
Abstract
Objective
To evaluate the 1-year clinical outcomes of patients who received the Resolute Onyx™ stent.
Methods
This was a single-centre, retrospective registry analysis that reviewed the clinical data from all patients who were implanted with a Resolute Onyx™ stent between March 2015 and February 2016. Clinical follow-up was performed at 1 year post-implantation.
Results
A total of 252 patients received a Resolute Onyx™ stent and two patients were lost to follow-up. The mean age of the cohort was 66.9 years and 113 (45.2%) had diabetes mellitus. Thirty-eight patients (15.2%) had left main disease and 73 (29.2%) had three-vessel disease. A total of 175 patients (70.0%) had small vessel disease (<2.75 mm) and 210 (84.0%) had long lesions (>20 mm). The 1-year target lesion failure was 4.4% (11 of 250), cardiovascular death occurred in eight patients (3.2%), ischaemia-driven target lesion revascularization was undertaken in five patients (2.0%) and stent thrombosis occurred in one patient (0.4%).
Conclusion
The Resolute Onyx™ stent showed a favourable 1-year clinical performance in a real-world population.
Introduction
Drug-eluting stents (DES) are widely used for the treatment of obstructive coronary artery disease. Despite concerns related to very late stent thrombosis associated with first-generation DES, continuing advancement in stent design, polymer and drug-eluting technology has improved the efficacy and safety of second-generation DES.1,2 The Resolute™ Integrity zotarolimus-eluting stent (R-ZES; Medtronic Inc., Santa Rosa, CA, USA) has been extensively studied in the Resolute Global Clinical Program, 3 which demonstrated favourable clinical outcomes in an all-comer population. The latest version of R-ZES, Resolute Onyx™, was launched in November 2014. This study investigated the 1-year clinical outcomes of patients who had received this new technology.
Patients and methods
Study design and population
This was a single-centre retrospective registry analysis. From the launch of Resolute Onyx™, all patients treated in the Division of Cardiology, Queen Mary Hospital, University of Hong Kong, Hong Kong who had been fitted with a Resolute Onyx™ stent between March 2015 and February 2016 were identified in the hospital database and recruited to the analysis. There were no exclusion criteria except patients lost to follow-up or those who could not be contacted for assessment at 1 year after stent implantation. Baseline demographics, procedural details and follow-up data were recorded. All treatment and clinical decision-making processes were subject to the attending cardiologists.
The study was approved by the Institutional Ethics Committee of Queen Mary Hospital, University of Hong Kong, Hong Kong (no. UW 17-026). Written informed consent was waived by the Institutional Ethics Committee as this was a retrospective analysis without any alteration in patient management.
Study endpoints
The primary endpoint was 1-year target lesion failure (TLF), defined as a composite of cardiac death, myocardial infarction (not clearly attributed to a non-target vessel), or a clinically indicated target lesion revascularization by percutaneous or surgical methods at 12 months. All clinical outcomes were defined according to the Academic Research Consortium (ARC). 4 Deaths were considered cardiac unless an unequivocal non-cardiac cause could be established. Secondary endpoints included individual components of the primary outcomes: target vessel myocardial infarction; clinically-driven target lesion revascularization (TLR), defined as repeat revascularization within the stented segment including 5 mm proximal and distal border zones; clinically-driven target vessel revascularization (TVR) and stent thrombosis defined according to the ARC as definite, probable, or possible. 4 A revascularization was considered clinically-driven if repeat angiography showed a diameter stenosis ≥50% with at least one of the following: (i) history of recurrent angina pectoris, presumably related to the target vessel; (ii) objective signs of ischaemia at rest or during exercise test by electrocardiogram, presumably related to the target vessel; (iii) abnormal test results of invasive functional diagnostic test (fractional flow reserve); or (iv) a TLR with a diameter stenosis ≥70% even in the absence of the aforementioned ischaemic signs or symptoms.
Study device
Resolute Onyx™ (Medtronic Inc., Santa Rosa, CA, USA) is a zotarolimus-eluting stent designed for higher procedural success and better acute performance. The design is based on its predecessor, the Resolute™ Integrity drug-eluting stent, which was extensively studied in the Resolute Global Clinical Program. 3 In brief, the stent is manufactured using continuous sinusoid technology that employs a single strand of wire to form a sinusoidal pattern of crowns, which is laser fused at selected crowns. This distinctive wire-forming facilitates smooth tracking in tortuous vessels and allows excellent conformability. 5 The drug polymer BioLinx is highly biocompatible with a hydrophilic surface designed to minimize inflammation. 6 The polymer elutes the drug zotarolimus, which is a synthetic analogue of sirolimus, over 180 days, with >85% of the zotarolimus dose released by day 60. 7 The latest version Resolute Onyx™ utilizes core-wire technology in which the cobalt alloy incorporates a platinum iridium core for increased radiopacity. Moreover, the strut thickness is further reduced to 81 µm (0.0032 inches) with maintained radial strength and the crossing profile is 0.037 mm for the 2.5 mm stent. The Resolute Onyx™ stents used in patients included in this registry study ranged from 2.0 mm to 5.0 mm diameters and the stent lengths were up to 38 mm.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 19.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Continuous variables are as mean ± SD. Categorical values are presented as absolute values or percentages. Comparison of continuous data was performed by one-way analysis of variance, Mann–Whitney U-test or independent-samples t-test depending on data distribution. χ2-test and Fisher’s exact test were used to compare categorical data. A two-sided P-value of ≤0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of patients who were implanted with Resolute Onyx™ stents between March 2015 and February 2016.
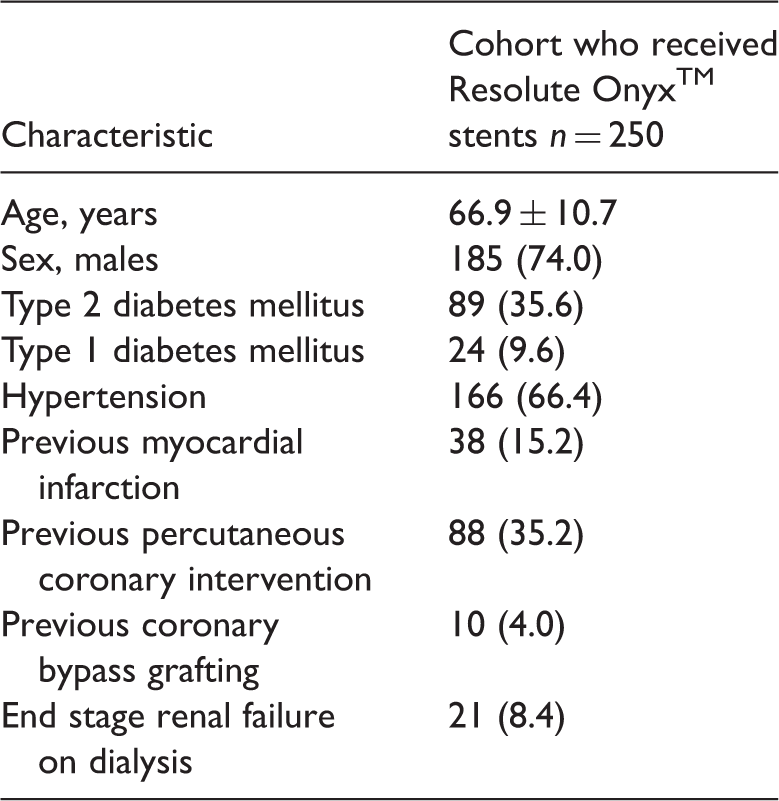
Data presented as mean ± SD or n of patients (%).
Procedural characteristics of patients who were implanted with Resolute Onyx™ stents between March 2015 and February 2016.

Data presented as n of patients (%).
Lesion characteristics of patients who were implanted with Resolute Onyx™ stents between March 2015 and February 2016.

Data presented as n of patients (%).
The 1-year clinical outcomes of patients who were implanted with Resolute Onyx™ stents between March 2015 and February 2016.

Data presented as n of patients (%).
Comparison of patients with or without small vessel disease who were implanted with Resolute Onyx™ stents between March 2015 and February 2016.

Data presented as mean ± SD or n of patients (%).
No significant between-group differences (P > 0.05).
Discussion
To the best of our knowledge, this is the first report of the medium-term clinical performance of the latest evolution of R-ZES, the Resolute Onyx™ stent. These present data demonstrated that the Resolute Onyx™ stent achieved similar efficacy and safety compared with most contemporary DES with a 1-year TLF rate of 4.4%. 1 In the Resolute All Comers trial, 8 the Resolute zotarolimus-eluting stent and an everolimus-eluting stent had 1-year TLF rates of 8.2% and 8.3%, respectively. Although this current retrospective registry has its inherent limitations, this post-marketing study allowed the analysis of all patients including those with ultra-high-risk characteristics. For example, this current cohort included patients with cardiogenic shock, patients with ESRF receiving dialysis, a high proportion of patients with T2DM and even patients who presented with cardiac arrest requiring haemodynamic support. This current cohort reflects real-world coronary intervention practices, which is difficult to study in prospective randomized clinical trials. In this present study, many of the TLFs occurred in those ultra-high-risk patients and this further provides insight into the use of the Resolute Onyx™ stent in a real-world population.
In the present study, 45% of patients had diabetes mellitus and 70% had small vessel disease. Small vessel stenting has traditionally been associated with higher rates of restenosis and repeat revascularizations.9,10 The degree of neointimal proliferation is relatively independent of the reference vessel size and hence the proportion of cross-sectional luminal narrowing is higher in small vessels compared with large vessels. 11 The problem is further complicated by the presence of T2DM that predisposes to neointimal hyperplasia while patients with T2DM tend to have diffuse small vessel disease. 12 These current data suggest that the Resolute Onyx™ stent had similar outcomes in small and large vessel diseases, which is similar to its predecessor stent as demonstrated by the Resolute Global Clinical Program small vessel subgroup analysis. 13 Even in ultra-small vessels implanted with a 2.0 mm Resolute Onyx™ stent, the results were satisfactory and further studies will be required to investigate the optimal treatment of ultra-small vessel diseases.
Of the patients in the current study who experienced TLF within 1 year, a significant proportion were patients with ESRF receiving dialysis (five of 11 patients). Chronic kidney disease (CKD) is known to be associated with increased mortality and morbidity from coronary artery disease. 14 Particularly in those with ESRF on dialysis, who are frequently excluded from clinical trials, treatment failures are common after revascularization no matter whether percutaneous coronary intervention (PCI) or coronary bypass grafting are performed. 15 Even with second-generation DES, the 1-year TLF rate approached 15% and more than 30% needed repeat revascularization in longer term follow-up.16–18 In this current registry, five out of 21 ESRF patients (24%) suffered from TLF within 1 year, which is quite a high proportion. With the aging population, increasing prevalence of T2DM, CKD and better renal support, the incidence of coronary artery disease in patients with ESRF is set to increase. Further advancements in coronary revascularization technology including PCI and stenting is imminently needed to address this future healthcare demand.
This study had several limitations. First, a lack of a control group prevents comparison with other stents. Secondly, the small sample size and low event rates render conclusive outcome and independent predictor analyses difficult. Furthermore, the retrospective study design was subject to selection bias, although it allowed recruitment of a real-world PCI practice cohort and only two patients were lost to follow-up.
In conclusion, the Resolute Onyx™ stent showed a favourable 1-year clinical performance in a real-world population.
Footnotes
Declaration of conflicting interests
Hung Fat Tse received consulting fees from Medtronic. The other authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.