
Abstract
Background
Palliative care is an essential component of health responses in humanitarian settings, yet it remains largely unavailable in these settings, due to limited availability of palliative care training for healthcare professionals. Online training programs which connect experts to clinicians in the field have been proposed as an innovative strategy to build palliative care capacity humanitarian settings.
Objective
To describe the implementation and evaluate the impact of delivering palliative care education using an established virtual learning model (Project ECHO) for healthcare clinicians working in the Rohingya refugee response in Bangladesh. Program acceptability and the impacts on learners’ self-reported knowledge, comfort, and practice changes were evaluated.
Methods
Using the Project ECHO model, an education program consisting of 7 core sessions and monthly mentoring sessions was developed. Each session included a didactic lecture, case presentation and interactive discussion. Surveys of participants were conducted before and after the program to assess knowledge, confidence, and attitudes about palliative care as well as learning experiences from the program.
Results
This virtual palliative care training program engaged 250 clinicians, including nurses (35%), medical assistants (28%) and physicians (20%). Most participants rated the program as a valuable learning experience (96%) that they would recommend to their colleagues (98%). Participants reported improvements in their knowledge and comfort related to palliative care after participation in the program, and had improved attitudes towards palliative care with demonstrated statistical significance (p < 0.05).
Conclusions
Virtual training is a feasible model to support healthcare providers in a humanitarian health response. Project ECHO can help to address the urgent need for palliative care in humanitarian responses by supporting healthcare workers to provide essential palliative care to the growing number of individuals with serious health-related suffering in humanitarian settings.
Keywords
Introduction
Palliative Care in Humanitarian Crises
Palliative care aims to alleviate physical, psychological, social, and spiritual suffering for individuals with serious progressive illnesses and their families. Despite the significant burden of health-related suffering and mortality, palliative care has been largely absent from humanitarian crisis responses.1,2 The 2018 Lancet Commission on pain relief and palliative care highlighted this need, describing an “abyss of access” while also identifying that basic palliative care interventions are relatively affordable and are “an essential component of any response to humanitarian emergencies and crises”. 3
In a recent global palliative care mapping study, Bangladesh was categorized as level 3a, which describes a country with “isolated palliative care provision” and Bangladesh was noted to have patchy provision of poorly supported palliative care services. 4 There are more than 600 000 people who are estimated to need palliative care at any point in time, but only a few palliative care services – primarily in the capital city of Dhaka – are in place. 5 The majority of individuals with cancer do not seek medical attention before the disease is advanced; and more than 80% of the individuals presenting to a tertiary cancer hospital (National Institute of Cancer Research and Hospital) have incurable disease at the time of presentation. 5
Despite availability of sustained-release and immediate-release oral morphine in Dhaka, opioids for pain relief are rarely available outside of the capital, leading to a significant burden of preventable suffering. Restrictive drug control policies, a lack of training among doctors and other health professionals, and myths regarding morphine lead to poor access despite demonstrable clinical need. 6 Furthermore, palliative care training is not comprehensively incorporated into professional training programs for physicians, nurses, or other healthcare professionals.
Palliative care education represents a critical step to increase access to this essential care in Bangladesh and other low- and middle-income countries (LMICs).
Project ECHO
Project ECHO (Extension for Community Healthcare Outcomes) is an online technology-enabled educational model designed to strengthen the knowledge and skills of community-level health care providers by providing remote teaching, guidance, and mentorship. In this model, multi-point videoconferencing is utilized to connect local healthcare providers (“spokes”) with specialists at a “hub” site (Figure 1).

Hub and Spoke model used in Project ECHO.
Project ECHO has been proposed as an innovative strategy to address the significant need for palliative care education in settings where resources are limited. Several studies in LMICs have described programs using Project ECHO to provide palliative care education and mentorship in these settings.7,8 A 2019 systematic review examining the impacts for healthcare providers participating in Project ECHO programs, identified very few studies in LMICs and the quality of evidence of most studies was low. 9 Several more recent studies of palliative care Project ECHO programs in Bangladesh and India report increased clinical knowledge and skills for participants.7,10
Despite the potential benefits of virtual learning, there are significant challenges to its implementation in resource-limited settings, including a lack of face-to-face interaction and the need to ensure adaptation of the training materials to the local healthcare environment and resource realities. 11 Virtual training programs in humanitarian crisis situations have not been widely reported, and this setting presents even greater challenges for such programs, including rapid staff turnover and poor internet connectivity. Exploring the use of virtual learning in humanitarian settings, using Project ECHO, will be important to guide the development of online education programs for future humanitarian health responses.
We developed and implemented a Project ECHO on Palliative Care for healthcare workers in the Rohingya Refugee Response in Bangladesh (RRC ECHO). The program is a partnership between Two Worlds Cancer Collaboration (TWCC), Palliative Care in Humanitarian Aid Situations and Emergencies (PallCHASE), and the Fasiuddin Khan Research Foundation (FKRF). The goal of the program was to develop a supportive learning community focused on strengthening participants’ confidence and skill in providing basic palliative care.
This study aimed to describe the implementation and evaluate the impact of delivering palliative care education and training using Project ECHO in a medical humanitarian response. We sought to assess program acceptability, and the impacts on learners’ self-reported knowledge, comfort, and practice changes.
Methods
Program Development
Learning Needs Assessment
We previously conducted 3 in-person training workshops (2-4 days duration) on palliative care for healthcare workers in the Rohingya response between June 2018 and Jan 2020, in Cox’s Bazar, Bangladesh. Participant and faculty feedback from these workshops informed the RRC ECHO program’s learning goals and helped to establish key topics for the program, which were further refined during the preparation phase (January - July 2020). We also incorporated experiences from experts and key leaders, as well as knowledge from our previous experiences with Project ECHO programs in India, Bangladesh, and Nepal. 7
Leadership Team Development
We established a core leadership team of physicians, nurses, pharmacists, social workers, and a project coordinator with experience in palliative care education in Bangladesh and in humanitarian settings. This interdisciplinary team included local and international palliative care experts. The team met during the planning phase to develop the learning program and share experiences regarding the healthcare system in the region, including information about the availability of essential palliative care medications and supplies.
During the first iteration of the course, the leadership team met after each session to debrief, review participant questions and comments, and strategize about necessary modification to the program. This facilitated rapid evolution to meet any shifting educational needs of the participant audience. After the first series of the course, the leadership team chose to reduce the frequency of debriefing to once or twice per course as course content became more firmly established.
Leadership team participants included 12 health care professionals (6 doctors, 3 nurses, 2 pharmacists, and 1 social worker) with expertise in palliative care, including 4 faculty members from Bangladesh, 1 from Kenya, and 7 from high income countries (Canada, US, The Netherlands). There was also 1 local program coordinator who provided technical and administrative support.
Course Content
Through a series of workshops, the leadership team developed the course structure and the topics for 7 core sessions. A pilot course (first cohort) was conducted in August to October 2020 and subsequent modifications were made to further adapt the content to the local healthcare situation. Didactic and case presentation content was peer reviewed by faculty members familiar with the local palliative care situation and medication availability to ensure that treatments discussed were available. Wherever possible, course content was tailored to the Rohingya humanitarian crisis. After the first cohort, the content was finalized, translated into Bengali, and video lectures were recorded in both Bengali and English (see Table 1).
Summary of Rohingya Refugee ECHO session topics.

*Topics both covered in one session.
**this topic was repeated twice due to high levels of interest.
Mentoring session topics are determined by discussion among the leadership team, which was based on feedback from course participants and included topics of relevance or interest to local health care professionals. This also included specific learning gaps that the faculty identified. Mentoring sessions are also intended to increase awareness about palliative care among the wider community of health care professionals in the Cox’s Bazar region.
Program Recruitment
We contacted local healthcare organizations and healthcare providers via social media, text messages, telephone, and word of mouth to invite healthcare providers to join the RRC ECHO. All healthcare providers were welcomed to participate free of charge. For the first two session of the course, participants who are not registered are permitted to join to explore whether the course was of interest to them, and were then encouraged to register to ensure if they wished to complete the course and be eligible to receive a certificate.
Program Structure
The RRC ECHO program includes 2 components: 7 core course sessions and ongoing mentoring sessions. The 7 weekly core course sessions cover key palliative care topics; participants are required to engage in all 7 sessions receive a course certificate. Optional monthly mentoring sessions are interspersed with the core sessions and are open to all previous and current participants and other health care workers in the region. These mentoring sessions provide continuing professional development through support as well as ongoing mentoring for past course participants.
Each core session consists of a short didactic teaching session which summarizes content from a 20–30 minute video that participants are required to watch before the teaching session itself. Faculty presentations are followed by group discussion and then a faculty-driven case presentation. Each case is designed to generate further discussion and provide opportunities for participants to reflect on implementing new content into clinical care.
Mentoring sessions follow a similar format, but without pre-recorded videos. For both types of sessions, participants are encouraged to participate actively in the discussion and ask questions either verbally or through the virtual chat. Several faculty members monitor and respond to chat questions throughout each session.
Learning Materials
After each live session, the session video recording is shared with participants, as well as key learning points and presentation materials (articles, slides). Participants are encouraged to join a private WhatsApp chat moderated by faculty, providing a forum to share additional resources and answer participants’ questions. Such asynchronous learning is intended to create a larger community of practice for participants.
During the first iteration of the course, participants were asked to complete a group assignment focused on challenges to practical implementation of palliative care in their work setting. Due to low levels of participation, and challenges for group members to work together as a result of distance and work schedules, the assignment was not used with future cohorts, instead assignment content was coved through case discussions and mentoring sessions. Further details of the development of our ECHO program, including key practices and modifications relevant to South Asia have been previously described. 7
Language
Participants are encouraged to ask questions in English or in Bengali depending on their comfort. There are Bengali and English versions of all core videos available for participants to review before the sessions, which contain identical content. There are Bengali speaking palliative care faculty present to answer questions, clarify points, and translate key ideas into Bengali during each session. In addition, a verbal Bengali language summary is provided at the end of each session.
Program Evaluation
We contacted all registered participants via email to complete short surveys at the time of registration and at the end of the 7 core sessions. These English-language surveys were developed from those previously developed for a pediatric palliative care Project ECHO in South Asia.7,10,12 The surveys explored participants’ experiences with palliative care training program, including participant knowledge, comfort, and attitudes about palliative care, with specific questions matching the content of the core course sessions. We asked participants about their experiences with the learning program, including program satisfaction, barriers, and factors which supported and/or enhanced their learning. We also asked participants about their use of the additional learning materials (session recordings and Supplemental materials) and to list any specific changes to their clinical practice. Demographic data including health professional education, medical specialty, professional role, years of experience, type of health facility, and the number of individuals needing palliative care who were seen on average each month were also collected.
We piloted this survey for the first cohort and subsequently modified the wording of comfort and attitudes questions based on this initial pilot to improve clarity and simplicity in English, and better reflect local palliative care concepts based on feedback from Bangladeshi leadership team members, who had detailed knowledge of the level of English proficiency of course participants. After cohort 1, we increased the number of Likert scale response options from 5 to 7 to provide more detailed response options. There were 21 participants who completed the end of course surveys during this pilot phase.
Statistical Analysis
Descriptive statistics were obtained using Microsoft Excel. Mann-Whitney U-tests were performed to evaluate differences between knowledge, comfort, and attitude scores that participants reported before and after the program. An a-priori statistical significance was set to p = 0.05.
Ethics Statement
The study was approved by the Children’s Hospital of Eastern Ontario Research Ethics Board (CHEO 17/201X).
Results
Program Characteristics
During the study time period (Sept 11, 2020 to Aug 13, 2021) 34 education sessions were conducted. This included 3 iterations of the 7 core didactic sessions and 13 optional mentoring sessions. The average number of individuals attending each session was 34 (SD 8.2, range 18-46).
Program Participants
During the study, 341 participants registered for Project ECHO during the study time frame. There were 250 health care professionals who attended at least one ECHO session, 89 of whom attended all 7 core sessions and received a certificate of course completion. Fifty-one participants completed the final follow up survey. Participant characteristics for those who completed the follow up survey are shown in Table 2. Participant characteristics for those who registered for the program were similar to those who completed the survey in terms of gender, education, profession, and practice characteristics.
Characteristics of participants for project ECHO on palliative care in Rohingya Refugee Response.

*Participants permitted to select more than one response.
Knowledge, Comfort and Attitudes Towards Palliative Care
At the course outset, participants reported the greatest lack of knowledge in end-of-life care (n = 14, 27%), breaking bad news (n = 9, 18%) managing pain (n = 13, 25%), and how to introduce palliative care (n = 14, 27%). These were similar to the areas in which participants self-reported their confidence in clinical skills as lacking, which included identifying patients needing palliative care (n = 16, 31%), treating pain (n = 13, 26%), identifying patients who are approaching end of life (n = 14, 27%), and serving as a palliative care expert in their workplace (n = 16, 31%). These statistics were determined by combining participant pre-ECHO responses of 1 strongly disagree, 2 disagree, 3 somewhat disagree, and 4 neutral. Further details are shown in Table 3.
Changes in Likert scale scores of participants’ knowledge, self-rated confidence, comfort, and attitudes about palliative care at baseline and the end of ECHO program.*
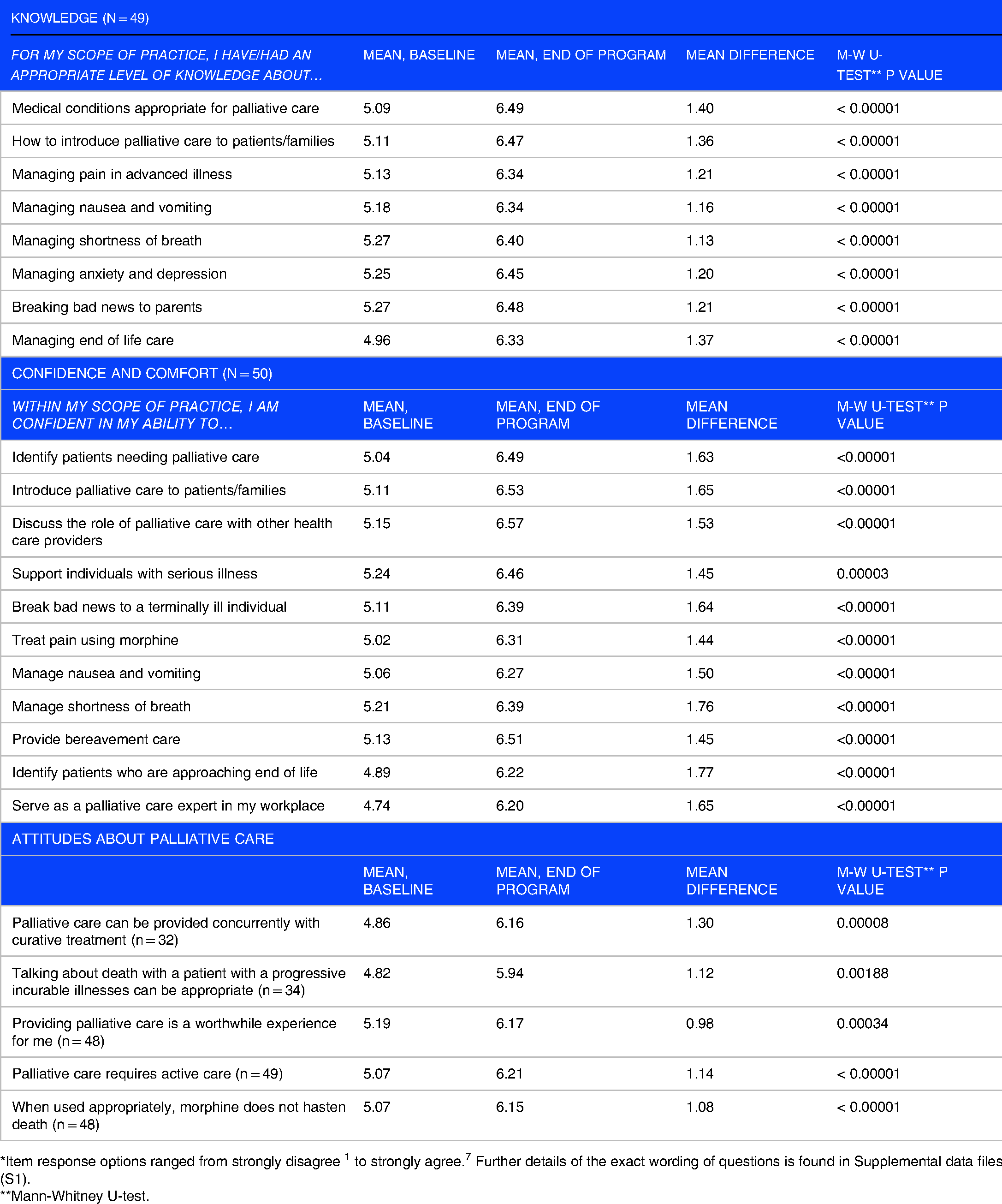
*Item response options ranged from strongly disagree 1 to strongly agree. 7 Further details of the exact wording of questions is found in Supplemental data files (S1).
**Mann-Whitney U-test.
Clinical Practice Changes
All participants agreed that since starting the ECHO program their knowledge of palliative care patient management had improved, with 98% reporting “better” or “a lot better” knowledge. When asked to list any specific changes in clinical practice as a result of ECHO, 5 participants (10%) noted improvements in their ability to provide appropriate wound care, 4 participants (8%) mentioned that they had started using a validated pain scale, 4 participants (8%) stated that they had started to respond more empathetically to patients’ mental health needs, and 4 participants (8%) felt better able to identify patients in need of palliative care. However, participants also noted that they needed additional clinical and/or formal teaching to increase their practice change. The cost and availability of palliative care medications were also identified as barriers for 22%, and 16% of participants respectively. During the study time frame, oral morphine was available from very few healthcare programs in the Cox’s Bazar region. Table 4 shows further details of participants’ learning experiences with the RRC ECHO.
Participants’ learning experience with the RRC ECHO program.

*Includes strongly agree, agree, or somewhat agree.
**Multiple responses permitted.
Program Acceptability and Satisfaction
The most frequent barriers to program participation included time (n = 23, 45%) and technical barriers (n = 30, 59%), with language noted by 9 participants (18%). Despite such challenges, participants reported a high level of course satisfaction, as indicated by their willingness to recommend the ECHO to colleagues (n = 50, 98%), and that they found the ECHO to be a valuable experience for them (n = 49, 96%).
Learning Resources
Almost all participants (>94%) were aware of the online learning resources, and most (>90%) chose to access them on their own time. Video recordings of program sessions were the most frequently accessed, with 57% watching the recordings to review or learn more and 51% watching recordings for sessions which they had missed. Participants also accessed the recordings to assist in their management of a specific patient (37%) or to teach colleagues (33%).
Discussion
We successfully developed, piloted and implemented a virtual palliative care training program for humanitarian healthcare providers in Bangladesh, using the Project ECHO model. Clinicians found this online learning to be a valuable and supportive learning experience that they would recommend to their colleagues. Participants reported improvements in their knowledge, comfort, and attitudes towards palliative care after participation in the program.
This is the first Project ECHO program exclusively focused on healthcare workers in humanitarian settings. We found the Project ECHO model to be successful in providing palliative care education to humanitarian healthcare providers in a remote region of Bangladesh, with more than 94% of participants agreeing that the program introduced them to best practices for providing care to individuals with serious illness. Most participants found the program valuable and would recommend it to their colleagues. Increased awareness and interest in the program was observed over the course of the study, with increased participant registration in subsequent cohorts, and sustained participation in ongoing mentoring sessions. Our findings provide evidence of the feasibility and value of delivering virtual palliative care education to address the continued gap in services for individuals with serious illnesses in humanitarian settings.3,13
Participants experienced significant benefits from the program, including improved knowledge and comfort in providing palliative care. Our findings mirror results from other ECHO programs in South Asia that have identified positive impacts on participants’ perceived knowledge and self-efficacy in palliative care. Our findings are particularly important since our study includes a relatively inexperienced group of clinicians (70% had less than 5 years of experience) where developing comfort in palliative care may be more challenging. These findings are particularly relevant in humanitarian settings, where there has been very limited palliative care clinical activity or training to date, and high staff turnover presents a further challenge. 1 Project ECHO may offer an innovative solution to address the gap in access to palliative care training in humanitarian settings, where a program structured around a short core program (7 modules) can provide basic training. This may then be further enhanced with ongoing monthly mentorship from faculty with knowledge of the local context. Further studies should explore the longer-term impacts of involvement in these types of educational programs.
Engaging community health workers in palliative care is critical to increasing access to services for seriously ill individuals who may not seek care from health facilities and often reside in rural or remote areas. 14 Our education program included a wide variety of health professions including nurses, physician assistants, as well as community health educators, whose highest level of formal education was secondary school. Further studies should explore how training programs can support the educational needs of a variety of health workers.
Developing training programs that address the learning needs of community-level health workers is especially important in humanitarian settings where there are frequently shortages of more highly skilled professionals.
A previous study of learners’ experiences with Project ECHO in South Asia identified language as a barrier to participation. 7 We modified the Project ECHO model to mitigate potential language barriers to participation. To address language challenges, we included Bengali speaking faculty, a Bengali summary at the end of the session, and Bengali pre-session videos. To allow opportunities for participants to review and study the course material at their own pace, we provided participants with presentations and other learning materials via social media to complement the live sessions. Despite these supports, 18% of participants in our study cited language as a barrier to active participation.
Complementing live ECHO sessions with social media and electronic resources also provides additional opportunities for learning, as described in our previous work on Project ECHO.7,10 We previously described how learners used these additional resources to teach their colleagues or students, share with colleagues outside of the ECHO, or as a guide when faced with a particular clinical situation. 10 Similarly, the participants in this study reported accessing materials to guide patient care and to teach or share with colleagues. These findings suggest that access to learning materials is particularly important and future studies should further explore the impact of these materials on participant learning.
Technical barriers are often identified as a significant barrier to e-learning in LMICs and were common in our study as well. 11 Despite nearly 60% reporting internet connectivity as a barrier to participation, participants remained highly satisfied with the program and found it to be a valuable experience. The availability of video recordings may have mitigated this issue. This experience mirrors findings from our pediatric palliative care ECHO program in India where participants also noted internet connectivity problems as a barrier. 7
Study Strengths
We describe an innovative virtual palliative care training program suitable for humanitarian settings, which includes experiences from a wide range of health professionals. The key features of this program include attention to the local healthcare situation and culture, suggesting that with these considerations the program may be transferable to other humanitarian settings.
Study Limitations
Although 250 participants joined the RRC ECHO Program, only 51 completed the full survey at the end of the program and the lower number of completed surveys could still lead to a selection bias in favor of those who found the ECHO to be most useful or participated more fully. Participants were also asked to self-report their knowledge, comfort, and attitudes towards palliative care, which may not accurately describe their abilities. Since surveys were in English, language barriers may also have affected survey responses and participation rates, despite our efforts after the pilot course to simplify the English used in the surveys and ensure that it was easily comprehensible to participants. We could not assess patient-level impacts. Future studies should seek to assess the impact of palliative care training on the clinical care experiences of individuals with serious illnesses and their families, including bereaved family members.
Conclusion
Virtual learning using Project ECHO is an innovative strategy to provide education in palliative care for healthcare providers in a humanitarian health response, which can improve access to palliative care services for individuals with serious health-related suffering.
Supplemental Material
sj-docx-1-mde-10.1177_23821205221096099 - Supplemental material for Using Virtual Learning to Develop Palliative Care Skills Among Humanitarian Health Workers in the Rohingya Refugee Response in Bangladesh
Supplemental material, sj-docx-1-mde-10.1177_23821205221096099 for Using Virtual Learning to Develop Palliative Care Skills Among Humanitarian Health Workers in the Rohingya Refugee Response in Bangladesh by Megan Doherty, Anisha Lynch-Godrei, Tasnim Azad, Fatima Ladha, Lailatul Ferdous, Rowsan Ara, Kathryn Richardson and Hunter Groninger in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to acknowledge the support of Two Worlds Cancer Collaboration Foundation, the Palliative Care in Humanitarian Aid Situations and Emergencies (PallCHASE), and the Fasiuddin Khan Research Foundation for their support with the implementation of this Project ECHO. The authors would like to express their sincere appreciation of the contributions of Saiduzzaman Bhuyian for his assistance with participant registration, attendance and communications.
Author Contributions
Conception and Design: MD ALG, HG, KR, TA, LF, RA
Provision of study materials or patients: MD, HG, TA, LF, RD, FL, RA
Collection and assembly of data: ALG, MD, HG
Data analysis and interpretation: ALG, MD, HG
Manuscript writing: all authors
Final approval of manuscript: all authors
Accountable for all aspects of the work: all authors
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Children's Hospital of Eastern Ontario Research Ethics Board (CHEO 17/201X).
Informed Consent
Study participants provided informed consent.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.