
Abstract
It could hardly be denied that healthcare should be patient-centred. However, some of the practices commonly described as patient-centred care may have ethically problematic consequences. This article identifies and discusses twelve ethical conflicts that may arise in the application of (some variants of) person-centred care. The conflicts concern e.g. privacy, autonomous decision-making, safeguarding medical quality, and maintaining professional egalitarianism as well as equality in care. Awareness of these potential conflicts can be helpful in finding the best way to ensure that healthcare has its focus on the needs and interests of the patients. Patient-centred care may have to take different forms, depending of the nature of the disease, the patient’s life situation, and the economic, organizational and technological resources available to the healthcare unit.
Keywords
Background
Who can be against patient-centred (or person-centred) care (PCC)?
1
Presumably, there are not many who subscribe to such a position. Indeed it would seem difficult to come up with an argument for why patients should not be at the centre of deliberations on, and activities of, healthcare provision. One group of researchers found that the staff in the healthcare unit they studied “… considered PCC to be a self-evident and important facet of care. In fact, our major challenge was not in persuading them to practice PCC, but rather in convincing them that they were not practicing PCC—at least not consistently or systematically.”
2
The term “patient-centred” seems to have been introduced in the late 1960s by Michael Balint and co-workers, who attributed the phrase “patient-centred medicine” to a Professor Millar at the University of Aberdeen. 3 (This was probably W.M. Millar who was professor of mental health at that university.) According to these authors, the patient-centred approach stands in contrast to the traditional illness-centred one. The patient-centred physician should think “in terms of personality problems, conflicts and disturbed human relationships, as well as physical illness”. Doing so “demands from the doctor a different relationship to the patient” than the one required in traditional, illness-centred, medicine. 4 In the mid-1990s, the term “patient-centred” became increasingly common. It still carried a meaning close to that propounded by Balint and his co-workers, but often with an increased emphasis on patient participation in decision-making, in stark contrast to the traditional paternalistic approach to medical decision-making. Advocates of patient-centred care wanted to enable patients to be autonomous agents and active participants in the planning and execution of their own treatment and care. More recently, the term “patient-centred care” has been used to denote a way to organize healthcare, such that “institutional resources and personnel are organized around patients rather than around specialized departments” (the MeSH definition). 5
There is still no single, generally accepted definition or description of what patient-centred care entails. It has often been pointed out that the term is rather vague; for instance Mead and Bower noted that “there is little consensus as to its meaning” 6 and Tanenbaum wrote that the meaning of patient-centred care is controversial and several models have been proposed. 7 In spite of this diversity, however, there are some recurring themes, or conceptual components, in the definitions and explications of the concept. 8 For our investigation of potential clashes with other ethical considerations, we have focused on three conceptual components that appear to be at the heart of such conflicts. They are all frequently referred to in the literature, and often conceived as essential constituents of patient-centred care. Although there is some overlap between them, they are distinct enough to be useful means to distinguish between different aspects of patient-centred care.
The first of these themes is holism. As observed by Olsson et al, the concept of person-centred care “has its roots within a holistic paradigm, which suggests that people need to be seen in their bio-psychosocial enti[re]ty.” 9 Holism can be interpreted in many different ways, and it is often far from clear exactly in what sense the term is used. 10 However, in all uses that we have seen of the term in a healthcare context, it requires that the caregiver’s attention goes beyond the patient’s medical condition, as conventionally defined, and includes the patient’s emotional and social situation in general. In much of the literature on patient-centred care, the patient’s narrative is taken to be the major means for obtaining the broad information about the patient that this approach requires.
The second theme is a personal relationship between caregiver and patient, a relationship that goes beyond the more restricted professional relationship that has traditionally been the norm. These relationships are often based on the patient’s narrative, as it provides the caregivers with the type of detailed and often personal information which allows them to get to know the patient.
The third theme is shared decision-making. This means that the physician and the patient jointly engage in making the treatment decisions. It is often interpreted as a decision-making model intermediate between old-fashioned medical paternalism and the modern model of the patient’s informed choice. (For a discussion on the relationship between PCC and shared decision making, see the section Conflicts relating to shared decision-making .)
In the following three sections, we will investigate the potential conflicts that could arise between, one the one hand, each of these components of patient-centred care, and on the other hand, various ethical principles and objectives that are prevalent in healthcare. It is important to note that these are potential conflicts. Whether or not they actually materialize will depend on factors such as the more precise version of person-centred care that is applied, the patient’s medical condition and situation in general, and the economic, organizational and technological resources available to the caregiver.
As will be noticed in what follows, several of the potential conflicts that we have identified have already been discussed in the literature, often in connection with proposals aiming at the resolution or mitigation of the conflict in question. What has been missing, however, is a comprehensive account of how patient-centred care is situated in the complex, and far from conflict-free, landscape of ethical principles and requirements in healthcare. This article is, as far as we know, the first attempt at such an account. We believe that such a general overview is needed as one of the starting-points for further developments of principles, models, and procedures of person-centred care that are suitable to be integrated into various forms of healthcare.
Conflicts relating to holism
As already mentioned, person-centred care is commonly conceived as involving a “biopsychosocial perspective” on the patient.
11
To achieve such a holistic understanding, caregivers are said to need “an integrated understanding of the patients’ world—that is, their whole person, emotional needs, and life issues”.
12
The patient narrative tends to generate the type of information required for such a broad perspective. “The patient narrative is the sick person's personal account of his/her illness, symptoms, and their impact on her/his life. It captures the person's suffering in an everyday context, in contrast to medical narratives that reflect the process of diagnosing and treating the disease. In our experience, the patient narrative constitutes the starting point for PCC and lays the ground for a partnership in care.”
13
We have identified six potential ethical conflicts involving the holism of patient-centred care. The first two originate in the extended solicitation of information about the patient through the patient narrative. They are followed by two potential conflicts that relate to the quality of care and two that concern equality and equal treatment.
Conflict 1: Holism versus privacy in the patient-physician and patient-nurse relationships
Asking a patient for a narrative of her life is likely to encourage her to reveal privacy sensitive information, e.g. sexual orientation, extra-marital affairs, economic distress, psychological problems, conflicts in the family, and worries about problems affecting family members. 15 It is often difficult for patients to know to what extent and for what purpose healthcare personnel need such information. When encouraged to talk about matters that she considers sensitive and/or embarrassing, a patient may mistakenly assume that the topic is medically relevant, and choose to share information although she would have preferred not to. For instance, a patient who prefers not to talk about her father can easily presume that the topic was brought up for some medical reason such as heredity, even if that is not the case.
Arguably, patients have an obligation to share sensitive information that their caregivers need to do their job. But, patients also have a right not to share information that is not needed for medical or caregiving purposes. Placing them in a situation of “narrative-sharing”, where they are expected to divulge sensitive information but, at the same time, are ill-placed to assess which information might be relevant for medical and caregiving purposes, increases the risk of over-sharing. Such a practice can in some cases be stressful and possibly amount to unethical privacy intrusions. For some patients the process of providing an extensive narrative can develop into a distressing experience that may be detrimental to the attainment of therapeutic goals. 16 We therefore have a potential ethical conflict between on the one hand the usefulness of a patient narrative for better understanding the patient’s life situation (including in some cases a positive therapeutic effect of the narrative process itself), and on the other hand the risk that the solicitation of narratives will infringe on the patient’s privacy.
Conflict 2: Holism versus IT (information technology) security
To the extent that physicians and nurses engaging in patient-centred care make use of sensitive personal information from the patient’s narrative, they will need to include much of that information in medical records. 17 This is needed both to support one’s memory (and avoid confusing two people’s life stories), and to make the information available to colleagues. However, as noted by Munthe et al, “the more information that is assembled in any sort of system (everything from the mind of a person or a group, over traditional archives to digital databases), the higher the risk that some sensitive information will leak.” 15 From the viewpoint of IT security it is always an advantage to include as little privacy sensitive information as possible in electronic databases. There is therefore a potential ethical conflict between IT security and the documentation of the patient’s narrative, which is a central component of many variants of patient-centred care.
Conflict 3: Holism versus avoiding medicalization
The holism of person-centred care implies that health care personnel should be willing to engage in the full range of difficulties that patients encounter, not just those that can be classified as biomedical. 18 If seriously pursued, this could induce physicians and nurses to feel responsible for dealing also with non-medical aspects of the patient’s problems. 19 They might end up trying to help patients with advice concerning personal relationships, family conflicts, economic difficulties, workplace problems, and so on. Such a practice can result in the medicalization of problems that have traditionally been considered to be non-medical. We therefore have a potential ethical conflict between, on the one hand, the person-centred ideal of doctors and nurses engaging with “the whole person”, and on the other hand, the ethical requirement to avoid the medicalization of non-medical problems.
An interesting comparison can be drawn with the practice of social prescription, which has occasionally been promoted as part of patient-centred care, 20 but is more commonly applied independently of PCC. Social prescriptions range from activities that are closely aligned with evidence-based medical recommendations, such as physical exercise and cooking courses focusing on healthy food, to activities that are presumed to promote the patient’s well-being in general rather than medical terms, such as debt advice and art courses. Unfortunately, the evidence of positive clinical effects of social prescription is extremely weak, 21 and there is also a lack of clear descriptions of its aims and the criteria by which it should be evaluated. 22 It is not unreasonable to ask whether some forms of social prescription may involve the medicalization of non-medical problems. However, in most programs of social prescription, the involvement of medical professionals is limited to referral, a limitation that is usually not recommended in the literature on patient-centred care.
The term “healthism” was introduced to describe an approach to life that concentrates on health at the expense of other aspects of wellbeing and a good life. 23 Critics have warned against an overzealous focus on health as “a kind of medicalisation, whereby domains of life previously not considered relevant to health, or as appropriately falling within the structures of healthcare, are newly seen through a medical lens”. 24 Interventions that go beyond the traditional medical realm may well be justified, but their potential value should always be weighed against the risks of contributing ethical and clinical problems that tend to follow with extensions of medicine to previously non-medical areas of human life.
Conflict 4: Holism versus avoiding “reverse quackery”
Engagement by healthcare personnel in patients’ non-medical problems can also lead to an overextension of professional scope that we may call “reverse quackery”. Quackery usually means that people who lack the necessary knowledge, skills, and qualifications for offering healthcare services offer such services of inferior quality. The reverse situation can arise when physicians or nurses give advice on non-medical problems. We therefore have a potential ethical conflict between, on the one hand, the requirement to see and help “the whole person” and on the other hand, the requirement that healthcare personnel should not transgress their areas of professional competence.
One possible area of such “reverse quackery” is the involvement of healthcare personnel in religious counselling or services. Such activities have been promoted by some adherents of person-centred care. For instance, Pfeifer and Cox advocate “a renewed recognition that good clinical care depends also on a wider understanding of the spiritual dimensions of health”. 25 In the same vein, Mezzich maintains that person-centred care “is dedicated to the promotion of health as a state of physical, mental, sociocultural, and spiritual well-being”. 26 Needless to say, patients asking for access to religious or spiritual services should be helped to get what they ask for, but the actual provision of such services is not part of what physicians and other health-care personnel should integrate into healthcare provision or perform themselves as part of their professional activities. There are at least three reasons for this: they have (usually) not been educated for doing so, patients wishing such services tend to have denominational or other preferences that may not coincide with the caregiver’s own approach, and patients not wanting the services offered may regard the offer as an undesired attempt at proselytizing.
Conflict 5: Holism versus professional non-judgmentalism
It is part of the professional ethics of healthcare personnel to be non-judgmental with respect to the patient’s moral character and the moral status of her actions, both in general and as they relate to the causes and the background of her disease. In particular, considerations of whether a patient is to blame for her disease or injury should not affect the treatment she receives. In some situations this non-judgmental approach is difficult to fully achieve. 27 Clearly it is important that healthcare personnel encourage patients to “take charge” of their lives, for instance by supporting decisions to adopt a more healthy life-style. However, it is not always easy to do so while at the same time refraining from blaming patients for past failures to make and carry through such decisions. 28
In order to further professional non-judgmentalism, healthcare should be organized and managed in ways that as far as possible (i) reduce the inducements to morally judge patients, and (ii) help to separate such judgments, whenever they occur, from professional decisions and activities. Unfortunately, the holistic and narrative-centred focus of patient-centred care can easily take forms that do not contribute to this. Learning more about another human being can make it harder not to make social and moral appraisals of her.
29
Based on anthropological fieldwork in surgical units, Joan Cassel concluded that knowledge of the patients’ stories often leads to negative moral judgments. “The nurses always know the patients’ stories: the accidents, tragedies, and sorrows that brought them to the hospital, their family constellations, and their clashes with others and, on occasion, with the criminal justice system. As a result, however, some nurses make harsh moral judgments.”
30
Conflict 6: Holism versus professional egalitarianism
One of the central tenets of medical ethics is the equal rights of patients to receive adequate treatment. When patients are treated differently, that should be for reasons based on their medical needs, as opposed to medically irrelevant reasons such as their economic or social standing or the personal relationships they build with healthcare personnel. For this to be achieved, healthcare professionals must refrain from all forms of discriminatory, preferential, or otherwise unequal treatment. Even in healthcare systems that recognize everyone’s equal right to treatment and care, there are several mechanisms that can undermine good practice in this respect. Patients risk being subjected to discriminatory treatment because they are perceived as irresponsible, blameworthy, overly demanding, or simply unsympathetic. On the other hand, patients with whom healthcare personnel can easily identify may be unjustly favoured. Such deviations from professional egalitarianism can become more difficult to avoid if the relationship between patients and personnel go beyond the bounds of professionalism, and the development of more personal relationships is encouraged.
Based on observations in Californian healthcare in the 1960s, Glaser and Strauss reported that the attention dying patients receive from their nurses is influenced by the degree of social loss that the nurses assign to their death. The social loss depends on how the patient’s life is valued “more or less, on the basis of various social characteristics: for example, age, skin color, ethnicity, education, occupation, family status, social class, beauty, ‘personality’, talent, and accomplishments.”
32
In consequence: “Low social loss patients may hardly bother them; high social loss patients can be very upsetting. The secondary impact of social loss is on patient care. Low social loss patients tend to receive minimal routine care. In some few cases, low social loss patients may receive less than routine care. For example, at peak hours on emergency wards, when the staff must engage in split-second priority decisions concerning attention and treatment, low social loss patients can easily be forgotten for several minutes. High social loss patients often receive more than routine care. Extra ‘good will’ efforts are made to talk with them, to keep up their spirits, to make them comfortable, and to watch for sudden changes in their condition. However, if the high loss of such a patient is too upsetting for the nurses, he may find himself, like the low social loss patient, receiving only routine care.”
33
These observations were made long before the advent of the modern movement for patient-centred care, but the discriminatory mechanisms they describe appear to be general in their nature. Increased knowledge about circumstances in a patient’s life may in some cases strengthen the tendency to perceive her as either ‘high loss’ or ‘low loss’. We then have a potential ethical conflict between, on the one hand, the usefulness of extensive information about the patient, and on the other hand, the caregivers’ ability to uphold equality in treatment, caregiving and other professional interactions with patients.
Conflicts relating to personal relationships with patients
The second group of potential conflicts relates to another common feature of patient-centred care, namely the establishment and maintenance of personal relationships between patients and healthcare personnel. The ideal is that these relationships should be mutual and go beyond the more limited types of relationships that are conceived as professional. The foundations of these more personal relationships are supposed to be laid down by the patient’s narrative, and then further strengthened through continued contacts and collaborations as well as through further additions to the narrative. “In patient-centered care, health professionals seek a partnership with each patient that features shared control in consultations, decisions, and management of health issues, and a personalized relationship with each patient that acknowledges the conditions that shape what is meaningful for each patient.”
34
Conflict 7: Personal relationships versus the advantages of specialization and teamwork
There is ample evidence that a high degree of specialization is helpful in healthcare. The quality of clinical judgment increases as physicians and nurses gain experience from a large number of patients with similar medical and psychosocial conditions. Similarly, the quality of interventions such as surgery increase when the same person performs many interventions of the same type. 36 Specialization is often coupled to teamwork in which healthcare personnel with different educations and specializations co-operate, each contributing their part to the treatment. Today, professionalism in the healthcare professions requires collaborations within and between professions and specialties. 37
The personal relationships that are fostered in person-centred care require continuity of care and concentrate the patient’s contacts with healthcare to a small number of healthcare personnel. Such arrangements tend to be advantageous in terms of the psychological quality of the patient’s encounters with healthcare. However, other aspects of the quality of care are often better served by a division of labour such that several specialists rather than a single generalist take care of the patient. There is a potential ethical conflict between on the one hand, the concentration of the patient’s contacts to a small number of persons with whom she can build personal relationships, and on the other hand, the medical advantages of specialization and teamwork. This conflict has been implicitly recognized in the literature on person-centred care where it is observed that “models of staffing, such as team medicine” are obstacles to patient-centred care and lead to a situation in which “the patient’s narrative and care are fragmented”. 38 The flip side of this coin is, of course, that the models of staffing required for such versions of patient-centred care can in some cases stand in the way of the medical advantages obtainable with specialization and teamwork.
Conflict 8: Personal relationships versus the well-being of healthcare professionals
Close personal relationships with patients can put severe demands on healthcare personnel. They have to develop “a personal way of approaching, connecting and partnering with patients and families that build[s] on social and interpersonal ethics and skills inasmuch as professional skills”. 39 This is said to require “clinicians extending themselves as full human beings”. 40 Extending oneself as a “full human being”, without the usual protection of professional detachment, can make the work more taxing and psychologically demanding. It is usually more stressful to console someone with whom one has a close relationship than someone with whom one has a more disengaged relationship. It may therefore be counterproductive to recommend healthcare personnel to unleash the same type of empathetic emotions professionally that they have towards people close to them in their private lives. This has been confirmed in recent findings on so-called empathy fatigue among healthcare professionals. While exerting a certain level of empathy has been shown to be positively correlated with physicians’ health and well-being, maintaining a high level of empathy in many patient encounters can be emotionally tasking and lead to empathy fatigue and burnout. 41 Interestingly, however, studies have shown that compassion is compatible with sustainable and efficient caregiving, 42 and that compassion training can increase prosocial behaviour among trainees. Such training can make it possible to provide compassionate and psychologically satisfactory care in ways that are sustainable also from the viewpoint of the healthcare practitioners’ own health and well-being. 43
In conclusion, there is a potential ethical conflict between, on the one hand, the positive effects for patients of being cared for by healthcare personnel going beyond the conventional limits of a professional relationship and, on the other hand, the well-being of these professionals.
Conflicts relating to shared decision-making
The concept of “shared decision-making” was introduced in the 1970s. It has increasingly been seen as an essential component of patient-centred care.
44
It has been described as “a technique that can be employed when trying to find common ground with patients”.
45
Charles et al. offer four criteria of shared decision-making: “1. At a minimum, both the physician and patient are involved in the treatment decision-making process. 2. Both the physician and patient share information with each other. 3. Both the physician and the patient take steps to participate in the decision-making process by expressing treatment preferences. 4. A treatment decision is made and both the physician and patient agree on the treatment to implement.”
46
Against this background, the promotion of shared decision-making as part of patient-centred care can be understood in two different ways. According to one interpretation, shared decision-making is not a specific form of decision-making, but rather a move away from the old paternalistic model. Sometimes this interpretation of person-centredness comes close to the model of the patient’s informed choice: “Person-centredness moves the onus of health care away from the paternalistic model … Instead it shifts power to the person … by providing knowledge and the ability to make relevant decisions. Recognising the person as the centre of care should encourage staff to respect and support the person’s decisions, particularly after ensuring the person is given the respect of full explanations. This empowerment acknowledges the lived experience and the experience to come.”
49
“The test of a shared decision (as distinct from the decision-making process) is if both parties agree on the treatment option. This does not mean that both parties are necessarily convinced that this is the best possible treatment for this patient, but rather that both endorse it as the treatment to implement … Through mutual acceptance, both parties share responsibility for the final decision. This is an important characteristic and helps to distinguish shared decision-making from other models of decision-making. In the extreme case of the paternalistic and informed models, decision-making and ultimate responsibility for the decision are clearly vested with the physician or the patient respectively, and whether the opposite party accepts the decision is not relevant.”
50
“Two models of the patient-professional relationship have dominated the debate surrounding this challenge. For the sake of simplicity, while recognizing the caricatures involved, these may be referred to as ‘medical paternalism’ and ‘patient sovereignty’. … In the view of the Commission, neither extreme adequately reflects the current nature and needs of health care. The debate has increasingly become an arid exercise, which the Commission believes should be replaced by a view that reflects the tremendous diversity of health care situations and relationships today. In this Report, the Commission attempts to shift the terms of the discussion toward how to foster a relationship between patients and professionals characterized by mutual participation and respect and by shared decision-making.”
51
The second of the two above-mentioned interpretations of shared decision making gives rise to value conflicts and dilemmas that differ from those emanating from the informed choice model. In what follows we will therefore focus on this intermediate interpretation of shared decision-making. We have identified four potential ethical conflicts that it might give rise to.
Conflict 9: Shared decision making versus patient autonomy
There is an obvious mismatch between shared decision-making and patient autonomy. As can be seen from the above quotations, proponents of shared decision-making have made it clear that they recommend healthcare professionals to consider themselves as participants in the decision-making process, rather than facilitators or advisors. This is particularly clear in the (not uncommon) practice of describing the decision-making process as a “negotiation” between a physician and her patient. 55
It has been argued that shared decision-making is preferable to the informed choice model since various factors, e.g. lacking education and a stressful situation, reduce patients’ abilities to make the decisions that the latter model assigns to them. Consequently, “expecting people to actively promote their own health is justified only when they have the capacity to be reasonably expected to do so and when others in society create a realistic opportunity for them to do so.” 56 It has also been argued that “an apparently under-examined, individualistic view of patient autonomy that isolates the patient as decision maker may linger among health professionals in practice and contribute to difficulties implementing patient-centred care.” 57 Such pronouncements confirm that there is a potential ethical conflict between shared decision-making and patient autonomy.
Conflict 10: Shared decision-making versus treatment quality and patient safety
In the standard approach to healthcare ethics, the principles of non-maleficence and beneficence have essential roles in safeguarding treatment quality and patient safety. Patients should only be offered treatments that are, according to the best available information, medically beneficial. In particular, interventions that are expected to have predominantly harmful effects should not be offered. The physician is responsible for not harming the patient. This is a responsibility that is not nullified by the patient’s consent, or even by the patient’s active request for the treatment in question. For instance, a patient with a heart condition that contraindicates sildenafil (a drug against erectile dysfunction) should not receive a prescription for the drug, even if he entreats for it. (It has been proposed that with patient-centring, physicians can “free themselves from some of the responsibility for unwise decisions or unfavorable outcomes”, which could be “the beginning of a sophisticated defense against malpractice litigation”. 58 The legal tenability of such a strategy is unclear.)
In the informed choice model, it is the physician’s task to offer treatment alternatives that are medically beneficial and provide the patient with the appropriate information and advice for choosing whether to accept some of these offers. The decision ultimately rests with the patient. The model of shared decision-making tones down the distinction between these two roles. In the previous section, we noted that the resulting indistinctness of the roles can infringe on the patient’s autonomy and sovereignty as a decision-maker. Further, particularly in a negotiatory framework, it can also weaken the physician’s mandate to identify and offer (only) treatments that are medically beneficial. Some proponents of shared decision-making do not seem to see this as a disadvantage. “Evidence-based healthcare will always, by definition, apply standardized care models based on the response of cohorts to treatment; when these models fail to capture minority responses of individuals, personalized medicine and PCC are ways for us to help nuance the models and identify and properly respond to individual exceptions.”
59
Conflict 11: Shared decision making versus avoiding treatments that harm others
The healthcare professions are fiduciary in the sense of involving a duty to serve, primarily, the medical interests of each individual patient. Like other fiduciary relationships it is restricted in various ways. One of these limitations precludes it from being conducted in ways that are harmful to third parties. The model of shared decision-making would seem to make it more difficult for the physician to turn down patients’ wishes for such interventions. Overuse of antibiotics is a prime example. The World Health Organization describes antibiotic resistance as “one of the biggest threats to global health, food security, and development today”, 61 and presumably, most physicians are well aware of the danger. However, some patients demand antibiotics even though no such drug is medically required or at all effective (e.g. viral infections). Due to factors such as empathy and a desire to maintain a good relationship with the patient, some physicians make medically unjustified prescriptions that contribute to resistance development. The less distinct role assigned to the physician in some versions of shared decision-making can make it more difficult to say no to a patient who insists that she needs an antibiotic. Gwyn and Elwyn noted that it “might be a misnomer” to describe an interaction in which a physician refuses to prescribe antibiotics that the patient desires as a case of “shared decision-making”. 62 It should also be mentioned that overuse of healthcare resources can have negative economic consequences for the healthcare system and for society at large. In conclusion, there is a potential ethical conflict between shared decision-making and the avoidance of healthcare decisions that are harmful to third parties.
Conflict 12: Shared decision-making versus equality and non-discrimination
As already mentioned, it is an essential tenet in healthcare ethics that the available resources should be allocated in accordance with the patients’ needs, objectively defined. 63 Overuse of scarce medical and caregiving resources can reduce or delay access to such resources for the patients who need them the most. A system of shared decision-making can be expected to provide resourceful patients with more opportunities to increase their share of healthcare resources. Since these resources are finite, their gains would come at the expense of other patients. The losers will likely be found among those who are already worst off in other respects, for instance among those with less than perfect mastery of the language in which the shared decision-making takes place, and other groups subject to structural discrimination. We therefore have reasons to be on our guard against a potential ethical conflict between shared decision-making and a non-discriminatory healthcare.
Conclusions
The twelve conflicts that we have identified are summarized in Figure 1. In conclusion, we would like to again emphasize our strong support of the basic principle that healthcare should have its patients at the centre of its activities and deliberations. However, in order to fully realize the potential of that principle, its application should be based on a careful analysis that also takes into account other sound ethical principles as well as the practical conditions under which various forms of healthcare take place. As a contribution to that analysis, we have set out in this article to identify major potential ethical conflicts that may have to be taken into account in the development and implementation of patient-centred care.
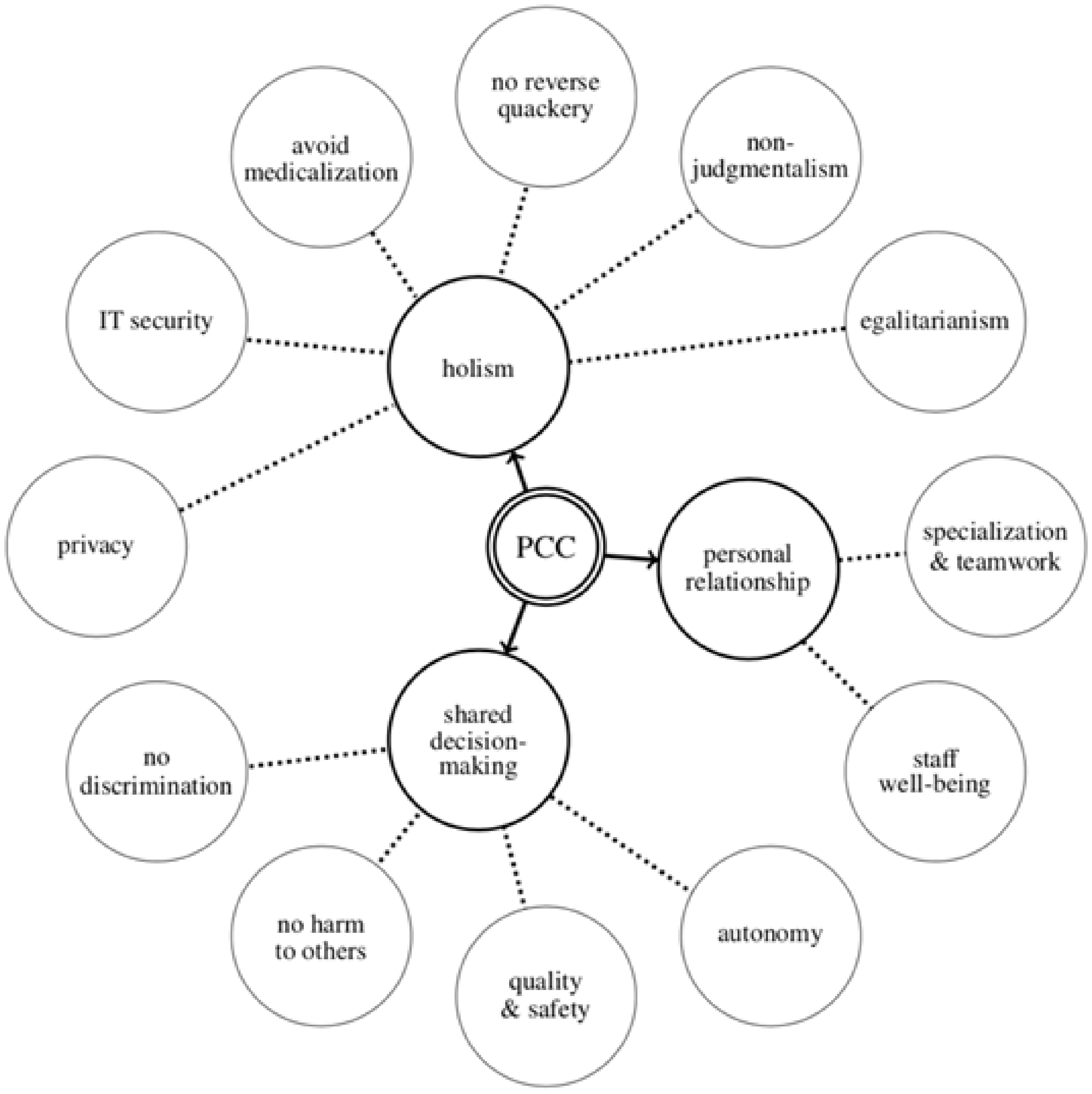
A schematic summary of the twelve potential ethical conflicts between patient-centred care and other ethical requirements in health care that are discussed in the article.
Our study confirms that some of the ways in which patient-centred care has been specified can potentially have ethically problematic consequences. One underlying theme that has a role in several of the potential ethical conflicts is the difficult balance between, on the one hand, making full use of the healthcare personnel’s expertise and professionalism, and on the other hand, honouring the wishes of the patient. Another such underlying theme is the limitation in financial and human resources that prevents the realization of many good ideas in healthcare, including some of those that are associated with patient-centred care.
Unfortunately, the discussion on patient-centred care has not been immune to over-simplifications such as a “one size fits all” perspective on patient-physician and patient-nurse relationships. Patient-centred care may have to take different forms, depending of the nature of the disease, the patient’s life situation, and the economic, organizational and technological resources available to the healthcare unit. For instance, the optimal form of a patient-physician relationship may differ radically between an orthopaedic clinic, a drug abuse clinic, and a unit for palliative care. A considerable diversity is desirable. We need a broad discussion of the goals, means, and methods of patient-centredness that does not take current specifications and conceptions of patient-centred care for granted.
Author's Note
Sven Ove Hansson is also affilaited with Department of Learning, Informatics, Management and Ethics Karolinska Institutet, Stockholm, Sweden.
Footnotes
Authors’ contributions
Both authors have contributed to an approximately equal extent both to the underlying research and to the writing of this article, the first author to a somewhat larger extent.
Acknowledgements
Thanks are due to our colleagues at the Royal Institute of Technology and Karolinska Institutet for valuable comments at seminars and in informal discussions.
Availability of data and material
The data used for this study consists in the publicly available research literature that is listed as references.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
No human participants, human data, or human tissue were used in this study. Therefore, according to Swedish law, ethics approval is neither required nor obtainable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was jointly supported by Vetenskapsrådet and Forte, award 2014-4024.