
Abstract
Background
This study was designed to investigate how patient-reported shared decision-making relates to other aspects of patient centredness and satisfaction.
Methods
Questionnaire study with patients. Consecutive patients in primary care responding post visit. Associations are presented as proportions, positive predictive values, with 95% confidence intervals.
Results
223 patient questionnaires were included. 62% (95% Confidence interval (CI): 55–69) of the patients indicated the highest possible rating of being involved in the decisions about their ongoing care (self-reported SDM). Self-reported SDM had a positive predictive value (PPV) of between 85% (CI: 77–90) and 95% (CI: 90–98) for five other patient-centred aspects and satisfaction.
Conclusion
The results suggest that shared decision making is the patient-centred aspect hardest to achieve and that a patient-centred process leading up to the decision-making increases the chance of the patient being involved in the decision-making.
Keywords
Introduction
There are many reasons why patient-centred care (PCC) is widely advocated: it urges the caregiver to consider the patients’ values and preferences and to encourage the patient to take an active role in decision-making. 1 Clinical health outcomes are improved using a PCC approach, with a reduced symptom burden, increased treatment precision, and the increase of the patient’s capacity to manage their illness and concerns.2–5 Patient safety and the effective use of common resources can also be improved by PCC through reduced prescriptions of clinically unmotivated medications and unnecessary clinical examinations as well as reduced need for referrals to other clinics.5–6
Two key aspects reoccur in the variety of patient-centred methodologies: the patient’s narrative and collaboration. 7 The narrative aspect refers to the notion that the patient is given an opportunity to share information, not only about biomedical signs and symptoms, but on broader personal aspects like current situation, preferences, ideas, concerns, and expectations about the health issue in focus and current/future care.7–9 The other key component, the collaboration between patient and doctor reflects the idea of a partnership between patient and caregiver, where information-sharing and decision-making is a process engaging both parties as active contributors.7,10 In this paper we have examined a selection of patient-centred aspects that are core items of the consultation model taught to medical students and their supervisors at Karolinska Institutet, Stockholm, Sweden. The model is similar to consultation models used in health care and education elsewhere in Sweden, Scandinavia, the Netherlands, Great Britain, and Canada.11–16 As the initial parts of the consultation have been thoroughly reviewed in previous research, and implementation of patient-centred strategies thereof has come farther,17–18 we have paid special attention to patients’ involvement in the decision-making, shared decision-making (SDM), that often takes place at the less studied end of the consultation. An additional reason to focus on SDM is that there are indications that SDM is not sufficiently practiced in Sweden, and there is sparse indication of its’ implementation moving in the right direction. 19 The conception of SDM varies greatly, with incompatible viewpoints and approaches, some models suggesting broader demands on the process and others being satisfied when patients’ preferences are discussed and accepted. 20
The aim of this study is to explore how SDM relates to other aspects of patient-centredness, individually and combined, and to patient satisfaction in patient-doctor primary care consultations. We did this by investigating the following research questions: (a) how does self-reported SDM correlate to each studied aspect of patient centredness and different combinations thereof? (b) how does self-reported SDM and each studied aspect of patient centredness, including different combinations of aspects, correlate with satisfaction? and (c) can SDM be achieved independently without the other patient-centred aspects?
Method
Data has been collected through a patient questionnaire regarding six patient-centred aspects and patient satisfaction. The study had ethical approval from the Stockholm Ethical Review Board (Dnr 2015/2193–31/5).
Participants
The survey was distributed to patients in connection with their healthcare meeting in a Primary Care Centre during two weeks in 2016. The practice is situated in a northern suburb of Stockholm and serves a population of 17,500 patients. The majority is born in Sweden, whereas elderly and patients born abroad are over-represented compared to the Swedish population in general. The Primary Care Centre also has research and medical student-activities. All consecutive patients aged 18 or above who attended a doctor, nurse, or assistant nurse in the practice during the research period were asked to participate in the study by independently filling out a questionnaire.
Of the paired questionnaires 36 (of 160) were excluded because they had been inadequately handled: the patient responses had identical answers both in wording and handwriting, which indicated that they had been filled out with the assistance of the healthcare provider, thereby potentially influencing the answers. Only a smaller number of questionnaires from patients who had met other professionals than doctors remained after this and were therefore excluded.
The remaining patients had either just met a doctor or filled out a questionnaire provided by researchers outside the consultation room. This means that we do not know in the latter cases which healthcare provider they had consulted. The inclusion of the latter was motivated partly because the information from this group was considered important, since they might have had a more stressed consultation, explaining why they were not provided with the questionnaire, and partly because most of them had seen a doctor. Contrary to instruction, seven children (and/or parents to children) completed one questionnaire each. These questionnaires have been included. Of the about 20 doctors in service during the research period, 16 (11 female and 5 male) participated in a base-line survey. Their self-rated experience of working in a patient-centred manner was large (nine doctors), limited (five doctors) or non-existing (two doctors). Detailed background factors of the participating patients have been presented elsewhere. 11
The questionnaire
Box 1. The seven aspects covered in the questionnaire
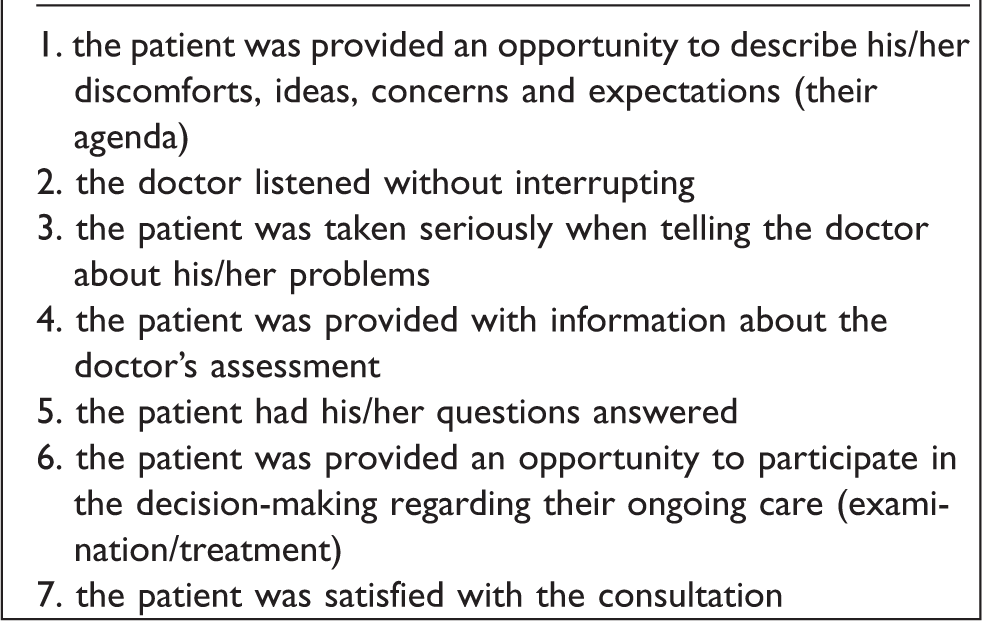
The seven aspects had four fixed response options given on a Likert scale: “I agree completely”, “I agree to a large extent”, “I disagree to a large extent”, or “I disagree completely”. In addition, the questionnaire had two initial questions on the patient’s main reasons for attending the clinic, where the patient was asked to provide a free-text description. Towards the end of the questionnaire, there was an option to provide a free-text commentary as well as four background questions including age, gender, country of birth (Sweden, other European, or outside of Europe), and education (primary school, secondary school/gymnasium, professional school, or university). The questionnaire was piloted among 95 patients during two days, leading to minor alterations. The responses of the pilot are not included in the present analysis.
Collection of data
At the end of the consultation, the doctors informed the patients about the study and asked if they wanted to participate. If they consented to participate, they were asked to answer the questionnaire in the waiting room. All approached patients were informed about the purpose and anonymity of the survey. By verbally consenting to participate and filling out the questionnaire the patient was included in the study, whereas those who declined participation opted out either by saying so or by not filling out the questionnaire. A new questionnaire was provided to the patient by a researcher in the waiting room if the doctor had failed to do so. All questionnaires filled out by the patients were collected by a researcher.
Data registration and analysis
The data on the seven patient-centred aspects and a condensed version on the free-text responses were registered into the statistical program Epi-info. The full free-text responses were registered in a Windows Excel document. The responses with four response options (see Box 1) were dichotomised into two groups: “I agree completely” and “I do not agree completely”, the latter covering the remaining three response options. 21 In the statistical analysis, we calculated proportions with 95% confidence interval, diagnostic accuracy measures, (Clopper-Pearson Exact) using medcalc statistical software, (https://www.medcalc.org/calc/odds_ratio.php, accessed august 27 2019) and epitools, (http://epitools.ausvet.com.au/ciproportion, accessed February 3 2020).
We analysed (a) each patient-centred aspect 1–5 and their associations to patient participation in decision-making, (b) all combinations of aspect 1–5 and their associations to patient participation in decision-making, (c) each patient-centred aspect 1–6 and their associations to patient satisfaction, and (d) all combinations of the patient-centred aspects and satisfaction.
Results
There were 223 patient questionnaires included. A few patients declined participation and among them language difficulties, anger with the visit, and severe illness was mentioned as reasons. The background variables of the patients are presented elsewhere. 11 The patients stated complete participation in the decision-making in 62% (CI: 55–69) and complete satisfaction in 78% (CI: 72–83) of the consultations. 11 To distinguish between aspect 6 of the questionnaire and shared decision-making in general, we use the term “self-reported SDM” when we refer to aspect 6 of the questionnaire.
Associations between shared decision making and five other patient-centred aspects
When aspect 3 (patient taken seriously) was given the highest possible rating (“I agree completely”), the positive predictive value (PPV) for highest possible rating of aspect 6 (self-reported SDM) was 70% (CI: 63–77). For aspect 5 (patient’s questions answered) the highest possible rating had a PPV for self-reported SDM of 78% (CI: 70–84). The PPV for self-reported SDM of the other patient-centred aspects varied in between these proportions (Figure 1). A combination of highest possible ratings of all five patient-centred aspects had a PPV of 88% (CI: 80–94) for the highest possible rating of self-reported SDM. Lowest frequency of highest possible rating of self-reported SDM had the patients who experienced that they were not completely listened to without interruption [PPV 23% (CI: 11–39)] and the patients who experienced that they did not get information to a full extent [PPV 27% (CI: 15–41)] (Figure 1).
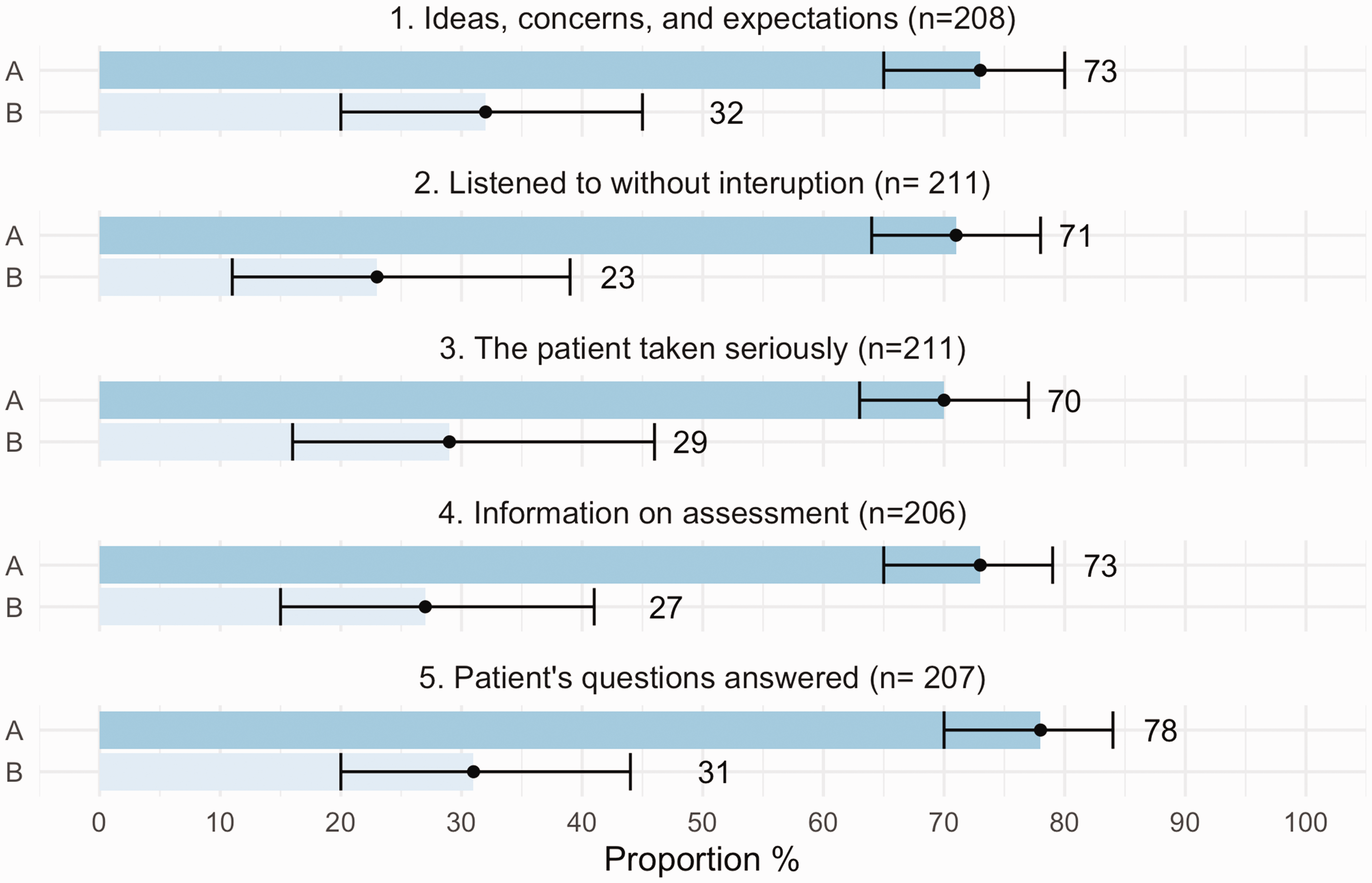
Patient-centred aspects and their PPV for highest possible rating of shared decision- making (self-reported SDM).
Patient ratings of shared decision-making in general practice consultations. Positive predictive value and 95% confidence interval for highest possible rating of shared decision-making for patients with highest possible rating (group A) and less than highest possible rating (group B) of five patient-centred aspects. The internal number of drop-out varied between 12–17.
Turning this around: highest possible rating of self-reported SDM had a PPV ranging from 85–93%, for the other five patient-centred aspects to be given the highest possible rating. Among the aspects, the highest PPV was for aspect 2, being listened to without interruption [93%, (CI: 87–97)]; see Figure 2.
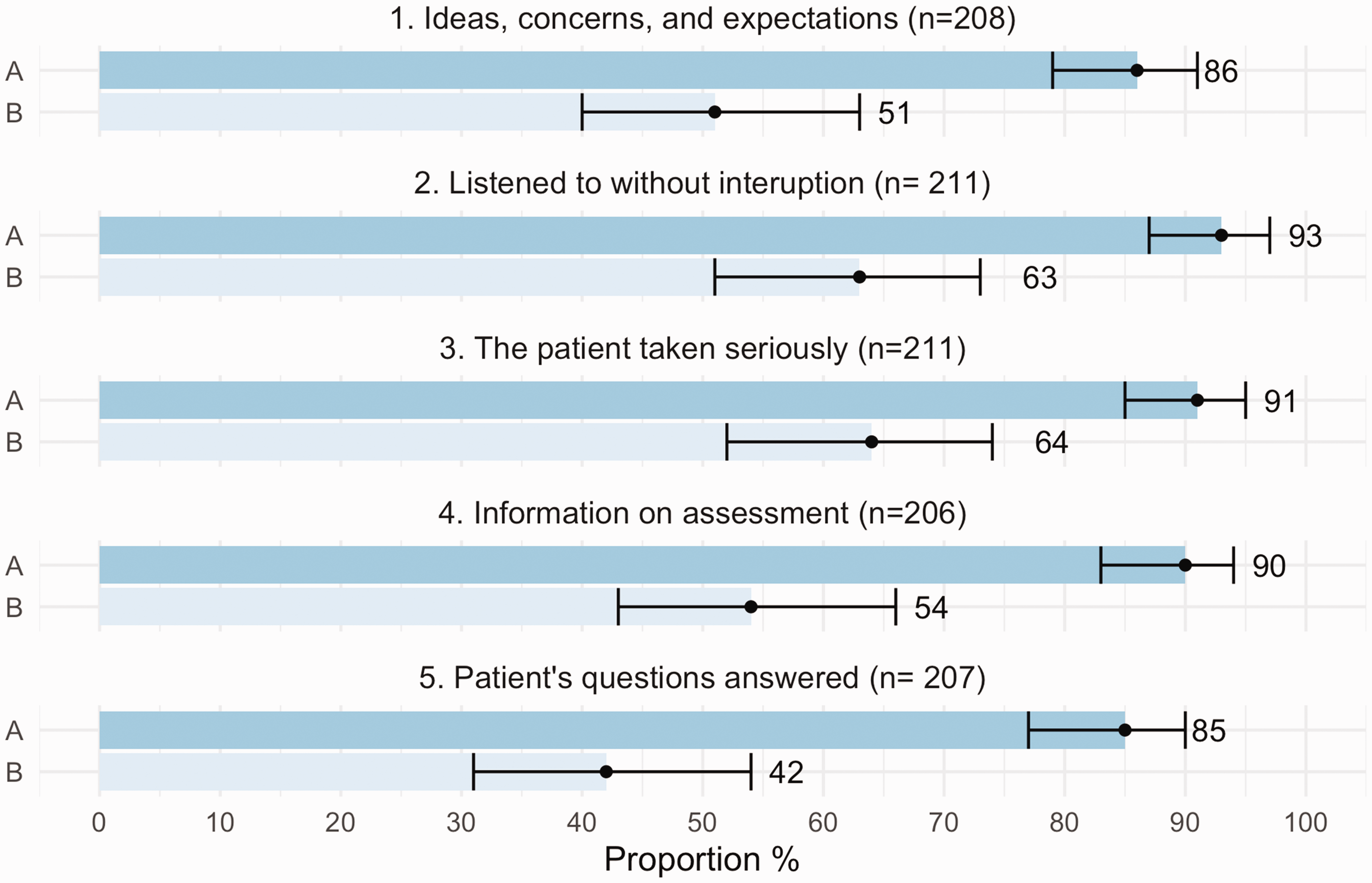
Self-reported shared decision-making and it’s PPV for highest possible rating of five other patient-centred aspects.
Patient ratings of five patient-centred aspects in general practice consultations. Positive predictive value and 95% confidence interval for highest possible rating of each aspect for patients with highest possible rating (group A) and less than highest possible rating (group B) of shared decision-making. The internal number of drop-out varied between 12–17.
Associations between patient-centred aspects and patient satisfaction
When aspect 1 (ideas, concerns, and expectations) was given the highest possible rating, the positive predictive value (PPV) for being completely satisfied was 87% (CI: 81–92). For aspect 6 (self-reported SDM) the highest possible rating had a PPV for patients being completely satisfied of 95% (CI: 90–98). The PPV for satisfaction of the other aspects varied in between these proportions (Figure 3). For every added aspect that was given the highest possible rating by the patients, satisfaction increased so that when all six patient-centred aspects were given the highest possible rating, the PPV for complete satisfaction was 100% (CI: 96–100). Among the patients, 45% (n = 89) stated the highest rating on all the patient-centred aspects and on satisfaction. For the rest of the patients, those who stated that they did not agree completely on at least one of the aspects, complete satisfaction ranged from 29% (CI:16–45) to 52% (CI: 38–65) depending on which aspect was evaluated (Figure 3).
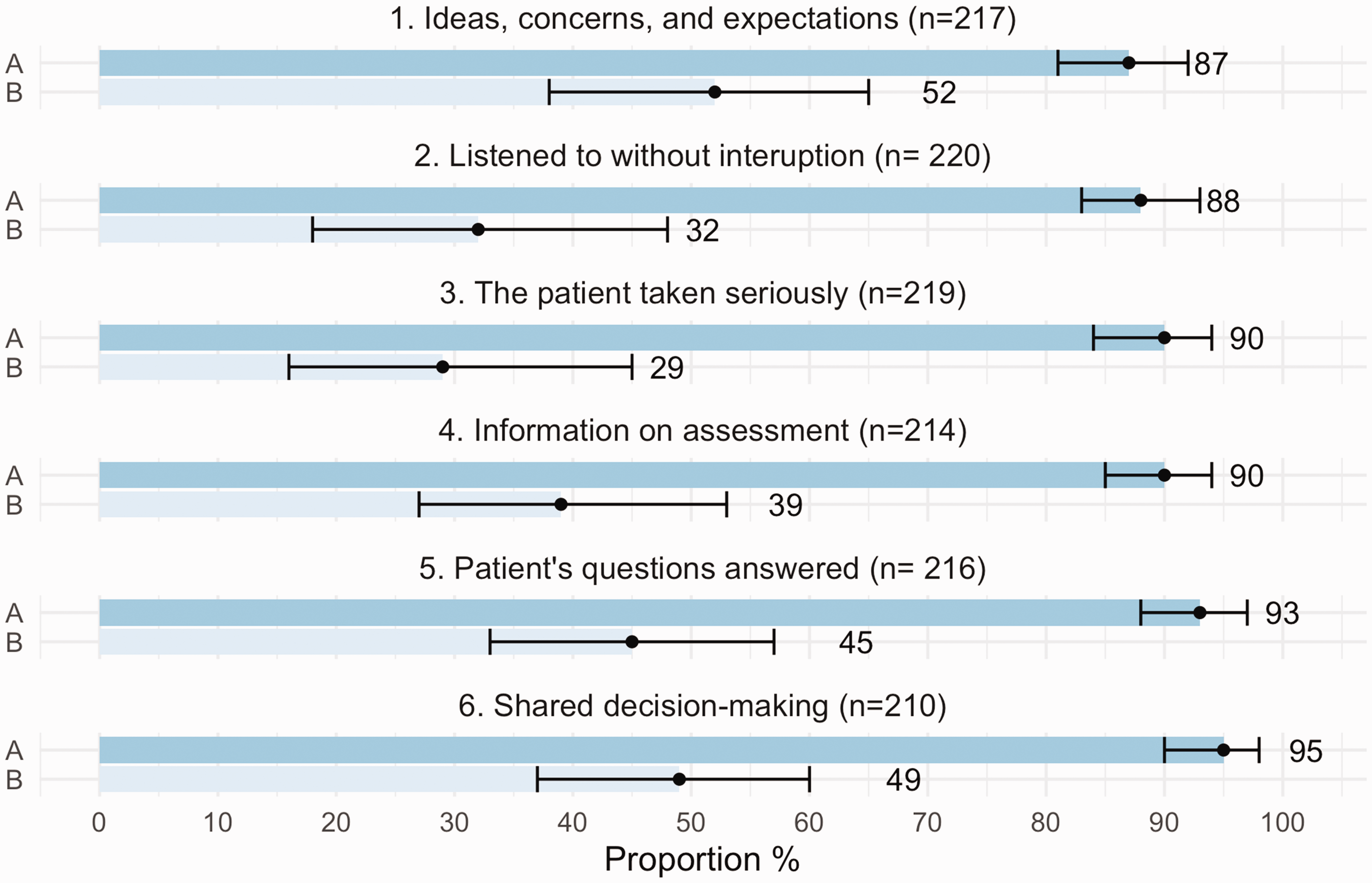
Patient-centred aspects and their PPV for highest possible rating of satisfaction.
Patient ratings of satisfaction in general practice consultations. Positive predictive value and 95% confidence interval for highest possible rating of satisfaction for patients with highest possible rating (group A) and less than highest possible rating (group B) of six patient-centred aspects. The internal number of drop-out varied between 3–13.
From the opposite direction, the highest possible rating of satisfaction had a PPV between 76% (CI: 69–82) and 93% (CI: 88–96) for the individual patient-centred aspect being rated highest possible, with the lowest PPV for self-reported SDM and the highest for being provided with information.
Discussion
The present results indicate a strong association between self-reported shared decision-making (SDM), other aspects of patient-centredness and patient satisfaction. For each added patient-centred aspect, satisfaction increased so that with all patient-centred aspects fulfilled to the highest degree, all patients experienced complete satisfaction with their consultation. Self -reported SDM had the highest positive predictive value (PPV) for patients’ satisfaction with their consultation. Complete achievement of all the first five patient-centred aspects strongly associated with the highest possible level of self-reported SDM. At the same time, SDM was the patient-centred aspect least frequently given the highest response in the patient-doctor consultations, suggesting that it is the hardest to achieve and one that requires that the other aspects are in place.
Obstacles, and means, to shared decision-making
The results of this study show that only 62% of the patients in this primary care context find themselves fully involved in the decisions about their own care – i.e., they agreed completely with the statement that they were provided an opportunity to participate in the decision-making regarding their ongoing care. We suggest that this reflects a lack of patient involvement. This interpretation is similar to what is previously argued in both national and international recent reports and papers.1,5,19,22,23 Lack of patient involvement has been problematised for several decades10,17 and the arguments have piled up over time: not only does it suggest that health care fails to implement the means to secure that the patient’s autonomy is respected in the healthcare meeting, but patient involvement in decision-making has also been suggested to promote health outcomes such as fewer function limitations, symptom alleviation, and improved health markers such as blood sugar control.24–25 One can expect a corresponding loss if this aspect is not sufficiently attended.
The findings in this study show an increased frequency of satisfaction for patients who experienced being involved in the decision-making. This indicates that the opportunity to take part in the decisions is welcomed by the patients in this primary care context.
Doctors have described their own difficulties in this area: if they have not solicited the patient’s agenda (ideas, concerns, and expectations), or given enough information, they found that SDM was harder to achieve. 26 These experiences are supported by the results of the present study: when physicians failed to fulfil one, or more than one, of the first five patient-centred aspects of the consultation, the patients’ experiences of being fully invited to shared decision-making decreased.
Our experience is that the concept of shared decision-making is sometimes misconceived as an independent part of the consultation, sometimes with the exception of information as the only prerequisite. By regarding shared decision making as informed choice, some of the doctors’ concerns would be justified and there would be an evident risk of patients feeling abandoned. 27 In this material, the patients that perceived a high level of patient-centred physician communication leading up to the decision-making (aspect 1–5) also perceived a higher level of shared decision-making. This might reflect an overall more patient-centred communication style of certain physicians or that the assessment concerns a less complex medical issue. 11 It might also reflect that other patient-centred aspects than sharing information, such as listening without interrupting, soliciting the patient’s agenda and answering the patient’s questions, facilitate the decision-making process and increase the chance of patient participation in the actual decisions. Regarding the decision-making process in this way suggests that shared decision-making is both dependent of previous steps of a patient-centred consultation and independent in such a way that the doctor needs to actively invite the patient into the actual decisions.
Why care about patient satisfaction if we care about patient-centredness?
Whereas satisfied patients are more adherent to their physician’s recommendations, 28 dissatisfaction is associated with less symptom reduction, missed follow ups, and patients being twice as likely to reconsult compared to satisfied patients.29–30 While dissatisfaction indicates that there is something that has failed in the delivery of health care and might threaten patients’ trust in health care, 31 satisfaction is no guarantee for high quality care or patient safety. Patient satisfaction ratings can mask deficiencies in quality.32–33 In a paper from 2012, Fenton and colleagues presented evidence suggesting that a higher grade of patient satisfaction was associated with not only increased inpatient utilisation, health care expenditure, and prescription of drugs but also a greater mortality risk. 28 The challenge is how patient satisfaction data should be taken into consideration. A suggestion is that dissatisfaction can be of interest as an indicator that things could be better from the patient’s perspective. If there are indications of patient dissatisfaction with health care this should be further investigated, for instance: does health care not deliver what they should in terms of measurements, such as investigations or treatments? Does health care lack in their way of communicating with the patients? Or do patients want something that health care should not or decided not to provide?
The tension between shared decision-making and patient satisfaction
This study has focused on SDM in patient-doctor consultations. Now, SDM might be conceived as questionable to start with. We strongly emphasize that SDM should not be thought of as giving the patient whatever they desire. The findings, that the individual patient-centred aspects have a high positive predictive value for satisfaction, are supported by multiple previous studies.34–36 Self-reported SDM as well as the combination of the aspects had a particularly strong association with complete satisfaction. A high level of patient satisfaction is desired by many, but we want patients to be satisfied for the right reasons. Although giving the patients what they want without much medical consideration or guidance could make most patients feel both content and involved, it would create adverse effects such as risking patient safety and increase unnecessary, costly, and possibly harmful investigations and treatments. It also contributes to the alarming situation that we see with the overuse of antibiotic treatment. 37 We suggest that SDM is not about always taking what the patient expresses as their desire at face value. Sometimes the superficial tension between what the patient wants and what is in their interest can be resolved by picking up on the superordinate wishes of the patient. If, for instance, the patient suspects that they suffer from osteoarthritis and suggests a magnetic resonance imaging (MRI) to see if that is the case, the expectation or wish would be to have an MRI, but the superordinate wish would be to know if they have osteoarthritis and to have a correct diagnosis. This notion can help the doctor in the consultation, by clarifying the mutual (and tension-free) agenda: helping the patient to get the correct diagnosis and addressing if osteoarthritis is it. By including this in the summary: “you suspect that you have osteoarthritis and wonder if MRI is the best way to check”, the doctor will have created a good opportunity for a mutual agreement in the end of the consultation: “After investigating your knee, I too believe that you have osteoarthritis. My suggestion is that you should have an x-ray, being a fast investigation that will answer our question.”
Most reliable indication: Pedagogical application
If a supervisor to a near self-sufficient medical student or junior doctor has not participated in a meeting between a patient and the student/doctor and has an opportunity to ask the patient only one question, which question would be most informative for the supervisor?
Satisfaction? If the patient is satisfied, the positive predictive value (PPV) for the other aspects was between 76% (self-reported SDM) and 93% (patient being taken seriously). With this answer the supervisor can conclude that the patient probably experienced being taken seriously by the medical student, but the supervisor will not know if the patient was sufficiently involved in the decision-making. One of the first five patient-centred aspects? If the patient gives the highest rating of one of the first five aspects there is a good chance that the patient is also satisfied with the visit (PPV between 87 and 93%, depending on the aspect) but the supervisor will not know if the patient was sufficiently involved in the decision-making (70-78%). SDM? If the patient gives the highest rating on being involved in decision-making, PPV for the five other aspects and satisfaction vary between 85–95%. When SDM is not given the highest rating, the supervisor has a good reason to investigate what happened in the consultation.
Out of the questions that we can ask the patient, rating SDM has the highest PPV for patient-centred communication and satisfaction in the studied context. It is the most reliable indication for the other aspects in the cluster of aspects studied.
Strengths and limitations of the study
A strength of the present study is that it illuminates the relation between the earlier stages of patient-centred consultation and the final stage, shared decision-making. It also throws light on the relation between and combinations of different aspects of patient-centred consultation and patient satisfaction.
The main limitation of the study is a potential response- and sample bias: content patients ticking the “I agree completely”-box frequently might provide the same answer again without much consideration of the actual question at hand, which might have resulted in an overestimation of the association between satisfaction and the patient centredness aspects.
It is difficult to distinguish Shared decision-making completely from other aspects of patient-centredness, since shared decision-making can be regarded as the process of communication leading up to the decisions as well as the sharing of the actual decision-making. To avoid the risk of circular reasoning we have used two terms: “Shared decision-making” when discussed in a general sense and “self-reported SDM” when we refer to the narrowly defined studied aspect of the questionnaire.
Conclusion
The results of this study suggest that shared decision making is the patient-centred aspect hardest to achieve and that a patient-centred process leading up to the decision-making increases the chance of the patient actually being involved in the decision-making. The results also suggest that a high patient-rating of shared decision-making could be regarded as a reliable indication that the doctor also had a high level of other patient-centred behaviour and that the patient was satisfied with the consultation.
Supplemental Material
sj-pdf-1-cet-10.1177_14777509211015897 - Supplemental material for Shared decision-making in patient–doctor consultations – How does it relate to other patient-centred aspects and satisfaction?
Supplemental material, sj-pdf-1-cet-10.1177_14777509211015897 for Shared decision-making in patient–doctor consultations – How does it relate to other patient-centred aspects and satisfaction? by Helene Bodegård, Gert Helgesson, Daniel Olsson, Niklas Juth and Niels Lynøe in Clinical Ethics
Supplemental Material
sj-pdf-2-cet-10.1177_14777509211015897 - Supplemental material for Shared decision-making in patient–doctor consultations – How does it relate to other patient-centred aspects and satisfaction?
Supplemental material, sj-pdf-2-cet-10.1177_14777509211015897 for Shared decision-making in patient–doctor consultations – How does it relate to other patient-centred aspects and satisfaction? by Helene Bodegård, Gert Helgesson, Daniel Olsson, Niklas Juth and Niels Lynøe in Clinical Ethics
Supplemental Material
sj-pdf-3-cet-10.1177_14777509211015897 - Supplemental material for Shared decision-making in patient–doctor consultations – How does it relate to other patient-centred aspects and satisfaction?
Supplemental material, sj-pdf-3-cet-10.1177_14777509211015897 for Shared decision-making in patient–doctor consultations – How does it relate to other patient-centred aspects and satisfaction? by Helene Bodegård, Gert Helgesson, Daniel Olsson, Niklas Juth and Niels Lynøe in Clinical Ethics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received - financial support for the research, authorship, and/or publication of this article. This work was supported by the Swedish Research Council and the Swedish Research Council for Health, Working Life and Welfare 2014 - 2024. The funding bodies had no influence over any part of the study.
Supplemental Material
Supplemental material can be found by contacting the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.