
Abstract
The COVID-19 pandemic has highlighted the difficult task of balancing access to misinformation with respect for patient decision-making. Due to its innate antagonism, the paradigm of “physician paternalism” versus “patient autonomy” may not adequately capture the clinical relationship. The authors hypothesized that most patients would, in fact, prefer significant physician input as opposed to unopinionated information when making medical decisions. There is a lack of empirical data corroborating this in the United States. To that end, a survey was distributed to 650 individuals through Amazon Mechanical Turk, of which 499 responses met pre-determined quality criteria. Most respondents believed their doctor's insight would be better than their own if injured or gravely ill. When asked to affirm preferences separately, a significantly higher proportion of respondents preferred guidance from their doctor when making medical decisions compared to being presented with unopinionated information (p < 0.001). Encouragingly, 93.1% believed that the doctor's primary goal was their health. When asked directly to compare physician guidance to unopinionated information, 69.1% respondents stated they would prefer physician guidance. We found a consistent association between educational/economic background and affirmative responses (p < 0.001), suggesting particular attention should be paid to patients that are disadvantaged with respect to these demographic factors. The belief in a shared goal, and a consistent preference for physician input, suggests that patients endorse a more collaborative view of the clinical dynamic than is suggested by the paternalism-autonomy paradigm. This pilot study suggests physicians should not be afraid to communicate conviction with regard to treatment decisions.
Introduction
Popularization of misinformation during the COVID-19 pandemic has showcased mistrust in the medical community and, in doing so, cast a spotlight on the paradigm of autonomy vs. paternalism. In a healthcare climate where both credible data and misinformation are so readily available to patients, the physician is tasked with providing guidance while simultaneously respecting patient decision-making. This balancing act of “shared decision making” (SDM) is best achieved in an openly collaborative, rather than covertly antagonistic, environment. In this paper, we provide empirical evidence that suggests the autonomy-paternalism paradigm does not adequately capture the patient–physician relationship.
The subtle pitting of patient against physician—autonomy against paternalism—may in part be due to a historical mistake. Jonsen and coauthors wrote Clinical Ethics: A Practical Approach to Ethics in 1982, aiming to give clinicians concrete guidelines based on the philosophical foundations established in 1979 in the well-known Belmont Report and Principles of Biomedical Ethics.1,2 However, Jonsen later described an important “conceptual mistake” in these texts—the conflation of research ethics and clinical ethics. 3 The basic problem that Jonsen identified is that the relationship between a researcher and subject is notably different from that between physician and patient. For various reasons, researchers are more readily at risk of violating Kant's dictum and treating their subjects “as a means only”—note that even the word “subject” suggests this. 4 In contrast, the core of the patient–physician relationship consists of a common goal: the patient's well-being. This common goal means the relationship is more like a partnership, and less like the contractual relationship of research, which is focused on keeping the subject safe from overreach. Because of this, Jonsen concludes, clinical ethics is a “thoroughly different matter” from research ethics. 3 Yet the confusion of the two domains has had downstream effects on the culture and ethical conscience of clinical medicine; insidiously, it may have fostered an unnecessary antagonism between physicians and patients. This background antagonism may have led to two problems.
First, conflating the position of the patient with that of the research subject may have helped promote individualistic notions of autonomy. Such accounts of autonomy have long been criticized, especially from within feminist philosophy.5–7 Relational accounts of autonomy, in contrast, acknowledge that “agents are situated in historical, social, class, race, and gender contexts” which are not so easily separable from the exercise of agency. 8 If this is indeed the case, a relational understanding of autonomy is essential to providing patient-centered care. 9 These insights have gained some traction in bioethics, in what has been described as “relational turn.” 10 However, the fundamental conflation described above may help explain the perseverance and prevalence of individualistic notions of autonomy in clinical practice.
Secondly, taking a research approach to medical decision-making places the associated responsibilities mostly on patients. The idea of “SDM” better captures the relationship that should be aimed for in a clinical context. 11 It consists of the patient and physician coming together to assess the available evidence and make a decision that aligns with the patient's values. SDM has been noted to improve the “quality of clinical decision-making,” 12 as evidenced by a Cochrane review examining patient decision aids for preference-sensitive decisions. 13 SDM has also gained traction internationally and has been endorsed in a consensus statement by representatives from at least 18 countries. 14 Savulescu has gone even further with his “liberal rationalism” model, arguing that if objectivism about value is true (i.e. that there are states that are objectively good for people), then there is a role for physicians to rationally discuss their own value judgments about a clinical situation with patients. 15 Thus, there are already established grounds for arguing that physicians should substantively contribute to medical decision-making, with the content of this input ranging from factual information for SDM to normative guidance in the liberal rationalist model.
Interestingly, to our knowledge no studies have surveyed a large cohort of the general public regarding attitudes toward receiving physician guidance during medical consultation. Given the severe degree of information asymmetry 16 in the clinical relationship, we hypothesized that most patients—especially when vulnerable or in pain—would prefer guidance over having their physician “spread an array of vendibles” in front of them. 17 The aim of this study was to provide insight into patient perspectives in the United States regarding this important issue.
Methods
This cross-sectional survey study design and data reporting was conducted in accordance with STROBE guidelines for observational studies. 18 A web-based survey was created using Qualtrics (Provo, UT). Evidence within policy writing research has shown that third-person language makes respondents more suggestible to “nudges,”19,20 so survey questions were written in the first person to minimize this effect. Five Likert-type questions were designed on a 5-point scale. 21 Demographic data was collected, including free-text options for sex and ethnic background. Economic background was assessed using the 2021 Department of Health and Human Services federal poverty guidelines of $12,880 per individual and $26,500 for a family of four. A case scenario describing a mangled finger was designed and reviewed by a board-certified Hand surgeon with over 30 years of experience (SK). A copy of the survey instrument is available as supplemental data, and we recommend a brief review of the scenarios described in question 17 (Appendix). Given the completely anonymized nature of the web-based survey, no IRB review was required.
Quality control questions included requiring the respondent to input their age in years with a separate question asking for their year of birth. Surveys with a discordance between these responses were eliminated. Additionally, one question asked the respondent to pick only one specific answer in a multiple-choice list, and any surveys with a different answer were eliminated. Any surveys completed unusually quickly were flagged by the Qualtrics software and eliminated. At the end of each survey, a unique code was generated, and any surveys with incorrect codes were eliminated. Answers were required for each question, so no incomplete surveys were collected.
The survey was administered through Amazon's Mechanical Turk (MTurk) to English-speaking respondents based in the United States, with a compensation of $0.75 per survey. A target response of 500 high-quality surveys was set, and it was estimated that 30% of responses would not meet criteria. Therefore, a total of 650 surveys were administered. The survey was available for a period of 24 h.
Data were analyzed using descriptive statistics. For statistical comparison, Likert item responses were grouped into affirmative and negative responses, with neutral answers eliminated. In order to test differences between proportions, two by two tables were analyzed using
Results
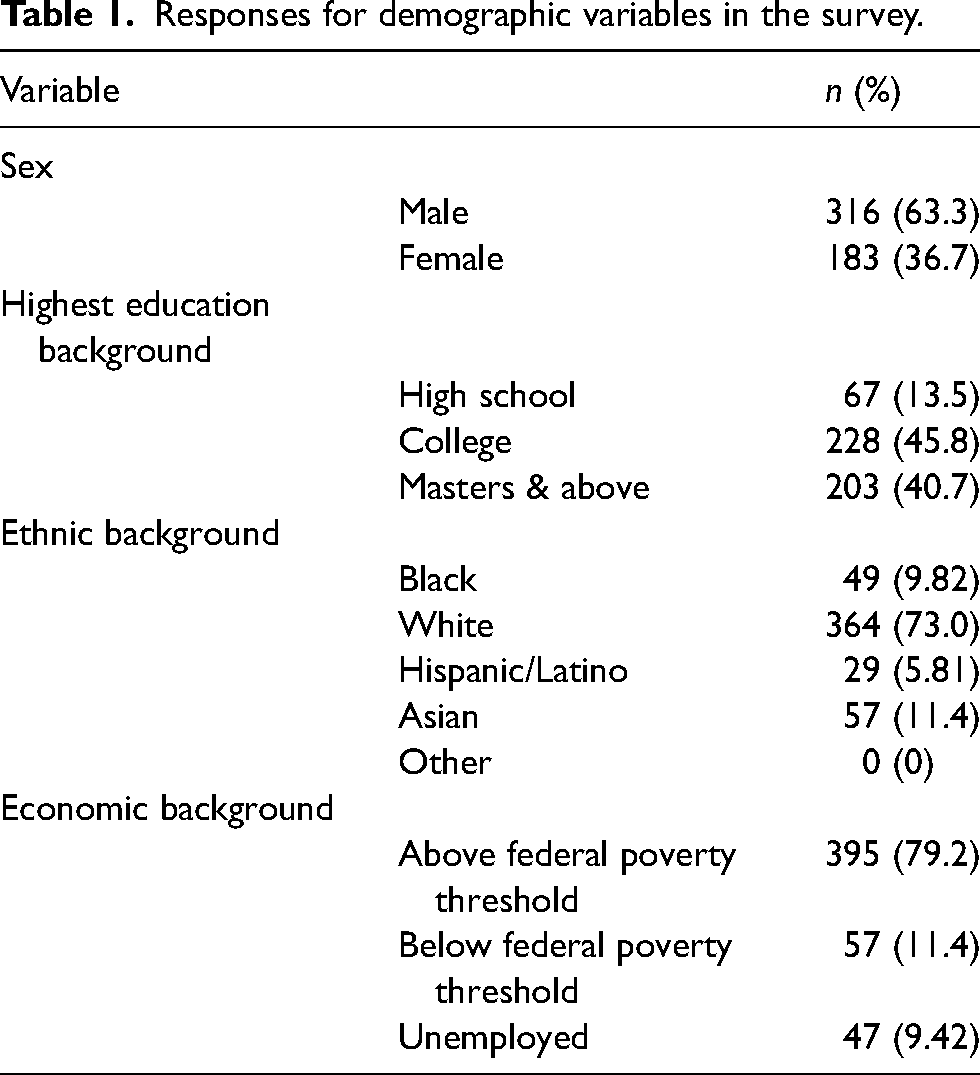
Six surveys were rejected due to incorrect codes and re-issued. A total of 650 surveys were completed. Of those, 151 surveys did not meet quality criteria, resulting in a total of 499 survey responses. 63.3% of respondents were male, and the average age was 36.4 ± 9.71 years. 45.8% reported a college degree. In terms of ethnic background, 73.0% identified as White, followed by 11.4% Asian, 9.82% Black, and 5.81% Hispanic/Latino. No free-text entries identifying as “other” were made. 79.2% reported being above the federal poverty threshold, 11.4% reported being below, and 9.42% reported being unemployed at the time of the survey. These findings are summarized in Table 1.
Responses for demographic variables in the survey.
95.8% of respondents reported being to a doctor within the last year, and 88.6% reported experiencing a physical disability or disfiguring injury requiring care. 87.2% reported having a chronic medical condition requiring care. Of patients who had received care, 88.2% reported feeling that they had formed a relationship with their doctor.
Responses to Likert questions 1 through 5 (LQ1–5) are graphically demonstrated in Figure 1. In response to LQ1, most respondents believed their doctor's insight would be better than their own if they were injured or gravely ill. Respondents were more likely to respond in the affirmative when stratified by educational or economic background (p < 0.001). For example, respondents above the federal poverty level were much more likely to believe their doctor's insight would be better compared to unemployed respondents (p < 0.001, OR 7.25, 95% CI 3.44–14.5). In response to LQ2, most respondents believed they would be able to make a rational, well-informed decision if sick or injured. Respondents were more likely to respond in the affirmative when stratified by educational or economic background (p < 0.001). For example, respondents with a master's degree and above were much more likely to respond in the affirmative compared to respondents with a high school degree (p < 0.001, OR 8.71, 95% CI 3.11–26.0). The overall proportion of affirmative and negative responses to LQ1 and LQ2 were compared and found to have no significant difference, with most respondents choosing an affirmative answer (Figure 2A).
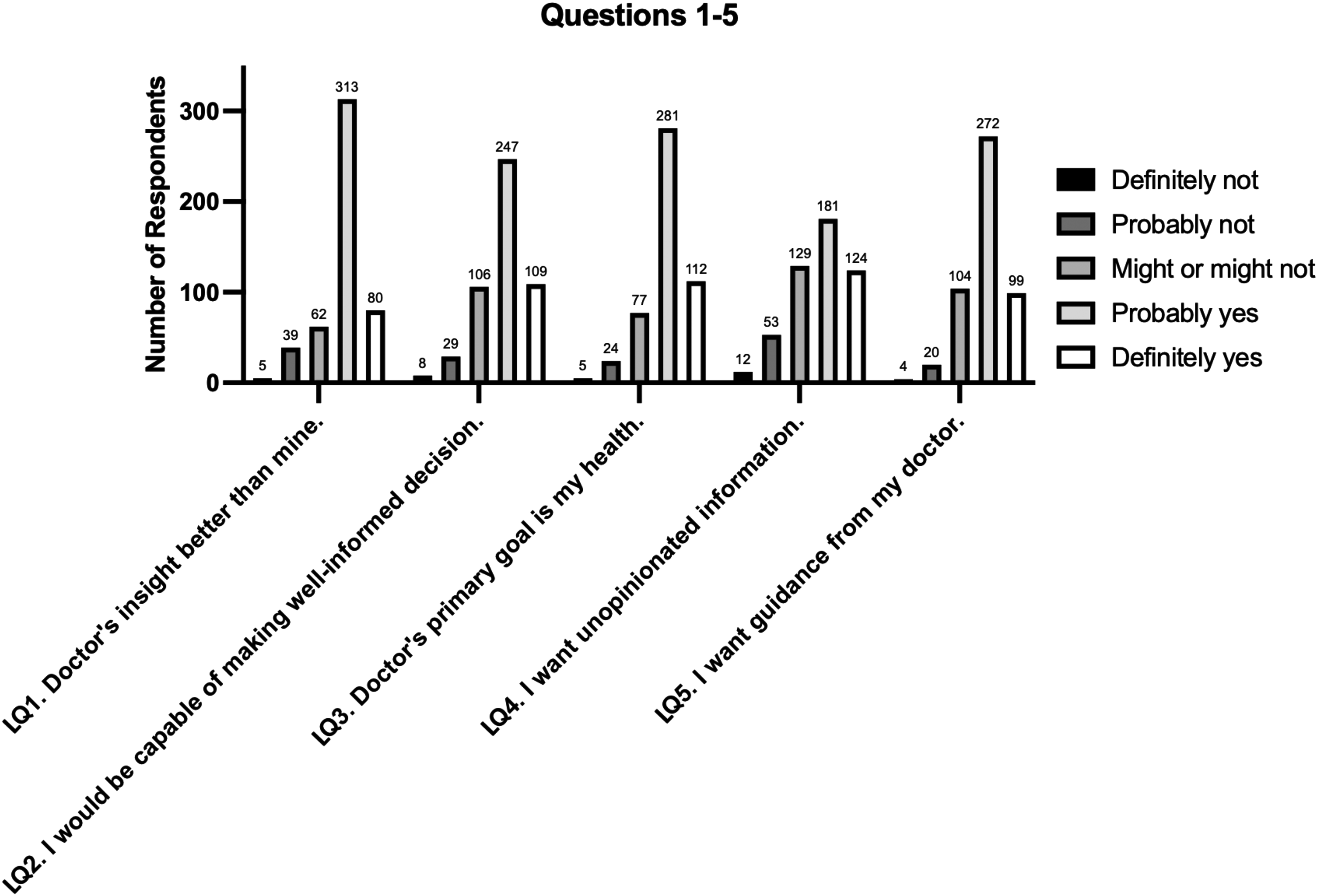
Frequency of responses to survey questions 1 through 5, on a 5-point Likert scale.
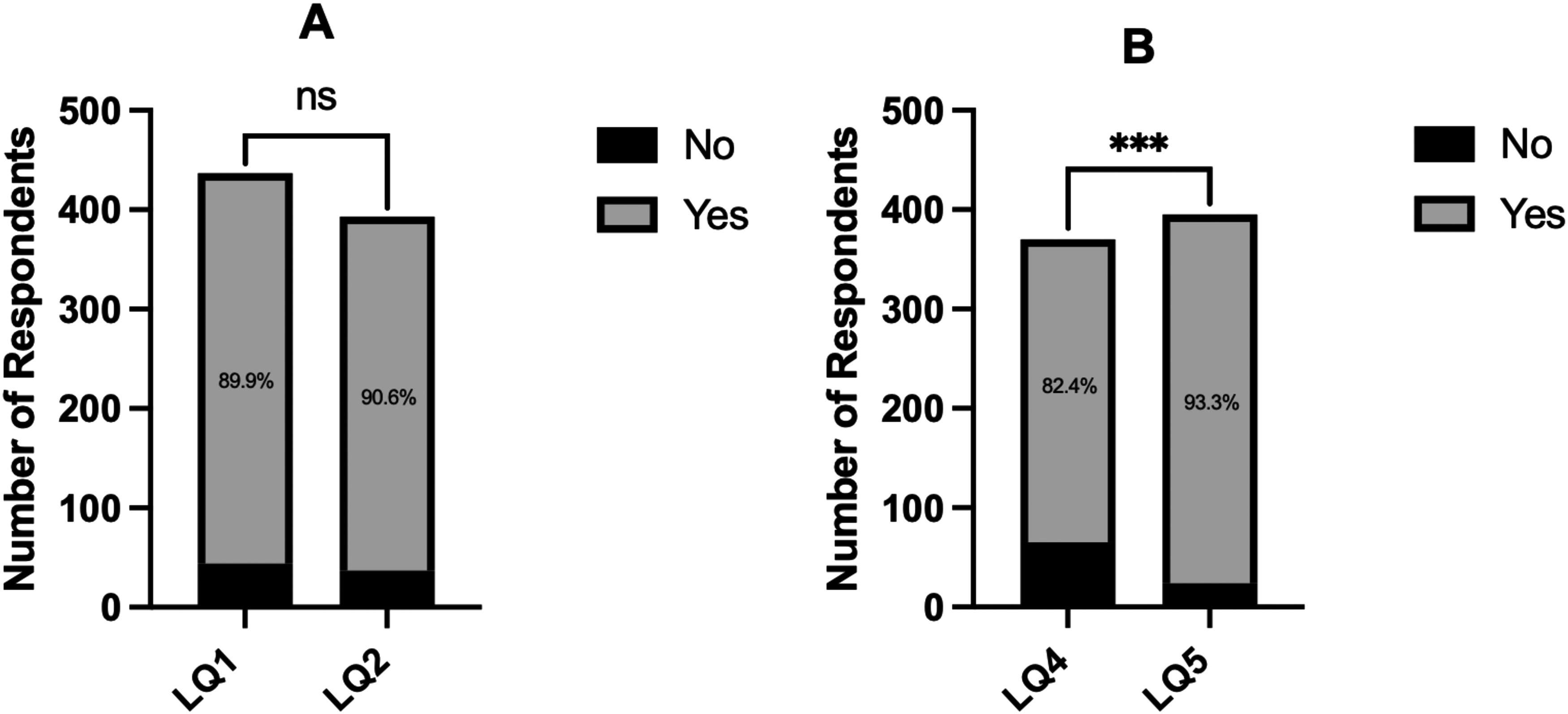
Response frequencies and statistical comparison of Likert questions 1 and 2 (A) and Likert questions 4 and 5 (B). ns = not significant.
Most respondents believed that the doctor's primary goal was their health, with 93.1% choosing an affirmative answer to LQ3. Respondents were more likely to respond in the affirmative when stratified by economic background (p < 0.001). For example, respondents above the federal poverty level were more likely to respond in the affirmative compared to unemployed respondents (p < 0.001, OR 4.52, 95% CI 2.08–9.95).
There was a more even distribution in response to LQ4, which queried the patient's desire for unopinionated information from their doctor. Again, we observed that respondents were more likely to respond in the affirmative when stratified by educational and economic background (p = 0.001 and p < 0.001, respectively). For example, respondents above the federal poverty line were more likely to want unopinionated information compared to unemployed respondents (p < 0.001, OR 4.14, 95% CI 2.12–8.20). A high proportion of affirmative answers was recorded in response to LQ5, which queried the patient's desire for guidance from their doctor. Respondents were more likely to respond in the affirmative when stratified by educational background (p < 0.001). For example, respondents with a master's degree or above were much more likely to desire physician guidance compared to respondents with high school degrees (p < 0.001, OR 6.58, 95% CI 2.23–20.0). The overall proportion of affirmative and negative responses to LQ4 and LQ5 were compared, which showed that a significantly higher proportion of respondents would prefer guidance from their doctor when making medical decisions compared to being presented with unopinionated information (p < 0.001) (Figure 2B).
When presented with the mangled finger scenario, most respondents reported that they would elect observation (40.7%) or repair (47.1%) despite the surgeon advocating for amputation (Figure 3A). Correspondingly, 356 (71.3%) reported that they preferred Scenario 1, where the surgeon presented the patient only with the treatment options and abstained from advocating for any one option (Figure 3B). No significant differences in response proportions were observed when stratified according to demographic variables.
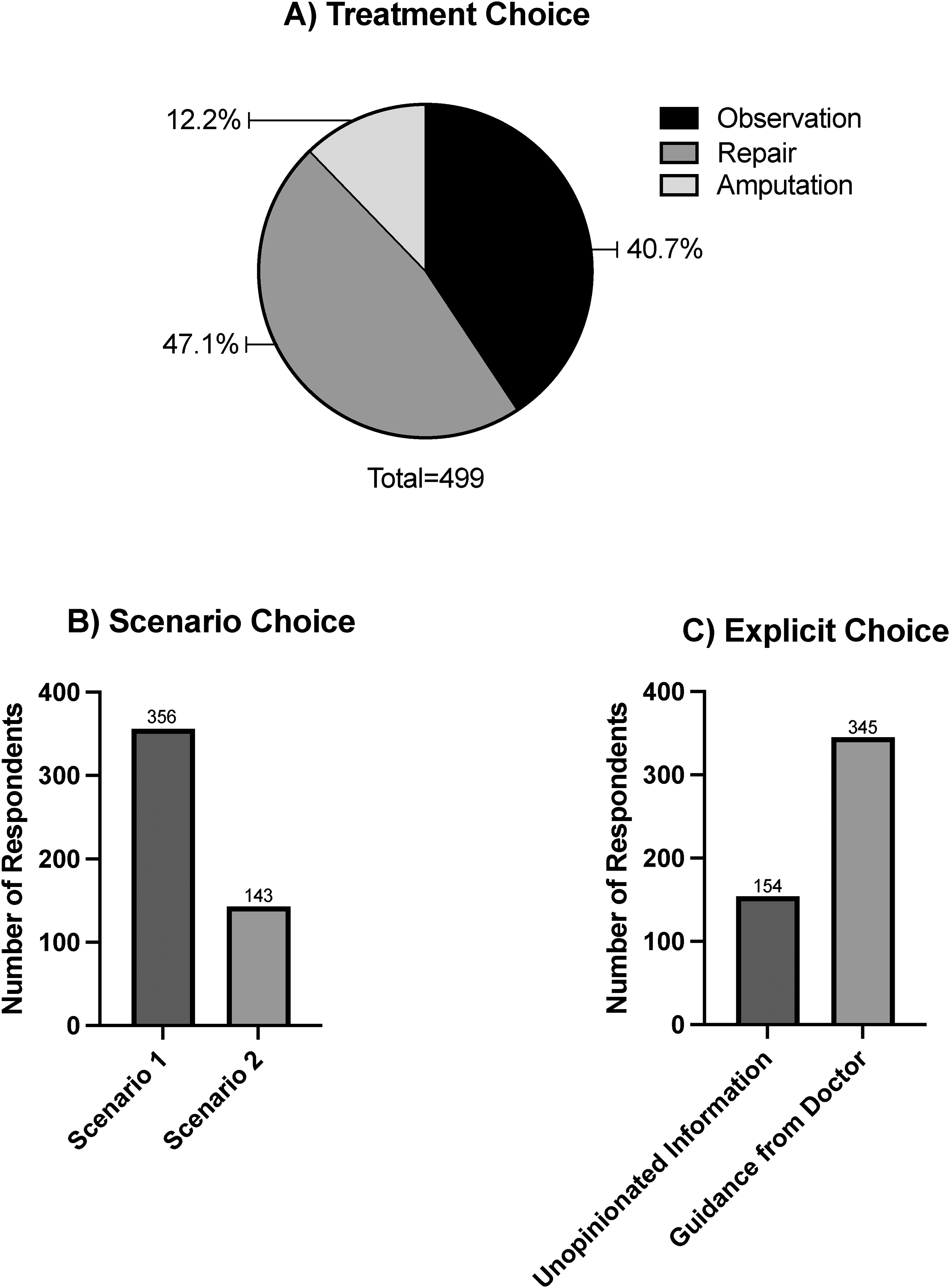
Responses to treatment choice (A) and scenario choice (B) for question 17 of the survey. Responses to direct final question regarding preference of unopinionated information versus guidance from doctor (C).
A direct, final question queried whether respondents preferred unopinionated information versus guidance from their doctor. Interestingly, the proportion of respondents indicating they wanted guidance from their doctor mirrored almost exactly the inverse of the Scenario preference (69.1%) (Figure 3C). Respondents were more likely to respond in the affirmative when stratified by self-reported sex and economic background (p < 0.001) (Figure 4). For example, females were over twice as likely to prefer guidance from doctor compared to males (p < 0.0001, OR 2.54, 95% CI 1.65–3.89) (Figure 4A). Overall, respondents thus appear to prefer guidance from their doctor when asked directly, despite indicating the opposite when presented with a difficult surgical scenario.
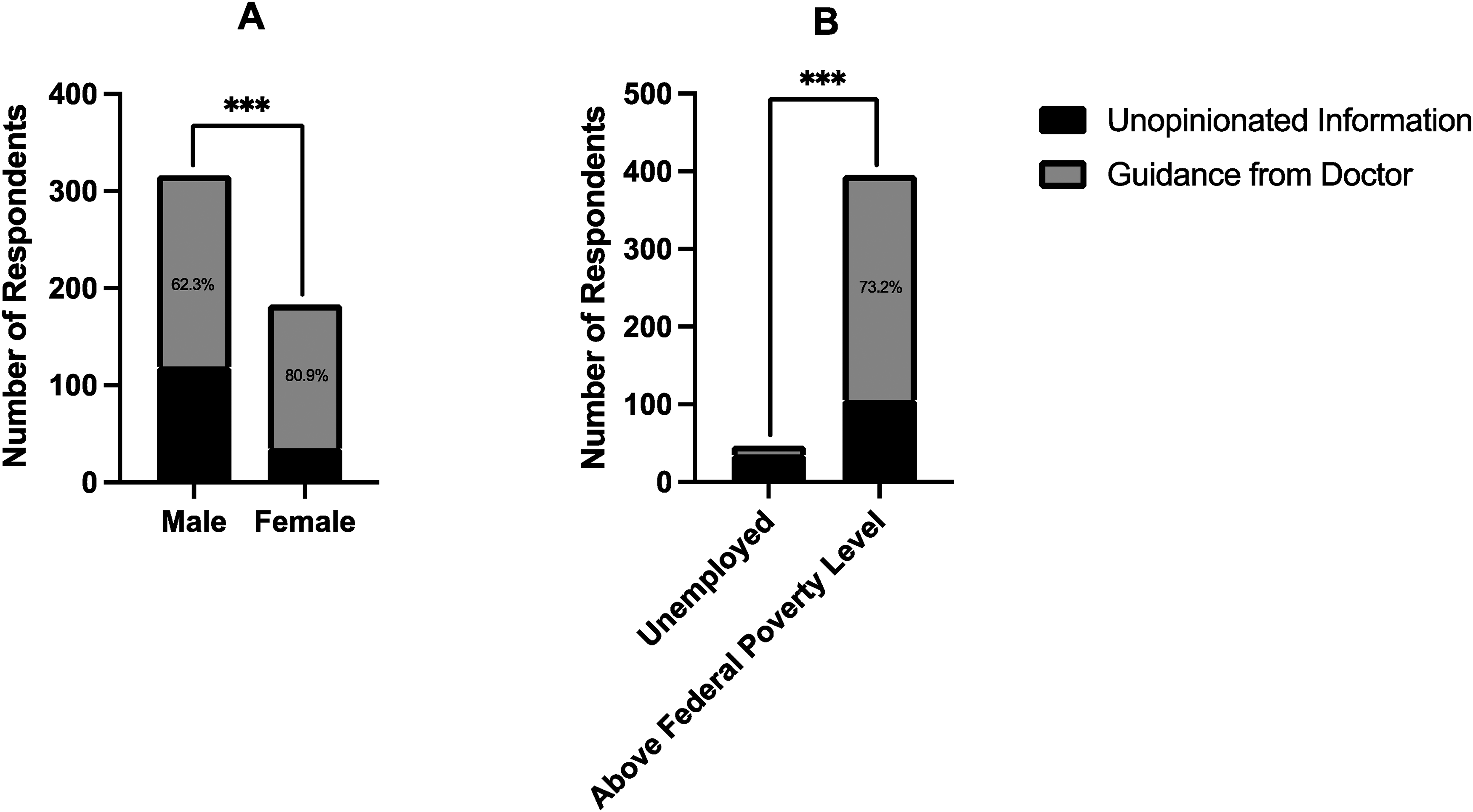
Response frequency and statistical comparison of question 18, which explicitly queried preference for unopinionated information versus guidance from doctor, when stratified by self-reported sex (a) or economic background (b).
Discussion
Most survey respondents (95.8%) reported receiving medical care within a year of completing the survey, indicating most had experienced being a patient. The data obtained from LQ1 suggests that most respondents value the insight of their physician and recognize that this insight may be better than their own even after multiple conversations. This reflects awareness of the information asymmetry inherently present in the patient–physician relationship. At the same time, responses to LQ2 suggest that respondents feel they would be capable of making a rational, well-informed decision when critically ill or injured. There was no significant difference in the proportion of affirmative responses between these questions. Given that the majority of responses to both LQ1 and LQ2 were affirmative, this suggests that most respondents think they are capable of making correct treatment decisions despite also believing that a physician's insight is better (Figure 2A). The two attitudes therefore do not appear to be mutually exclusive.
Over 78% of all respondents to LQ3 chose affirmatively to the suggestion that a doctor's primary goal is their health, with 15% choosing a neutral response. Furthermore, an encouraging 88% of those who had received medical care felt that they had formed relationships with their doctors. Mutual good faith as well as the belief in a common goal are critical to the clinical relationship. As Jonsen beautifully stated, the primary quality of healing is “the formation of a trusting alliance between physician and patient, in which the focus on the patient's needs is straight and clear, communication is honest and illuminating, and acceptance and collaboration are real.” 3 The philosophical roots of this idea extend even into the Kantian ethics that Jonsen asserts the Belmont Report was based on; indeed, the categorical imperative to treat persons as an end and never as a means only unifies two rational beings under in what he called a “kingdom of ends.” 4
LQ4 and LQ5 were designed to probe opinions on receiving unopinionated information and guidance in a non-mutually exclusive way, i.e. participants were given the opportunity to express a preference for both. It is possible that patients prefer to have guidance in some circumstances, and unopinionated information in others. The responses for LQ4 and LQ5 show an overall affirmative response to both questions, indicating these options are not necessarily seen as mutually exclusive. Notably, however, a statistically significantly higher proportion of respondents desired guidance from their doctor (LQ5), compared to those who wanted unopinionated information (LQ4) (Figure 2B). In contrast to LQ4 and LQ5, the final question of the survey was designed to force participants to choose between the two options. For this question, respondents were asked frankly whether they preferred guidance or unopinionated information, and overwhelmingly chose guidance (Figure 3C). Taken together, we believe that the non-comparative Likert questions and the comparative final question suggest an overall preference for guidance.
However, when presented with the case scenario, most people resisted the suggestion of finger amputation, with only 12.2% choosing the option recommended by the surgeon (Figure 3A). Although it is difficult to ascertain whether the responses indicate primarily an aversion to the recommended treatment (amputation) or a preference for unopinionated information, in the context of the rest of the survey the results may suggest that patients change their opinion on how they want information delivered based on the perceived acceptability of the doctor's recommendations. In this scenario, the surgeon recommended amputation of the mangled digit, which would result in better long-term functional outcomes but may appear more threatening to patients in the short term. This phenomenon has been previously observed. Rosenbaum described cognitive overload in patients for whom a coronary artery bypass graft would be more beneficial than a percutaneous coronary intervention in the long run, but who balk at the former option at the description of “cracking open” the chest. 22 She observes that patients often “make choices favoring the present over the long term.” 22 Our case scenario corroborates this same tendency, with a substantial portion of patients choosing treatments that were described as negatively affecting overall hand function in the long run. How information is presented certainly matters, but when discussing finger amputation or the cracking open of chests, physicians may need to go beyond presenting options. Communicating conviction regarding the best treatment plan may be as important as communicating the treatment plan itself.
There appeared to be a consistent association between educational background and affirmative responses. For example, patients with a master's degree or above were much more likely (OR 6.58) to desire guidance from their doctor compared to patients with a high school degree (LQ5). Similarly, economic background had a consistent association with affirmative responses. Employed respondents were more than seven times more likely to desire physician guidance in the final question of the survey compared to unemployed respondents. They also appear to have less trust in their doctor at the outset, as respondents above the federal poverty line were much more likely (OR 4.52) to believe their doctor's primary goal was their health compared to unemployed respondents (LQ3). We believe these results suggest particular attention should be paid to forging a relationship with patients of disadvantaged economic and educational backgrounds.
Few studies have empirically evaluated patient perspectives on the delivery of information during medical decision-making. Murgic et al. surveyed several focus groups regarding their perspectives on autonomy in post-soviet Croatia. 23 One of these groups included nine patients suffering from chronic disease. Interestingly this group acknowledged differences in the willingness to receive information, hinting at the cognitive overload described above. As stated by one patient: “… I wonder if all this information we hear confuses us and burdens us more than we can bear.” 23 Avitzour et al. conducted a survey in Israel on the concept of “nudging”—an idea which the authors argue has been studied from the perspective of state agencies and large employers, but without much empirical evidence from a doctor–patient relationship. 24 Although some perspectives were different between doctors and patients, there was no overall difference in the moral assessment of, and support for, “nudging” in clinical medicine. 24
Our findings provide further evidence that the paradigm of “paternalism versus autonomy” may incorrectly capture the clinical relationship. This paradigm may have arisen, in part, from a misunderstood historical context. Mccullough has convincingly argued that the “founding story” of contemporary bioethics involves an incorrect picture of rampant paternalism in medicine. 25 One example is the evidence used to support the view that paternalism is prevalent among physicians. A frequently-cited study published in 1961 found that 88% of physicians surveyed at a single institution had a policy of not informing patients of their cancer diagnosis. 26 However, on closer examination of this number, only 8% of physicians never told their patients, while “agreement was essentially unanimous that some family member must be informed if the patient is not made aware of the diagnosis.” 26 Well-known bioethics textbooks27,28 are also used to trace paternalistic principles to the Hippocratic tradition, due in part to its admonition to conceal aspects of care from the patient. This admonition should be taken in a context in which physicians were exhorted to protect trade secrets, in a society that did not share our contemporary views on individualism. 25 Furthermore, Mccullough points out that the tradition of reciting the Hippocratic Oath did not become commonplace until after WWII, suggesting its longstanding influence on the practice of medicine is unlikely.25,29 Lastly, there are known cultural 30 and inter-familial 31 differences regarding how patients want information delivered to them. These differences may be accounted for with the flexibility afforded by a trusting clinical relationship, less so by the rigidity of the contractual researcher-subject paradigm which pits the patient against the physician.
Some limitations of this study include differences in demographic characteristics of respondents that may limit generalizability. For example, despite only setting geographic cutoffs to our survey, our sample had a much higher proportion of males (63.3%) and most respondents were white (73.0%). It is possible that this affected the overall response patterns observed. However, neither sex nor ethnic background was consistently associated with significantly different response patterns to LQ1-LQ5. In contrast, respondents consistently had significant differences in response to these questions when stratified by education level and economic background. Furthermore, female respondents were significantly more likely to choose “guidance” for the final question compared to males (Figure 4A). This indicates that, even though they were the minority of respondents (36.7%), the responses provided by females were in overall alignment with the rest of the study. Another limitation present in our study is that we did not conduct qualitative interviews or collect free-response answers to elucidate why patients chose certain answer choices. It is possible that respondents understood certain terms (such as “guidance” or “unopinionated”) differently, which might have impacted response patterns. Such insights might have provided further information as to any observed discrepancies. With regard to LQ4 and LQ5, even though there was a significant difference between the proportion of affirmative responses, there was a general trend towards affirmative responses for all the Likert questions (Figure 1). The authors also acknowledge that p-values are no absolute indication of correlation and certainly not of causation. However, given the large sample size and low alpha value, we do believe the differences in proportions observed are not likely due to chance. Finally, in the case scenario, it is difficult to ascertain whether the overall negative responses to the surgeon's suggestions are because respondents disliked the recommended choice (amputation) or because they preferred non-opinionated information. Future studies should include several scenarios where the recommended options differ in severity, in order to elucidate whether there is a discernable trend. Additional future directions include conducting qualitative, one-on-one interviews with patients, as well as evaluations in different global regions.
Conclusion
This survey of nearly 500 respondents in the United States demonstrates that patients respect their physician's insight and desire guidance from them when making medical or surgical decisions. This propensity varies by certain demographic factors, especially economic and educational background. However, patients also appear less likely to prefer scenarios where physicians provide opinionated guidance when the advice is difficult to receive. This highlights the importance of establishing relationships and trust with patients. Finally, this study provides empirical evidence of the view that the paternalism-autonomy paradigm may not adequately capture the clinical relationship from the patient's point of view. The intrinsic information asymmetry between doctor and patient can only be overcome in the context of viewing the relationship as a partnership—as opposed to the implied antagonism brought about by the paternalism-autonomy paradigm.
Supplemental Material
sj-docx-1-cet-10.1177_14777509231210770 - Supplemental material for Communicating conviction: A pilot study of patient perspectives on guidance during medical decision-making in the United States
Supplemental material, sj-docx-1-cet-10.1177_14777509231210770 for Communicating conviction: A pilot study of patient perspectives on guidance during medical decision-making in the United States by Karel-Bart Celie, Allyn Auslander and Stuart Kuschner in Clinical Ethics
Supplemental Material
sj-xlsx-2-cet-10.1177_14777509231210770 - Supplemental material for Communicating conviction: A pilot study of patient perspectives on guidance during medical decision-making in the United States
Supplemental material, sj-xlsx-2-cet-10.1177_14777509231210770 for Communicating conviction: A pilot study of patient perspectives on guidance during medical decision-making in the United States by Karel-Bart Celie, Allyn Auslander and Stuart Kuschner in Clinical Ethics
Footnotes
Acknowledgements
The authors would like to thank Joanna Demaree-Cotton, PhD, for comments that helped improve this paper. They would also like to thank the two anonymous reviewers whose comments improved this manuscript. This study was presented by the first author (KBC) at the International Conference on Clinical Ethics and Consultation (ICCEC) 17th Annual Meeting, June 2023, in Rome, Italy. Attendance at this conference was made possible by a grant from the Dean of Graduates Fund, awarded by Pembroke College at the University of Oxford.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.