
Abstract
Keywords
Introduction
CPD is any learning outside undergraduate and postgraduate education and is an essential component of the health service, as it provides support to healthcare workers to keep up to date with best practices and helps to address deficits in their knowledge and practice (Al-Ismail et al., 2022; Forsetlund et al., 2009). It is recognised that CPD remains an underutilised strategy of improving healthcare quality and safety (Davis & McMahon, 2018). The reasons for this are multifactorial ranging from poorly designed CPD activities that do not use objective performance data to failure to appreciate the learning needs of practitioners (Al-Ismail et al., 2022). There are arguments as to how effective CPD is in changing physicians practice due to the inherent challenges of measuring its impact (Mansouri & Lockyer, 2007; Samuel et al., 2021). A survey by the American Hospital Association found that most of its members felt that CPD was of value in addressing key competencies, such as medical knowledge and patient care, but found it to be less effective in promoting team-based care, system-based care delivery, communication skills and improving the efficiency of doctors’ practice (Combes & Arespacochaga, 2014).
The available CPD activities in some resource constrained settings can be classified as educational meetings, usually arranged by hospitals through their ‘in-service committees’ as well as by the relevant departments of health and in some cases non-governmental organisations. A Cochrane systematic review of 81 randomised control trials reporting on objective measures of professional practice or healthcare outcomes concluded that such meetings alone are not likely to be effective for changing complex behaviours (Forsetlund et al., 2009). Furthermore, the didactic nature of these meetings makes them not as effective unless used with other methods (Chekijian et al., 2021; Forsetlund et al., 2009).An additional concern is that in peripheral hospitals and health centres practitioners do not have the same opportunities to take part in CPD activities when compared to their colleagues in the main hospitals.
CPD looks at ways in which medical practitioners acquire new knowledge, competencies, and skills over the course of their career, and ultimately or hopefully improve patient care (Van Nieuwenborg et al., 2016). Continuous Medical Education (CME) is a component of CPD, though the terms have been used interchangeably consensus now views them as separate entities (The consortium et al., 2013).
This scoping review aims to summarise the information reported on CPD models since 2010. As there is currently no objective evidence to suggest that one CPD system is preferable or more effective than another (McBride et al., 2022; The consortium et al., 2013), it is hoped that some countries can learn important lessons from this scoping review as they move to establish or improve their own systems of continuing professional development.
Methods
The framework employed for this review was based on work done by Arksey and O’Malley, and further elaborated by Levac et al., as well as on the PRISMA checklist for scoping reviews (Arksey & O’Malley, 2005; Levac et al., 2010; Moher et al., 2009). The scoping review questions were as follows: 1) What CPD models are available in various settings globally? 2) What are the perceptions and views of medical practitioners towards these CPD models?
The inclusion criteria were as follows: 1. Studies reported in English that were published from 2010 to date. 2. Those that described CPD models in use, 3. Those detailing the perceptions and views of medical practitioners towards such interventions, irrespective of study design, 4. Commentaries, editorials, letters, studies and online sources (CPD guidelines and policies from regulatory authorities in the Sothern African Development Community (SADC) region and international ones) describing the CPD models.
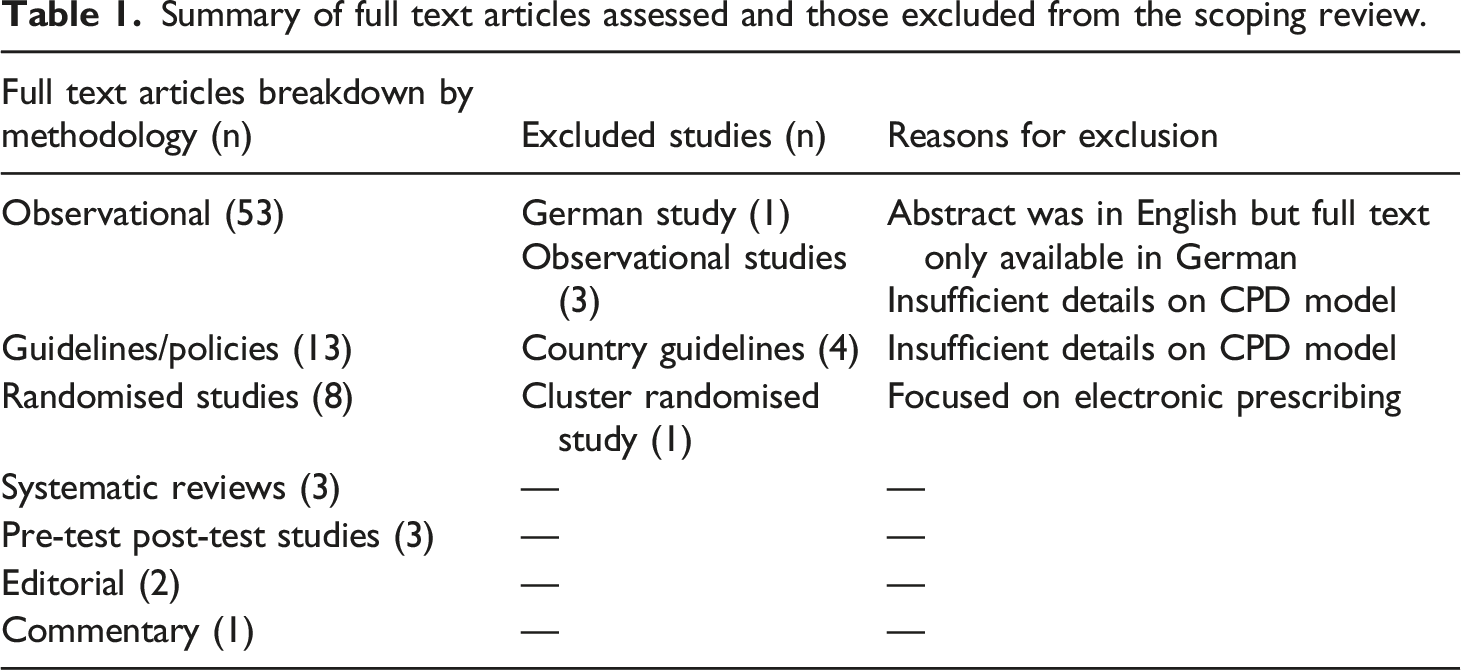
We excluded references that did not describe the CPD models in sufficient detail, and those where the full paper could not be obtained from the databases searched.
Search strategy and study selection
On 05 October 2021 and 21 April 2022, we searched PubMed, Web of Science and Scopus databases for articles published from 01 January 2010. The grey literature searches were restricted to regulatory authority websites in the Southern African (the authors’ practice setting), Australian, European and American regions, as these offered websites in English. The 2359 retrieved studies were exported into Mendeley, from which duplicates were automatically identified and removed. Two scholars (author 1 and 3) independently screened the titles and abstracts for eligibility, any inconsistences that occurred in their selection were solved by discussion. Finally, one scholar (author 1) ensured literature saturation by searching the reference lists of the included studies and the regulatory authority guidelines, where available.
Data extraction
A data extraction form was developed on an Excel® spreadsheet to collect the information necessary for data synthesis. Two scholars (Author 1 and 3) independently performed a pilot data extraction on a random sample of five articles and subsequently refined the form.
The extracted data consisted of
1. Publication characteristics: title, year of publication, author, author’s affiliation and country. 2. Characteristics of the CPD model: a) Population (e.g. general practitioner, physician), b) Study design (e.g. Randomised Controlled Trial), c) Details of implementation, d) Challenges 3. Practice points from the papers
The scholars (author 1 and 2) then independently performed data extraction for all studies except for the grey literature (guidelines from regulatory authorities) which was done by one scholar (author 1). Differences between reviewers were discussed and solved by consensus. The database and grey literature search yielded 1961 citations after deduplication (Figure 1), and after screening the titles and abstracts, 66 papers were included. A further 17 references from forward citation searching were included. Nine full-text articles were excluded during screening with reasons (Table 1) which resulted in a total of 74 references for full-text review. Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Moher et al., 2009). Summary of full text articles assessed and those excluded from the scoping review.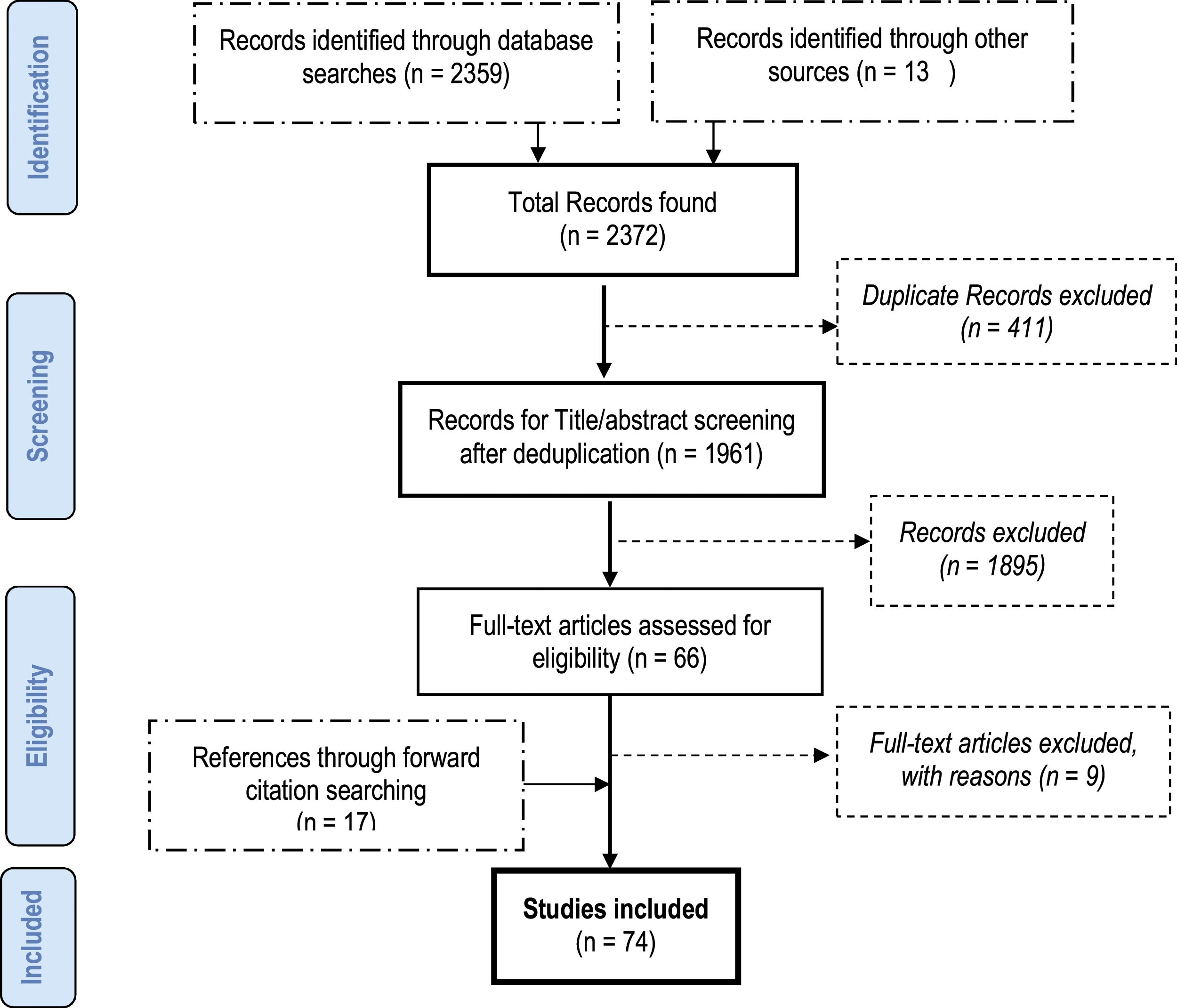
Data synthesis
Following data extraction, author one performed the initial categorisation using conventional content analysis (Allen et al., 2019), which was verified and refined by author three, with data being categorised with respect to the two questions: 1) What CPD models are available in various settings globally? a) Legislation, theoretical framework/learning theories b) CME credit systems, revalidation/recertification and maintenance of certification c) Content delivery (choice of format) d) Quality standards, monitoring and evaluation e) Funding f) Country/regional CPD models 2) What are the views and attitudes of medical practitioners towards these models? g) Barriers to CPD and practical solutions
Limitations
This scoping review has some limitations. Firstly, the methodological qualities of the studies were not assessed as it was not part of the scope of this study, the intention being to provide an overview of the evidence available from the past decade. Secondly, restricting the search to certain databases, or not having standard search terms for the individual databases searched and limiting the search period to the last decade, may have excluded relevant publications. This was intended to identify the most recent innovations in CPD and allow for a meaningful overview to be given, but admittedly means that important papers published before 2010 were excluded. Thirdly, it is possible that evidence of models may have been missed that has not been reflected in the published or grey literature but are used in practice. The section on the different CPD systems focused on regional Southern African countries and a few international examples for comparison. The local focus was due to the challenges experienced within this region being similar. However, this meant that other countries with potentially suitable systems were not reviewed. In addition, only those regional countries with clearly defined guidelines on CPD for doctors available online were considered.
Results
The data is presented with respect to the seven categories that were divided between the two research questions:
1) What CPD models are available in various settings?
a. Legislation, theoretical framework/learning theories
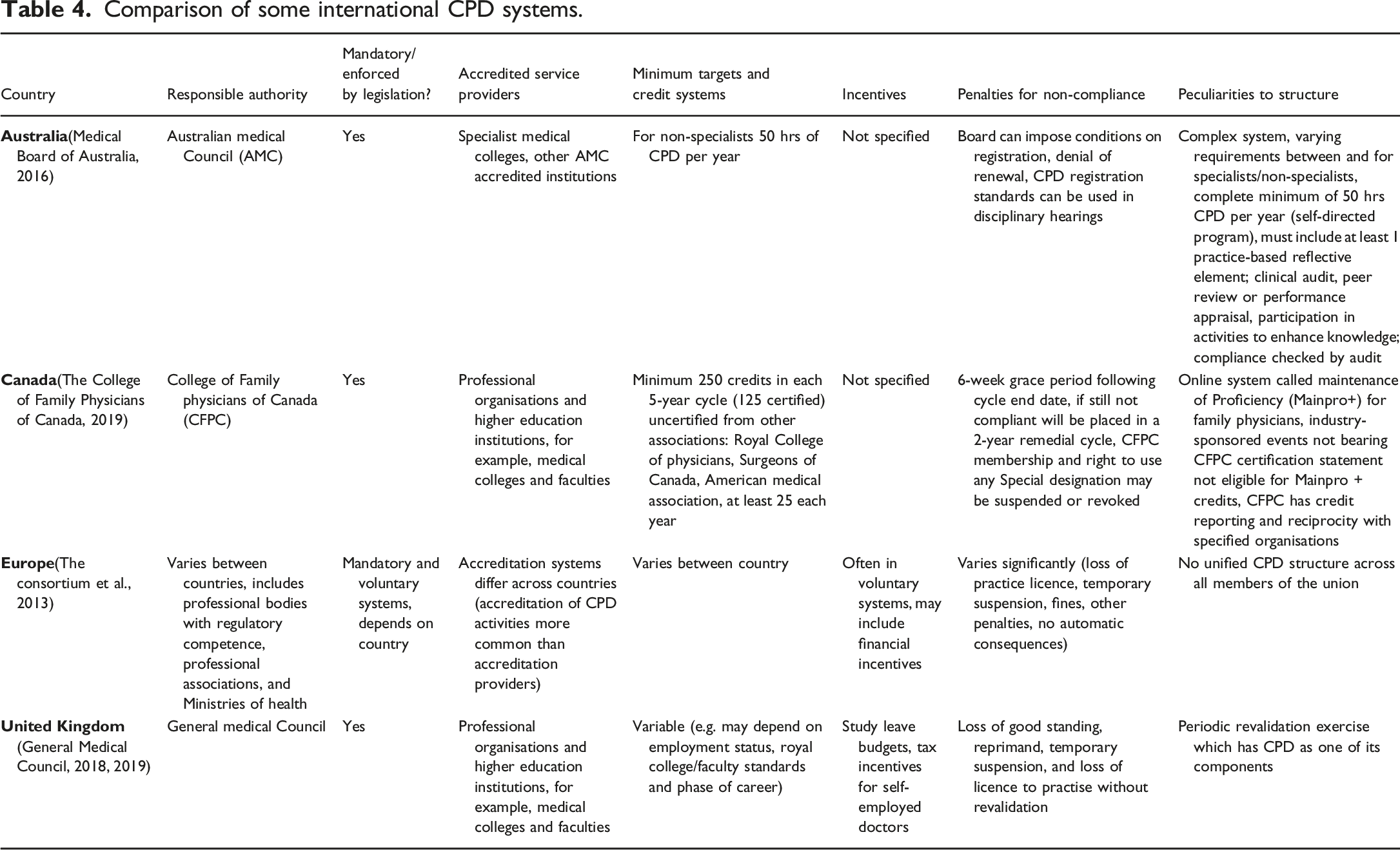
In most countries, governments (usually through quasi-state or professional bodies) have a legislative framework and a responsibility to implement and develop regulations impacting medical practice (Faghihi et al., 2017). There may however be no legal obligation for doctors to keep abreast of trends in their profession and mandatory versus optional CPD is a common discussion (Waheed et al., 2019). A structured program with clear and enforced targets encourages more widespread participation in CPD activities, but in some countries, practitioners address their identified needs and engage in CPD activities without legal enforcement (Abdul Samad et al., 2014). By 2014, a few European Union (EU) countries were still allowing self-regulation to ensure compliance with CPD requirements to maintain competence while most had specific systems in place (Solé et al., 2014).
Theory-based model development has been touted as one of the most effective ways to plan CPD activities, with some theories having been validated. Andragogy refers to the methods used by adults to learn, their learning process being different to children, and among themselves in terms of needs and styles (Seymour-Walsh et al., 2020a; Van Nieuwenborg et al., 2016). Adult learning theory (Andragogy) as described by Knowles (1985), has been used to develop some CPD programmes for doctors in Belgium, and focuses on five concepts, namely, self-concept (self-directed learning); adult learner experience (drawing from previous experience in order to learn new things); readiness to learn (easier to learn when there is a reason to acquire new knowledge or skill); orientation of learning (learn things that are applicable to their practice) and motivation to learn (want to learn for intrinsic factors, for example, to improve self-esteem, advance their careers) (Knowles, 1985; Van Nieuwenborg et al., 2016).
The theory of planned behaviour (TPB) and social learning theory were used in a Welsh study, in which ‘the why of change’ had its foundation in exposure to evidence and expert opinion, while ‘the how of change’ was rooted in clear communication strategies being taught to practitioners, allowing them to determine the unspoken motives and intentions of patients and respond appropriately to their needs (Bekkers et al., 2010). The TPB states that a practitioner’s behaviour is determined by the intention to perform certain clinical practices, these being favourably or adversely impacted by factors such as perceived behavioural control (ease of conducting the task) and subjective norms (influence form experts) (Tian et al., 2010).
Problem-based learning (PBL) is where learners improve their critical-thinking skills using clinical scenarios (Berjano et al., 2018). PBL, such as clinical case discussion facilitated by an expert, may be more appropriate than traditional lecture-based teaching (Berjano et al., 2018). A European study found that the effectiveness of PBL was enhanced when participants were allowed to anonymously respond to periodic multiple choice questions during the case discussion, the results of the voting system would then be discussed (facilitated by an expert) to enable consensus to be reached in a second round of voting (Berjano et al., 2018).
Reflective practice has been described in a number of papers, with one describing a variation of reflective practice, called the Practicum Script Concordance Test (Hornos et al., 2013). This uses an online platform to foster reflection on clinical practice through daily testing (using clinical scenarios) and detailed feedback on their performance in the scenarios, with an expert panel providing the answer key for the clinical cases (Hornos et al., 2013).
Quality improvement CME (QI-CME) integrates concepts of traditional CME with those of quality improvement (QI) (Shojania et al., 2012). One paper suggested four levels of integration that could be attempted, with the lower levels being simpler and less resource intensive than the higher ones (Shojania et al., 2012). Level one examined clinical areas with challenges (e.g. in diabetes management where focus should not only be about blood glucose control but also include foot care and diet counselling). This allows doctors to be sensitised about quality gaps in care of their patients while gaining knowledge on managing conditions. The second level is to overtly add QI in the CME of specific topics through the inclusion of sessions on how practitioners can identify and address gaps in their own practice. The third level was to complement second level CME with post-event outputs, where a scenario would be presented, and specific QI processes and goals taught that the practitioner could apply in their own practice. This could be submitted as a QI project to the CME providers for CME credit. The fourth level entails embedding CME in a larger QI strategy, for example, having a broader QI goal to improve a certain clinical problem or gap, then instituting multiple multimodal CME sessions in line with that goal and based on current best practices (Shojania et al., 2012). A QI-CME program called the ‘pink card’, a pocket memory prompt with indications and guidance on post-operative analgesic use for hand surgery resulted in a decrease in prescription size and standardised use of opioids in one United States of America (USA) study (Stanek et al., 2015). A growing proportion of CME activity in the USA is now part of the health system and institution quality improvement (Mcmahon, 2016).
Some authors have proposed learning from a cyclical assessment and feedback data model: a four-phase approach to CPD built upon using practice/performance data (Sargeant et al., 2013). In this model, the first step is to have access to data, this being available from sources such as electronic records, chart audits and patient surveys. Practitioners should be trained and afforded protected time to access the data. The second step is training doctors on data interpretation so they can engage with the data. Here, expert/peer facilitated reflection and feedback is important. The third step is using the data for learning and change; the practitioner is trained to make realistic goals and action plans to achieve them. The last step is the ability to measure outcomes and evaluate change (Sargeant et al., 2013).
Interactive strategies that are based on established education theory and evidence, founded on the perceived need of practitioners, and involve multiple exposures to material are effective ways to design CPD models (Mcmahon, 2016; Shojania et al., 2012). The CPD model should also encourage self-directed learning, allow time for practice, and consider the diversity of medical practice (Schostak et al., 2010; Zabar et al., 2010).
b. CME credit systems, revalidation/recertification and maintenance of certification
CME credit system may assist individuals to achieve the minimum level of learning required, and some countries have made them prescriptive and compulsory for practice license renewal (Faghihi et al., 2017). From 2010, the USA Medical boards required between 12 and 50 hours of CME credit hours yearly for re-registration (Yousem & Nidecker, 2010). There is a gradual shift worldwide from time-based to more value-based credit systems. While the challenges and complexities of relating such changes to health outcomes remains, there is general agreement that on its own a time-based system is inadequate (General Medical Council, 2019; Yousem & Nidecker, 2010).
Registration, revalidation and licensing are complex processes that may involve more than just CPD. These terms do not have one universal meaning, and depending on the country, may refer to the same or different thing. In some areas, licensing/registration is lifelong, while in others it is time limited, and practitioners can either apply for a license renewal or they may need to demonstrate ongoing competence or fitness to practice, this being known as revalidation in the United Kingdom (General Medical Council, 2019; The consortium et al., 2013). Workplace-based assessment (Multi-Source Feedback) is increasingly used to appraise competence and is part of recertification/revalidation process in Australia, UK and Canada (Narayanan et al., 2018). A European study described systems for ensuring fitness to practice in the European Union (EU) as falling in a continuum, from implicit to explicit (Solé et al., 2014). In implicit systems (e.g. in Spain), incentives are provided through voluntary accreditation and there is periodic assessment of competence, which has no bearing on their status as health care practitioners (Solé et al., 2014). In explicit systems, there are interventions (e.g. license revocation and fines) on licensing/accreditation, such as in the UK, where an external review of one’s practice is an additional requirement to CME program attendance (Solé et al., 2014). Other countries fall between the two extremes, such as Belgium and Hungary, where the level of regulation is not as stringent as in fully explicit systems but is not as relaxed as in implicit systems (Solé et al., 2014). In one country (e.g. USA), there may be differences within different regions and specialties regarding licencing requirements (Aparicio, 2015; Solé et al., 2014; The consortium et al., 2013).
The American Board of Medical Specialties (ABMS) approved the maintenance of certification (MOC) in 2000 to improve the quality of care offered by certified specialists and increase public accountability (Cook et al., 2015). While there is no argument that there is a need for doctors to maintain competence throughout their careers, there are differing views whether formal MOC is the way in which this can be accomplished (Sawalha & Coit, 2019). There is a paucity of data to fully support its implementation and controversy around how competence can both be developed and demonstrated (Cook et al., 2016; Sawalha & Coit, 2019). The cost and cost effectiveness of the MOC program is regularly debated, with many doctors viewing it as a burden (Cook et al., 2016). In 2010, the American board of Radiologists (ABR) introduced a MOC, which consisted of four levels of assessment, these being: cognitive expertise (examination), self-assessment, prescribed hours of CME credit and conducting a prescribed number of practice quality improvement measures (PQI) over a certain period (Yousem & Nidecker, 2010). The lack of awareness of PQI and complexities surrounding it has led to unfavourable views being expressed by doctors about MOC (Yousem & Nidecker, 2010). Others suggest wider acceptance of MOC is possible if it is integrated into everyday clinical work and relevant to local needs (Cook et al., 2016). However, doctors distrust the board-certifying institutes and feel that MOC has increased the burden on practitioners who are already prone to burnout and early retirement (Sawalha & Coit, 2019).
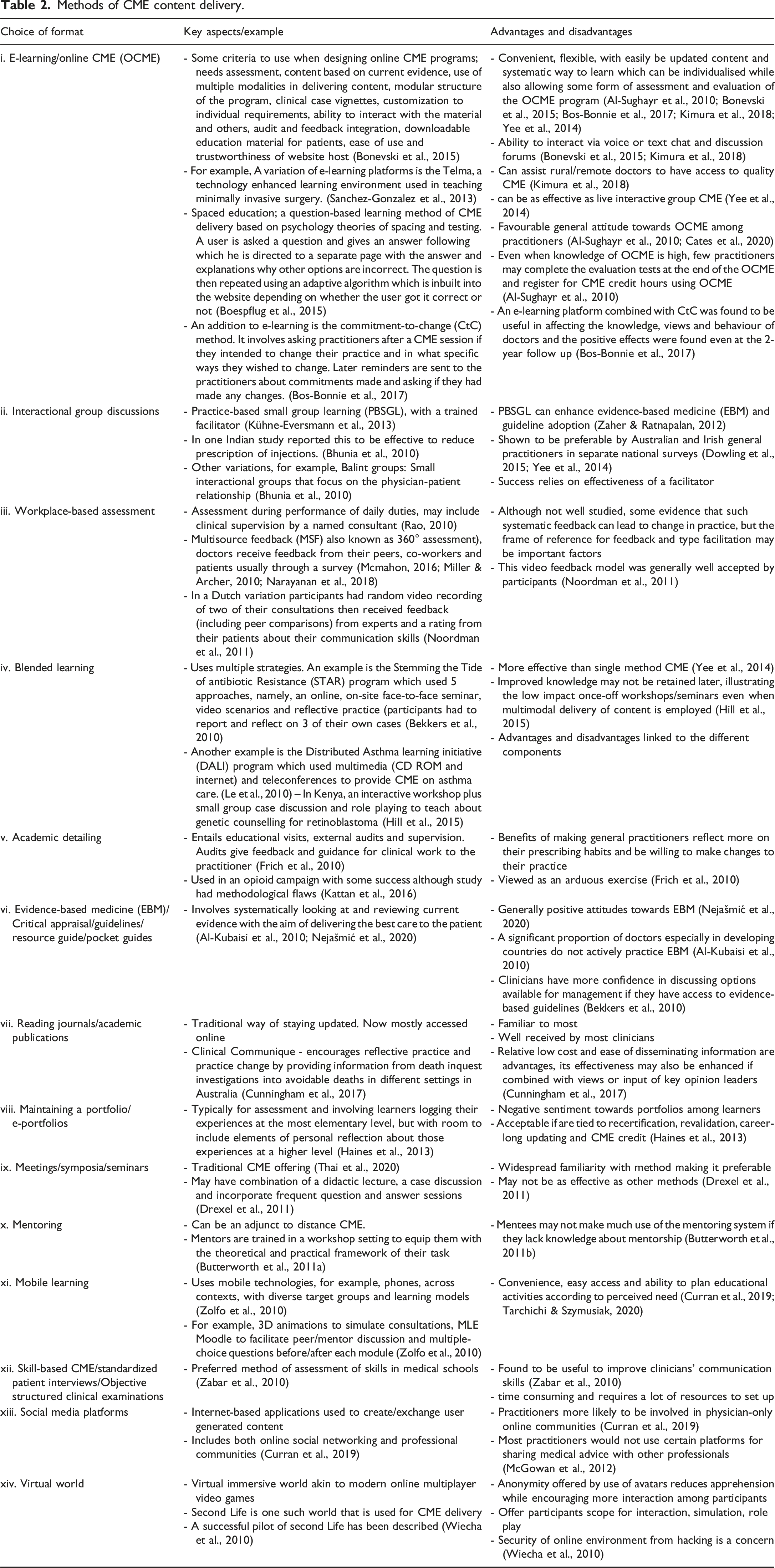
c. Content delivery (choice of format)
Methods of CME content delivery.
d. Quality standards, monitoring and evaluation
There are few validated theoretical frameworks for evaluating CME (Tian et al., 2010). One of the more widely used models for evaluation is Kirkpatrick’s four level outcome evaluation model that looks at training effectiveness, with the contents being evaluated in terms of reaction, learning, behaviour and results(Tian et al., 2010). There have been various adaptations of the model, specifically for CME evaluation, including one in which the four levels are modified to learner satisfaction, learning outcomes, performance improvement and health outcomes (Tian et al., 2010). In this adaptation, there is a gradual shift from one level to another, with information gained from the previous levels being used as the foundation for the next. This is time consuming and requires complex analysis to progress to the next level (Tian et al., 2010).
A paper by Somasekhar et al. discusses Moore’s seven level pyramid of outcomes measurement (participation, satisfaction, learning, competence, performance, patient health and community health), and contends that a growing public health awareness has resulted in the latter four components being required for meaningful CME (Somasekhar et al., 2012). However, there is an increasing need to assess higher level outcome measures, which are time consuming, complex and costly to measure. The paper also lists audits and patient chart reviews as the preferred methodologies to evaluate outcomes of CME programs (Somasekhar et al., 2012). The USA Accreditation Council for Continuing Medical Education (ACCME) stipulates that CME providers should evaluate their programs using outcome measures to obtain accreditation (Cook et al., 2015). Another resource is the adaptable 12 item instrument for assessing the impact of CME on physician behaviour change based on validated socio-cognitive theories (Légaré et al., 2017).
Pre and post-test assessments are usually used to evaluate CME related knowledge gain, while Objective Structured Clinical Examinations (OSCEs) can be used to assess skill acquisition and questionnaires can be used to assess the intention to change practice (Fraguas et al., 2020). The issue of ensuring the quality of a CPD/CME activity is another area of concern. One paper identifies indicators of quality for a CME program which include self-assessed improved knowledge, growth in the number of participants, mean length of time users spend on e-learning platforms, improvement of practice and guideline adherence (Van Nieuwenborg et al., 2016).
e. Funding
One of the most contentious aspects of CPD programs relate to how they are funded, with self-funding through registration fees often being seen as a burden to practitioners who may thus be unwilling to participate (Stephenson et al., 2020). Despite this, registration fees constituted the largest source of accredited CME funding in the USA in 2018 (McMahon, 2018). However, government supported CPD programmes (such as the UK CPD support grant for staff doctors in England) indicate that in settings where resources permit, this model can assist in reducing the burden of additional costs on the health practitioner (Bimpong et al., 2020).
Pharmaceutical industry funding is common globally, with most conferences and approximately half of the revenue of educational companies involved in CME coming from commercial sponsorship (Torgerson et al., 2022). However, in the current regulatory environment which insists on objectivity and freedom from commercial bias, there is a reluctance to promote such sponsorship, even when there is evidence that such industry funded programmes can be unbiased (Chekijian et al., 2021). Measures put in place to ensure this impartiality include peer review of CME content (material), development of content in the absence of industry influence, declaration of conflict of interest among organizers/presenters, and prohibiting marketing activities within the meeting area (Chekijian et al., 2021; Torgerson et al., 2022). Some have cautioned that there may still be some subtle bias in industry funded CME modules; they appeared to minimise dangers of opioid use (death and addiction) while promoting (through use of a new disease term Breakthrough pain), off-label use of the drug fentanyl for chronic rather than cancer pain (Infeld et al., 2019).
Other authors have suggested that there is a need to institute clear policies to avoid ethical conflicts related to funding, and identified four components to include (Sahm, 2013; Torgerson et al., 2022). Firstly, establish code of ethics to guide the professions; secondly, have clear guidelines to deal with how practitioners will relate with pharmaceutical companies, limiting payments that can be made, and enforcing financial disclosure rules. Thirdly, have programs to ensure that doctors have a robust academic mind-set, and lastly, establish and enforce laws that impose penalties for unethical conduct and encourage vigilance in adherence to the policies (Infeld et al., 2019; Sahm, 2013).
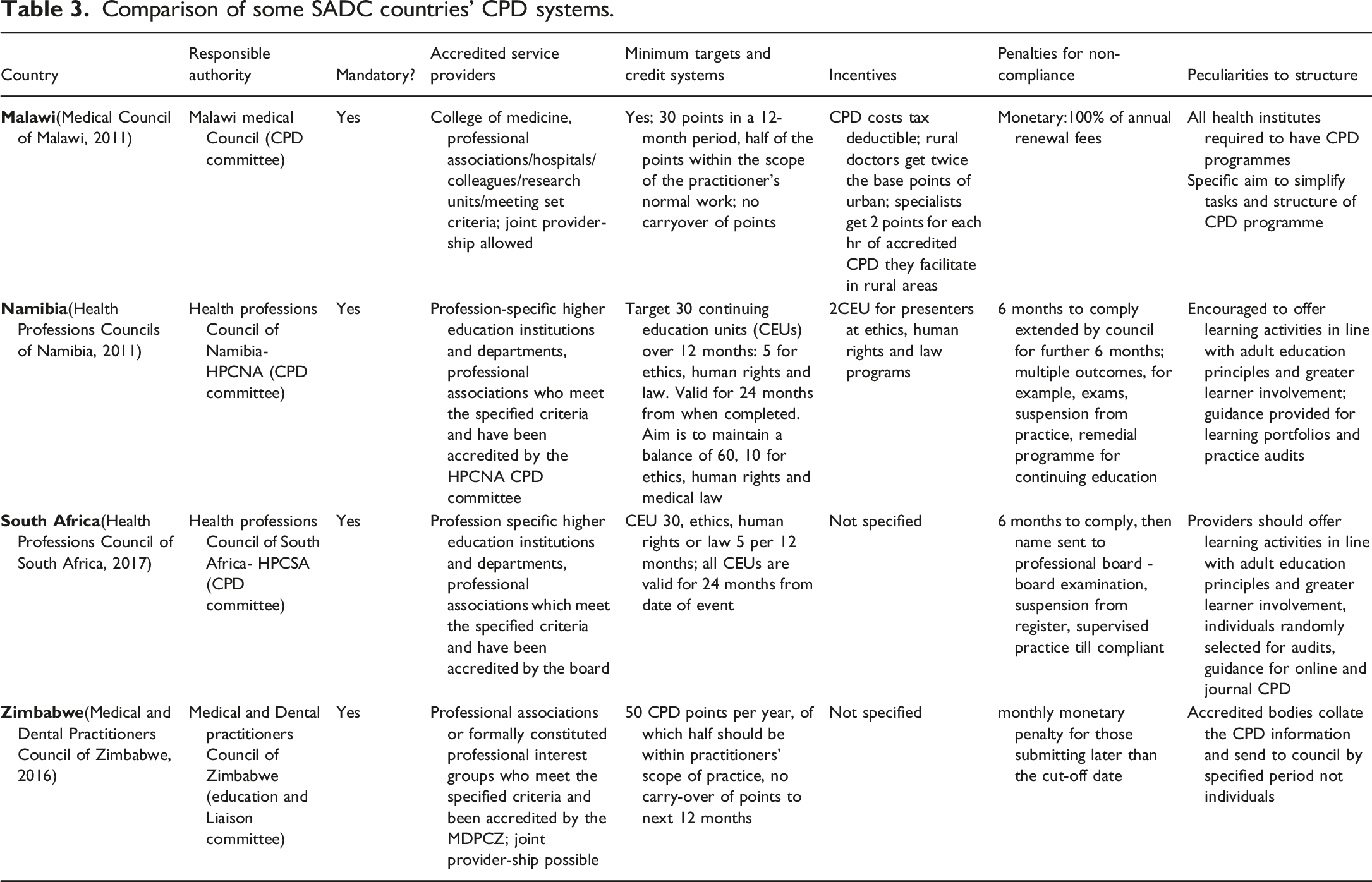
f. Country/regional CPD models
Comparison of some SADC countries’ CPD systems.
Comparison of some international CPD systems.
2) What are the views and attitudes of medical practitioners towards these models?
Barriers to CPD
Impractical CME programmes and content, which fail to address the needs of practitioners and issues they face in their daily practice are common (Faghihi et al., 2017). This can be addressed by continuous needs assessments (Simper, 2021).
Barriers to CPD and suggested solutions.
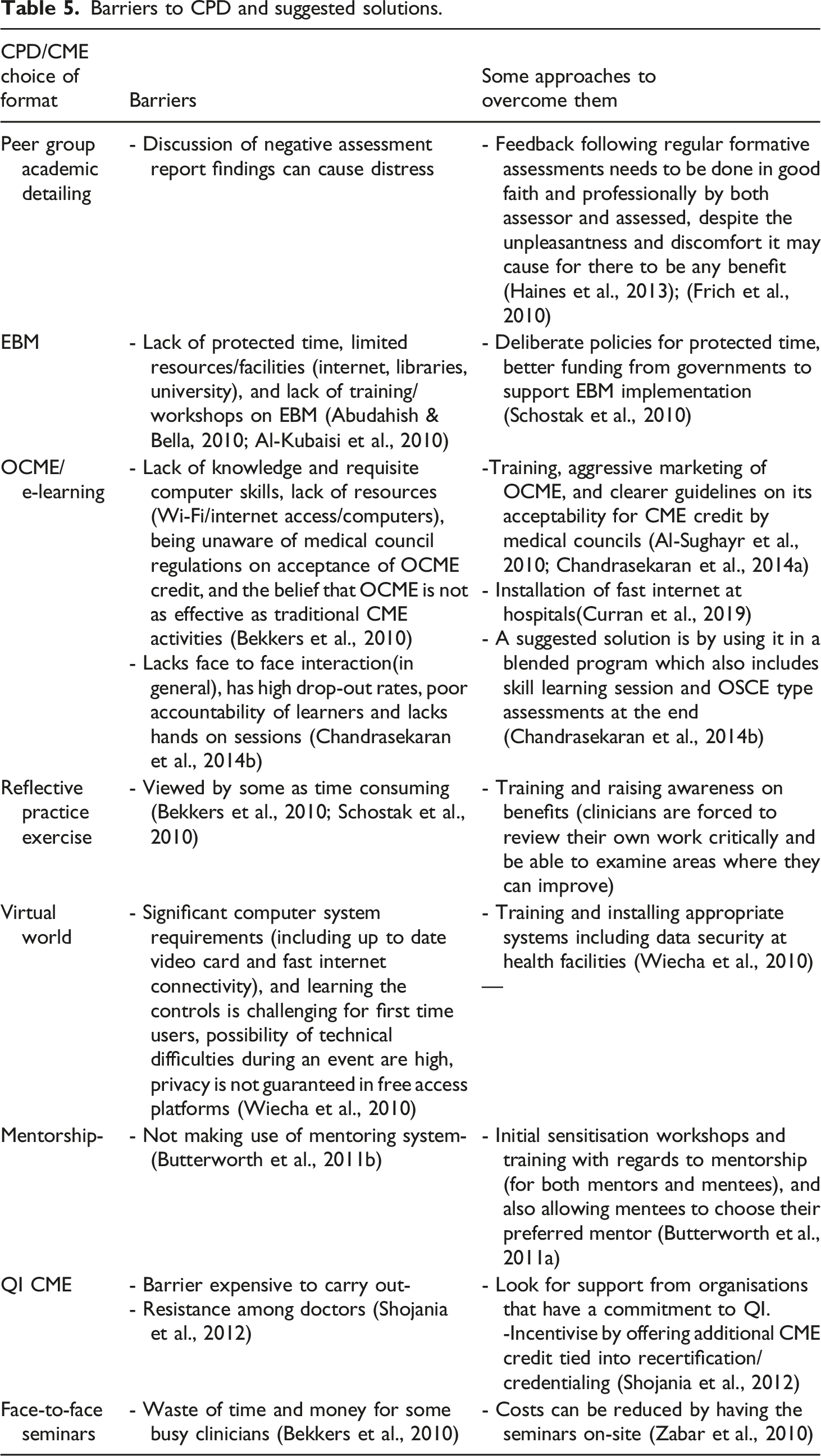
Time constraints are usually sited as a barrier to participation in CPD activities; in the UK protected time for CPD is offered to address this (General Medical Council, 2019). Online CPD activities can also assist by being flexible enough to allow practitioners to participate at their convenience (Chandrasekaran et al., 2014).
Costs of CPD are often prohibitive and most countries acknowledge these challenges(Stephenson et al., 2020). Partnerships with pharmaceutical companies under strict ethical guidelines may assist in addressing this. The initiative by the South African Medical Association (SAMA) through its company Medical Practice Consulting (MPC) which offers online journal access is a good example. Some of the access to these journals is industry sponsored (MP Consulting, 2019).
Availability of mentors/expert advisors is an important barrier especially in developing countries. In Nepal, partnering with established institutions through teleconferencing facilities allowed practitioners in less resourced areas to access CPD activities and expert advice (Butterworth et al., 2011a). Faculty development through mentorship training of specialist and other key opinion leaders is a sustainable way to build local expertise (Butterworth et al., 2011b).
Access to appropriate CPD activities is often a challenge (Arisanti et al., 2019). Given that medical practice is very heterogeneous, a CPD model designed for anaesthetists may not necessarily work for general practitioners (Schostak et al., 2010). Trying to accommodate this heterogeneity comes at a significant financial cost.
Discussion
1) CPD models
a) Legislation, theoretical framework/learning theories
A legislative framework is a fundamental requirement in ensuring credible CPD. This framework can be further enhanced by multilateral agreements which ensure standardisation of CPD policy in specific regions of the world. A consultative process with various stakeholders to determine whether the model adopted should be mandatory or optional is important as there is no evidence to suggest that one is more effective than the other. The appeal of a mandatory system is that it is in line with many other countries in the world and may ensure widespread participation. The downside is that significant resources will be required to make CPD available to all practitioners.
Regulations for accrediting CPD activities should include a requirement that all of them should be based on validated theories. There is no evidence that any of the theories is better than others; however, there is consensus that the use of a validated theory improves the learning experience and potentially influences adoption of what has been learned into clinical practice. QI-CME can be introduced in CPD activities because of its potential to improve healthcare systems and patient care. A cyclical assessment and feedback data model may be difficult to implement in resource constrained settings due to the challenges of obtaining adequate practice data since electronic records are not widely available. It may be possible to implement using inpatient records for practitioners working in public hospitals and facilities in which detailed paper records are kept.
b) CME credit systems, revalidation/recertification and maintenance of certification
Although time-based CME points systems are giving way to value-based credit systems, they are still widely used in the Southern African region. It is important for countries to consider recognition of the CPD credits from other jurisdictions should they meet certain clearly defined and agreed upon standards. The number of CME credits per year is a matter which can be determined through a wide stakeholder consultative process. Such a process would consider the available CPD opportunities and how these vary between different regions. In the countries considered in this review, around 30 to 50 points per year is the standard, (Health Professions Council of South Africa, 2017; Medical and Dental Practitioners Council of Zimbabwe, 2016; Medical Council of Malawi, 2011).
The responsible authority should accredit CPD providers, using well defined regulations outlining criteria for an organisation to get provider status. It is possible to grant provider accreditation to universities, hospitals, non-governmental institutions and professional associations if these meet a set of established criteria. Joint-provider-ship agreements are an important consideration in limited resource settings as they can potentially increase available CPD activities. Clear regulations should be provided to specify the roles of accredited and non-accredited provider organisations. The regulations should also ensure ethical conduct of CPD offerings to ensure commercial bias is minimised.
Maintenance of certification and similar models as used in the United States remain very controversial with their processes, costs, cost-effectiveness and outcomes in question even to date. More research is needed in this area.
c) Content delivery (choice of format)
Given the diverse ways in which CPD content can be delivered, it is prudent that a variety of formats be used if they meet a set criterion as defined by the regulating authorities. In resource constrained settings, it may be difficult to use such methods as virtual world and OSCEs. However, it is possible to take advantage of telecommunication technologies which can facilitate mobile and web-based formats. Improving access to Wi-Fi and training of practitioners on use of different web and mobile technologies will assist wider adoption of CPD. Specialists and other experts can be trained on mentorship and be involved in mentorship programmes in more remote areas. They can also be requested to assist in developing CPD material and adapting material (including guidelines) from other countries and the WHO to their local setting. Even where there are few specialists available, they would have more impact on the health system by being able to mentor general practitioners through such formats as interactional group discussions, mobile/web-based leaning, social media platforms and academic detailing. Use of technology also allows CPD activities happening at major hospitals to be shared with practitioners in private practice and those in remote settings. It also enables international faculty to assist in delivering content.
Social distancing measures and other restrictions that have come with the coronavirus disease (COVID-19) pandemic have limited face-to-face teaching and learning and promoted online CME delivery (Seymour-Walsh et al., 2020b). Even courses for COVID-19 by WHO have been made into OCME offerings. Some have argued that this should not be viewed as a temporary measure but should be taken as an opportunity for improving access and quality of OCME to benefit clinicians in rural and remote regions (Seymour-Walsh et al., 2020b).
An understanding of the capability of online systems for online learning is important for choosing the most appropriate one to adopt for CPD (Seymour-Walsh et al., 2020b). OCME delivery can be both synchronous and asynchronous and thus is a convenient way to deliver content to busy clinicians who can catch up with the content later if unable to attend live events. Potential distractions are well documented barriers to learner engagement with material in online learning. It is therefore important to clearly define expected conduct before each interactive session (e.g. turning off push notifications and placing phones on silent mode) (Seymour-Walsh et al., 2020b). Another consideration is limiting the amount of information into smaller bits that can be well understood and applied, while ensuring that the session involves significant interaction among participants (Seymour-Walsh et al., 2020a). OCME should be critiqued and assessed using a validated framework to ensure that it meets the set objectives and required standards.
d) Quality standards, monitoring and evaluation
Although currently there is no consensus on how quality standards of CPD can be monitored or evaluated, there is a general agreement that behaviour change, and patient outcomes are important considerations. To this end, one of the methods above which have been shown to have utility, the Kirkpatrick’s four level outcome evaluation model and its adaptations can be used (Tian et al., 2010). These allow gradual shift from basic evaluation (reaction and learner experience) to more complex measures such as performance improvement and health outcomes.
e) Funding
Sustainable funding strategies are essential for the success of any CPD model, as financial limitations are likely to adversely affect the quality and quantity of contents available. Various incentives can be put in place to ensure that practitioners are not overburdened by cost of the CPD program and can include tax incentives and government subsidies for the fees. Engaging with industry partners and non-governmental organisations to fund programs can be beneficial but should be done in the presence of a suitable framework that prevents unethical practices and bias.
f) Country/regional CPD models
It is important to have clear, simple policies relating to CPD. The common findings, such as the mandatory nature of CPD, time-based credit systems and the presence of penalties for non-compliance are important considerations in drafting a CPD policy. It is also important to consider incentives to make the program more accessible and affordable to practitioners, specifically those in resource constrained settings.
2. What are the views and attitudes of medical practitioners towards these models?
An understanding of the perceived and real barriers encountered in various CPD models allows for them to be minimised. The model must incorporate regular needs assessment to keep it relevant to its target group, and to create capacity to develop local content through available experts.
In terms of learning formats most studies reviewed emphasised the use of multiple methods and encouraged interaction and feedback. Blended learning is preferred by many practitioners, its main barrier being cost (Bekkers et al., 2010). All material developed for use needs also to be based on relevant peer reviewed evidence and evidence-based medicine is an important one consideration. Internet-based learning is set to increase and installation of fast internet at all hospitals and health centres is key in enabling available resources to be used effectively. Practitioners will also need to be trained on the use of mobile technologies and on critical evaluation of data available. Clear guidelines on the acceptability of online-CME activities for CPD credit are needed. Traditional face-to-face seminars are popular but are costly and may not be suitable for busy clinicians or doctors working in more remote areas. The use of technology platforms which allow live streaming, remote participation or recording of events and viewing it later, can assist. Interaction between facilitators and practitioners during educational meetings can be addressed by redesigning such activities to be in line with adult learning theories. The cost of CPD can be significant and affects its accessibility. Tax incentives, funding from pharmaceutical companies and other NGOs, partnerships with universities and other organisations can be encouraged under well-defined guidelines.
Conclusion
A CPD model that is supported by appropriate legislation, addresses the needs of the doctors, and is based on valid adult education theories is likely to be both effective and acceptable to medical practitioners. Additionally, it should include a blended way of delivering its content while keeping abreast with current best practices. There should also be a mechanism to conduct continuous quality assessments and improvement in knowledge and practice for better patient care and outcomes. The model should take cognisance of the views of various stakeholders (including doctors, patients, regulatory authorities and government) and have a sustainable funding model. More research is required into effective methods of identifying individual practitioners’ learning needs to make relevant CPD activities. Also essential is research into CPD needs and barriers to participation in CPD for each category of medical practitioner (various specialties and general practice) as these may be unique to the group. At government level it is important that policies are developed that foster continued evolution of CPD. Further research is required to evaluate the learning outcomes of CPD offerings on healthcare quality and sustainable funding models (and related policies including implementation).
Supplemental Material
Supplemental Material - Continuing professional development in the last decade – A scoping review
Supplemental Material for Continuing professional development in the last decade – A scoping review by Rodney H Magwenya, Andrew John Ross and Logic S Ngatiane in Journal of Adult and Continuing Education
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.