
Abstract
Metabolic syndrome (MetS) is defined as a cluster of numerous cardiovascular risk factors, which encompasses obesity, dyslipidaemia, insulin resistance and hypertension. Patients with MetS are more prone to developing cardiovascular events than other patients. To date, several approaches such as physical exercise, dietary control and invasive and non-invasive therapeutic interventions for dyslipidaemia, hypertension and insulin resistance have been used to manage MetS. However, there is a progressive elevation in the incidence of fatal and non-fatal cardiovascular events due to the increased prevalence of obesity and diabetes. Percutaneous coronary intervention has emerged over the last few years as an effective revascularisation strategy for those with coronary artery disease, in parallel with the development of effective anti-platelet medications and newer drug-eluting stents. In recent years, considerable research efforts have been undertaken to elucidate the pathophysiology of re-stenosis and develop strategies to prevent re-stenosis following percutaneous transluminal coronary angioplasty and stent implantation. Although the rate of stent re-stenosis and target-lesion revascularisation has been reduced, there is little information in the literature on the outcome of MetS in the pathophysiology of re-stenosis. In this review article, we summarise the recent development and progress on re-stenosis and the role of drug-eluting stents, particularly in MetS.
Introduction
Metabolic syndrome (MetS) is defined as the cluster of physiological and metabolic abnormalities including obesity, impaired glucose tolerance, hyperinsulinaemia or type 2 diabetes mellitus, dyslipidaemia (a combination of low levels of high-density lipoprotein cholesterol and high levels of triglycerides) and hypertension. 1 According to the National Cholesterol Education Program – Adult Treatment Panel III (NCEP-ATP III), metabolic syndrome is defined as a combination of any three of the following features: 1. Abdominal obesity (waist circumference >102 cm in males and >88 cm in females); 2. increased serum triglycerides (≥150 mg/dl); 3. decreased HDL cholesterol (<40 mg/dl in males and <50 mg/dl in females); 4. hypertension (≥130/≥85 mm Hg); and 5. hyperglycaemia (fasting glucose ≥110 mg/dl). 2 This disorder, previously termed ‘syndrome X’ by Reaven and ‘insulin-resistance syndrome’ by others, has currently become popular as ‘MetS’. The incidence of MetS is on the increase in proportion to the increased incidence of both obesity and diabetes. Those with diabetes with or without MetS have a higher prevalence of coronary artery disease (CAD) and a higher tendency to suffer from silent myocardial ischaemia and infarction. Currently, MetS affects over a quarter of the population in developed countries, and its prevalence is increasing dramatically. 3
To date several interventional approaches, both invasive and non-invasive, have been designed to manage coronary events in MetS. However, following coronary interventions such as angioplasty and stent implantation in patients, re-stenosis is considered as a common and severe complication. In re-stenosis, damage to the blood vessel wall activates an inflammatory response, which culminates in neo-intimal hyperplasia, which is markedly enhanced in the presence of MetS. 4 In the pathogenesis of MetS-associated re-stenosis, the release of inflammatory adipocytokines such as leptin, adiponectin, tumour necrosis factor-α (TNF-α), plasminogen activator inhibitor-1 (PAI-1), resistin and interleukins 1 and 6 is known to play an important role (Figure 1).
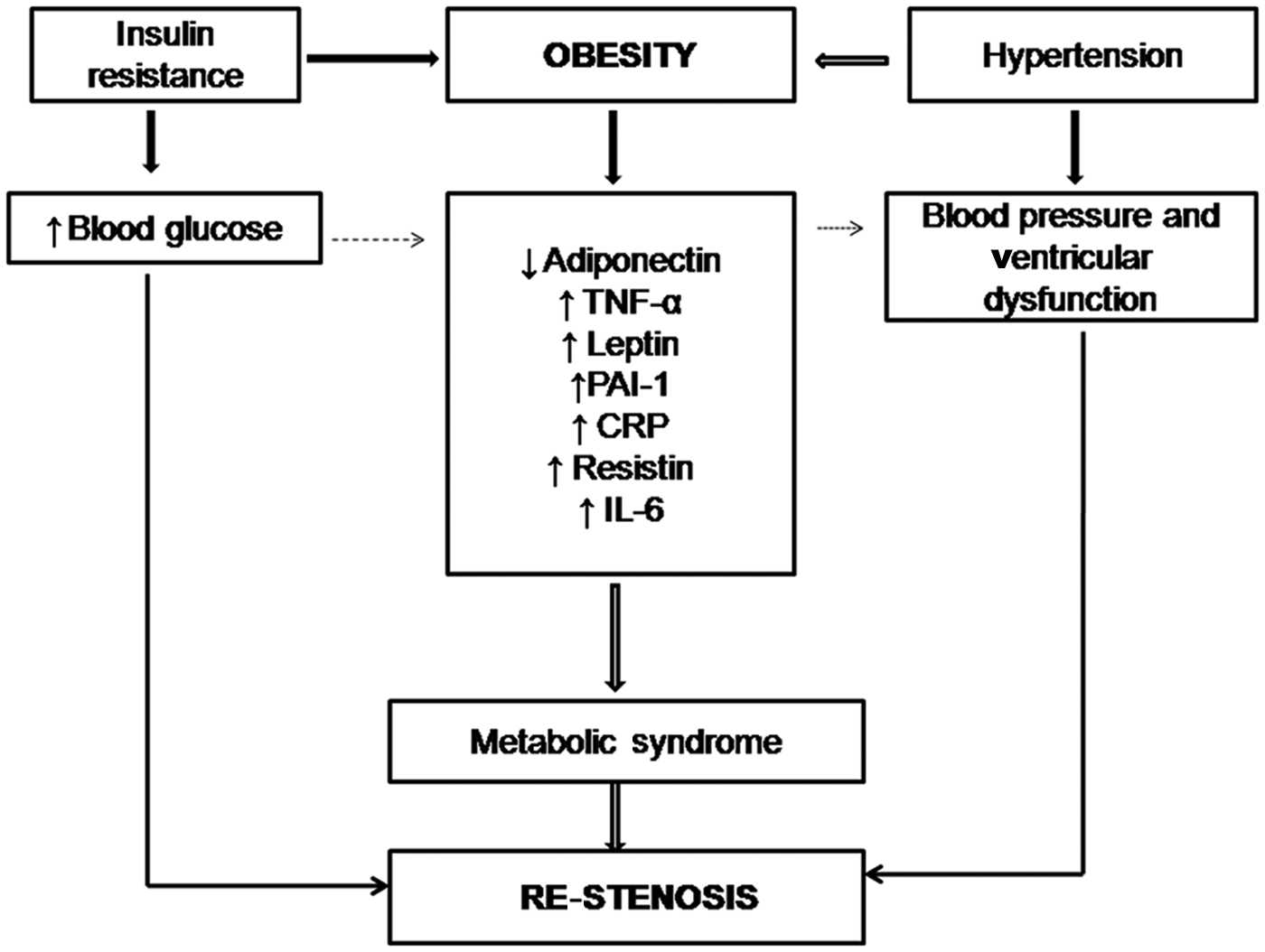
Role of metabolic syndrome in re-stenosis.
Background to angioplasty and re-stenosis
In 1977, Andreas Gruentzig introduced the technique of percutaneous transluminal coronary angioplasty (PTCA), commonly termed angioplasty, with a high initial rate of success (approximately 90%). Angioplasty is a safe and effective way of opening clogged coronary arteries. 5 Initially, angioplasty was performed only with balloon catheters, but current practice is to implant small, metallic, spring-like ‘stents’, which serve as scaffolds in maintaining the patency of the vascular lumen. 6 Angioplasty, together with stenting, is widely used worldwide as an alternative to medical therapy and bypass surgery for improving blood flow to the tissues. However, re-stenosis is one of the major limitations associated with angioplasty and stenting (Figure 2).5,6 Re-stenosis means the reoccurrence of stenosis, and thus restriction of blood flow to the organ again. 7 Balloon inflation breaks down atherosclerotic plaque and activates platelets that release mitogens, including thromboxane A2, serotonin and platelet-derived growth factor, which promote smooth muscle cell proliferation leading to hyperplasia. Consequently, many activated smooth muscle cells migrate to the intima. A dysfunctional endothelium might also contribute to smooth muscle proliferation and migration as healthy endothelial cells inhibit smooth muscle cell growth through nitric oxide production. Thereafter, collagen fibres and extracellular matrix accumulate leading to re-stenosis. Re-stenosis occurring after the use of stents is referred to as ‘in-stent re-stenosis’. 8 Initially, new tissue grows inside the stent, which facilitates the smooth flow of blood over the stented area without clotting. Afterwards, scar tissue may form beneath the new healthy lining and, in 25% of patients, this growth can obstruct blood flow and produce a blockage. 6 Generally, in-stent re-stenosis is typically observed within 6–8 months, and diabetics are more prone to its development. Re-stenosis rates of up to 60% have been reported after the placement of stents. 6
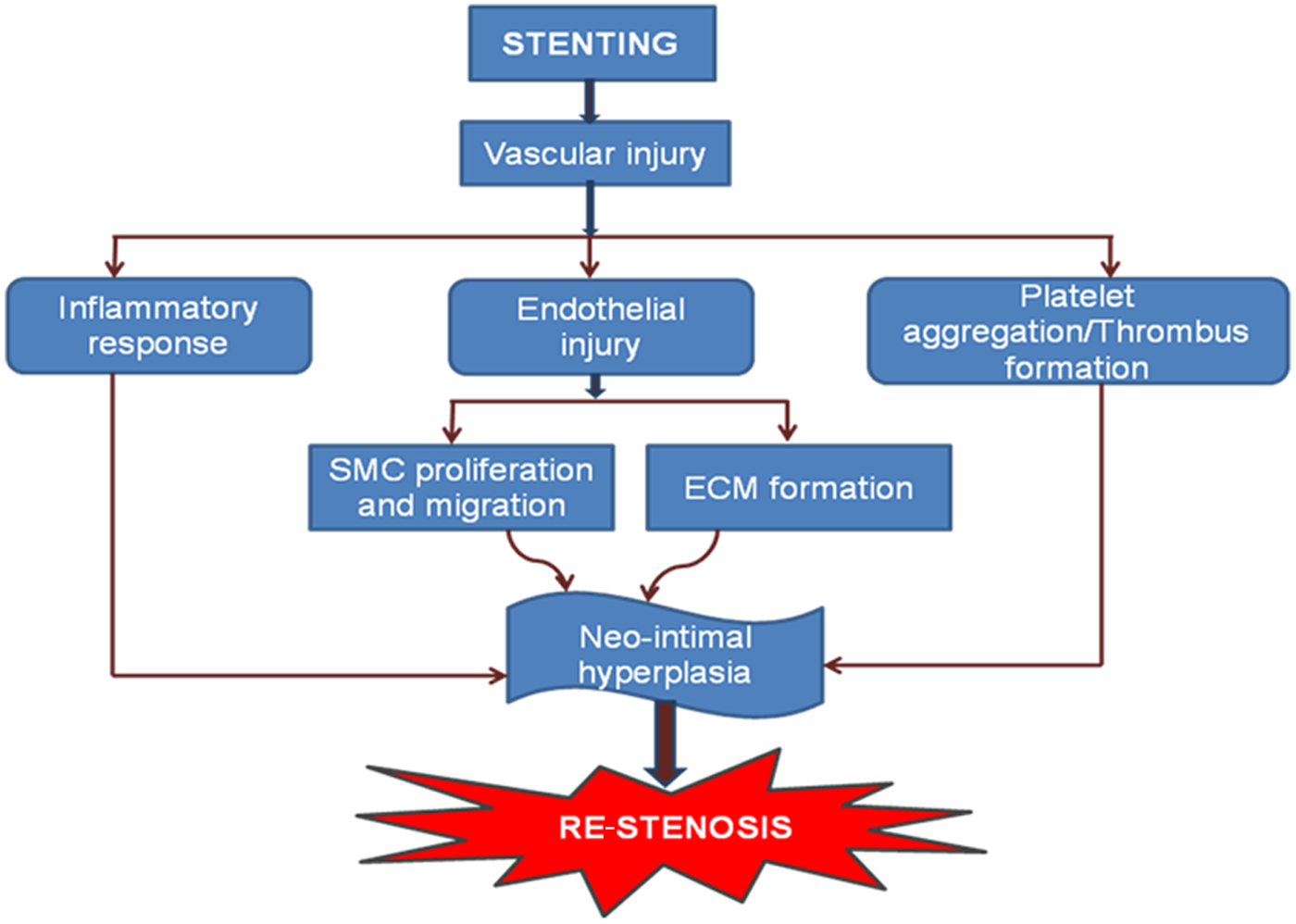
Pathways of development of re-stenosis.
In designing strategies to reduce the rate of in-stent re-stenosis, it is important to identify and understand the predisposing factors. Currently, these can be divided into patient-related, procedure-related and lesion-related factors. Patient-related factors include MetS, a history of smoking and one or more previous episodes of re-stenosis. Patients with MetS, and even those with isolated type 2 DM, have been demonstrated to be at greater risk of re-stenosis. 9 The effect of smoking on re-stenosis is controversial. Some studies have failed to show any significant difference in the rate of re-stenosis between smokers and non-smokers,10,11 while others have concluded a beneficial re-stenosis profile on smoking cessation12,13 and yet others have paradoxically reported decreased rates of re-stenosis among smokers. 14 Despite such conflicting results, it is expected that smoking cessation would be beneficial in preventing re-stenosis as it would prevent a further progression of CAD. A past history of re-stenosis suggests a greater probability of in-stent re-stenosis during a subsequent stent implantation, due to the risk of CAD progression. 15 Previous studies have reported the development of re- stenosis multiple times within the same patient. 16 The procedure-related factors include the number of stents being used, length of the stent and stent overlie and malapposition of stents. The stent design may have a significant impact on the severity of neo-intimal hyperplasia. 17 In-stent re-stenosis was observed by Santos et al. 18 and attributed to stent malapposition seven years after a bare metal stent insertion. Lesion-related characteristics include small vessel size, long lesion length, formerly revascularised chronic total occlusions and severity of pre-treatment, as well as post-treatment lesion stenosis.
Pathophysiology of in-stent re-stenosis
The basic mechanisms involved in in-stent re-stenosis are elastic recoil, arterial remodelling and neo-intimal hyperplasia. 19 Elastic recoil is the immediate shrinkage of vessels after percutaneous coronary intervention (PCI) due to the elastic properties of the arterial wall, usually observed within 24 h of the procedure. Arterial remodelling is a process of local contraction of the arterial wall and narrowing of the lumen at the injured vascular segment, and may be related to the healing process or the interaction between endothelial cells and non-laminar blood flow. In neo-intimal hyperplasia, proliferation and migration of smooth muscle cells usually takes place from the media to intima. The occurrence of negative remodelling and neo-intimal proliferation usually require weeks to months. Elastic recoil and negative arterial remodelling may be the main causes of re-stenosis, but can be down-regulated by the use of stents. The third mechanism, neo-intimal hyperplasia, is the predominant mechanism in the pathogenesis of in-stent re-stenosis. 19
Currently, several approaches employing gene therapy to prevent or ameliorate neo-intimal hyperplasia are under evaluation. Adenoviruses have been deployed as vectors for gene delivery to the areas of vascular injury, and the genes so delivered encode for proteins which are either cytotoxic or cell cycle-inhibitory in nature. The mode of gene delivery may be by either endoluminal administration of DNA containing solutions or direct contact with the arterial wall using a DNA-eluting polymer-coated stent. 20 Another approach that has been suggested to reduce in-stent re-stenosis is the administration of matrix metalloproteinase (MMP) inhibitors that inhibit smooth muscle cell migration and proliferation. However, this technique has not been documented in the prevention of in-stent re-stenosis. 21 Radiation therapy has evoked significant interest and has been found promising. Both intraluminal irradiation with a beta or gamma emitter sited within the coronary vessel using afterloading techniques and the use of a radioactive stent (brachytherapy) have been evaluated, and found successful. Radiation therapy can be applied to prevent the first episode of in-stent re-stenosis as well as to inhibit recurrent in-stent re-stenosis. Waksman et al. described a significant reduction in neo-intimal formation in pig coronary arteries treated with gamma-irradiation (192Ir) or beta-irradiation ( 90 SR/Y) prior to stent placement, 22 while Hehrlein et al. were the first to use stents to deliver radiation in an animal re-stenosis model. 23 However, radiation therapy has now been superseded by the availability of drug-eluting stents (DES) 24 , the reasons for which are elucidated below.
Coronary stenting
In 1987, Sigwart and colleagues undertook the first human stent placement clinical trial, 25 and following that the US Food and Drug Administration (FDA) approved the first phase 1 trial using an intra-coronary artery stent. In 1993 the FDA approved the use of the Gianturco–Roubin stent for acute or threatened closure during coronary intervention, and the Palmaz–Schatz balloon-expandable stent (Cordis Corporation, Warren, NJ, USA) in 1994 for primary patient treatment. 26 Worldwide, approximately 25 different stent designs are now employed clinically, seven of which are commercially available for use in the USA. 5 Stents may be categorised by their type of delivery system (self-expanding or balloon-expandable), composition (stainless steel, platinum–iridium, cobalt-based alloy, tantalum, nitinol, biodegradable polymer) or configuration (tubular mesh, slotted tubes and coils). The majority of stents approved by the FDA and presently undergoing FDA evaluation are balloon-expandable. These stents are mounted on an angioplasty balloon catheter and delivered with or without a protective sheath. Two types of balloon-expandable stents are available – metallic coils and slotted tubes. The anticoagulant heparin is coated on the stent to prevent stenosis after placement and has shown promising results in randomised clinical studies. 27 However, the sudden occlusion of a vessel due to sub-acute stent thrombosis and late in-stent re-stenosis persist as two major complications that were initially encountered with the widespread use of bare metallic stents, in spite of the fact that thrombosis rates are now significantly reduced by the employment of antiplatelet therapy (e.g. aspirin and clopidogrel as well as the new antiplatelets prasugrel and ticagrelor). 28 Anticoagulation and antiplatelet therapies are standard adjuncts in the USA during stent placement to prevent postoperative re-stenosis. 26 Antiplatelet drugs prevent platelet aggregation and, hence, formation of thrombi, thus helping prevent in-stent re-stenosis. Although aspirin, in combination with clopidogrel or ticlopidine, has been conventionally used for this purpose, 29 the newer antiplatelets prasugrel, ticagrelor and cangrelor have also been found to be efficacious in this regard. PLATO (Platelet Inhibition and Patient Outcomes) concluded that ticagleror is superior to clopidogrel in preventing cardiovascular death after placement of DES. 30 Similar trials to compare cangrelor with conventional antiplatelets are currently under way. 31
The TAXUS-V ISR clinical trial observed a significantly higher rate of re-stenosis in patients treated with intravascular brachytherapy as compared with paclitaxel-eluting stents, the latter group being associated with a lower rate of major adverse cardiac events. 32 At the same time, DES have been found to be equally safe and efficacious as brachytherapy for the treatment of in-stent re-stenosis, as reported by Mishra et al. 33 Hence, brachytherapy is now being replaced in almost all centres by DES, almost rendering brachytherapy an obsolete procedure.
Stent-based drug delivery system
Diabetes mellitus and insulin resistance have been incriminated as the two main risk factors for re-stenosis in patients requiring myocardial revascularisation.34,35 In fact, patients with a BMI ≥25 kg/m2 have been reported to respond suboptimally to administration of standard antiplatelet agents, namely aspirin and clopidogrel, thus exposing them to a greater likelihood of suffering from cardiovascular mortality and morbidity. 36
The introduction of DES has been a revelation, as it has appreciably reduced re-stenosis rates as compared with those for bare metal stents, both in non-diabetic and diabetic patients; significantly superior outcomes have been recorded in regard to major adverse cardiac events (MACE) – death, myocardial infarction or the need for repeat revascularisation, 37 although conflicting results have also been obtained by some researchers. 38 Techniques have been so devised that the stents themselves can release the drugs by elution at the site of placement (i.e. within the blood vessel). The earliest drugs employed for this purpose were sirolimus and paclitaxel, which prevent re-stenosis by reducing the proliferation and migration of smooth muscle cells and production of extracellular matrix, thus helping prevent neo-intimal hyperplasia.39,40 Everolimus, a congener of serolimus, was approved by the FDA in 2008 for use in DES. 41 DES have now become the mainstay of therapy in coronary artery stenosis due to the very low expected rate of in-stent re-stenosis, while simultaneously brachytherapy is now virtually obsolescent.32,33 DES provide local delivery of an appropriate concentration of an effective agent to halt the process of neo-intimal hyperplasia without exposing other organs of the body to the toxic effects of the drug, thus making the drug better tolerated.
As MetS encompasses many risk factors for in-stent re-stenosis, the current need is a more aggressive approach to prevent the development of neo-intimal hyperplasia, which is the basic incriminating factor for in-stent re-stenosis. Consequently, the treatment of MetS patients by DES, which have shown improved vascular patency rates over other approaches in the prevention of in-stent re-stenosis, now assumes much greater clinical significance. This is further exemplified by the higher mortality rate during follow-up in patients with MetS as compared with controls, and by the fact that the treatment of these patients with DES improves mortality outcome more effectively than other therapeutic approaches. A reduction in re-stenosis rates of 50% has also been reported through the deployment of DES on long-term follow-up of patients undergoing PCI. Thus, the introduction of DES promises to be an excellent preventive approach in reducing the rate of re-stenosis and its consequent complications.
The drug-eluting stent consists of a metallic platform, a drug carrier vehicle and a therapeutic agent, the latter reducing neo-intimal growth induced by stent implantation. 42 Numerous methods of coating DES with drugs have been developed. Some drugs can be bonded directly to a metal stent (e.g. prostacyclin, paclitaxel), but most agents must be bonded to a matrix polymer, which acts as a drug reservoir. The DES tested most successfully to date were coated with synthetic polymers – poly-n-butyl methacrylate and polyethylene-vinyl acetate with sirolimus and a poly (lactide- co-Σ-caprolactone) co-polymer with paclitaxel. 43 These naturally occurring organic materials are both bio- and haemo-compatible. Additionally, fibrin, cellulose and albumin have also been tested in animal models, but only phosphorylcholine (e.g. Bio-divYsio®) is recommended for clinical purposes due to its ability (though unlikely) to elicit inflammation and interfere with re-endothelialisation of the stent surface. 44 Another good example is the ZoMaxx stent; constructed from stainless steel and tantalum and possessing a phosphorylcholine reservoir, this stent gradually releases zotarolimus, another congener of sirolimus. 45 Apart from sirolimus and paclitaxel, other drugs employed in DES include everolimus, tacrolimus (FK-506), zotarolimus, ABT-578, interferon, dexamethasone and cyclosporine. Sirolimus and its derivatives were shown to reduce intimal thickening. The dexamethasone-coated Bio-divYsio® stent also showed mild to moderate benefits in reducing re-stenosis. 46 Paclitaxel has been approved for clinical use and ABT-578 has also been found promising. 47 Batimastat, an inhibitor of MMPs, has shown tremendous therapeutic potential in preventing in-stent re-stenosis. Unfortunately, a clinical study using a batimastat-coated stent failed to show a reduction in re-stenosis rates when compared with BMS. 48 The sirolimus-eluting CypherTM stent (Cordis Corp.) and the TaxusTM stent (Boston Scientific, Natick, MA, USA), both loaded with paclitaxel, are the commercially available stents most often used in the USA. 49
Studies comparing stents have not succeeded in establishing a clear superiority of one design over any other. Chiu and co-workers observed that non-diabetics given sirolimus stents required a repeat revascularisation procedure less frequently as compared with those receiving paclitaxel stents; however, no such difference existted among the diabetics, who responded equally to both stents. 50 Similarly, Maurice and co-workers did not find any difference in the rates of re-stenosis or major adverse cardiac events in de novo coronary artery lesions treated with either sirolimus or paclitaxel-eluting stents. 51 As such, the available literature does not provide any clear-cut evidence in favour of sirolimus over paclitaxel; however, the general consensus among clinicians is to favour the former. 52 The newest generation of stents is loaded with everolimus which, surprisingly, however, rather than tacrolimus, has been suggested to improve upon sirolimus stents in terms of safety and efficacy, with lower rates of stent thrombosis and subsequent myocardial infarction being observed in various trials.53,54 However, a significant difference was not observed by Brugaletta et al. between sirolimus, everolimus and zotarolimus in terms of clinical outcomes. 55
Stenting: a stimulus of the inflammatory response
Adipocytes are active endocrine cells that secrete several cytokines and non-cytokine proteins, termed adipokines. These participate in and regulate inflammatory, immune, haematopoietic and vascular reactions. 56 In atherosclerotic plaques cytokines are released from adipose tissue, macrophages, dendritic cells, T cells, endothelial cells and smooth muscle cells (IL-1β, TNF-α, IL-6, IL-8, leptin, resistin, PAI-1 and adiponectin). 57 Among these, adiponectin and leptin are associated with increased insulin sensitivity, while TNF-α, resistin and PAI-1 mediate insulin resistance. Adipokines are secreted in proportion to the fat mass excepting adiponectin, whose secretion is decreased in obesity. Although the precise role of adipocytes in the development of MetS and atherosclerosis is unclear, cytokines and adipokines can both directly and indirectly influence the atherosclerotic processes through inflammation, plaque rupture and abnormalities in coagulation and fibrinolysis. In addition, IL-1 and -6 also play a causal role in the progress of MetS and diabetes. 56
Adiponectin
Adiponectin, a key hormone that participates in the pathogenesis of MetS, is synthesised by adipocytes. It has been reported to possess insulin-sensitising, anti-inflammatory and anti-atherogenic properties. 58 Unlike most other adipokines, a paradoxical decrease in the levels of adiponectin has been reported in obesity, insulin resistance, CAD and dyslipidaemia, 59 thus further increasing peripheral insulin resistance. Plasma adiponectin rapidly accumulates in the sub-endothelial space of the injured human artery. 60 Okamoto et al. reported an increase in serum adiponectin levels and decrease in atherosclerotic lesion size by about 30% following treatment with recombinant human adiponectin. 61 Recently, Arita et al. demonstrated that adiponectin treatment inhibits growth factor-induced proliferation and migration of vascular smooth muscle cells, the key pathogenetic mechanism in in-stent re-stenosis. 62 These findings indicate that adiponectin acts as an endogenous anti-atherogenic factor and is very likely to be regulated in individuals on a routine physiological basis. Physiological concentrations of adiponectin inhibit the expression of adhesion molecules, including intracellular adhesion molecule-1 (ICAM-1), vascular cellular adhesion molecule-1 (VCAM-1) and E-selectin. Moreover, adiponectin has also been shown to inhibit TNF-α-induced nuclear factor-κB (NF-κB) activation, which could be a key mechanism for the inhibition of monocyte adhesion to endothelial cells and prevention of the re-stenosis process. Adiponectin also inhibits the expression of the scavenger receptor class A-1 of macrophages, resulting in a marked decrease in the uptake of oxidised low-density protein and, hence, inhibition of foam cell formation. Similarly, it has also been shown to inhibit proliferation and migration of smooth muscle cells and to prevent re-stenosis. Higher levels of adiponectin have been found to be associated with a reduced risk of type 2 diabetes. 63 Thus, to summarise, adiponectin plays a vital role in the pathophysiology of re-stenosis and in future, adiponectin mimetics might aid in the treatment and prevention of re-stenosis.
TNF-α
The pro-inflammatory cytokine TNF-α has been found to be localised in human atheromatous plaques and it contributes to plaque progression, destabilisation and rupture, as well as the progression of re-stenosis. 64 In native coronary vessels, TNF-α contributes to the instability of plaques by augmenting the local inflammatory response via multiple effects. 64 TNF-α-induced biological effects include the release of cell surface adhesion molecules such as ICAM-1 and VCAM-1, increase in thrombotic activity and induction of endothelial as well as smooth muscle cell apoptosis by increased formation of reactive oxygen species within the plaque. In addition, TNF-α has also been demonstrated to increase the activity of MMPs that contribute to plaque instability. Furthermore, it also induces smooth muscle proliferation and increases the adherence of leucocytes to endothelial cells by inducing the expression of cell adhesion molecules. Hence, TNF-α plays a vital role in the pathophysiology of re-stenosis, and therefore inhibitors of TNF-α could potentially prevent re-stenosis. 65
Leptin
In 1994 the identification in adipose tissues of leptin, a 16-kDa pleiotropic adipokine, has opened the door on to a new era of research focusing on adipocyte endocrinology. Circulating levels of leptin correlate precisely with body fat mass. 66 Over the past decade, the endocrine role of leptin has been extensively investigated and has now been expanded from regulation of reproduction to include immune function, glucose homeostasis, vascular biology, tumour development, lipoprotein metabolism and inflammation. 67 Leptin, being a mediator of these metabolic processes, contributes to obesity by playing an important role in the development of MetS. Hyperleptinaemia has been shown to promote MetS, and dysregulation of leptin signalling in obese individuals results in reduced glucose uptake and fatty acid oxidation. Piatti et al. reported that an increased leptin level in coronary heart disease patients was associated with higher incidence of in-stent re-stenosis. 68 Stephenson and co-workers also demonstrated that neo-intima formation following vascular injury was reduced in leptin receptor mutant mice. In addition, leptin-deficient ob/ob mice were naturally protected from arterial thrombosis and/or neo-intimal hyperplasia induced by arterial injury. 69 Leptin has also been shown to augment the accumulation of cholesterol esters in foam cells, especially at high glucose concentrations. This effect results from the up-regulation of acyl-CoA:cholesterol acyltransferase and down-regulation of cholesterol esterase. Thus, leptin may increase cholesterol levels and decrease cholesterol removal from peripheral tissues. Considering these effects, it has been suggested that an increased level of leptin might contribute to the pro-inflammatory state associated with obesity, and its inhibition could offer an important therapeutic strategy.
Plasminogen activator inhibitor-1
Fibrinolysis is the process by which the fibrin in blood is proteolytically cleaved and the patency of the vessel is maintained. Similarly, in tissues, the extracellular matrix is cleaved to regulate cell adhesion and migration. Fibrinolysis is primarily regulated by PAI-1, an inhibitor of endogenous tissue plasminogen activator, which prevents the escape of this potentially destructive protease system. It is secreted by adipocytes and has been discovered to be elevated in obesity. Numerous studies have suggested that the fibrinolytic system plays an important role in stent-induced injury. 70 It has been demonstrated in animal models that the expression of PAI-1, the primary physiological inhibitor of plasminogen activation in plasma and tissues, coincides with smooth muscle and neo-intimal proliferation. Furthermore, studies in knock-out mice have also shown that PAI-1 deficiency antagonises the re-stenosis process. 71 Several studies demonstrated a positive correlation between increased PAI-1 levels or a lack of decreased PAI-1 activity with late re-stenosis, immediately follwing PCI (with or without stent implantation), following balloon angioplasty alone or following coronary atherectomy. 72 Increased PAI-1 activity following balloon angioplasty has been reported to improve the predictive value of Tl-201-scintigraphy for re-stenosis in asymptomatic patients. Overall, these data supplement the hypothesis that PAI inhibition has the potential to reduce re-stenosis process and obesity, and may represent a new therapeutic target. Further experimental and clinical studies are needed better to understand this complex interplay.
C-reactive protein
C-reactive protein (CRP) is a classical plasma protein, elevated during any inflammatory process. The plasma level of CRP is a reliable marker of the risk of coronary events and re-stenosis following percutaneous coronary intervention. An association between elevated CRP levels and an increased risk of cardiovascular events supports this relationship between inflammation and atherosclerosis. The major functions of CRP include its ability to bind to various ligands exposed on damaged tissue or bacteria for the enhancement of phagocytosis and activation of the complement pathway, thereby enabling it to exert both pro- and anti-inflammatory functions. In 2004, Kawamoto and co-workers observed that in-stent re-stenotic tissue showed more immunoreactivity for CRP than tissue that had undergone re-stenosis following directional coronary atherectomy. 73 Though the origin of CRP in re-stenotic lesions remains unclear, it is assumed that CRP is mainly produced by the liver and enters the arterial wall along with blood flow at the sites of endothelial dysfunction. It may also additionally be synthesised by hepatocytes and macrophages. Interestingly, coronary plaque tissue obtained during directional coronary atherectomy expressed the CRP gene, suggesting that coronary plaque is also a CRP production site. 74
Resistin
Resistin is a 10 kDa protein that belongs to the resistin-like molecule family. It was cloned in 2001 as a thiazolidinedione-regulated cytokine expressed in adipose tissue. Resistin is up-regulated during adipogenesis and down-regulated on treatment with PPAR-γ agonists. 75 Its effects on insulin action have been extensively investigated in mice, where it has been shown to be involved in hepatic glucose and lipid metabolism and has been found to be a major determinant of hepatic insulin resistance in high-fat diet-induced insulin resistance. 76 Subsequent studies in rodents have suggested that resistin acts as a link between obesity, insulin resistance and diabetes. Some investigators indicated that an increase in serum resistin levels is associated with re-stenosis progression, insulin resistance and type 2 diabetes. 77 The injection of resistin into wild-type mice was shown to result in reduction in both glucose tolerance and insulin activity, whereas the injection of neutralising antibodies into diabetic obese mice improved insulin activity. 75 When resistin was infused in physiological concentrations in the presence of physiologically high levels of circulating insulin, lower rates of glucose infusion were necessary to maintain basal glucose levels. Insulin resistance caused by resistin infusion has been attributed to an increased rate of glucose production rather than to an increase in glucose uptake. This clearly indicates that resistin has a profound and rapid effect on hepatic insulin sensitivity.
Interleukin-6
Interleukin-6 is a pleiotropic cytokine that has been shown to be involved in several biological activities including inflammation, immune regulation and haematopoiesis. It also stimulates the release of white blood cells and platelets from the bone marrow, as well as that of CRP, endothelin and fibrinogen. Similar to leptin, IL-6 also increases adiposity and circulating IL-6 concentrations have been shown to correlate highly with percentage body fat and insulin resistance. 78 In MetS, the IL-6 level has been documented to be increased by secretion by T cells, macrophages and adipocytes.
During angioplasty, the production of IL-6 has been shown to be up-regulated and increase in local IL-6 concentration is associated with recurrent luminal narrowing. IL-6 has a pivotal role in stimulating the acute phase response, including the release of fibrinogen and CRP, both of which are potent predictors of re-stenosis following angioplasty. IL-6 is also believed to be directly involved in re-stenosis, as it has been shown to stimulate endothelial activation, leukocyte recruitment into the vessel wall and vascular smooth muscle cell proliferation, which participate in the formation of a hypertrophic neo-intima following PTCA and luminal loss. 79
Role of DES in management of stent-related inflammatory issues
A myriad of adipokines, as discussed above, promote smooth muscle cell proliferation that ultimately contributes to neo-intimal hyperplasia, the basic pathophysiology underlying in-stent re-stenosis. As discussed previously, the drugs eluted by DES counteract this neo-intimal hyperplasia by exerting anti-proliferative effects, and thus are now widely acclaimed as the mainstay of preventive therapy for in-stent re-stenosis.
Animal models of re-stenosis
To date, considerable research efforts have been undertaken to understand the pathophysiology of re-stenosis and to develop novel strategies to treat and prevent this major shortcoming of PTCA and stent implantation. Additionally, several drugs have been successfully investigated to prevent re-stenosis in animal models, but the majority of these have unfortunately been found to be ineffective in human clinical trials.4,80 Therefore, the indispensability of a suitable animal model, which would aid the understanding of the pathophysiology and mechanisms of re-stenosis, cannot be understated. An important distinction between human atherosclerotic coronary arteries and those of the rat, rabbit and pig is the morphological differences among these species. A human atherosclerotic plaque is usually subject to ulceration, calcification, thrombosis and haemorrhage. In addition, certain cellular components, such as monocyte-derived macrophages, are also abundant in atherosclerotic plaques. Activated macrophages contain numerous protein and lipid mediators, such as TNF-α and heparin-binding epidermal growth factor, which are uncommon but have been reported in animal models, even in the hyperlipidaemic rabbit. 80 Thus, inflicting damage to a vessel rich in macrophages might elicit hyperplasia by mechanisms similar to those seen in human arteries. Also, species differences and the fibrinolytic system may affect the amount of neo-intima formation, despite similar degrees of arterial injury.
Rat carotid artery model
The rat carotid artery model has become the standard for the investigation of re-stenosis, due to its ready availability, easy handling and economical housing. 81 This model is based on the induction of endothelial injury with a low-pressure balloon at the intimal layer of the vessel. 82 However, the disadvantage of this model lies in the gross anatomical differences from human coronary arteries, which makes it difficult to extrapolate the results to humans. The rat artery lacks a vasa vasorum and has a very small elastin content in the media. These differences would appear to be important, as it has been speculated that the vasa vasorum arterial component is substantially involved in vessel cell proliferation in humans.83,84 Using this model, the impact of angiotensin-converting enzyme inhibitors on the formation of neo-intimal thickening has been investigated. 85 However, clinical studies were of limited success in confirming this effect in humans. 86
Rabbit iliac model
The rabbit atherosclerotic iliac re-stenosis model is frequently employed in the evaluation of drugs used to combat re-stenosis and in furthering understanding of the re- stenosis process. 87 On a normal diet most rabbit strains do not develop atherosclerosis, but on a high-cholesterol diet atherosclerosis has been reported. Arterial lesions were induced by arterial injury (e.g. endothelial denudation by a Fogarty catheter) and subsequent feeding of a high-cholesterol diet. 88 Rabbit models serve as single-, double- or triple-injury models, which can be induced as biochemical damage with hypercholesterolaemic diets, or as mechanical injury through either balloon catheter or air dessication bilaterally in the femoral artery. 87 The stenotic lesions induced by this technique predominantly consisted of lipid-laden foam cells, which are frequently found in human plaques. A major advantage of this model is that the size of the rabbit iliac artery is similar to that of the human coronary artery, which facilitates the evaluation of new revascularisation devices.
Porcine model
The porcine coronary model of in-stent re-stenosis was first described in 1990 as an adaptation of the porcine coronary balloon angioplasty model, using oversized metallic stents placed into the normal, non-atherosclerotic coronary arteries of domestic juvenile swine, with a thick neo-intima reliably induced by 28 days and persisting for six months. 89 With regard to the cardiovascular system, the porcine heart and its coronary artery system have morphological and anatomical similarity to that of the human. 90 Furthermore, atherosclerotic lesions observed in this model closely resemble plaque-induced injury in humans. The histopathological characteristics of the neo-intima following balloon dilatation or stent implantation have also been shown to be similar to those seen in human re-stenosis. 91 Also, the response to vessel wall injury has been precisely quantified in porcine coronary stent models. This model has proved popular in the evaluation of DES. Heldman et al. reported a dose-dependent decrease in in-stent re-stenosis by using a paclitaxel-eluting Palmar–Schatz stent. 92 Similar findings have been reported for sirolimus-eluting stents. 93 Continuous systemic administration of angiopeptin has been observed to reduce neo-intimal hyperplasia by 60% as compared with the control group. 93 Although the porcine model fulfils many criteria of an ideal model of atherosclerosis and re-stenosis, maintaining these animals is quite expensive and requires extensive logistical effort.
Canine model
Canine models of re-stenosis are popular due to their size, cost and ready availability. However, dogs are relatively resistant to diet-induced atherosclerosis and develop atherosclerotic lesions only following thyroidectomy. 94 Despite this major disadvantage, the canine model has been used in basic cardiology research as the size of canine coronary arteries is very similar to that of humans. 91 Following stent implantation, reduction in neo-intimal injury suggests that canine arteries are relatively inert to vascular injury. 95 Also, dogs have a high fibrinolytic activity, which is markedly different from that of the human coagulation system. 91 These considerations mark the dog as a poor model for re-stenosis.
Conclusion
MetS is a common metabolic disorder contributing to the increased prevalence of re-stenosis following stenting. Though the cellular and molecular mechanisms are yet to be comprehensively elucidated, there has been improvement in the range of theoretical knowledge of a variety of mechanisms. Due to the complexity of the re-stenosis process, experimental results from modelling this biological process can only be applied with caution for angioplasty or stent implantation in human atherosclerotic lesions. On the other hand, in-stent re-stenosis is a major challenge for the interventional cardiologist, with none of the available interventional modalities proving to be ideal. Currently, efforts are ongoing to prevent in-stent re-stenosis using techniques such as DES, which inhibit the biological reaction of the vessel wall. Based on the advent of genomics and an understanding of the molecular pathogenetics involved in MetS, micro-RNAs (miRNAs) and epigenetics appear to hold a key position, warranting future investigations to illuminate the therapeutic potential of epigenetic modifiers and miRNAs.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
All authors have no conflicts of interest.