
Abstract
Objective:
Hyperglycaemia enhances the risk of cardiovascular events and death, while high-density lipoprotein cholesterol (HDLc) is protective. Information on these associations among the elderly population is scanty. We applied a cardiometabolic risk index (CMRI) based on HDLc and fasting plasma glucose (FPG) in an elderly Swedish population.
Methods:
In total, 432 75-year-olds were followed for 10-year mortality. The impact of risk factors on survival was analysed using Cox regression.
Results:
HDLc (mmol/l; median and interquartile range) was 1.6 (1.3–2.0) in women and 1.4 (1.2–1.5) in men, while FPG was 5.9 (5.5–6.6) and 5.9 (5.5–6.5). Some 89 persons were at high risk according to CMRI, and 163 persons died. FPG was related to mortality in women (HR; 95% CI: 1.23; 1.10–1.37) and there was a similar trend in men (1.08; 1.00–1.17; p = 0.061). Increasing HDLc was protective in men (0.38; 0.19–0.77) but not in women (0.77; 0.45–1.29). CMRI was related to mortality in both genders even after adjustment for established risk factors (1.79; 1.14–2.79; p = 0.011).
Conclusions:
The CMRI helps identify elderly subjects at risk and may serve as a cost-effective risk prediction tool.
Introduction
Type 2 diabetes is a well-recognised risk factor for atherosclerosis. It is apparent that during the prodromal period prior to the development of overt diabetes, several years of impaired glucose tolerance also enhances cardiovascular (CV) risk. Thus, the ongoing global increase in the prevalence of glucose perturbations 1 predicts a subsequent increase in diabetes-related CV events2,3 and rising health care costs. Early detection and management of glucose perturbations must therefore have high priority. These conditions are often associated with obesity, hypertension and dyslipidaemia including high triglycerides (TG) and low high-density lipoprotein cholesterol (HDLc). CV risk factors tend to cluster, triggering the development or progression of established atherosclerosis and precipitating CV events. This clustering has been referred to as the metabolic syndrome (MetS) as summarised by Alberti et al. 4 and Grundy et al. 5 The association between the components of the MetS, morbidity and mortality is well established in middle-aged people, but less is known about their importance in the elderly, who constitute a rapidly increasing proportion of the population. Accordingly, further investigations are needed to estimate risk factors for CV events, alone or in combination, among elderly people in order to explore their importance, taking potential gender differences into account.
The Cardiometabolic Risk Index (CMRI) introduced by Anselmino et al. incorporates easily available clinical variables such as age, fasting plasma glucose (FPG) and HDLc, and has been shown to have prognostic value in middle-aged populations.6,7 However, it is still unclear whether it could be used to stratify CV risk in elderly subjects.
The aim of this study was to test the hypothesis that the CMRI would contribute important prognostic information beyond that revealed by single risk factors in an elderly population.
Methods
Study population
The city of Västerås (130,000 inhabitants) situated in central Sweden has a population considered socioeconomically representative of the country. In 1997 a random sample of 618 of the 1100 inhabitants born in 1922 (i.e. 75 years old) were invited to take part in a CV health survey. The final number of participants was 432 (70% of those invited; 222 women; 210 men). Reasons for non-participation were unknown (n = 46) or distributed as follows: never reached (n = 29), died before examination (n = 2), language or logistical problems (n = 27), locomotive impairment (n = 28) or unwilling due to diseases under treatment (n = 54). A detailed description of patient selection and study design has been presented elsewhere. 8 Information of importance for the present study is described below.
Clinical and laboratory investigations
Recorded information included: history of CV and/or pulmonary diseases, diabetes mellitus, ongoing medication, body mass index (BMI), heart rate, blood pressure and lifestyle habits such as self-reported smoking.
Venous blood was sampled in the fasting (≥ 12 h) state. Blood glucose was determined on an automatic analyser by a glucose dehydrogenase method (Cobas Mira, Roche Diagnostics Ltd, Rotkreuz, Switzerland). FPG was computed from venous whole blood glucose using the formula: FPG = 0.558 + 1.119 * whole blood fasting glucose. 9 Total serum cholesterol, TG and HDLc levels were determined enzymatically with an automated analyser (Hitachi 717, Boehringer Mannheim, Mannheim, Germany). Low-density lipoprotein cholesterol (LDLc) was calculated according to the Friedewald formula 10 as LDLc = Total cholesterol – (TG/2.2 + HDLc). Such values could not be obtained in eight persons since this formula does not permit an accurate estimation of LDLc if the TG level is > 4.2 mmol/l.
Blood pressure was recorded following 5 min of supine rest and reported to the nearest 5 mmHg. Waist circumference was measured in the horizontal plane midway between the inferior margin of the ribs and the superior border of the iliac crest.
Information on previous myocardial infarction (MI), stroke, and diabetes was based on the self-reported case history and verified by medical records. Hypertension was defined by physician-diagnosed high blood pressure in combination with regular blood pressure-lowering treatment. Smoking status was classified as non-smoker, former smoker or current smoker.
Risk factors for MetS were assessed according to the recommendation by the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III). 11
Cardiovascular prognosis
The CMRI defined by Anselmino et al. was applied to explore if it could be useful for risk prediction in an elderly population. 6 The CMRI is the output from a single hidden layer neural network with the following input variables: FPG, HDLc and age (a constant equal to 75 in the present study). This neural network model can be considered a generalisation of the logistic regression model (see appendix for a mathematical formulation), since the relationship between the latent variables and the output is the logistic function. Originally constructed as a measure of diabetes risk, the CMRI turned out to be an accurate predictor of future death, with value above 0.5 indicating high risk. For a complete description of the neural network model see Anselmino et al. 6
Prospective follow-up
All-cause mortality served as primary endpoint. The study cohort was followed from the index examination in 1997 until 31 December 2007 or to the first primary endpoint, resulting in a median follow-up of 10.6 years. Dates and reasons of death were obtained from the Swedish population register and the Swedish National Cause of Death register. No participants were lost to follow-up. The registers were linked to individuals participating in the study via the unique personal identification number allocated to all Swedish citizens. The 10th revision of the International Statistical Classification of Diseases was used to identify primary causes of death. In the present study causes of death were grouped into 10 categories. However, the study was not powered to analyse specific causes of death.
Statistical analysis
Continuous variables were summarised by median and interquartile range and categorical variables by counts and proportions. The Wilcoxon Mann–Whitney’s rank sum test was used to compare continuous, and Fisher’s exact test to compare categorical, variables. Crude prospective associations of FPG, HDLc, CMRI and all-cause mortality were analysed in men and women separately using Cox proportional hazard regression (PHREG) models to study gender-related differences in the strength of association between survival, CMRI. Gender and its interaction with CMRI were included in the model. In case of a non-significant interaction (two-sided p > 0.05) a pooled analysis was performed adjusting for gender.
Multivariable Cox PHREG analyses were performed to assess the independent associations between CMRI and all-cause mortality, controlling for confounding prognostic variables and pooling for gender if non-significant gender*CMRI interaction. Confounding prognostic variables were selected using a best subset approach with Akaike information criterion (AIC) as performance measure. The AIC is defined as, AIC= -2ln(L) + 2*k, where L is the maximised value of the likelihood function for the estimated model (in this context the Cox PHREG model) and k is the number of estimated parameters. Given a set of candidate models for the data, the preferred model is the one which minimises the AIC value. The predictive ability of the CMRI was assessed by the time-dependent area under the receiver operating characteristic (ROC) curve, AUC t = P[Zi > Zj |Di(t) = 1, Dj(t) = 0], where Zi and Zj are independent predicted risk scores, under the Cox PHREG model, for subject i and j and D.(t) = 0/1 is an indicator variable indicating whether an event has occurred by a specific time t. 12 The proportional hazard assumption was assessed by visual inspection of the log[-log(cumulative survival)] for categorical and continuous variables, the latter after categorisation. Cumulative survival was estimated by means of the Kaplan–Meier method. Ten-year survival in men and women stratified by dichotomised CMRI; low/normal (≤ 0.5) and high (> 0.5) was illustrated by Kaplan–Meier survival curves.
A two-sided p-value < 0.05 was regarded as statistically significant. Minitab version 16 and SAS version 9.2 was used for the analyses.
Ethics
The study was approved by the ethics committee at Uppsala University, Sweden, and performed in accordance with the Declaration of Helsinki. All study subjects gave their informed consent.
Results
Table 1 presents baseline characteristics of the participants by gender. Besides expected differences in waist circumference and HDLc levels, women had significantly higher BMI and systolic blood pressure. They also had significantly higher total cholesterol and LDLc but lower prevalence of previous MI and established coronary artery disease (CAD). At the time of the index examination statin use was low, without any observed difference between genders (3.3% in men and 3.1% in women). No gender difference was observed in treatment of hypertension (27% men and 29% women). There were no gender-related differences in the FPG levels.
Baseline characteristics of the study population stratified by gender. Data are expressed as median (lower, upper quartile) and number (%). a
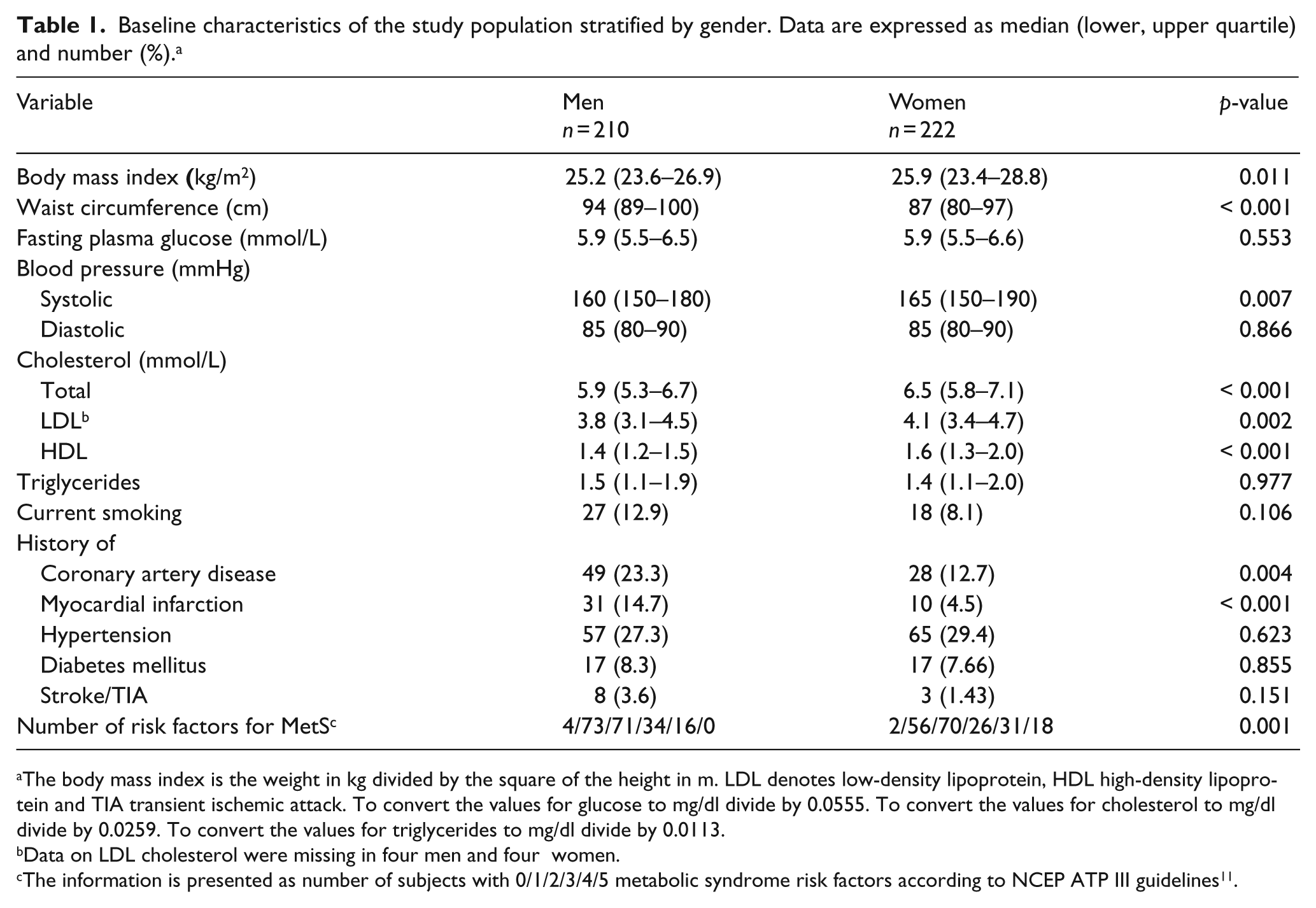
The body mass index is the weight in kg divided by the square of the height in m. LDL denotes low-density lipoprotein, HDL high-density lipoprotein and TIA transient ischemic attack. To convert the values for glucose to mg/dl divide by 0.0555. To convert the values for cholesterol to mg/dl divide by 0.0259. To convert the values for triglycerides to mg/dl divide by 0.0113.
Data on LDL cholesterol were missing in four men and four women.
The information is presented as number of subjects with 0/1/2/3/4/5 metabolic syndrome risk factors according to NCEP ATP III guidelines 11 .
Mortality and cardiovascular risk predictors
During a median follow-up of 10.6 years (range 0.2–11.0 years) 163 individuals (38%) died, of whom 98 (47%) were men and 65 (29%) women. The total number of person-years of follow-up was 3918, implying a number of deaths per 1000 person-years at risk of 47 (men 55, women 31). Overall, 77 of the deaths were due to CV reasons and 81 non-CV (including 40 attributed to malignancy). The cause of death was unknown in five cases. Mortality among the 185 invited non-participants was considerably higher (total = 67%; men = 74% and women = 46%) than among the participants (data on file).
Comparing baseline characteristics for survivors and non-survivors by gender, non-survivors had a somewhat higher risk factor profile. Women with unfavourable outcome were more often smokers, while men had a more frequent history of CV disease and hypertension compared with their surviving counterparts (data not shown). Some 48 (22%) women and 41 (20%) men were characterised as high-risk individuals by the CMRI (> 0.5). Cumulative survival according to gender and high risk (yes/no) is presented in Figure 1.
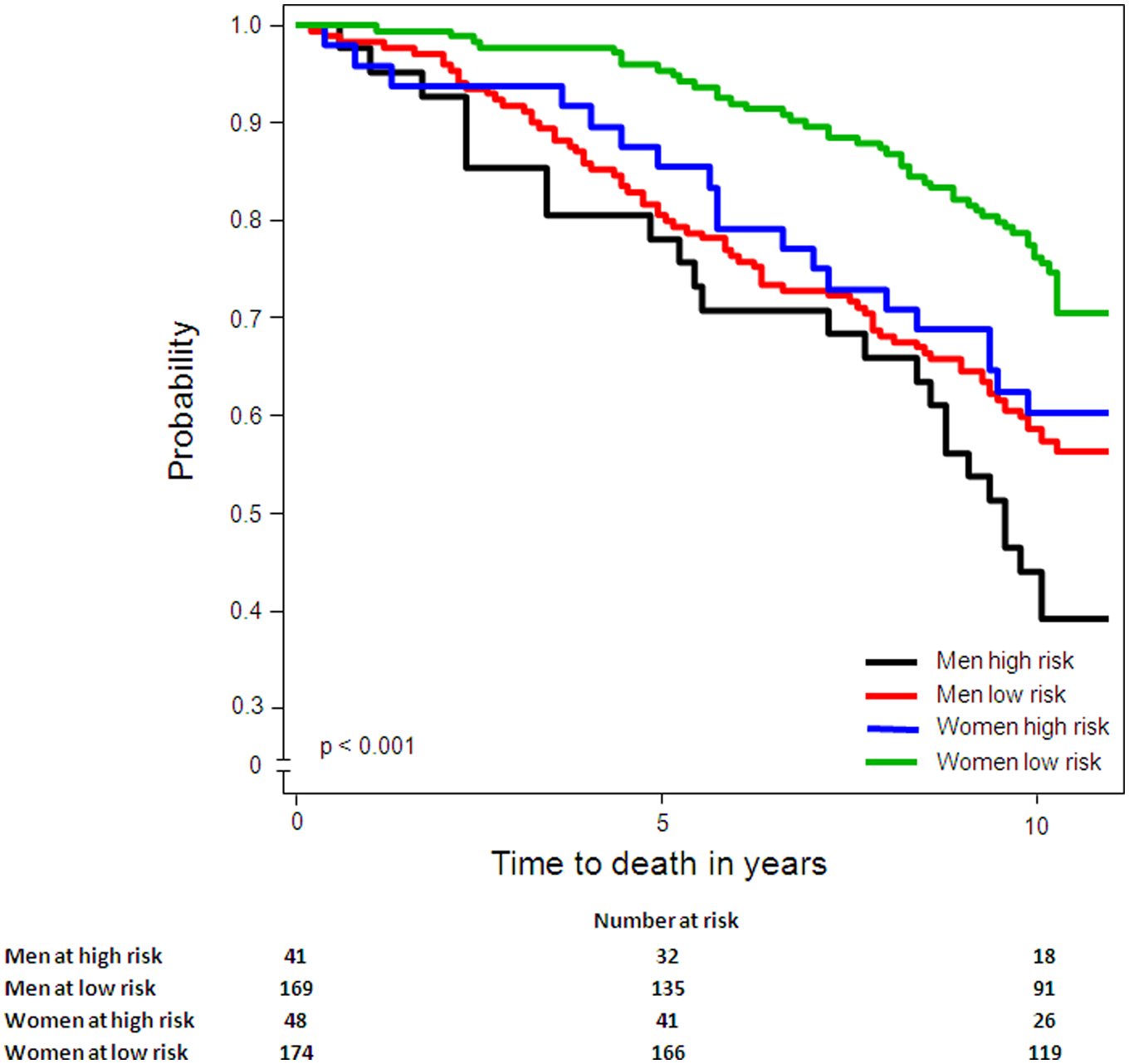
Kaplan–Meier curves showing cumulative survival according to gender (men; n = 210 and women; n = 222) and the Cardiometabolic Risk Index (high/low).
FPG was significantly related to mortality in women (hazard ratio (HR): 1.23, 95% confidence interval (95% CI): 1.10–1.37) with a similar trend in men (HR: 1.08, 95% CI: 1.00–1.17). HDLc had a significantly inverse effect on mortality in men (HR: 0.38, 95 CI%: 0.19–0.77) but not in women (HR: 0.77, 95% CI: 0.45–1.29; see Table 2). Ten-year all-cause mortality categorised by FPG (below/above median) and HDLc (below/above median) are shown in Figure 2 for men and women separately.
Crude (gender specific and pooled) and adjusted prospective associations between all-cause mortality and cardio-metabolic (CM) risk factors given as hazard ratios (HR) with 95% confidence intervals (95% CI). a
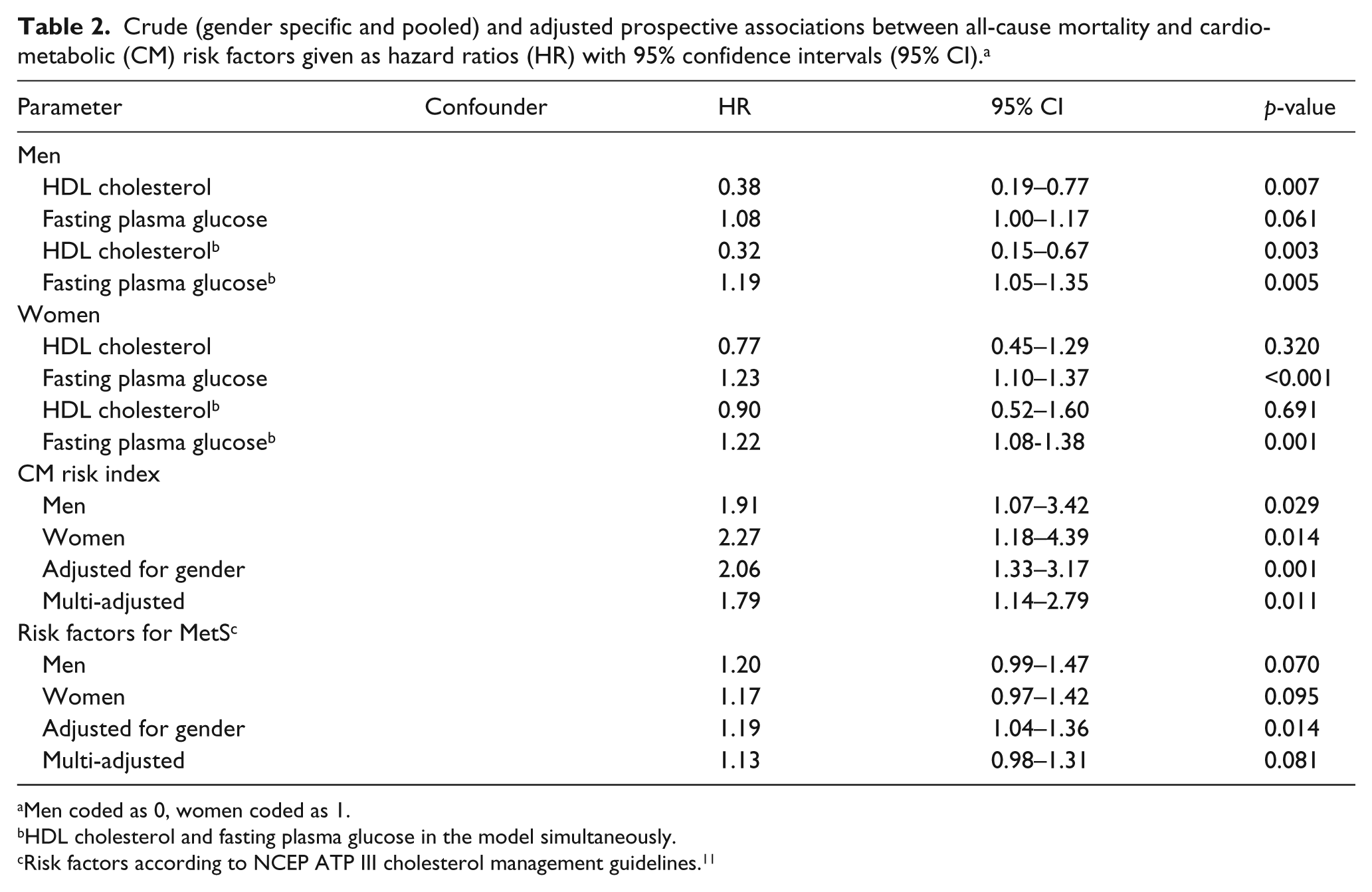
Men coded as 0, women coded as 1.
HDL cholesterol and fasting plasma glucose in the model simultaneously.
Risk factors according to NCEP ATP III cholesterol management guidelines. 11
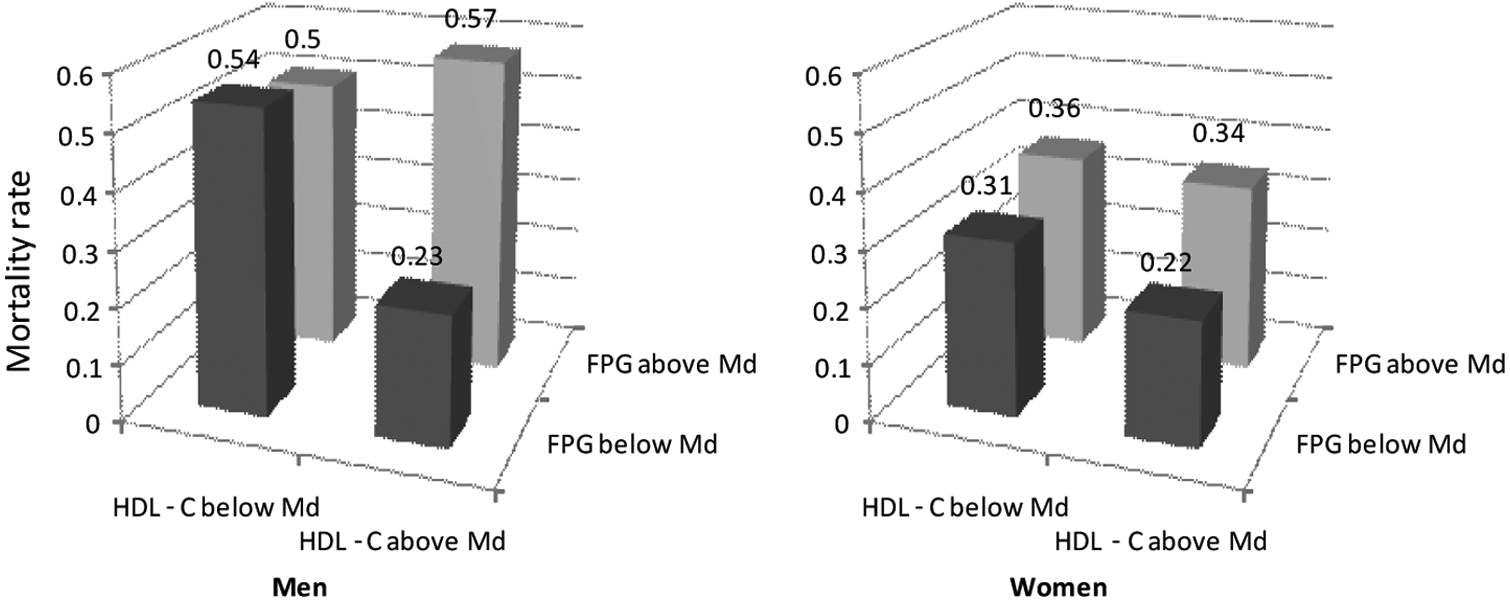
10-year all-cause mortality in men (n = 210) and women (n = 222) categorised by fasting plasma glucose (below/above median = 5.93 mmol/l) and HDL cholesterol (below/above median = 1.46 mmol/l).
Crude and adjusted HR (95% CI) for the associations between mortality and CMRI, estimated by multivariable Cox PHREG regressions, are presented in Table 2. The adjusting variables were, besides gender, previous MI, known hypertension and current smoking, the only significant risk factors applying a best subset approach using AIC as performance measure. Both crude and adjusted HR for CMRI was significant. As shown in Figure 3 the CMRI increased AUC t =10 yrs from 0.57 to 0.68 when added to the prognostic variables previous MI, known hypertension, current smoking and gender. There were no significant interactions between gender and FPG, HDLc or CMRI, while the interaction between FPG and HDLc was significant in men (p = 0.041) although not in women (Figure 2).
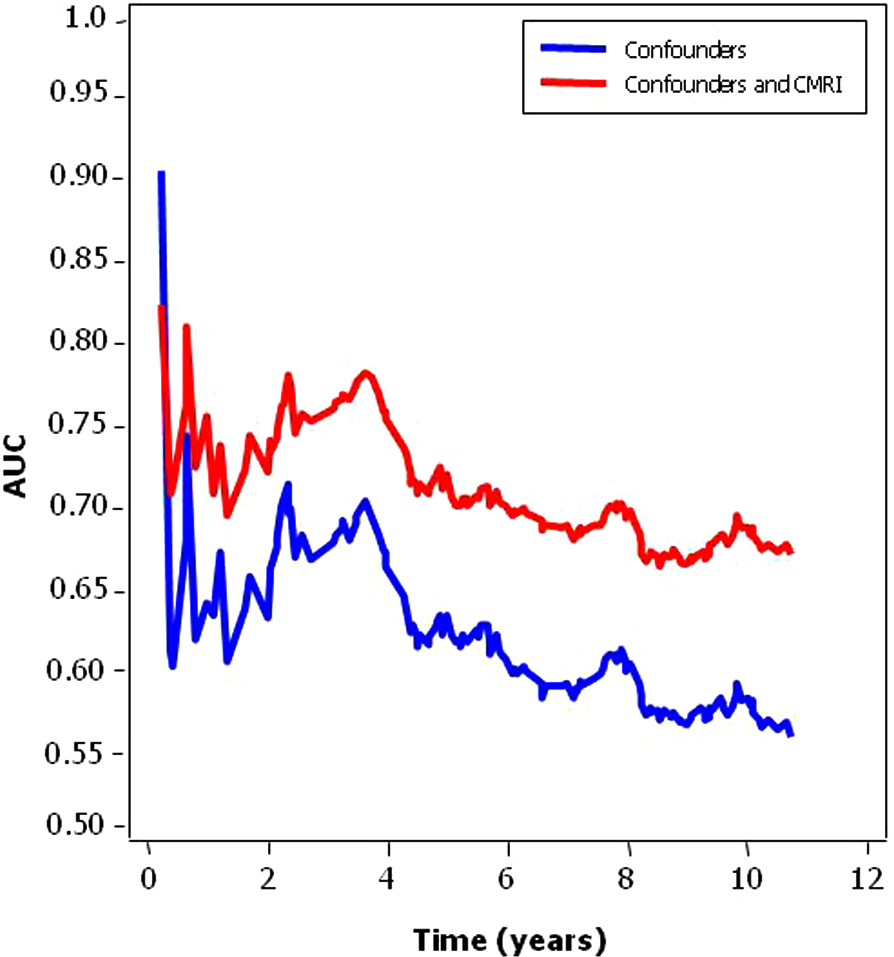
Time-dependent area under the ROC curves for two models: (1) confounders only (previous myocardial infarction, known hypertension, current smoking and gender) and (2) the cardiometabolic risk index (CMRI) and confounders.
We used the number of MetS risk factors according to NCEP ATP III 11 to predict 10-year survival. The crude prospective association with all-cause mortality was significant, but after adjusting for gender, previous MI, known hypertension and current smoking, the association vanished (Table 2).
Discussion
This study confirmed the hypothesis that a risk prediction model based on two easily available biomarkers, fasting glucose and HDLc, contributes important prognostic information beyond that revealed by single risk factors in an elderly population. These findings were robust when adjusted for existing CV disease and other established CV risk factors.
An increase in CV risk in the elderly is to a large extent explained by the influence of age itself, but may also relate to prolonged exposure to risk factors, as illustrated by the improved prognosis seen in the HYVET trial following adequate blood pressure control in patients aged ≥ 80 years. 13 Gender is, besides age, an important variable when estimating total CV risk. As a general rule females are at less risk before menopause, following which the CV risk successively equals out. 14 Comprehensive data on risk factors contributing to CV disease, including their coexistence and combined power to accurately predict mortality, are scarce in aging populations. This study was conducted to shed some light on this knowledge gap. A problem when performing such analyses is the lack of algorithms for risk stratification tailored specifically for the elderly. In consideration of the great importance of gluco-metabolic risk factors, the CMRI, originally developed for a younger population, 6 was used to evaluate whether easily available information would keep its prognostic value even in an elderly population, an assumption that proved to be correct. Biomarkers associated with poor outcome (FPG and HDLc) were used in the risk prediction model. HDLc was chosen as a relatively stable variable independent of lipid-lowering treatment. The CMRI was an efficient independent predictor of all-cause mortality in both genders, predicting poor outcome even after adjusting for traditional CV risk factors such as smoking, hypertension and previous MI. Thus the CMRI may be considered as a valuable tool when evaluating the cumulative individual risk in elderly subjects and targeting their treatment.
The reason to focus on risk factors influenced by glucose metabolism is the propensity for an increasing prevalence of such perturbations by age. 15 By applying a gender perspective, interesting observations were made on differences in metabolic risk factors, their interactions and predictive abilities. The differences in risk factor profile were consistent with previously reported data. 16 Although elderly women had higher BMI, waist circumference and worse serum lipid profile, they less often presented a history of CAD and MI compared with men. Despite their more advanced risk factor profile and, at their present age, lack of beneficial effects of ovarian hormones, their all-cause mortality was lower. 17 The levels of FPG did not differ significantly between the two genders, and this variable was strongly associated with an unfavourable outcome in women but not in men. In contrast, the HDLc levels were higher in women. Their protective effect 18 was, however, exclusively seen among men, predominantly in those with normal FPG. Due to lack of information it is still debated whether low HDLc is an independent predictor for all-cause mortality in elderly subjects. In some respects our findings support results from the Bronx Aging Study 19 and from an elderly Finnish population showing that low HDLc was independently associated with mortality in elderly men. 20 However, Zambon et al. presented contradictory results in elderly Italians, 21 in whom low HDLc was a predictor of mortality in elderly women but not men. Unfortunately, for further comparisons, data on the association between FPG and HDLc were not presented in any of the previous studies. Potential explanations for the discrepancies in the Italian study were that the population was somewhat younger and followed for a shorter period of time. It may be hypothesised that rapid changes of risk predictor profiles may appear at old age, not least because gluco-metabolic perturbations may deteriorate quickly. High FPG levels are strong predictors of mortality in both genders, and in particular related to CV risk in women.22,23 Thus it is reasonable to assume that our results are applicable to people at or above the age of 75 years. The practical implication is that adequate glucose control seems important both in men and women, with a particular attention paid to men with low HDLc. Introduction of HDLc-increasing agents may be considered to manage this risk, but this needs confirmation in randomised trials.
Risk prediction is a prerequisite for therapeutic attempts to lower the likelihood for an unfavourable outcome. Although such interventions may seem less attractive late in life, pharmacological treatment has proven beneficial in an elderly population, as demonstrated by the HYVET study 13 randomising hypertensive patients with a mean age of 84 years to strict blood pressure-lowering treatment or placebo for a median of 1.8 years. In the actively treated group there was a 21% reduction in all-cause mortality from 59.6 to 47.2 events/1000 patient years. Although a mortality reduction was not confirmed by a recent meta-analysis of randomised controlled trials of antihypertensive treatment in patients ≥ 80 years it revealed significant reductions of the risk of stroke by 35%, CV events by 27% and heart failure by 50%. 24 This should encourage further research to provide a basis for the impact of therapeutic strategies intended to improve the outcome in elderly populations. The present findings provide a base for targeting gluco-metabolic risk factors, and the prognostic index may serve as a tool for selecting subjects for such trials.
Study limitations and strengths
The relatively small number of subjects may be seen as a limitation. Moreover, although participation rate was high considering the character of the study it has, in the light of the mortality among the non-participants, to be acknowledged that the studied population represents a group at a proportionately lower risk than the total population. It is, however, reasonable to assume that the healthier group could benefit most from risk prediction and management, and that unhealthy people are already known to the health care providers.
The uniform age, even gender distribution, well-defined area of recruitment and long period of follow-up, in combination with a relatively high mortality, may be considered as a strength. Still, there may be difficulties in generalising the findings to other populations even if in the same age range; however, it is likely that the results are applicable in elderly Caucasian populations.
Conclusions
Emphasis should be placed on assessment of cardiometabolic risk factors and their clustering in elderly populations, in particular as regards their lipid profile and glucose perturbations, important markers of an increased risk for mortality. The CMRI helps in identifying individuals in need of intervention, and may serve as a cost-effective tool only requiring a fasting blood sample for risk prediction. The present findings should encourage further research to provide a basis for the impact of therapeutic strategies intended to improve the outcome in elderly populations.
Footnotes
Appendix
The CMRI is the output of a single hidden layer feed-forward Artificial Neural Network (ANN). The study population in EuroHeart survey on Diabetes and the Heart was used to select the input variables, number of hidden variables and to estimate the parameters of the ANN; for a more thoroughly description see Anselmino et al. 6
Mathematically, CMRI is given by the following formulae:
h1 = tanh(−13.71 + 1.75*FPG + 0.029*Age − 0.22*HDL–c)
h2 = tanh(−21.42 + 3.47*FPG)
h3 = tanh(10.12 − 0.16*Age)
h4 = tanh(5.38 − 1.69*FPG + 3.59*HDL-c),
where hi denotes variable i and tanh(x) = [exp(x) − exp(−x)]/[exp(x) + exp(−x)].
The CMRI is then given by:
CMRI = Prob(High Risk) = y3/( y1 + y2 + y3), where
y1 = [1 + exp(−(−1.51 − 1.88*h2 + 0.53*h3 + 0.38*h4))]−1
y2 = [1 + exp(−(−2.06 − 2.76*h1 + 1.46*h2 − 0.31*h3))]−1
y3 = [1+exp(−(−0.22 + 1.84*h1 − 0.93*h4))]−1
Acknowledgements
The authors are grateful to Professor Jerzy Leppert for getting full access to the database and Doctor Pär Hedberg for confirming the causes of death.
Funding
The study was supported by the Swedish Heart and Lung Foundation and AFA Insurance.
Conflict of interest statement
None of the authors has any financial interests, apart from research funding as outlined above. All authors have read and agree to the manuscript as written.