce the incidence of CVD events. 41
Our survey has both limitations and strengths. First, this study was not powered to report sex-specified analysis due to few CVD events. Second, we could have had some kinds of misclassification because we excluded CVD subjects at baseline, according to self-report, and we defined the categories of glucose homeostasis based on the results of a single OGTT at baseline. Third, subjects could have had changes in their FPG and 2h-PG during the follow-up period, a concern that applies to most epidemiologic studies that only use baseline information on the exposure variable. The patients with newly established DM have been referred to the clinics out of TLGS study; therefore, we do not have any data regarding the quality care of these patients during whole period of follow-up. Fourth, physical activity level of subjects was evaluated with qualitative questionnaire LRC, which, despite its simplicity and being completed using participants’ oral responses, has not yet been validated in our country. Fifth, as we mentioned, 23.9% of the without diabetes group had IFG or IGT. This may lead to an increased risk of CVD event in the without-diabetes group and may dilute possible difference in comparison to IPH group. However, we have to keep in mind that our primary aim was to compare different categories of abnormal glucose metabolism based on proposed definition. Therefore, this limitation would be of minor concern. Moreover, adjustment for baseline FPG did not change the results. Finally, we did not take into account the role of dietary intake and socio-economic status. However, the large sample size, relatively young participants, low rate of loss to follow-up and adjustment for conventional risk factors are the strengths of our study that need to be mentioned.
In conclusion, based on the results of this study, it would seem that, among middle-aged adults, after adjustment for metabolic risk factors, IPH has no significant association with development of CVD. Therefore, reduction of cardiometabolic risk factors is more important than treatment of hyperglycaemia per se in subjects having this range of mild fasting hyperglycaemia. In fact, it appears that 2-hPG as an epiphenomenon does not require special attention in this phenotype.
Footnotes
Acknowledgements
We thank Mrs Sarbakhsh for her help with statistical analysis, Mrs Nilufar Shiva for her assistance in language editing and the staff and participants in the TLGS study for their contributions.
Conflict of interest
Nothing to declare.
Funding
This work was supported by the Research Institute of Endocrine Science, Shahid Beheshti University Medical Science, Iran (grant no. 098).