
Abstract
Continuing medical education (CME) is essential for medical practitioners to update their knowledge and skills periodically to provide clinical care in keeping with the evidence available. Traditional methods of CME such as workshops, conferences, and seminars are helpful to bridge the gaps in practice. With advancing technologies, online format is used to deliver CME with appropriate modifications. Although there are distinct advantages of online CME in regards to wider reach and flexibility, there are certain drawbacks beyond just technological limitations. Interactivity using ingenious ideas may be required to motivate and engage learners during online CME.
Keywords
Traditional vs Online CME
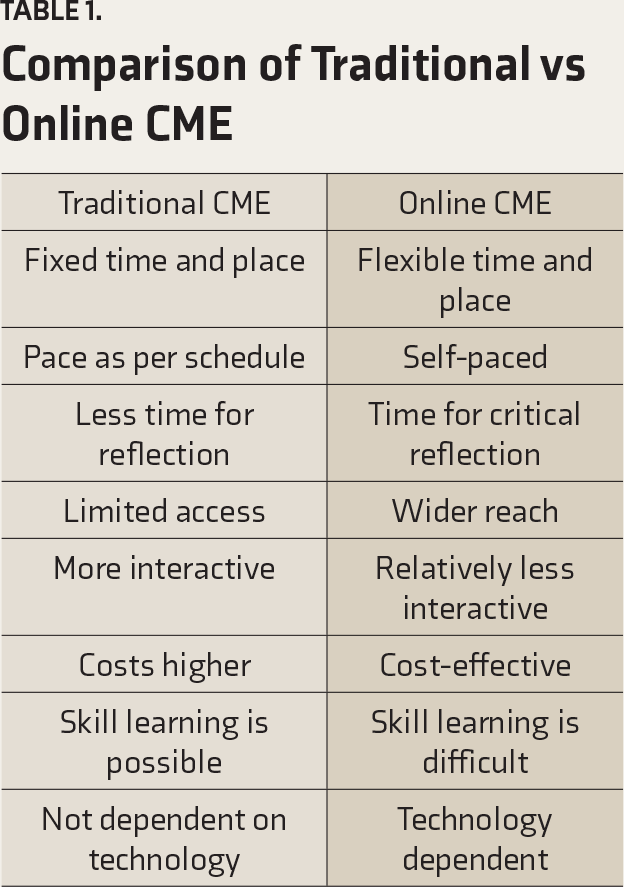
Comparison of Traditional vs Online CME
CME has also been delivered online using telemedicine systems, which allow remote delivery of content without any geographical limitation. One way to expand the reach of traditional CME to remote audiences is the transmission of live activity through satellite or the internet. Depending on the type of delivery, it can be either synchronous (i.e., in real-time) or asynchronous (i.e., prerecorded content is available to the participants to access at their convenience). Teleconferencing is a real-time and live interaction between participants in different locations using audio and/or video, for the purpose of CME.
Theoretical Frameworks for Online CME
In developing CME activities, including online ones, the adult learning principles should be employed. Knowles described an adult learner as someone with self-directedness who requires education to be (a) relevant to their practice, (b) in keeping with their learning style, and (c) in a nonthreatening and supportive manner. 7 Adult learning includes self-directed learning, which is characterized by discipline and motivation, critical thinking, ability to reflect and be self-aware, curiosity, openness and flexibility, independence and self-sufficiency, information seeking and retrieval skills, and good general learning skills. 8
Adult learning involves the principle of reflective practice, which includes abilities such as self-appraisal and self-awareness during learning, that is, reflecting on the content and process of learning. 9 Such reflection may result in developing zones of mastery around the areas of competence, that is, practicing almost at an automatic level. Kolb described a similar internal process of “experiential learning,” in which the learner moves, through reflective observation, from concrete experience to a more abstract understanding of a concept. 10
Also relevant for online CME is situated learning theory, which encourages learners to construct meaning together by integrating what is already known and experienced, with the new information gathered in a specific context. 11 In these situated environments, learning results from collaborative engagement within “communities of practice,” that is, “groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly.” 12 Major components of situated learning include problem-based learning activities to increase learner motivation and engagement, access to expert guidance and feedback, a kind of “scaffolding” that provides a cognitive framework for learning (e.g., providing learning resources, templates, or guides), and opportunities to consider multiple perspectives through interactive discussion and reflection.
Advantages of Online CME
The most important advantage of online CME is the possibility to exchange health information and provide education over a distance, without the need to move the participants, including patients, practitioners, or educators, that is, distance learning. In settings that have a solo practitioner or fewer professionals to carry out the work, it may not be feasible for them to travel to a distant site to attend the program. Added to this is the cost of travel and logistics, which can sometimes be prohibitive, especially for international events. The broad geographical reach of online CME is a definite advantage for many learners. This is of particular advantage in pandemic situations (e.g., COVID-19 pandemic of 2020), with travel restrictions and safety precautions in place, when only the online mode of CME is possible.
Most online CME programs will be based on self-directed learning principles, which have several advantages. They can be flexible and self-paced, that is, performed as per the learner’s schedule. The learning material can be used at convenient speeds, and revisited and the content revised as necessary. Multiple exposures to the same content are known to enhance learning and retention, but the options for that are limited in traditional CME. The inclusion of self-assessments can enhance reflection and the learning experience. For the instructor, the possibility to teach a large group of participants over a wide geographical area is an added benefit. These advantages can be summarized in the phrase “anytime, anyplace.”
The use of video teleconferencing allows two-way interaction between the participants, with an experience almost like face-to-face meetings. With good quality cameras and other advanced technologies, it is possible to have veridical experience during online CME. A good platform or application to run the event enhances user experiences, especially if it has many built-in interactive elements. With the simultaneous use of multiple elements, such as videos, transcripts, discussion boards, and quizzes, different learner needs can be satisfied. It is possible to access the educational content using a wide variety of interfaces, such as personal computers, laptops, tablets, or even smartphones. Also, with wider availability of broadband network facilities, Wi-Fi connectivity has resulted in accessing educational content synchronously from almost anywhere.
A variety of educational programs can be conducted online. The online equivalent of seminars, called webinars, allows the delivery of educational content using the internet, with the possibility of some interaction between the presenter and participants using online interactive tools. They can accommodate more participants than a physical conference room setting that could be limited by space and accessibility. Webinars provide the participants the convenience of attending an academic presentation from the comfort of their offices or homes. This can be particularly useful for very focused topics with very few interested persons around the world, which can lead to the development of communities of practice. These groups can adopt online technologies to enhance social ways of learning. For example, the use of chat rooms can enhance interactions that may be personal as well as on work-related topics. As needed, more formal discussions around clinical topics, either synchronous or asynchronous, are possible. Some forms of asynchronous discussion may be preferred by busy clinicians who find it challenging to make arrangements for face-to-face meetings, teleconferences, or online synchronous conferences. Another advantage of online CME is the possibility of inclusion of several experts in a panel discussion, which may be, due to logistic reasons, difficult in physical CME.
Disadvantages of Online CME
Many educators believe that self-directed, informal methods of learning are not as effective as traditional CME and that they should not be equated. For most of the traditional programs, especially those organized by medical associations, there is some screening of the speakers by a committee, thus ensuring some quality standards. However, this may be less stringent for online CME and webinars, some of which could be self-styled and self-promoted, as exemplified by the current flurry of webinars with the COVID pandemic. In such situations, it will be incumbent upon the participants to carefully choose which webinar to attend, as against most standard CME programs.
There is some, albeit older, evidence to suggest that many clinicians prefer traditional CME delivery methods over online programs.13, 14 Specifically, online learning may not appeal to those who prefer face-to-face contact with teachers or fellow learners. Also, interactions in a traditional CME go beyond the classroom to other areas, including dining tables, which may foster networking and other collaborations, which is possible only with socialization.
As we understand more about the use of online technologies, it has become apparent that to be effective, just like off-screen education, these activities must be interactive in order to engage the learner and improve their impact. In this context, there is a limitation regarding which interactions can happen during an online CME. The experience of online interaction itself is very different from that of in-person interaction. When the streaming is such that only the slides are visible on the screen (or, even if the presenter too is visible, it is only the person’s face, that too in a small rectangle in a corner of the screen), communication through nonverbal means gets hampered and the communication becomes less effective. Interruptions due to technical reasons too can adversely affect the experience of learning—It is not uncommon to see poor video quality and pixelation, voice cracks, freeze, and drops. Similarly, though access to the CME is possible through many types of devices, the experience may be very different with smartphones as compared to large-screen computers. It is also possible that devices that are commonly used for the purpose of fun and entertainment, when used for a serious academic purpose, may not elicit the same level of engagement from all learners.
As the online CMEs are dependent on technology, which is not uniform across the country, their accessibility may be limited in areas with poor internet connectivity and low bandwidth. Also, accessing the CME content from home or other places with multiple other distractions may be very different from the experience of sitting in a hall dedicated to the CME program, where one can focus more on the task at hand. Furthermore, during online CME, participants may get involved in other work whilst “watching online content,” which may reduce their concentration and complete participation.
Efficacy of Online CME
The efficacy of telemedicine for improving clinical outcomes has been established. However, the efficacy of online CME using telemedicine is less researched. Kirkpatrick and Kirkpatrick have described assessment at four levels to evaluate the effectiveness of learning
15
:
Reaction, which is studied by feedback from the participants and includes initial comments, overall experience, satisfaction levels, etc. Learning, which involves knowledge and skills gained, examined as pre- and post-tests. Transfer, which involves changes in behavior after the training program and is evaluated 3–6 months following the program. Results, which include changes in patient outcomes as a result of changes in practice.
Several studies have reported a positive experience and increase in physician knowledge following online CME (Kirkpatrick levels 1 and 2), but few studies have examined their effects on practice behavior and patient outcomes (Kirkpatrick levels 3 and 4).16–18
There is very weak evidence that online CME is actually superior to traditional CME.19–23 Cook et al., in their systematic review, suggested that elements such interactivity, practice exercises, repetition, and feedback are associated with improved learning outcomes in online formats, whereas the evidence for other variations in online instructional formats (e.g., the spacing of material, blended learning, use of animations) was inconclusive. 24
A pragmatic effectiveness trial may be challenging to carry out, as the major difference between traditional and online CME involves geographic accessibility. Also, several e-learning modules and CMEs are created by a wide range of public and private organizations, and there is no pedagogical standard to examine the quality of these courses. At most, the content and course development have been examined as some of these require accreditation and certification.
Quality of Online CME
Many times, the online CME often consists of “re-purposed” live, formal activities. As we start to understand the nuances of the use of rapidly developing technologies, it is becoming more apparent that principles of online learning could be very different from those of learning in traditional CME. The elements should, instead, evolve over time to increase the quality of learning experiences. Establishing a “set of standards,” in the form of quality criteria, will help optimize online learning.
Rather than merely repurposing content that was intended for a live audience, it is preferred that online education be designed appropriately for the medium. Talking heads or dense pages of text will not keep the learners engaged. Developing for smaller formats such as hand-held devices requires even more sensitivity to sizing and length of content.
Based on a consensus, the following quality criteria have been proposed for developing online CME modules; they should (a) be needs-based, (b) be presented in a clinical format (using case vignettes), (c) use evidence-based information, (d) permit interaction with content and experts, (e) facilitate and attempt to document practice change, (f) be accessible for later review, and (g) include a robust course evaluation. 25
Future of Online CME
Regardless of content, these technology-based activities allow for new approaches to CME. For example, online communities of learners can be formed to allow for follow-up reminders, reporting of practice changes, as well as networking and consulting among peers. These groups can assist in evaluating the effectiveness of the education as well as determining the needs for new activities. However, these online CME need to be accredited by MCI or SMC.
Planning an Online CME
All CME should be learner-centered, relevant to learners’ needs, able to engage learners actively, and able to bring about behavioral changes. 26 Hence, multiple teaching strategies, rather than only a single lecture or simple online text, are essential for changing the practice behavior of clinicians. 27 Certain design elements and strategies are common to both traditional and online CME, such as need assessment, educational objectives, identification of learning outcomes, building on prior knowledge, learner engagement and interactions, feedback and guidance on learning, and authentic assessment methods that contribute to learning. The following are essential elements while planning online CME.
Needs Assessment
All CME, including online ones, should cater to the needs of learners. The clinical care gaps should be established and the educational objectives determined based on these needs. This can be accomplished by using surveys or interviews or even from studies on patient outcomes.
Educational Objectives
In the recent decades, there has been a change in the focus of learning objectives. The desired outcomes have changed from simple acquisition of knowledge to more complex outcomes involving skills, changes in practice, and patient outcomes. All CME, including online ones, should focus on these higher-order learning outcomes.
Educational Content
The actual content of the CME should be given to “content-experts” who have requisite knowledge, skills, and expertise in teaching and have demonstrated credibility in the field. They should have the ability to deliver the content, synthesizing the available evidence without any bias and in a manner that effectuates behavioral changes in the learner.
Format
CME may be likened to a teaching intervention that can be strategically planned to improve learner outcomes. The PRECEDE model is a structural framework for a behavior change intervention. 28 It suggests that while planning a CME, one should consider the predisposing elements (characteristics of the participants, such as knowledge, beliefs, values, and attitudes), enabling elements (social and environmental factors such as access, resources, and skills), and reinforcing elements (positive or negative feedback from others).
Interactivity
Effectiveness of learning is improved by increased interaction between the expert and the participants and among the participants themselves. Use of case-based discussion, multiple strategies to promote interactions, and appropriate use of formative assessments are required to ensure enough interaction.
Strategies
A back-up plan should always be ready because issues, such as technical problems with the devices, speaker backing out, may arise. As the target participants are busy clinicians, online CME should stick to time. Some of the time spent for interactions between the participants, speakers, and the technology can be perceived as a waste of time by certain participants, leading to frustration and reduced motivation in them. 29
Orientation
A period for online orientation, prior to the actual program, may help the speakers and the participants to learn how to access the site, get familiar with the app, install browser plug-ins, learn how to download and upload files, and in general, become used to the technologies. This time can also be used to introduce the speakers and the participants, instill in them a sense of community, and enhance the opportunities for interactions.
Tools
The choice of learning resources and tools should be based on the appropriateness to that particular learning activity rather than going by the latest fad or trend, which may hamper learning. It should not be based on assumptions about the age, skills, knowledge, or preference of prospective participants.
E-Moderating
Although moderating an online discussion is similar to moderating a face-to-face discussion, there are substantial differences. Salmon has described the five-step approach for e-moderating. (a) Access and motivation: Participants are welcomed and made familiar with the e-learning material. They may need help with technical aspects during this step. (b) Online socialization: Participants begin interaction online, which leads to the formation of a group identity. The role of the moderator is to ensure participation of all, that is, encouraging the lurkers to engage actively. (c) Information exchange: Participants are actively involved with course content and online activities. Moderators provide encouragement and guidance in participation. (d) Knowledge construction: Participants discuss the content and come up with new knowledge. The moderator facilitates discussions, summarizing the progress. (e) Development: At this stage, participants take active responsibility for learning online, and the role of the moderator is more supportive and may be to respond occasionally. 30
Research on Online CME
Educational research is limited in the Indian setting, and effectiveness of CME, including online CME, has not been evaluated. Most published research is limited to feedback from participants or a pre- and post-test to examine the changes in knowledge. More research is needed to study higher-order changes, that is, behavioral changes in practices and patient outcomes (Kirkpatrick levels 3 and 4), to demonstrate the effectiveness of online programs. This is relevant in the context of a pandemic of webinars in the background of the current COVID-19 situation, which has curtailed all face-to-face CME activities. Standards need to be formulated, based on established quality criteria, to evaluate the online CME.
Recommendations for Regulating Online CME
In India, CMEs are regulated by MCI and SMCs, which mandate at least 30 accredited CME credit hours every five years for renewal of registration. 13 The quality of CME is monitored by the accrediting bodies, based on the organizing body, speakers, topic, duration, and feedback from participants. 13 The CME credit hours vary from 2–4 for a full day event, for which prior approval is necessary. 3 Online CME should be included by MCI and SMC at par with traditional ones, and accredited based on the consensus quality criteria 25 listed above. More elaborate criteria to evaluate the quality of CME is given by the Accreditation Council for Continuing Medical Education. 31
Conclusion
Clinicians are encouraged to regularly update their knowledge and skills and maintain the standards of clinical excellence required for the optimal care of patients through CME that is aimed at improving performance and optimizing the outcomes of practice. Rapidly evolving technologies have made it possible to develop and implement high-quality online CME courses that can meet the diverse needs of practitioners with convenient and flexible access. However, there is limited evidence to conclude that online delivery is superior to traditional CME. Also, interactive elements are essential to increase motivation and engage learners online, maybe, more so than in conventional settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.