
Abstract
Background:
Drug-eluting stent has been shown to reduce the risk of repeated revascularization. However, as shown for first-generation drug-eluting stent, they may be counterbalanced by a potential higher risk of stent thrombosis, especially among ST-segment elevation myocardial infarction patients. In addition, diabetes has been shown to be an independent predictor of poor survival and repeated target vessel revascularization. No data have been reported so far on the long-term benefits and safety of new-generation drug-eluting stent in ST-segment elevation myocardial infarction according to diabetes. Therefore, the aim of this study was to evaluate whether diabetes may impact on the benefits from everolimus-eluting stent versus first-generation drug-eluting stent in patients undergoing primary angioplasty.
Methods:
We combined data from two randomized trials (PaclitAxel or Sirolimus-Eluting Stent vs Bare-Metal Stent in Primary Angioplasty and randomized comparison of everolimus-eluting stents and sirolimus-eluting stents in patients with ST elevation myocardial infarction) including consecutive ST-segment elevation myocardial infarction patients admitted within 12 h of symptom onset undergoing primary angioplasty and stent implantation at a tertiary centre with 24-h primary percutaneous coronary intervention capability. Primary endpoint of this study was major adverse cardiac events at 3-year follow-up. Secondary endpoints were as follows: (1) death, (2) reinfarction, (3) definite or probable ST and (4) target vessel revascularization at 3-year follow-up. No patient was lost to follow-up.
Results:
Our population is represented by 680 ST-segment elevation myocardial infarction patients treated with drug-eluting stent (180 enrolled in the PaclitAxel or Sirolimus-Eluting Stent vs Bare-Metal Stent in Primary Angioplasty trial, treated with first-generation drug-eluting stent, and 500 patients in the randomized comparison of everolimus-eluting stents and sirolimus-eluting stents in patients with ST elevation myocardial infarction, randomized to everolimus-eluting stent or sirolimus-eluting stent). Diabetes was observed in a total of 178 patients (26.1%) and associated with higher major adverse cardiac events, mortality, reinfarction, stent thrombosis and target vessel revascularization. Similar outcome was observed in terms of overall major adverse cardiac events, mortality, recurrent myocardial infarction, target vessel revascularization, with everolimus-eluting stent as compared to first-generation drug-eluting stent in both diabetic and non-diabetic patients, whereas everolimus-eluting stent was associated with a significantly lower rate of stent thrombosis only in diabetic patients (1.6% vs 9.6%, hazard ratio (95% confidence interval) = 0.15 (0.02−0.98), p = 0.04) whereas no difference was observed in non-diabetic patients.
Conclusion:
This study shows that among ST-segment elevation myocardial infarction patients undergoing primary angioplasty, diabetes is associated with a significantly worse outcome at 3-year follow-up. A similar outcome was observed between everolimus-eluting stent and first-generation drug-eluting stent in non-diabetic patients, whereas among diabetic patients everolimus-eluting stent was associated with a significant reduction in stent thrombosis.
Keywords
Several randomized trials have clearly shown the adjunctive benefits in terms of mortality from primary percutaneous coronary intervention (PCI) as compared to thrombolysis as reperfusion strategy in the treatment of patients with ST-segment elevation myocardial infarction (STEMI).1,2 Even though stent implantation has reduced the occurrence of restenosis as compared to balloon angioplasty in selected STEMI patients,3,4 the outcome of bare-metal stents (BMSs) seem to be worse in unselected patients with a rate of target vessel revascularization (TVR) up to 20%.5,6 Several randomized trials and meta-analyses have shown that drug-eluting stents (DES) are associated with a significant reduction in restenosis and TVR in STEMI patients as compared to BMSs.7–10 However, concerns have emerged on the higher risk of stent thrombosis with first-generation DES. 10 Diabetes has been shown to be an independent predictor of poor short- and long-term survival and repeated TVR and stent thrombosis.11–16 However, no data have been reported so far on the long-term efficacy and safety of new-generation DES in STEMI according to diabetes that is therefore the aim of this study.
Methods
We combined data from two randomized trials (PaclitAxel or Sirolimus-Eluting Stent vs Bare-Metal Stent in Primary Angioplasty (PASEO) and randomized comparison of everolimus-eluting stents and sirolimus-eluting stents in patients with ST elevation myocardial infarction (RACES-MI)) including consecutive STEMI patients admitted within 12 h of symptom onset undergoing primary angioplasty and stent implantation at a tertiary centre with 24-h primary PCI capability. Detailed data on these two trials have been already reported.7,17 These two trials included consecutive STEMI patients undergoing primary angioplasty who fulfilled all the following inclusion criteria: (1) chest pain for more than 30 min and (2) ST-segment elevation of 1 mm or more in two or more contiguous electrocardiograph (ECG) leads or with presumably new left bundle-branch block. Exclusion criteria included the following: (1) active internal bleeding or a history of bleeding diathesis within the previous 30 days; (2) contraindication to dual antiplatelet therapy for 12 months; (3) known allergy to taxol, sirolimus or everolimus; (4) a history of stroke within 30 days or any history of haemorrhagic stroke; (5) history, symptoms or findings suggestive of aortic dissection; (6) pregnancy and (7) participation in other trials. No angiographic exclusion criteria were used. The Institutional Review Board of the Ospedale S.G. Moscati (Avellino, Italy) approved the protocols.
Primary endpoint of this analysis was major adverse cardiac events (MACE) at 3-year follow-up. Secondary endpoints were as follows: (1) death, (2) reinfarction, (3) definite or probable ST and (4) TVR at 3-year follow-up. No patient was lost to follow-up.
Medications
All patients received 70 U/kg IV bolus of unfractionated heparin (UFH), aspirin intravenously (500 mg) and clopidogrel (600 mg loading dose). GpIIb–IIIa inhibitors administration and the number and length of stents to be implanted were left to the operator’s discretion. Post interventional antiplatelet therapy for all patients consisted of aspirin (100 mg/day) indefinitely and clopidogrel (75 mg daily recommended for 12 months).
Angioplasty procedure
Stenting procedures were performed according to standard techniques. The number and length of stents to be implanted were left to the operator’s discretion. The operator was allowed to implant DES to cover the entire length of the lesion with coverage of the entire stented segment and of 5 mm proximal and distal segments. The use of intravascular ultrasound (IVUS), adjunctive thrombectomy devices, distal protection devices and intra-aortic balloon pump (IABP) were left to the operator’s discretion.
Angiographic analysis
Thrombolysis in myocardial infarction (TIMI) grade 3 coronary flow in the treated vessel and a residual stenosis less than 30% were the criteria used to define a successful PCI. Quantitative angiographic analyses (Integris Allura; Philips, The Netherlands) were performed online and offline by two experienced technician who were unaware of treatment assignment with the averaging scores if they were none in agreement.
Data collection and follow-up
As per protocol, patients were reviewed at our outpatient clinic or by telephone interview at 6, 12, 24 and 36 months. For patients, who died during follow-up, hospital records and necropsy data were reviewed, when possible. No patient was lost to follow-up.
Study endpoints and definitions
The primary endpoint was MACE at 3-year follow-up, defined as combined death, reinfarction, definite or probable stent thrombosis and TVR. Secondary endpoints were cumulative occurrence of (1) death, (2) reinfarction, (3) definite or probable stent thrombosis according to Academic Research Consortium (ARC) definition 18 and (4) TVR at 3-year follow-up. Recurrent myocardial infarction (reMI) was defined as recurrence on angina symptoms with typical ECG changes and increase above upper limit of normal of creatine kinase-MB (CK-MB) or troponin. The indication for a second intervention had to be substantiated by symptoms or by ECG or scintigraphic evidence of ischaemia at rest or during exercise. Subsequent revascularization of other coronary arteries did not constitute an endpoint. All events were reviewed by two cardiologists blinded to treatment assignment.
Statistical analysis
Continuous data were expressed as mean [standard deviation (SD)] and categorical data as percentages. The analysis of variance was appropriately used for continuous variables. The χ2 test or the Fisher’s exact test was used for categorical variables. The difference in event rates between groups during the follow-up period was assessed by the Kaplan–Meier method with the log-rank test. Furthermore, Cox-regression analysis was performed to correct the results for any difference in baseline demographic, clinical, angiographic or procedural characteristics that were different between the two groups. A probability value of p < 0.05 was considered significant. Data were analysed according to intention to treat analysis. Statistical analysis was performed using SPSS 17.0.
Results
Patient characteristics and procedural results
From 2005 to May 2009, 770 STEMI patients were enrolled in PASEO and RACES-MI trials.10,17 A total of 90 patients randomized to BMS in the PASEO trial were excluded. Therefore, our final population is represented by 680 STEMI patients, 250 treated with everolimus-eluting stent (EES) and 430 with first-generation DES [90 with paclitaxel-eluting stent (PES) and 340 with sirolimus-eluting stent (SES)]. Diabetes was observed in a total of 178 patients (26.1%). As reported in Tables 1 and 2, no difference was observed in terms of baseline demographic, clinical and angiographic characteristics between diabetic and control patients. No difference was observed between the groups in terms of number of implanted stent per patient (1.13 ± 0.39 vs 1.15 ± 0.41, p = 0.64). As shown in Table 2, no difference was observed in terms of angiographic and procedural characteristics. Almost 50% of patients underwent PCI of left anterior descending artery. Procedural success was obtained in 93%−95% of patients. No difference was observed in medical therapy at discharge (Table 3).
Baseline demographic and clinical characteristics according to diabetes.
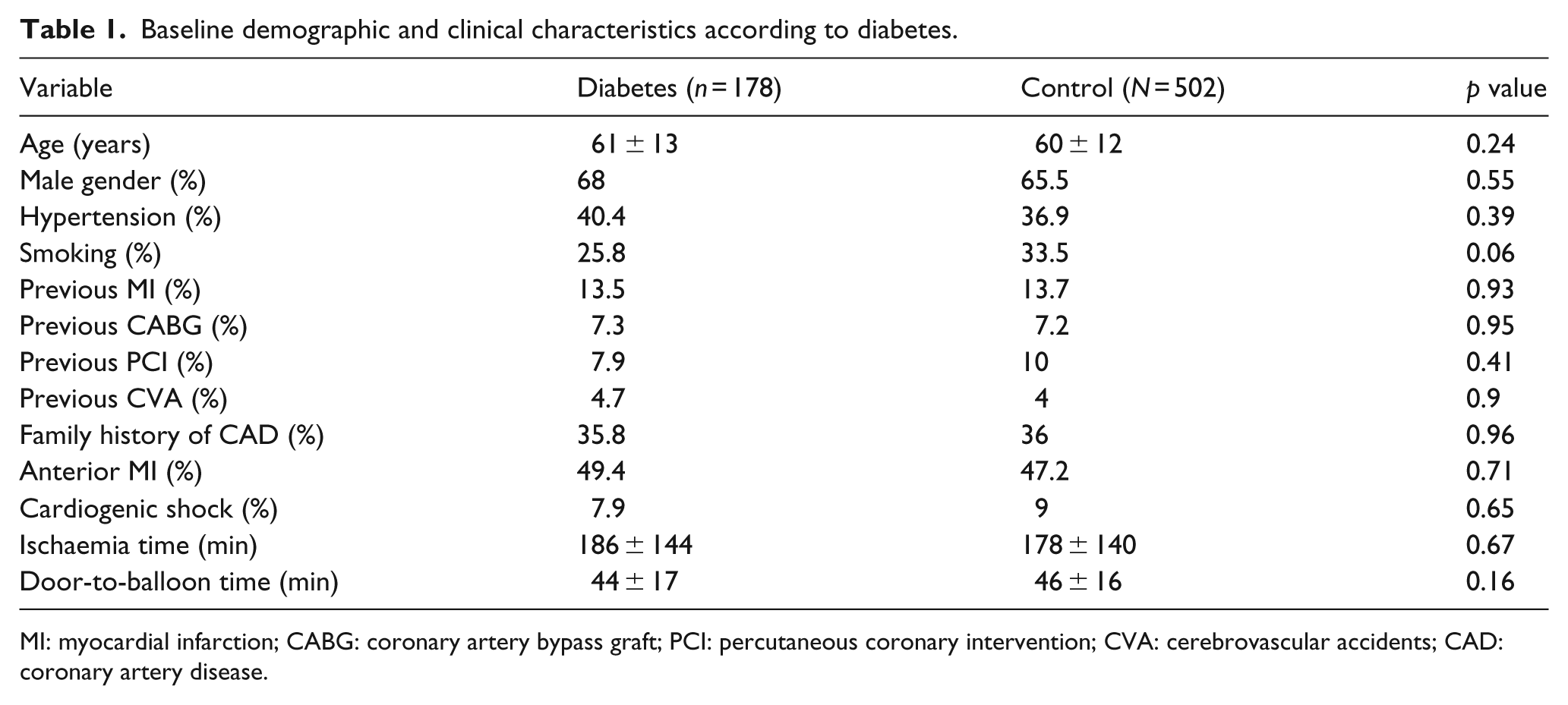
MI: myocardial infarction; CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention; CVA: cerebrovascular accidents; CAD: coronary artery disease.
Angiographic and procedural characteristics of the two groups of patients.
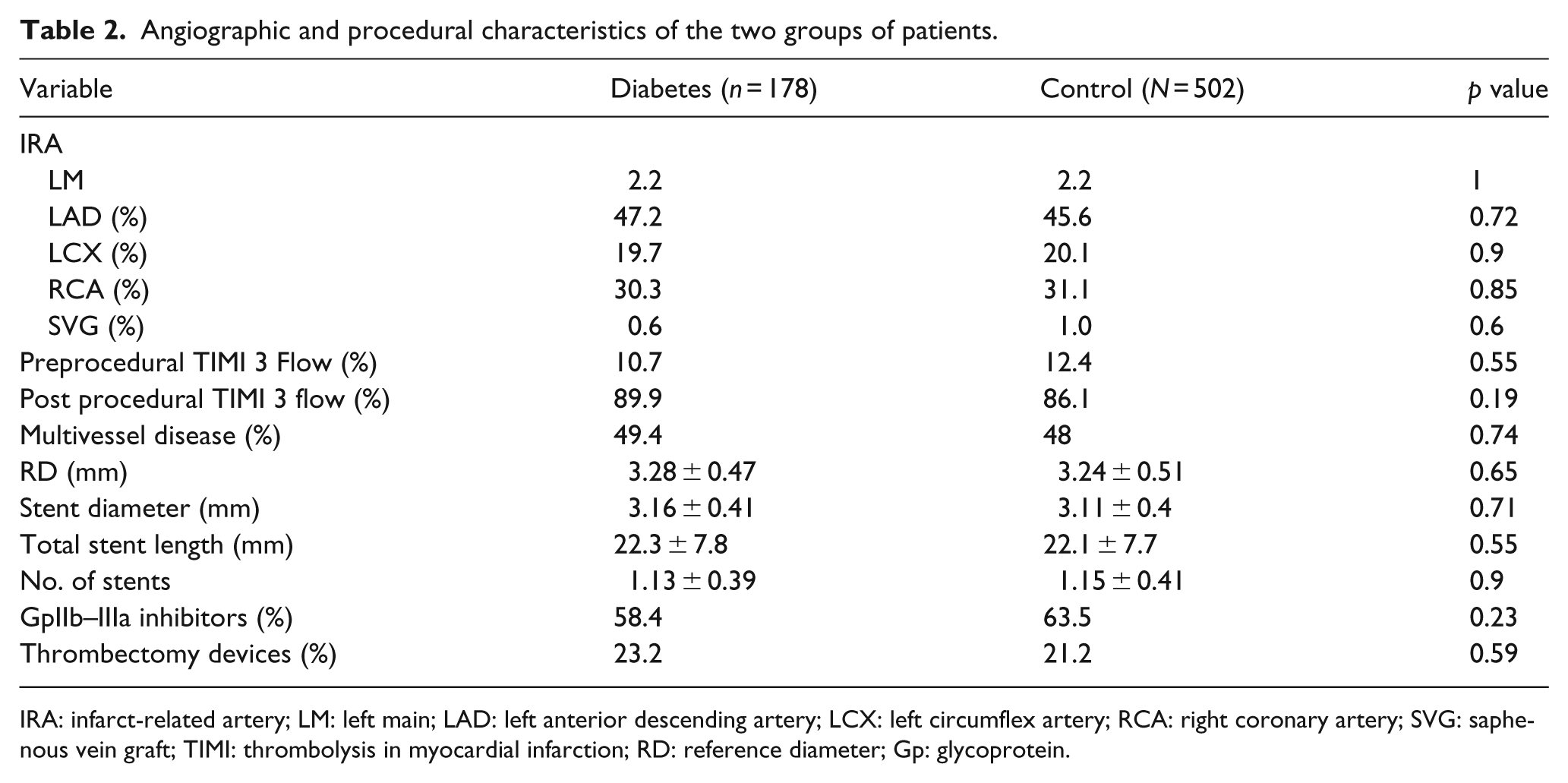
IRA: infarct-related artery; LM: left main; LAD: left anterior descending artery; LCX: left circumflex artery; RCA: right coronary artery; SVG: saphenous vein graft; TIMI: thrombolysis in myocardial infarction; RD: reference diameter; Gp: glycoprotein.
Therapy at discharge.

Clinical outcome at follow-up
Diabetes versus control patients
Follow-up data were available in all patients (1095 ± 159 days). No difference was observed in terms of duration of dual antiplatelet therapy between the two groups. Diabetes was associated with higher MACE (35.4% vs 13.3%, hazard ratio (HR) (95% CI) = 3.1 (2.2–4.33), p < 0.001) (Figure 1), mortality [12.9% vs 3.6%, HR (95% CI) = 3.82 (2.1–7.1), p < 0.001], reinfarction (15.2% vs 5.6%, HR (95% CI) = 3.05 (1.8–5.15), p < 0.001) (Figure 2), TVR (9.0% vs 3.6%, HR (95% CI) = 2.6 (1.3–5.05), p = 0.007) and stent thrombosis (6.7% vs 2.4%, HR (95% CI) = 3.0 (1.34–6.65), p = 0.007) (Figure 3).
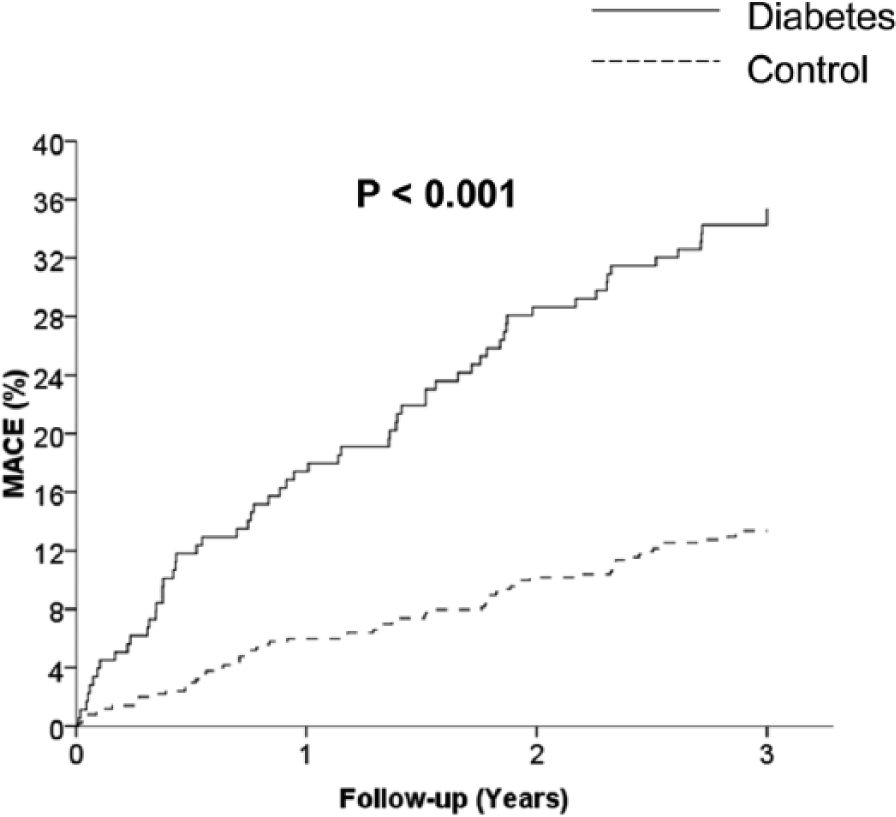
Kaplan–Meier curves showing the impact of diabetes on the occurrence of MACE.
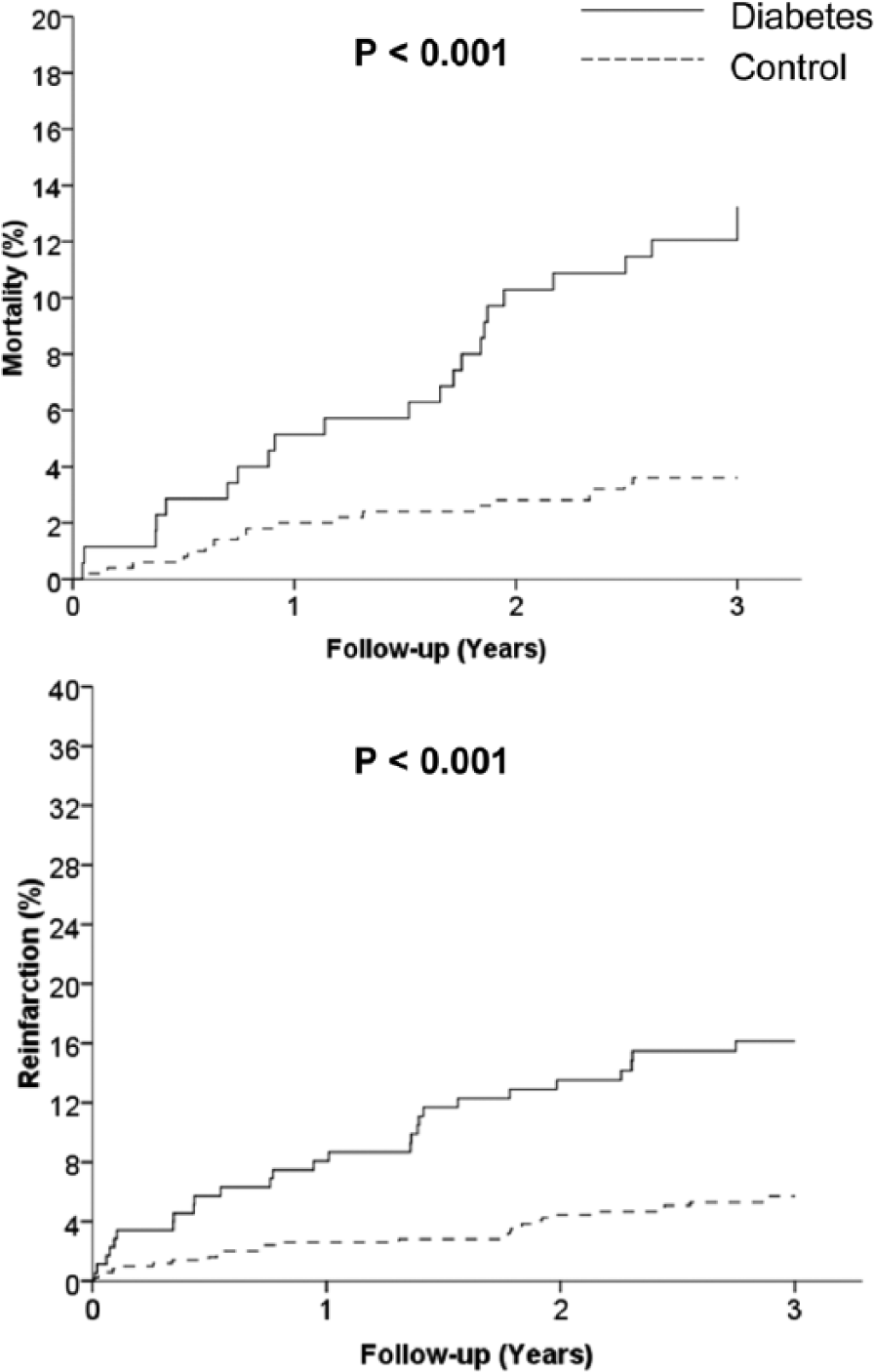
Kaplan–Meier curves showing the impact of diabetes on the occurrence of death (upper graph) and reinfarction (lower graph).
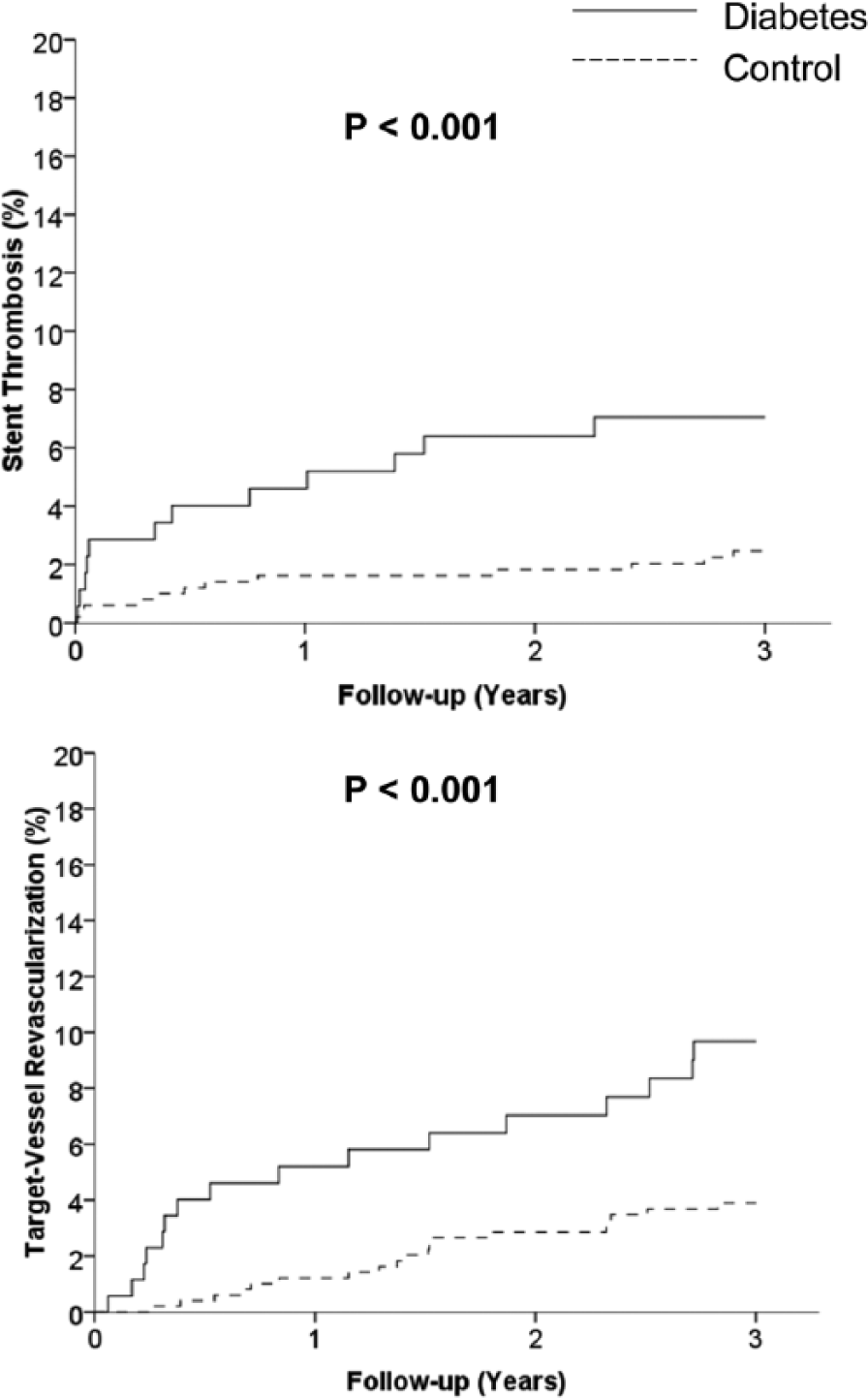
Kaplan–Meier curves showing the impact of diabetes on the occurrence of stent thrombosis (upper graph) and target vessel revascularization (lower graph).
EES versus first-generation DES
MACE
MACE was observed in a total of 92 patients (13.5%). As shown in Figure 4, no significant difference was observed between EES and first-generation DES (16% vs 20.8%, HR (95% CI) = 0.8 (0.55–1.16), p = 0.24). The results were confirmed in both diabetic (34.4% vs 36%, HR (95% CI) = 0.95 (0.57–1.6), p = 0.85) and non-diabetic patients (10.8% vs 14.9%, HR (95% CI) = 0.7 (0.42–1.19), p = 0.19).
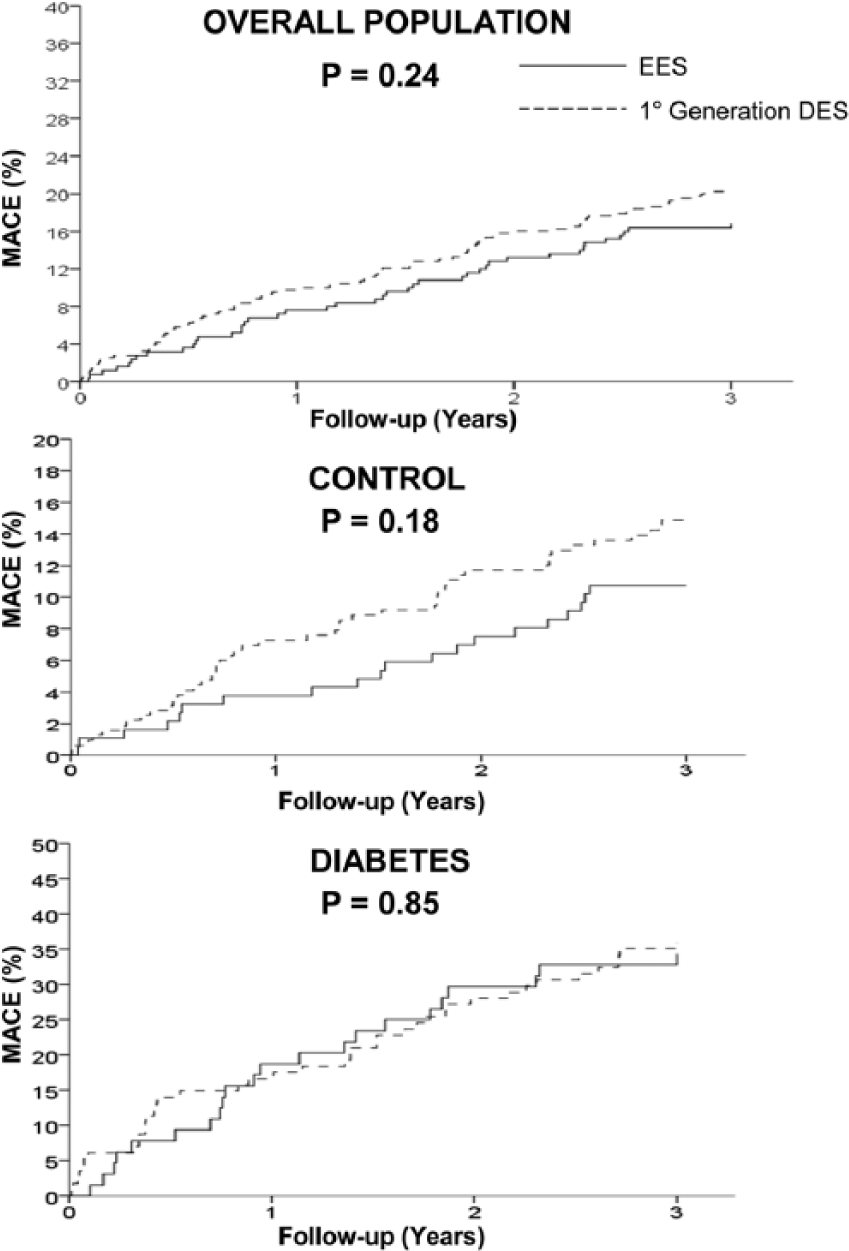
Kaplan–Meier curves showing the impact of EES as compared to first-generation DES on the occurrence of MACE in overall population (upper graph), in control patients (middle graph) and diabetic patients (lower graph).
Secondary study endpoints
Mortality
A total of 41 patients (6%) had died at follow-up. As shown in Figure 5, no difference was observed in death between EES and first-generation DES (5.2% vs 6.5%, HR (95% CI) = 0.8 (0.41–1.52), p = 0.48). Similar results were observed among diabetic (10.9% vs 14%, HR (95% CI) = 0.76 (0.31–1.85), p = 0.54) and non-diabetic patients (3.2% vs 3.8%, HR (95% CI) = 0.84 (0.32–2.25), p = 0.73).
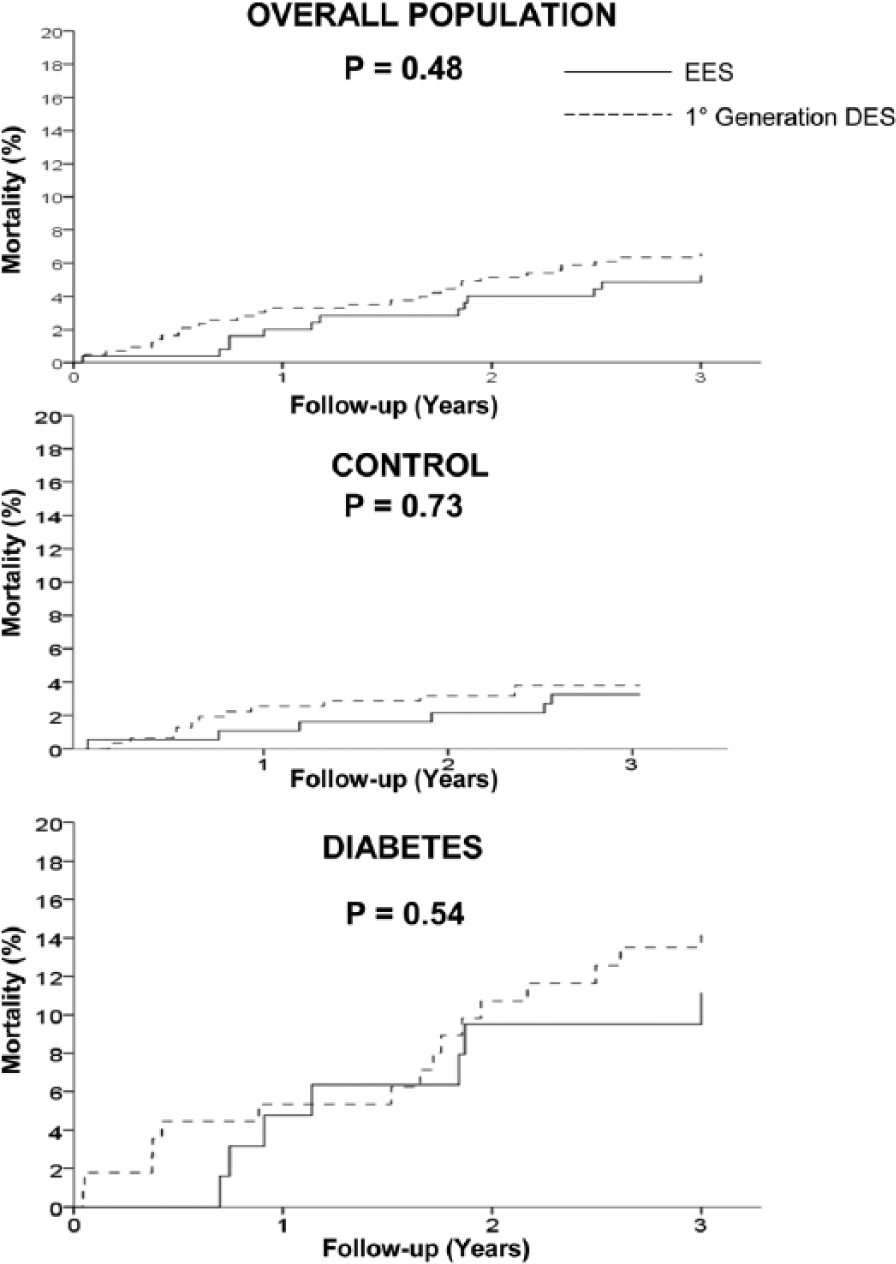
Kaplan–Meier curves showing the impact of EES as compared to first-generation DES on the occurrence of death in overall population (upper graph), in control patients (middle graph) and diabetic patients (lower graph).
reMI
reMI was observed in 55 patients (8%). As shown in Figure 6, no difference was observed between EES and first-generation DES (6.4% vs 9.1%, HR (95% CI) = 0.68 (0.38–1.22), p = 0.2). Similar results were observed among diabetic (14.1% vs 15.8%, HR (95% CI) = 0.84 (0.38–1.87), p = 0.67) and non-diabetic patients (3.8% vs 6.6%, HR (95% CI) = 0.55 (0.23–1.3), p = 0.17).
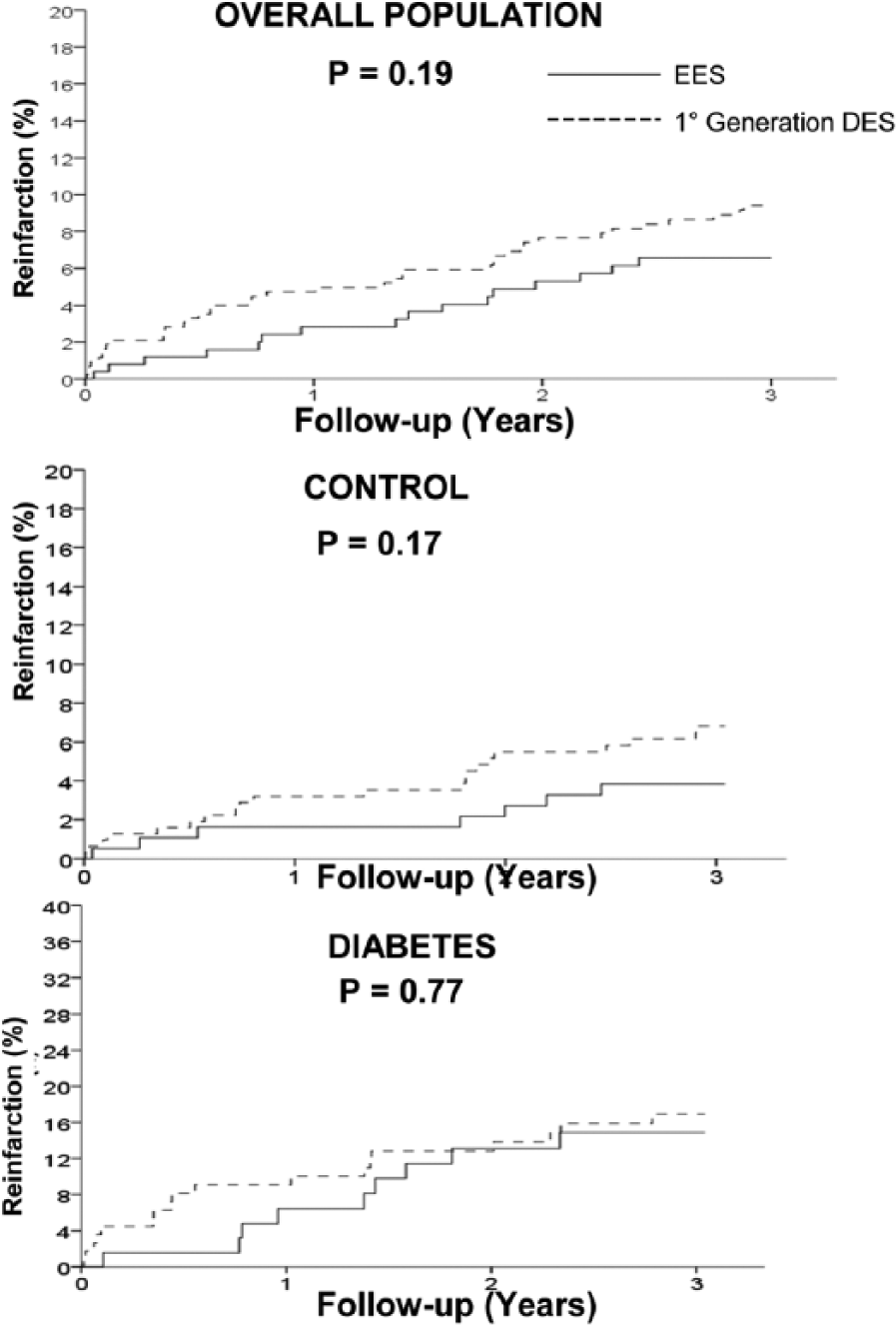
Kaplan–Meier curves showing the impact of EES as compared to first-generation DES on the occurrence of reinfarction in overall population (upper graph), in control patients (middle graph) and diabetic patients (lower graph).
Stent thrombosis
Stent thrombosis was observed in a total of 24 patients (3.5%). As shown in Figure 7, EES was associated with a significant reduction in ST as compared to first-generation DES (1.6% vs 4.7%, HR (95% CI) = 0.34 (0.11–0.99), p = 0.04). Interestingly, the benefits in ST with EES were observed only among diabetic patients (1.6% vs 9.6%, HR (95% CI) = 0.15 (0.02–0.98), p = 0.04) but not in control patients (1.6% vs 2.8%, HR (95% CI) = 0.56 (0.15–2.07), p = 0.39).
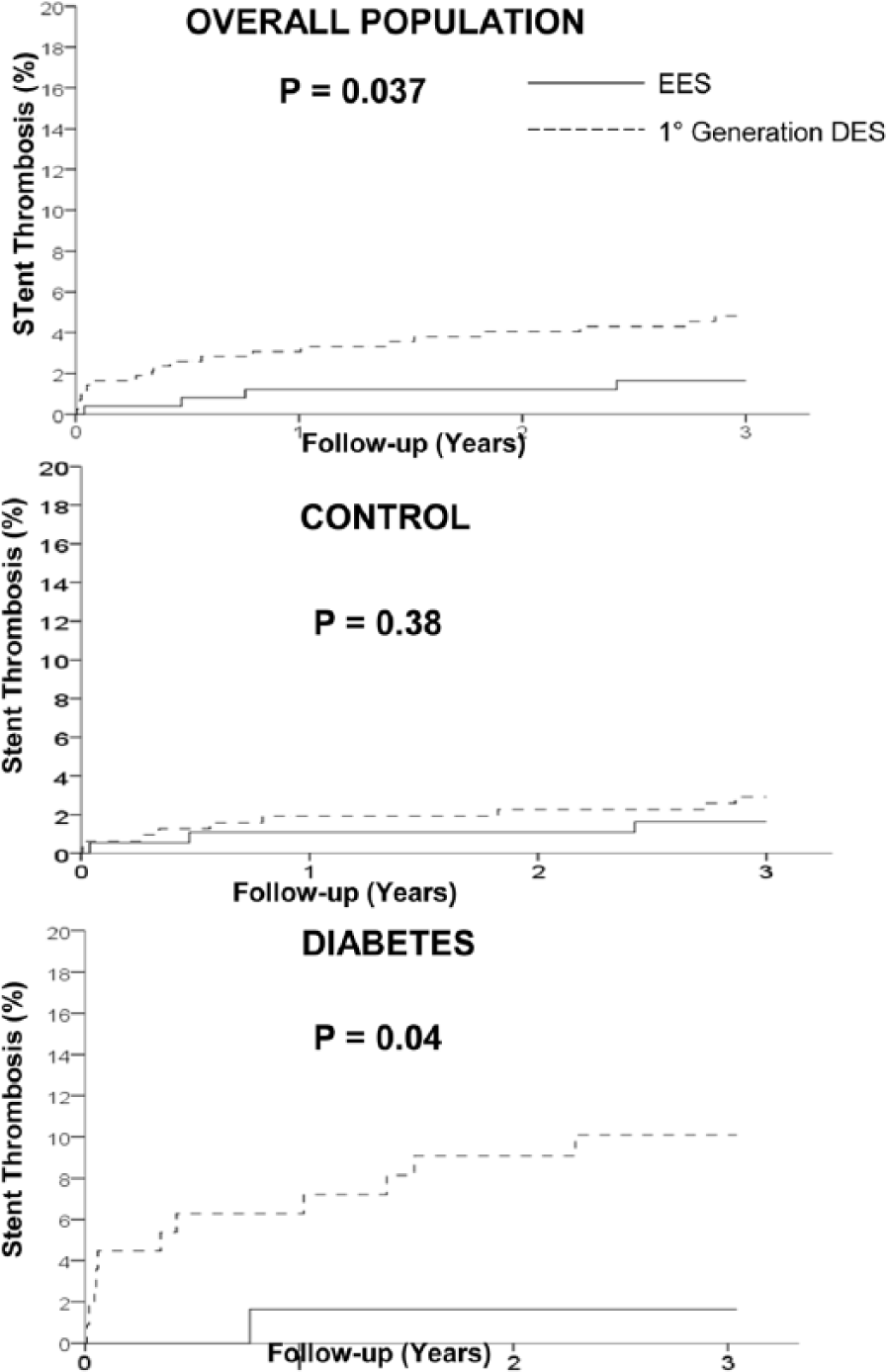
Kaplan–Meier curves showing the impact of EES as compared to first-generation DES on the occurrence of stent thrombosis in overall population (upper graph), in control patients (middle graph) and diabetic patients (lower graph).
TVR
TVR was observed in a total of 35 patients (5.1%). As reported in Figure 8, no difference was observed in terms of TVR between EES and first-generation DES (4.8% vs 5.3%, HR (95% CI) = 0.9 (0.45–1.8), p = 0.76). Similar results were observed among diabetic (9.4% vs 8.8%, HR (95% CI) = 1.09 (0.4–3), p = 0.87) and non-diabetic patients (3.2% vs 4.1%, HR (95% CI) = 0.77 (0.29–2.04), p = 0.6).
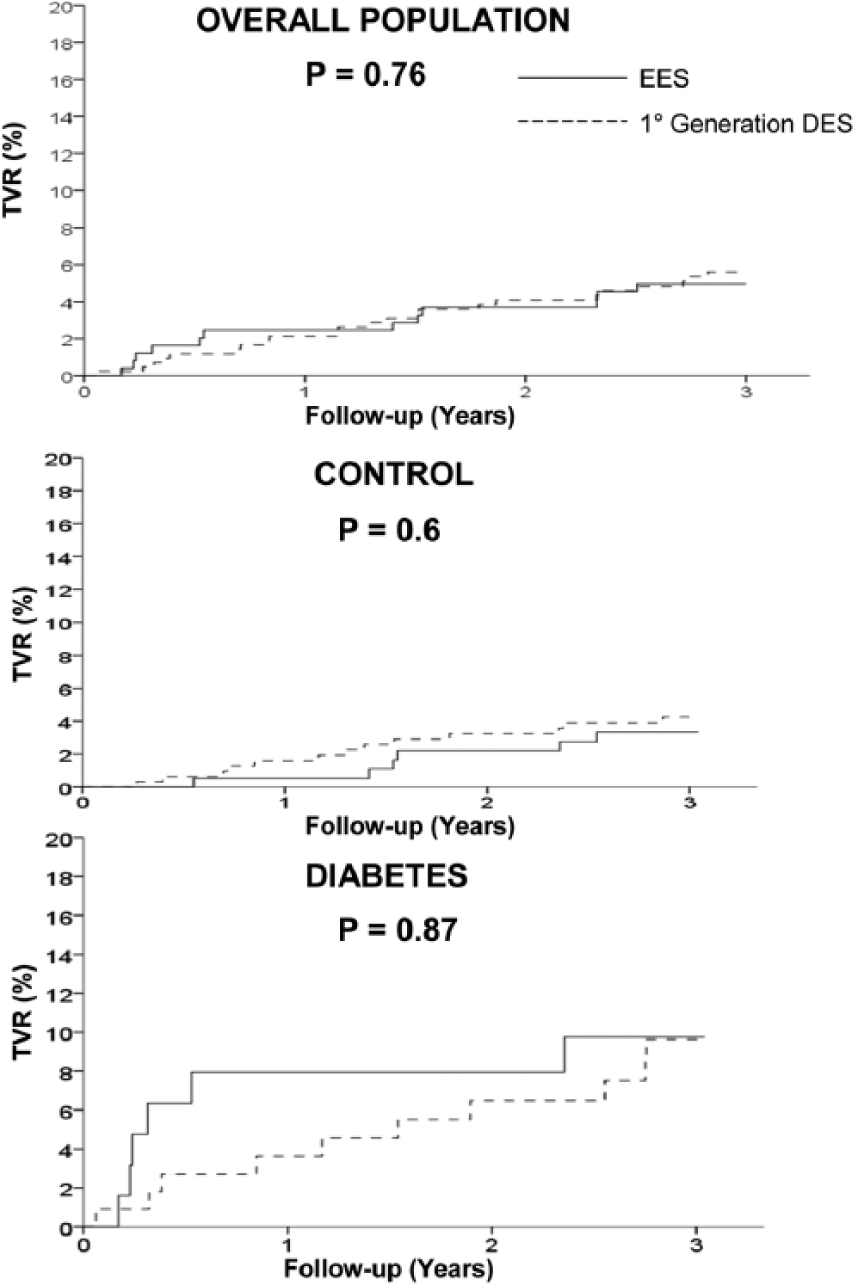
Kaplan–Meier curves showing the impact of EES as compared to first-generation DES on the occurrence of target vessel revascularization in overall population (upper graph), in control patients (middle graph) and diabetic patients (lower graph).
Discussion
This is one of the first studies evaluating the impact of diabetes on the benefits from EES as compared to first-generation SES and PES in patients undergoing primary angioplasty for STEMI. The main finding of this study is that at 3-year follow-up, EES as compared to first-generation DES performed similarly in both diabetic and non-diabetic patients in terms of MACE, death, reMI and TVR. However, EES provided significant benefits in terms of ST only among diabetic patients.
After initial safety concerns, numerous studies and randomized trials have demonstrated the safety and efficacy of stenting in the setting of STEMI.3 –6 A recent comprehensive meta-analysis in patients undergoing primary PCI have shown the benefits of stenting compared to balloon angioplasty alone in terms of reducing TVR, although no definite impact on death and reinfarction was present. 4 However, restenosis rates after BMS in STEMI patients are still high, especially in unselected patients with complex lesion morphology.5,6 Many randomized trials have been conducted therefore on the use of DES.7 –10 However, recent concerns have emerged regarding the risk of late stent thrombosis and death associated with DES. A recent individual patients’ data meta-analysis including more than 6000 patients has shown that first-generation DES are associated with a significant reduction in TVR, but higher rates of late stent thrombosis as compared to BMS. 10 Therefore, the attention of research has been focused on new DES technologies with more biocompatible or bioabsorbable polymers. Among elective patients, those stents have shown to further improve outcome as compared to first-generation DES. 19 Few studies have so far investigated new-generation DES in the setting of STEMI.
The Comparison of Biolimus Eluted From an Erodible Stent Coating With Bare-Metal Stents in Acute ST-Elevation Myocardial Infarction (CONFORTABLE-AMI) 20 compared biolimus-eluting stent (BES) with biodegradable polymer versus BMS in 1500 patients. At 1-year follow-up, MACE occurred in 24 patients (4.3%) receiving BES and 49 patients (8.7%) receiving BMS (p = 0.004). The difference was driven by a lower risk of target vessel–related reinfarction (0.5% vs 2.7%, p = 0.01) and ischaemia-driven target lesion revascularization (1.6% vs 5.7%, p < 0.001) in patients receiving BES compared with those receiving BMS.
In the Everolimus-Eluting Stents Versus Bare-Metal Stents in ST-Segment Elevation Myocardial Infarction (EXAMINATION) trial, 21 1498 STEMI patients were randomly assigned to receive EES or BMS. At 1-year follow-up, the primary endpoint (patient-oriented combined endpoint of all-cause death, any reMI and any coronary revascularization) was similar in both groups (11.9% in the EES group vs 14.2% in the BMS group; p = 0.19). However, EES was associated with significantly lower rates of target lesion and vessel revascularization (2.1% vs 5.0%, p = 0.003 and 3.7% vs 6.8%, p = 0.0077) and stent thrombosis (0.5% vs 1.9% for definite and 0.9% vs 2.5% for combined definite or probable stent thrombosis; both p = 0.019).
In the XienceV Stent versus Cypher Stent in Primary PCI for Acute Myocardial Infarction (XAMI) 22 trial, a total of 625 patients with AMI were randomized (2:1) to receive EES or SES. Primary endpoint was MACE at 1 year consisting of cardiac death, nonfatal AMI or any TVR. EES was associated with a significant reduction in the primary endpoint (4% vs 7.7%, p = 0.048), whereas no difference was observed in terms of cardiac mortality (1.5% vs 2.7%, p = 0.36), and definite and/or probable ST (1.2% vs 2.7%, p = 0.21).
In our previous report, 17 we found that among STEMI patients undergoing primary angioplasty, EES and SES equally performed in terms of efficacy (similar TVR rates), whereas EES was associated with a significant reduction in ST.
Several subanalysis of large randomized trials have fo-cused on the comparison between EES and first-generation DES in diabetic patients, showing conflicting results, with significant benefits with EES in some studies,23,24 whereas no difference was observed in other ones.25 –27
However, no data have been reported so far on diabetic patients with STEMI. In fact, diabetic patients have been shown to have a significantly worse outcome in terms of mortality, TVR and stent thrombosis. Therefore, the benefits from EES may be more pronounced among this high-risk subgroup of patients.
This is the first report evaluating the impact of diabetes on the effectiveness of EES as compared to first-generation DES in the setting of STEMI. We found no significant difference in outcome between EES and first-generation DES between diabetic and non-diabetic patients, with the only exception of stent thrombosis that was significantly reduced only among diabetic patients.
Limitations
Due to a relatively late randomization strategy (after initial angiography), patients have for the most part been selected, and thus, the conclusion of this trial cannot be extended to all patients undergoing primary angioplasty for STEMI. The usage of GpIIb–IIIa inhibitors have been significantly reduced across years, as they were administrated in 100% of cases in the PASEO trial and in 50.6% of the patients in the RACES-MI trial. Finally, a larger use of thrombectomy devices, by reducing the thrombotic burden, might have potentially affected the results of our analysis. 28
Conclusion
This study shows that among STEMI patients undergoing primary angioplasty, diabetes is associated with a significantly worse outcome at 3-year follow-up. A similar outcome was observed between EES and first-generation DES in non-diabetic patients, whereas among diabetic patients EES was associated with a significant reduction in stent thrombosis.
Footnotes
Acknowledgements
Prof. De Luca and Dr Di Lorenzo had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author’s contribution
G.D. Luca helped with (1) conception and design, (2) statistical analysis, (3) interpretation of the data, (4) drafting of the article and (5) final approval of the manuscript. E.D. Lorenzo helped with (1) data collection, (2) interpretation of the data, (3) drafting of the article and (4) final approval of the manuscript. R. Sauro, A. Varricchio, M. Capasso, T. Lanzillo, F. Manganelli, G. Carbone, F. Lanni, Maria Rosaria Pagliuca, G. Stanco, G. Rosato and H. Suryapranata helped with (1) interpretation of the data, (2) critical revision of the article for important intellectual content of the article and (3) final approval of the manuscript.
Declaration of conflicting interests
None of the authors have any conflict of interest to disclose with this study.
Funding
This study had no financial support.