
Abstract
The low-density lipoprotein cholesterol (LDL-C) lowering efficacy of switching to ezetimibe/simvastatin (EZ/S) 10/20 mg versus doubling the run-in statin dose (to simvastatin 40 mg or atorvastatin 20 mg) or switching to rosuvastatin 10 mg in subjects with cardiovascular disease (CVD) and diabetes was assessed. Endpoints included percentage change in LDL-C and percentage of patients achieving LDL-C <70 mg/dL. Significantly greater reductions in LDL-C occurred when switching to EZ/S versus statin doubling in the overall population and in subjects treated with simvastatin 20 mg or atorvastatin 10 mg (all p < 0.001). The LDL-C reduction was numerically greater when switching to EZ/S versus switching to rosuvastatin (p = 0.060). Significantly more subjects reached LDL-C <70 mg/dL with EZ/S (54.5%) versus statin doubling (27.0%) or rosuvastatin (42.5%) in the overall population (all p < 0.001) and within each stratum (all p < 0.001). Switching to EZ/S provided significantly greater reductions in LDL-C versus statin doubling and significantly greater achievement of LDL-C targets versus statin doubling or switching to rosuvastatin.
Introduction
Patients with diabetes have an overall increased risk of cardiovascular disease (CVD)1,2 and CVD events.3,4 Therefore, US and European treatment guidelines, including those from the American Diabetes Association and American College of Cardiology Foundation, recommend reducing low-density lipoprotein cholesterol (LDL-C) to <70 mg/dL (<1.81 mmol/L) in patients with diabetes and CVD, and Canadian treatment guidelines, the Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology and the European Association for the Study of Diabetes recommend reducing LDL-C to at least <77 mg/dL (<2.00 mmol/L) in patients with diabetes, regardless of baseline LDL-C level.5 –9
To achieve these aggressive lipid-lowering goals, many at-risk patients may require LDL-C lowering beyond that achieved by recommended starting doses of statin therapies. Recent comparative studies with a placebo run-in period have demonstrated that in high-risk patients, the combination of ezetimibe/simvastatin was more effective than atorvastatin or rosuvastatin in lowering LDL-C at each dose comparison.10,11 In another study with a placebo run-in, the combination of ezetimibe/simvastatin was also shown to more effectively lower LDL-C versus atorvastatin across a range of doses in subjects with type 2 diabetes. 12 However, using a placebo run-in does not reflect the usual clinical approach of physicians who up-titrate or switch their high cardiovascular risk patients with unsatisfactory LDL-C levels to a more potent statin. This study was designed to approximate the clinical practice of changing treatments by assessing the additional LDL-C percent reduction by switching to ezetimibe/simvastatin 10/20 mg versus doubling the initial statin dose or switching to rosuvastatin 10 mg in diabetics with CVD treated with simvastatin 20 mg or atorvastatin 10 mg but not at LDL-C goal (<70 mg/dL). The primary efficacy hypothesis was that the percent reduction in LDL-C would be greater with ezetimibe/simvastatin than when doubling the baseline statin dose following 6 weeks of treatment. There were three secondary efficacy hypotheses: (1) In the subpopulation of subjects treated with simvastatin 20 mg at baseline, following 6 weeks of treatment, the percent reduction in LDL-C would be greater when switched to ezetimibe/simvastatin 10/20 mg than when doubling the statin dose to simvastatin 40 mg; (2) in the subpopulation of subjects treated with atorvastatin 10 mg at baseline, following 6 weeks of treatment, the percent reduction in LDL-C would be greater when switched to ezetimibe/simvastatin 10/20 mg than when doubling the statin dose to atorvastatin 20 mg and (3) in the overall population of subjects treated with simvastatin 20 mg or atorvastatin 10 mg at baseline, following 6 weeks of treatment, the percent reduction in LDL-C would be greater when switched to ezetimibe/simvastatin 10/20 mg than when switched to rosuvastatin 10 mg.
Materials and methods
This was a 12-week randomized, double-blind, active-controlled study conducted between June 2009 and March 2011 in 86 centres in Austria, Bulgaria, Chile, Costa Rica, Croatia, Egypt, Estonia, Germany, Greece, Hungary, Italy, Latvia, Lithuania, Peru, Portugal and the United States. This study was conducted in conformance with Good Clinical Practice standards and applicable country and/or local statutes and regulations regarding ethical committee review, informed consent and the protection of human subjects participating in biomedical research.
Eligible subjects were ≥18- and <80-year-old adults with type 1 or 2 diabetes mellitus (HbA1c ≤ 8.5%) and symptomatic CVD, who were naïve to statin and/or ezetimibe or were taking a stable dose of approved lipid-lowering therapy, and if needed, taking stable anti-diabetic medication for 3 months prior to the screening visit, and were willing to maintain an approved cholesterol- and glucose-lowering diet for the duration of the study. In order to be considered eligible for randomization, subjects were required to complete the screening/stabilization period on simvastatin 20 mg or atorvastatin 10 mg with LDL-C ≥70 mg/dL (1.81 mmol/L) and ≤160 mg/dL (4.14 mmol/L), alanine transaminase (ALT) and aspartate aminotransferase (AST) ≤2.0 × upper limit of normal (ULN; no active liver disease), creatine kinase (CK) ≤3 × ULN and triglycerides ≤400 mg/dL (4.52 mmol/L). Subjects were excluded if they were Asian (since rosuvastatin prescribing information recommends a 5 mg starting dose for Asians), had uncontrolled endocrine or metabolic disease that impacted lipids/lipoproteins, uncontrolled or recent-onset diabetes, congestive heart failure, hypertension, digestive disease/intestinal malabsorption, were taking agents impacting lipids, potent CYP3A4 inhibitors, >1 quart/day grapefruit juice, systemic corticosteroids, cyclosporine, danazol or fusidic acid, or agents increasing risk of myopathy or warfarin.
Randomization and blinding
Subjects were randomly assigned to one of the blinded treatment groups using an interactive voice-response system. The subjects were stratified according to the statin taken during the run-in period (simvastatin 20 mg or atorvastatin 10 mg) to ensure distribution of subjects across treatment groups in a 2:1:2 ratio within strata defined by statin potency (simvastatin 20 mg and atorvastatin 10 mg; Figure 1). The subjects who met eligibility criteria at the screening visit were provided with open-label simvastatin 20 mg or atorvastatin 10 mg tablets. At randomization, subjects were supplied with bottles of blinded ezetimibe/simvastatin 10/20 mg or matching placebo, simvastatin 40 mg or matching placebo, atorvastatin 20 mg or matching placebo and rosuvastatin 10 mg or matching placebo in a double dummy fashion. A blocked randomization was used with a block size of 5. The subjects, investigators and study personnel involved in the study remained blinded during the study period until the data were complete and clean and a database lock was obtained.
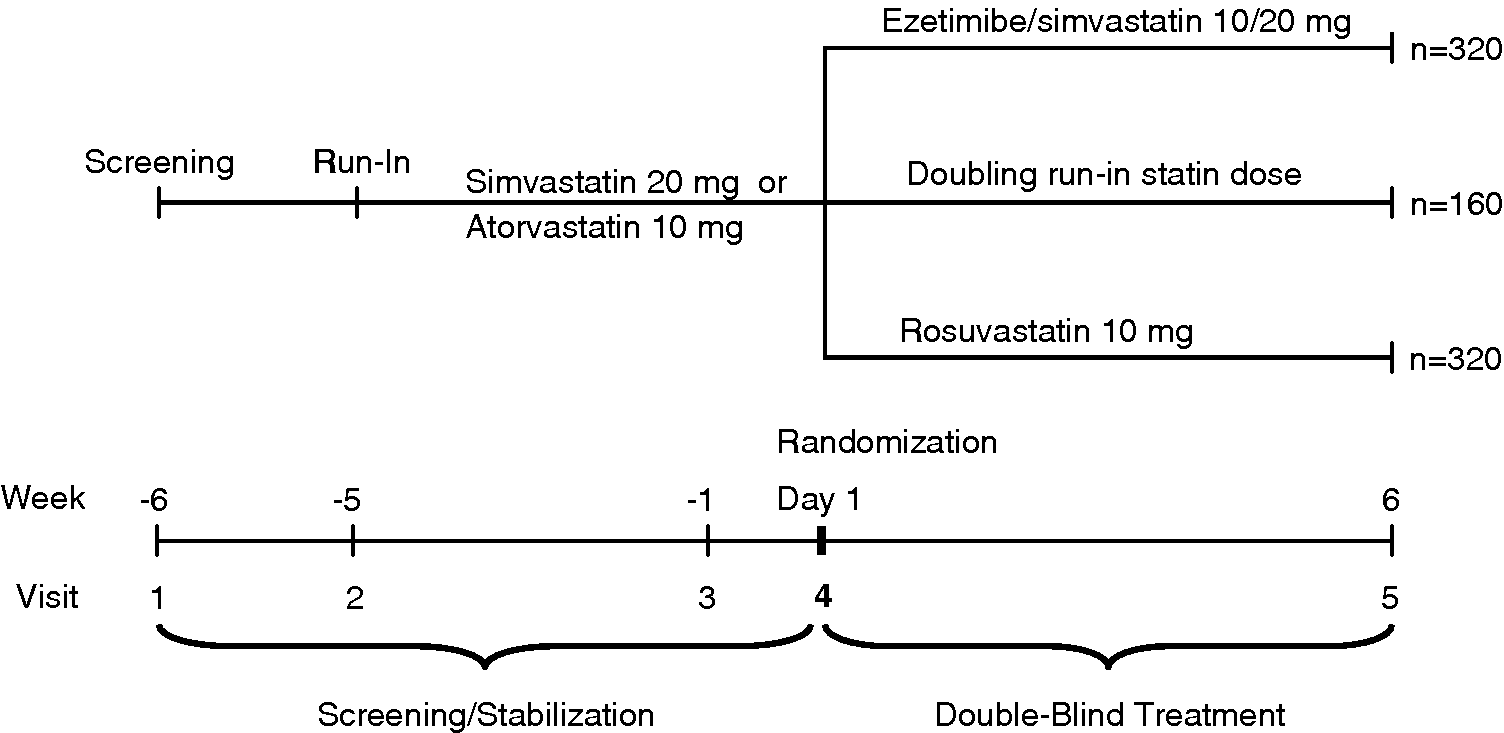
Study schematic showing subject randomization after screening and stabilization during run-in.
Efficacy endpoints
The primary efficacy endpoint was the percent change from baseline in LDL-C at Week 6. Secondary efficacy endpoints were the percent change from baseline in total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), non-HDL-C, apolipoprotein (Apo) B, Apo A-I and high-sensitivity C-reactive protein (hs-CRP) at Week 6 and the percent of patients with LDL-C <70 mg/dL (1.81 mmol/L) at Week 6. In addition, exploratory endpoints included the percent of patients at Week 6 with LDL-C <100 mg/dL (2.59 mmol/L), LDL-C <77 mg/dL (2.00 mmol/L), non-HDL-C <100 mg/dL (2.59 mmol/L) or Apo B <80 mg/dL (0.80 g/L).
Safety endpoints
Pre-specified adverse events of interest were gastrointestinal-related, gallbladder-related, allergic reaction/rash-related and hepatitis-related adverse events; consecutive elevations in ALT/AST ≥3 × ULN, ≥5 × ULN and ≥10 × ULN; consecutive elevations in ALT and/or AST ≥3 × ULN, ≥5 × ULN and ≥10×ULN; elevations in ALT or AST ≥3 × ULN, with serum alkaline phosphatase ≥2 × ULN and total bilirubin >2 × ULN and elevations in CK ≥10 × ULN, elevations in CK ≥10 × ULN with muscle symptoms and elevations in CK ≥10 × ULN with muscle symptoms that are considered drug related.
Statistical methods
Randomizing 800 patients was expected to yield 750 evaluable patients in the full analysis set (FAS) population (a 2:1:2 ratio − 300 each for ezetimibe/simvastatin and rosuvastatin and 150 for statin at double baseline dose) to achieve 99% power (2-sided, α = 0.05) to demonstrate the primary hypothesis that ezetimibe/simvastatin 10/20 mg is superior to doubling baseline statin dose as measured by percent change from baseline in LDL-C at Week 6. This was based on the assumption of an underlying treatment difference of 10% and a standard deviation of 22% for percent change from baseline in LDL-C.
The FAS was used for the primary efficacy analyses and included all randomized subjects who took at least one dose of the study drug and had baseline data. The per-protocol (PP) population was used for supportive efficacy analyses of the primary endpoint and excluded pre-specified protocol violators. The all-patients-as-treated (APaT) approach was used for the safety analyses and included all randomized patients who received at least one dose of the study drug and included all safety data up to 14 days after the last intake of study medication. A constrained longitudinal data analysis (LDA) method, including both baseline and the calculated post-baseline percent change from baseline measurements as response variable, was used to analyse between-group differences in the percent change from baseline in LDL-C (primary endpoint) and the percent change from baseline in other lipid/lipoprotein parameters (secondary endpoints). The data for triglycerides and hs-CRP were log-transformed due to the non-normal distribution. A logistic regression model was used to analyse between-group differences in the percent of subjects with LDL-C <70 mg/dL (1.81 mmol/L), non-HDL-C <100 mg/dL (2.59 mmol/L) and Apo B <80 mg/dL (0.80 g/L). Descriptive statistics were provided for the percent of subjects at endpoint with LDL-C <100 mg/dL (2.59 mmol/L) and LDL-C <77 mg/dL (2.00 mmol/L; exploratory endpoints) in the restricted population of subjects not attaining the corresponding target goal at baseline, respectively.
There were one primary and three secondary efficacy hypotheses. The primary efficacy hypothesis on the single treatment comparison of ezetimibe/simvastatin 10/20 mg versus doubling statin dose at baseline (pooled across strata) for the primary endpoint, percent change from baseline in LDL-C, was performed at significance level 0.050. A closed-step down testing procedure, which keeps the overall Type I error at level 0.050 if each test is performed at level 0.050, was used across the primary and secondary efficacy hypotheses; the closed testing procedure was first used to step down from the overall population (across strata) to each stratum; that is, significance within stratum was only considered if the main comparison (both strata) was significant. The secondary hypothesis related to treatment comparison of ezetimibe/simvastatin 10/20 mg versus rosuvastatin 10 mg (pooled across strata) for the primary endpoint was performed if the primary endpoint for the treatment comparison of ezetimibe/simvastatin 10/20 mg versus doubling statin dose was significant across strata and within each stratum. As some deviation from normality was observed for the percent change from baseline in LDL-C, a post hoc sensitivity analysis on log-transformed data was performed to corroborate the results from the primary analysis on untransformed data.
For the safety analysis, pre-specified adverse events of interest were analysed using the Miettinen and Nurminen method; p-values and 95% confidence intervals (CIs) were provided for between-group differences in the percent of patients with events. For other adverse events reported herein, between-group differences in percent of patients with events were analysed using the Miettinen and Nurminen method, and only 95% CIs were provided.
Results
The flow of patients through the study is shown in Figure 2. Of the 808 randomized patients, 406 patients (50.2%) were stratified to Stratum 1 (simvastatin 20 mg) and 402 (49.8%) were stratified to Stratum 2 (atorvastatin 10 mg) during screening (Figure 1). At randomization, 322 subjects received ezetimibe/simvastatin 10/20 mg, 162 subjects had their run-in statin dose doubled and 324 subjects received rosuvastatin 10 mg. However, there was one patient randomized to ezetimibe/simvastatin 10/20 mg and one patient randomized to rosuvastatin 10 mg that took only blinded placebo. Both subjects were included in the efficacy analyses (based on FAS) and were analysed according to the randomization group. These two subjects were not included in the safety analyses. Baseline demographics and clinical characteristics were generally similar between treatment groups, although there was a slightly higher percent of males in the rosuvastatin group (56.2%) than in the ezetimibe/simvastatin (49.7%) or statin doubling treatment groups (49.4%; Table 1). Mean age (± standard deviation) was 64 (± 8.5) years and mean duration of diabetes mellitus was 9 (± 7.1) years.
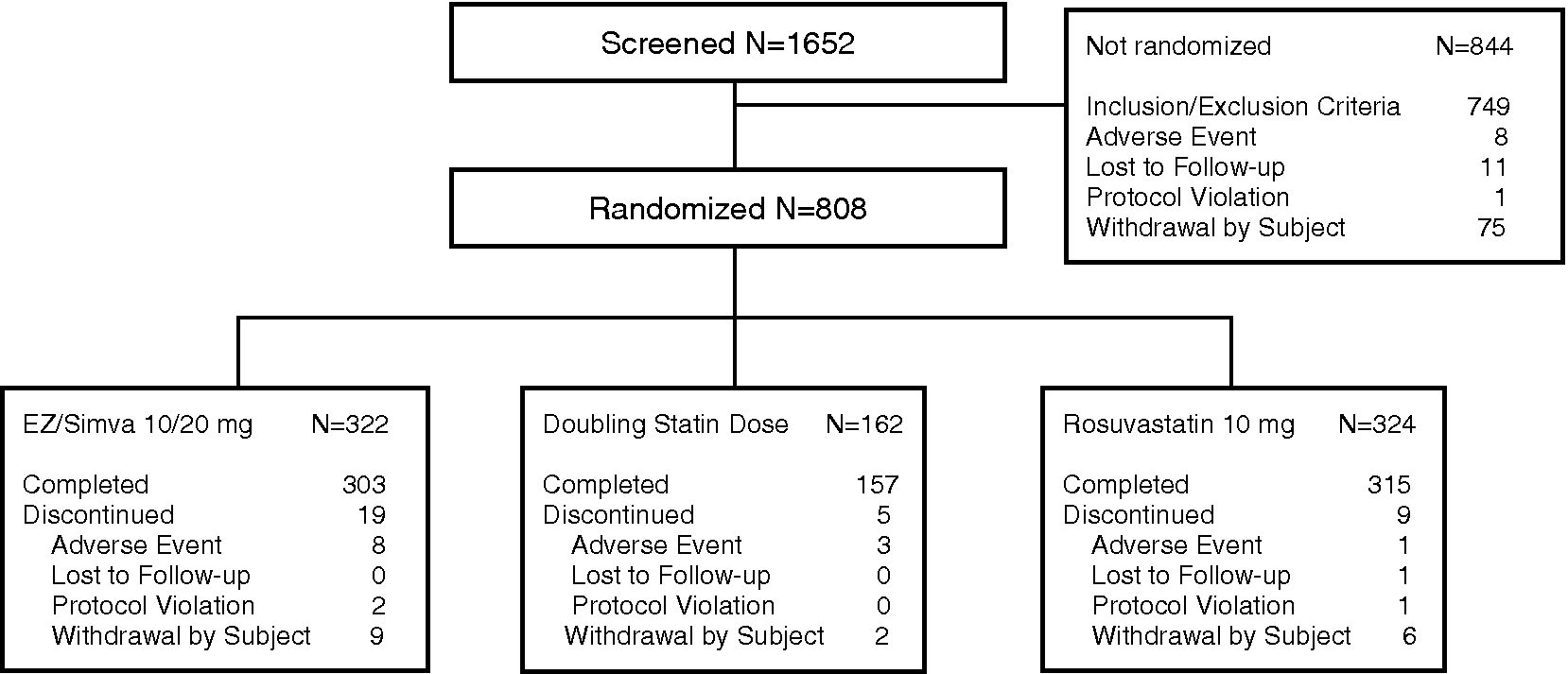
Flow of patients through the study.
Baseline demographics and clinical characteristics.
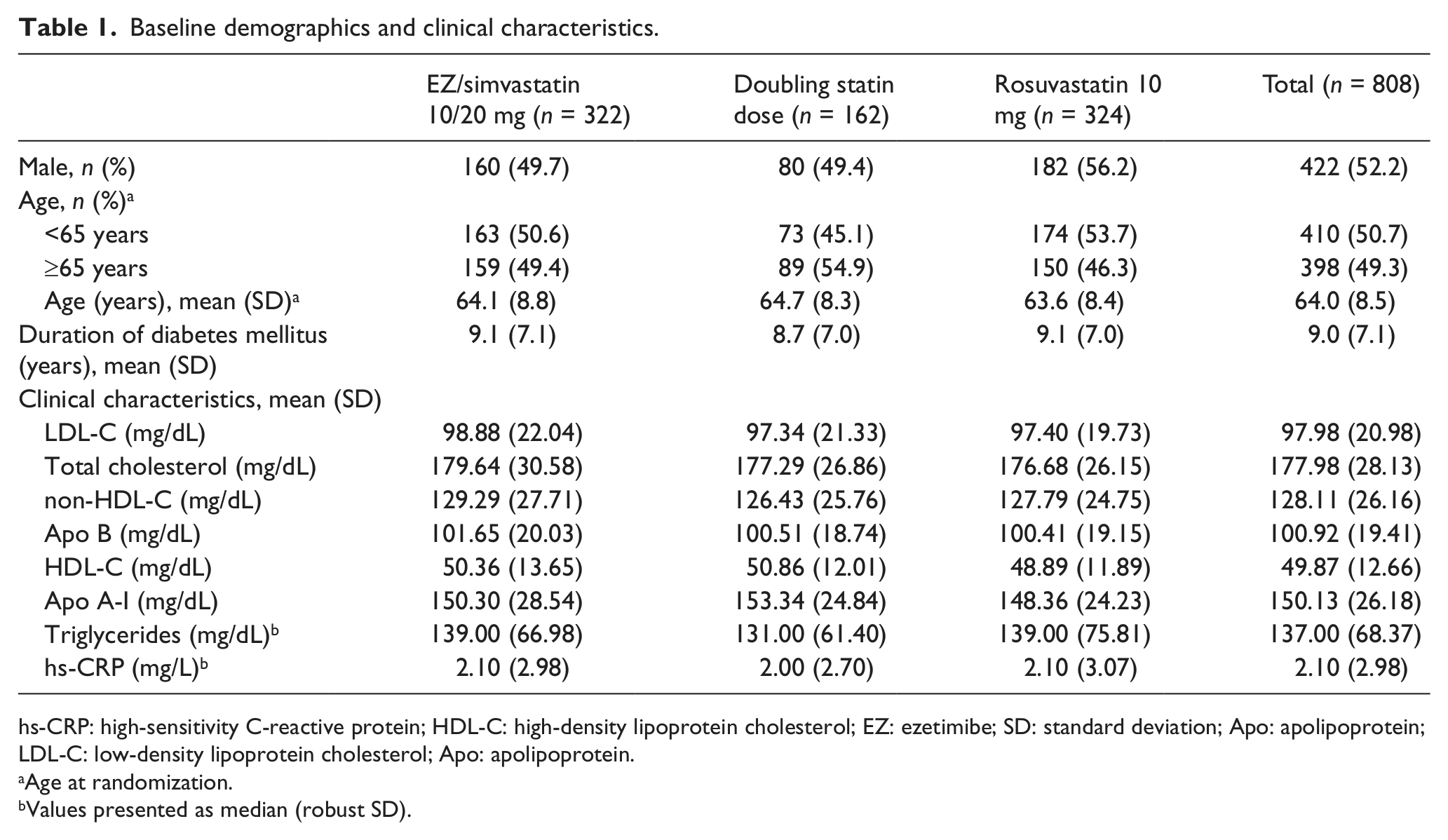
hs-CRP: high-sensitivity C-reactive protein; HDL-C: high-density lipoprotein cholesterol; EZ: ezetimibe; SD: standard deviation; Apo: apolipoprotein; LDL-C: low-density lipoprotein cholesterol; Apo: apolipoprotein.
Age at randomization.
Values presented as median (robust SD).
Treatment with ezetimibe/simvastatin 10/20 mg resulted in a significantly greater reduction in LDL-C compared with doubling the baseline statin dose (−23.13% vs −8.37%; p < 0.001, Figure 3). Both subpopulations of subjects treated with simvastatin 20 mg or with atorvastatin 10 mg at baseline experienced a significantly greater reduction in LDL-C when switched to ezetimibe/simvastatin compared with doubling the dose to simvastatin 40 mg (−21.59% vs −7.98%; p < 0.001) or atorvastatin 20 mg (−24.58% vs −8.85%; p < 0.001, Figure 3) for 6 weeks. In the population of patients receiving simvastatin 20 mg or atorvastatin 10 mg at baseline, the percent reduction in LDL-C was numerically, but not statistically significantly, greater when switched to ezetimibe/simvastatin than when switched to rosuvastatin 10 mg following 6 weeks of treatment (−23.13% vs −19.32%; p = 0.060; Figure 3).
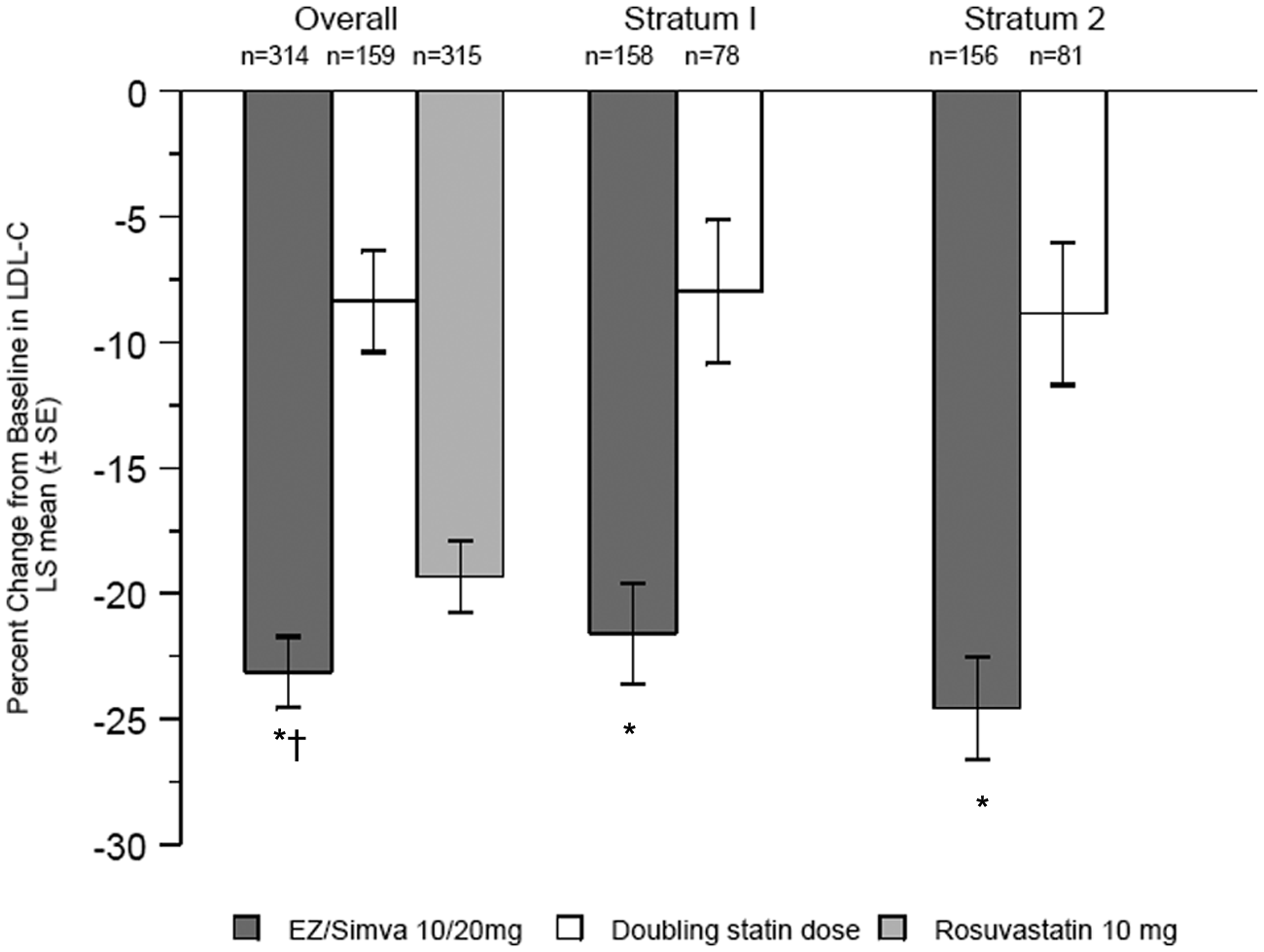
Percent change from baseline in LDL-C by treatment group after 6 weeks of treatment (FAS population). Within Stratum 1, doubling statin dose corresponds to simvastatin 40 mg; within Stratum 2, doubling statin dose corresponds to atorvastatin 20 mg.
The results from the pre-specified supportive analysis using a PP approach applied to the primary variable were generally consistent with those from the primary analysis using the FAS population. However, in this analysis, the percent reduction in LDL-C was significantly greater for subjects switched to ezetimibe/simvastatin 10/20 mg than for those switched to rosuvastatin 10 mg (−24.76% vs −20.10%; p = 0.018). In the overall population, as well as within each stratum, the results of a post hoc sensitivity analysis on log-transformed data were also consistent with those of the main analysis for the comparison of ezetimibe/simvastatin 10/20 mg versus doubling the baseline statin dose (−27.58 vs −11.29; p < 0.001, Figure 4). However, in contrast to the pre-specified secondary analysis, but similar to the supportive PP analysis, the results of the post hoc sensitivity analysis showed that the percent reduction in LDL-C was significantly greater when subjects switched to ezetimibe/simvastatin than when switched to rosuvastatin 10 mg (−27.58 vs −22.20; p = 0.002, Figure 4).
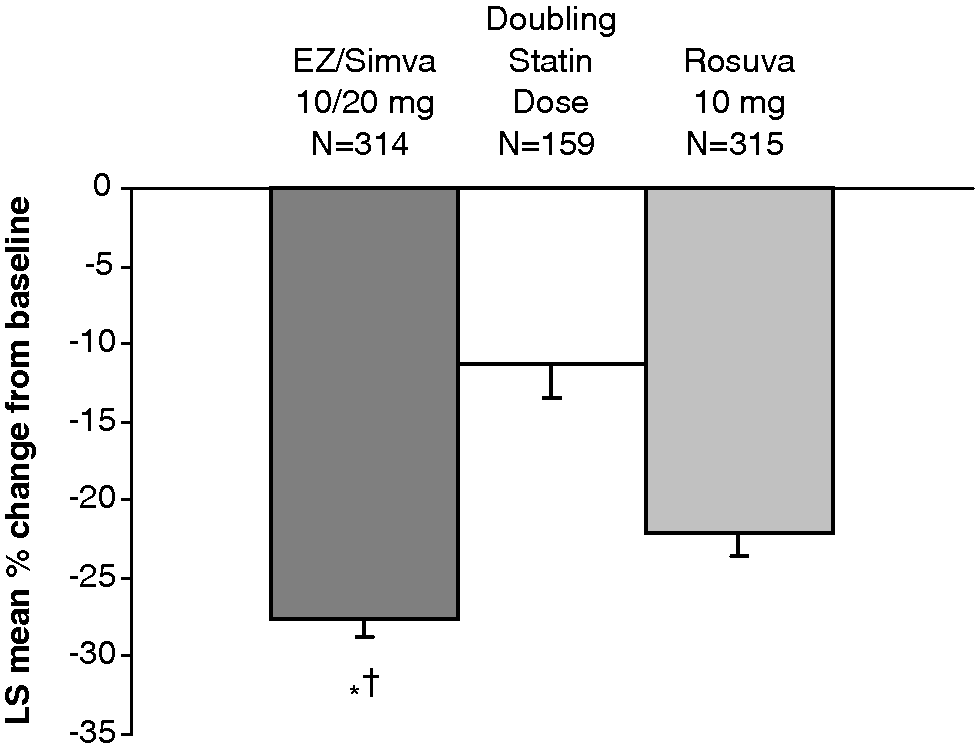
Percent change from baseline in LDL-C by treatment group in the overall population after 6 weeks of treatment (Sensitivity analysis in the FAS population). Doubling statin dose corresponds to simvastatin 40 mg or atorvastatin 20 mg.
The percent changes from baseline in other lipids and lipoproteins are shown in Figure 5. There were significantly greater reductions in total cholesterol and Apo B in subjects taking ezetimibe/simvastatin 10/20 mg compared with subjects who doubled their statin dose (both p < 0.001) and with those taking rosuvastatin 10 mg (both p < 0.05). There were significantly greater reductions in non-HDL-C in subjects taking ezetimibe/simvastatin 10/20 mg compared with subjects who doubled their statin dose (p < 0.001). For all other lipids and lipoproteins, the percent changes were not statistically significantly different between treatments.
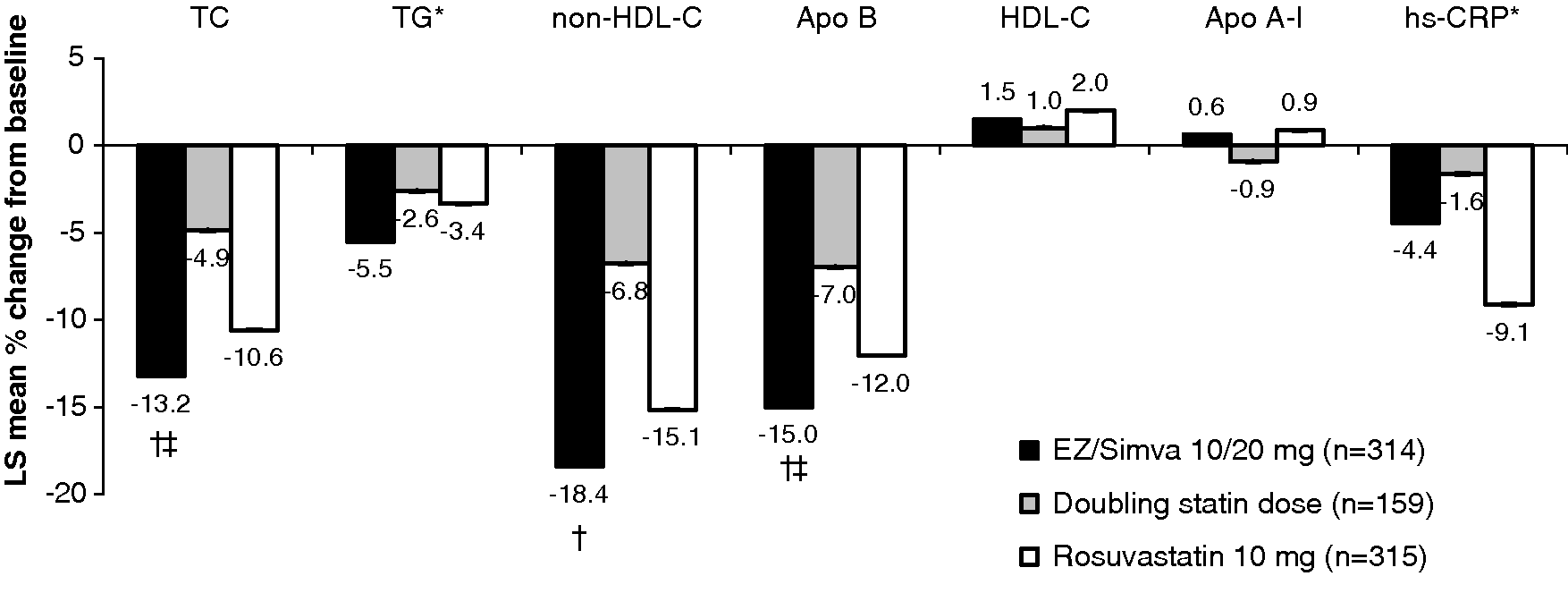
Percent change from baseline in secondary lipid endpoints and hs-CRP (FAS population).
The percent of patients reaching LDL-C goal of <70 mg/dL (1.81 mmol/L) was significantly greater with ezetimibe/simvastatin (54.5%) versus doubling the baseline statin dose (27.0%) or switching to rosuvastatin 10 mg (42.5%) in the overall population (both p < 0.001; Figure 6). Similarly, the percent of patients reaching LDL-C goal of <70 mg/dL (1.81 mmol/L) was significantly greater with ezetimibe/simvastatin within each stratum separately [Stratum 1: ezetimibe/simvastatin vs simvastatin 40 mg (53.2% vs 24.4%; p < 0.001) and Stratum 2: ezetimibe/simvastatin vs atorvastatin 20 mg (55.8% vs 29.6%; p < 0.001); Figure 6]. The percent of subjects reaching LDL-C goal of <100 mg/dL (2.59 mmol/L) was greater with ezetimibe/simvastatin 10/20 mg (71.1%; 95% CI: 62.1, 79.0) versus doubling the baseline statin dose (50.8%; 95% CI: 37.9, 63.6) or switching to rosuvastatin 10 mg (63.3%; 95% CI: 53.8, 72.0). Moreover, the percent of subjects reaching LDL-C goal of <77 mg/dL (2.00 mmol/L) was greater with ezetimibe/simvastatin 10/20 mg (61.4%; 95% CI: 55.4, 67.1) versus doubling the baseline statin dose (31.5%; 95% CI: 23.4, 40.4) or switching to rosuvastatin 10 mg (49.8%; 95% CI: 43.7, 55.9).
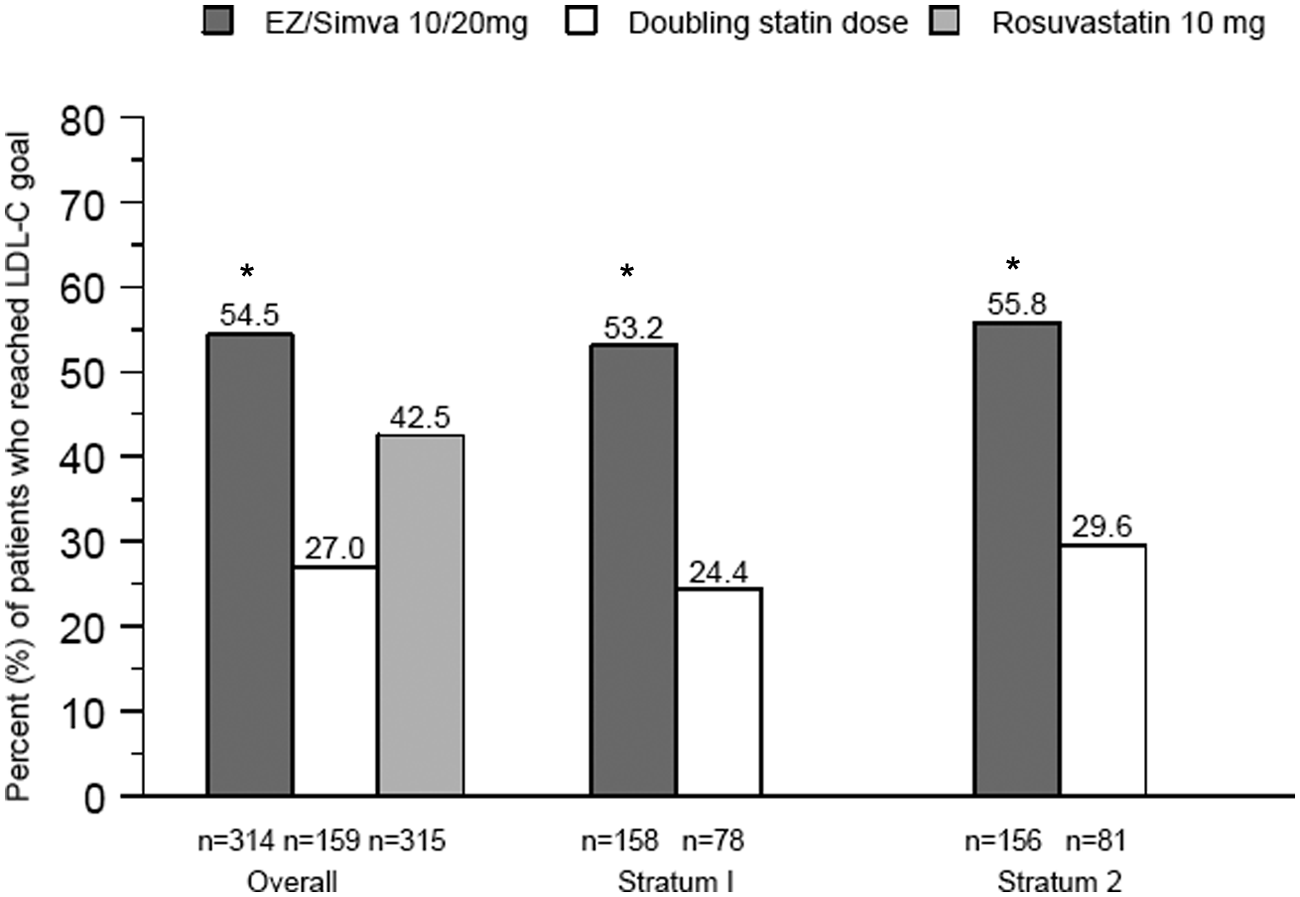
Percent of subjects achieving LDL-C <70 mg/dL (1.81 mmol/L) after 6 weeks of treatment (FAS population).
The percent of patients reaching non-HDL-C <100 mg/dL (2.59 mmol/L) was greater with ezetimibe/simvastatin 10/20 mg versus doubling the baseline statin dose (57.0% vs 30.8%; p < 0.001) or versus rosuvastatin 10 mg following 6 weeks of treatment (57.0% vs 45.1%; p < 0.001). In addition, the percent of patients reaching Apo B <80 mg/dL (0.80 g/L) was greater with ezetimibe/simvastatin 10/20 mg versus doubling the baseline statin dose (47.6% vs 28.3%; p < 0.001) or rosuvastatin 10 mg (47.6% vs 38.5%; p = 0.007).
The overall safety profile appeared generally comparable between ezetimibe/simvastatin (10/20 mg) versus doubling the baseline statin dose and versus rosuvastatin 10 mg. There were no notable differences between treatment groups in the proportion of patients with clinical adverse events, serious adverse events, drug-related adverse events, serious and drug-related adverse events or adverse events leading to discontinuation, except that the proportion of patients with clinical adverse events leading to discontinuation tended to be higher in the ezetimibe/simvastatin (10/20 mg) treatment group compared with the rosuvastatin 10 mg treatment group (Table 2). There were no significant differences between treatment groups in the percent of patients with gastrointestinal-related, allergic reactions– or rash- and hepatitis-related adverse events, except that significantly more patients on rosuvastatin 10 mg had hepatitis-related adverse events than ezetimibe/simvastatin (4 vs 0, p = 0.046; Table 3). Four patients from the rosuvastatin 10 mg group experienced increased levels of gammaglutamyltransferase; two of them also experienced increased ALT and AST. No patients from the ezetimibe/simvastatin (10/20 mg) group and doubling the baseline statin dose group experienced hepatitis-related adverse events. No gallbladder-related clinical adverse events occurred in the study. There was only one patient in the rosuvastatin 10 mg group who experienced elevations in AST ≥3 × ULN; no patient in the other groups experienced such elevations. There were no elevations in ALT ≥ 3× ULN or in CK ≥10 × ULN.
Summary of safety data (APaT population).
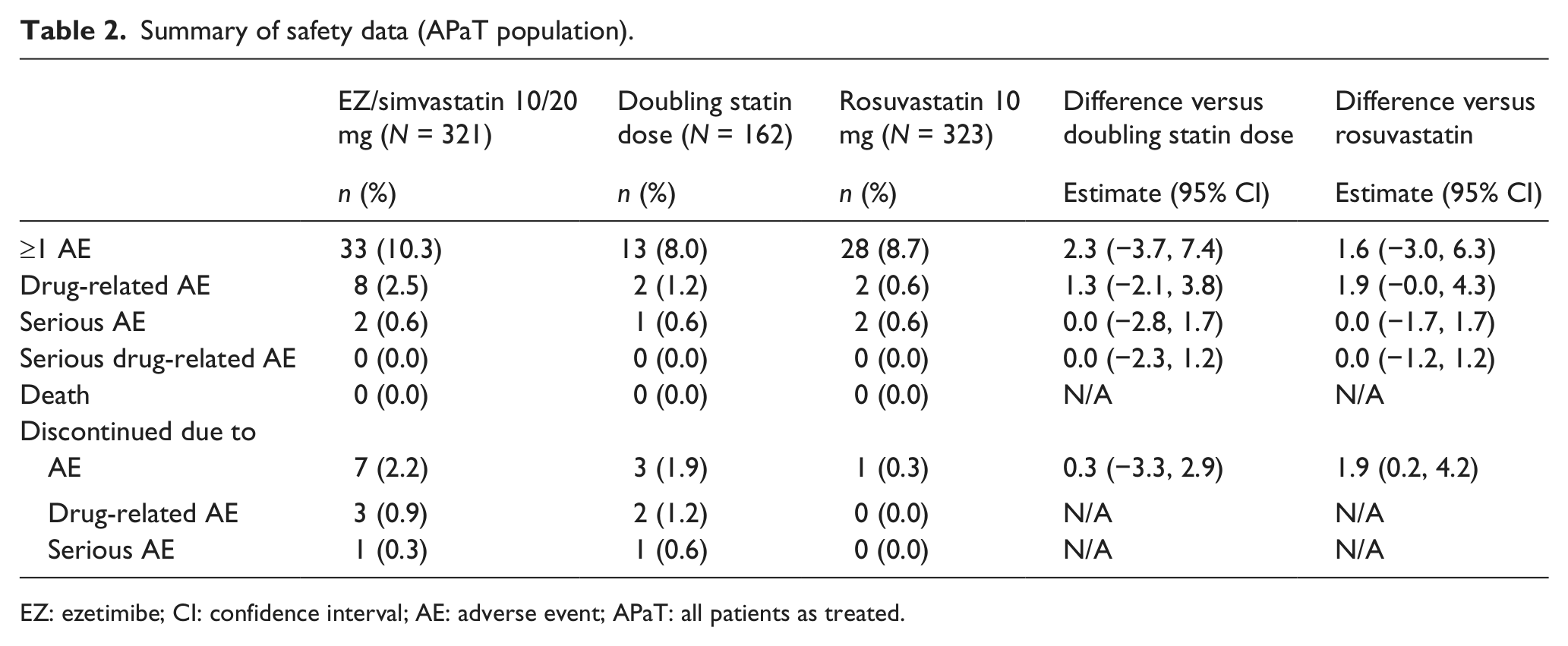
EZ: ezetimibe; CI: confidence interval; AE: adverse event; APaT: all patients as treated.
AEs of special interest (APaT population).
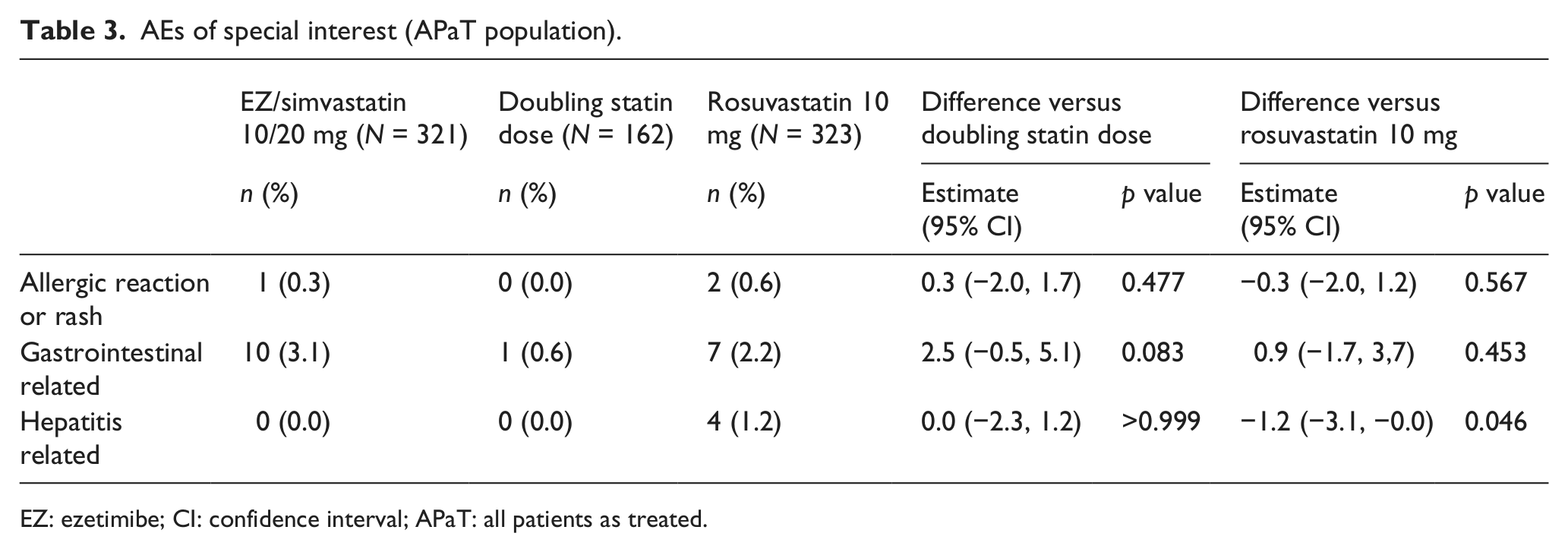
EZ: ezetimibe; CI: confidence interval; APaT: all patients as treated.
Discussion
In this study, compared with doubling the baseline statin dose to simvastatin 40 mg or atorvastatin 20 mg, switching to ezetimibe/simvastatin resulted in significantly greater reductions in LDL-C levels and greater achievement of pre-specified LDL-C targets in subjects with CVD and diabetes mellitus treated with simvastatin 20 mg or atorvastatin 10 mg with LDL-C ≥70 mg/dL (1.81 mmol/L) and ≤160 mg/dL (4.14 mmol/L) at baseline. In addition, total cholesterol, non-HDL-C and Apo B were reduced significantly more with combination treatment compared with doubling the statin dose. The safety and tolerability profiles were generally similar for all treatments.
Although the percent reduction in LDL-C was numerically greater in subjects switched to ezetimibe/simvastatin compared with those switched to rosuvastatin, the between-groups difference was not statistically significant in the pre-specified analysis. However, it was noted in the post hoc sensitivity analysis on log-transformed data that the between-treatment difference was statistically significantly greater in subjects who switched to ezetimibe/simvastatin versus those who switched to rosuvastatin 10 mg. A recent study compared the efficacy of ezetimibe/simvastatin, rosuvastatin and atorvastatin in high-risk (based on Framingham assessment) hyperlipidaemic subjects derived from the Veterans Affairs Health Care System taking at least 40 mg simvastatin but not attaining LDL-C <100 mg/dL. 13 Consistent with the post hoc analysis results of the current study, Furman et al. 13 demonstrated significantly greater reductions in LDL-C with the combination of ezetimibe/simvastatin versus rosuvastatin and versus atorvastatin (average doses used were 9/64, 18 and 68 mg for ezetimibe/simvastatin, rosuvastatin and atorvastatin, representing 80%, 45% and 85% of maximum recommended doses, respectively; p < 0.05). The IN-CROSS study also provided evidence that ezetimibe/simvastatin 10/20 mg was significantly more effective in reducing LDL-C compared with rosuvastatin 10 mg (p < 0.001) in high-CVD-risk subjects who had not achieved LDL-C targets while taking a statin. 14
Traditionally, statins are the first-line choice to achieve LDL-C or other lipid targets defined by treatment guidelines. However, even the higher potency statins may not be sufficient to achieve cholesterol targets in patients at very high risk of CVD events, in part due to the aggressive nature of the targets (i.e. < 77 mg/dL in Canada and <70 mg/dL in Europe and the United States). The Hungarian CORVUS (COntrolled TaRgets for High Vascular Risk Patients Using Effective Statins) trial included 1385 subjects, 1077 of whom were at very high risk, taking rosuvastatin monotherapy. 15 While 58% of the total population achieved the 100 mg/dL LDL-C target, only 19% of the very-high-risk subjects reached their <70 mg/dL target after taking rosuvastatin for 3 months. Treatment with ezetimibe combined with a higher potency statin has been shown to produce greater achievement of LDL-C targets. In a study by Bays et al., 16 attainment of LDL-C ≤70 mg/dL was significantly greater for subjects receiving ezetimibe added to rosuvastatin 5 mg compared with doubling the rosuvastatin dose to rosuvastatin 10 mg (adjusted odds ratio = 5.1; p < 0.001) and also for subjects receiving ezetimibe added to rosuvastatin 10 mg versus rosuvastatin 20 mg (adjusted odds ratio 11.4; p < 0.001). In another study of 579 high-risk CVD subjects (294 had diabetes mellitus), treatment with the combination of ezetimibe plus atorvastatin 40 mg resulted in significantly greater achievement of LDL-C<70 mg/dL compared with subjects treated with atorvastatin 80 mg (74% vs 32%; p <0.001). 17 In the current study, over half of the very-high-risk subjects (55%) achieved the most aggressive LDL-C target (<70 mg/dL) and the majority of subjects (71%) achieved LDL-C <100 mg/dL after taking a recommended starting dose of combination ezetimibe/simvastatin for 6 weeks. It is also important to note that a significantly higher proportion of subjects achieved the specified non-HDL-C target with the combination of ezetimibe/simvastatin compared with any of the statin monotherapies. A recent meta-analysis showed that on-treatment levels of LDL-C and non-HDL-C were associated with risk of future major cardiovascular events and that the association was greater for non-HDL-C than for LDL-C. 18 The achievement of these target levels and good tolerability with a recommended starting dose of ezetimibe/simvastatin is important to note also for patients who may not want to titrate their current statin but could tolerate the addition of ezetimibe to a low-dose statin to achieve their LDL-C target.
The overall tolerability profiles of the study treatments appeared to be generally comparable in this study, although more subjects taking ezetimibe/simvastatin discontinued due to adverse events compared with rosuvastatin. Other trials comparing the safety profile of ezetimibe combined with simvastatin versus statins do not suggest that there are significant tolerability differences between these treatments; 19 however, the use of the highest dose (80 mg) of simvastatin has been restricted by the US Food and Drug Administration due to the higher risk of myopathy/rhabdomyolysis. 20 Moreover, primary studies and sub-analyses in high-risk diabetic subjects do not reflect tolerability issues with the combination treatment, which could increase discontinuations in this population.9,12,13 The safety results of this study should be interpreted with caution since the study was not powered to detect very rare adverse events and was of relatively short duration.
Few studies have compared the efficacy of the combination of ezetimibe/simvastatin 10/20 mg with both atorvastatin 20 mg and rosuvastatin 10 mg in the same trial, and this is the first trial to assess these lipid-lowering therapies at these doses in a very-high-risk diabetic population in a trial approximating clinical practice. These results provide evidence that switching to combination ezetimibe/simvastatin 10/20 mg provides a well-tolerated lipid-lowering effect in diabetic hypercholesterolaemic subjects who have not achieved a goal of LDL-C <70 mg/dL (1.81 mmol/L) while on simvastatin 20 mg or atorvastatin 10 mg.
Footnotes
Acknowledgements
Conflict of interest
J.B.R.’s institution received grant support and support for travel to meetings related to the study from Merck. J.G.J. received travel support from Merck and MSD. V.P. and H.V. have no conflicts to declare. M.E.H., R.M., G.M., P.B. and J.T. are employees of Merck or MSD Belgium (RM) and may own stock or hold stock options in the company.
Funding
The trial was funded by Merck Sharp & Dohme Corp., Whitehouse Station, NJ, USA.