
Abstract
Rare diseases are characterized by a wide diversity of signs and symptoms and vary not only from disease to disease but also from person to person, and living with a disease leads patients to peculiar experiences, without limits of time and space, as they extend to various environments and relationships of their lives. Therefore, the objective of this study is the theoretical interaction between value co-creation (VC) and the stakeholder theory (ST) with the shared decision-making (SDM) health care theory, to enable the analysis of the relationships between patients and their stakeholders in the co-creation of value for decision-making focused on the patient’s quality of life. It is configured as a multi-paradigmatic proposal by enabling the analysis of multiple perspectives of different stakeholders in health care. Thus, co-created decision-making (CDM) emerges with emphasis on interactivity of the relationships. As previous studies have already highlighted the importance of holistic care, seeing the patient as a whole and not just the body, studies with CDM will be beneficial for analyses that go beyond the clinical office and doctor–patient relationships, extending to all environments and interactions that add value to the patient’s treatment. It was concluded that the essence of this new theory proposed here is neither in patient-centered care nor in patient self-care, but in co-created relationships with and between stakeholders, including non-health care environments that are important to the patient, such as relationships with friends, family, other patients with the same disease, social media, public policies, and the practice of pleasurable activities.
Keywords
Introduction
The objective of this study is to analyze the theoretical interaction between value co-creation (VC) and the stakeholder theory (ST) with the shared decision-making (SDM) health theory, to enable the analysis of the relationships between patients and their stakeholders in the co-creation of value for decision-making focused on the patient’s quality of life. It is configured as a multi-paradigmatic proposal by enabling the analysis of multiple perspectives of different stakeholders in health care.
Studies with SDM in health care have focused on the relationship between the patient and the doctor,1,2 including other health providers and the family in decision-making in clinical and hospital settings.3,4 The contribution of VC and ST theories is to expand these studies beyond health care organizations, identifying other stakeholders that are important to patient health and how these relationships co-create value in decision-making. For that purpose, a detailed narrative analysis of the literature was carried out, based especially on the main authors of the three researched theories, based on their seminal articles, without seeking to exhaust the sources of information. Despite the selection of studies and the interpretation of information were subject to the subjectivity of the authors, an attempt was made to minimize this issue through an extensive bibliographical review.
SDM can be defined as a formal process or tool that helps clinicians and patients work together in the decision-making process about diagnosis, treatment, or follow-up that best reflects medical evidence and the patient’s individual priorities and goals for their care.1,2,4,5 The concept of co-production, also seen in these relationships between physicians and patients, is understood as the participation of the consumer (the patient, as seen in SDM) in operational activities. 6 The advance that is expected with this new proposed theoretical interaction is in the concept of VC itself, which refers to the active participation of the client (in this research, the patient) with relevant stakeholders of the experience network, resulting from interactions that produce solutions perceived as superior those produced by isolated parts. 7 It is not just sharing, but relationships and interactions that promote a co-creation of value between people and groups, interested and interesting, that affect and are affected by the patient’s well-being.
Just as in the marketing literature, initiatives directed to the health area are already found, based on the incorporation of marketing methods and techniques applied to the health organizations sector;8,9 similar initiatives are also identified in the ST literature, such as dialogue between a pharmaceutical industry and patients’ organizations about health education. 10 However, the focus remains on generating wealth and prosperity to health care organizations.
Therefore, a theoretical advance that this study aims to achieve is to understand individuals, in this case patients, as organizations to study the relationships of the patient and his stakeholders, having marketing and strategy as tools to benefit the individual and not the organizations, where the final objective is the welfare of society by improving health care, not wealth and prosperity. In other words, the same concepts created and developed aiming at the survival and growth of organizations, through their relationships with several stakeholders, are proposed here aiming at the survival and improvement of patients’ lives (health organizations’ clients), through their relationships with several stakeholders, among them the organizations themselves, with the patient as the central focus.
This contribution of the administration theories to the health area has become relevant, because diseases such as non-communicable diseases (NCDs), also known as chronic diseases, tend to be of long duration and kill 41 million people each year, equivalent to 74% of all deaths globally. 11 Among the NCDs are rare diseases, which are usually chronic, although not every chronic disease is rare. An evidence-based study produced a conservative estimate for the population prevalence of rare diseases of 3.5%–5.9%, which equates to 263–446 million persons affected globally. 12 The rare diseases are characterized by a wide diversity of signs and symptoms and vary not only from disease to disease but also from person to person. 13 Also, a few rare diseases are preventable or curable; 12 treatment is lifelong, leading the patient to need other health care providers, such as nurses, nutritionists, psychologists, and physical therapists.
Thus, this study may be very relevant, but not restricted, to patients with rare diseases, as they need to interact frequently with physicians and other stakeholders, co-creating value to reduce suffering in facing their illnesses, the side effects of medications, and also to reduce the risk of mortality. But what value can be co-created in the relationships between patients and their stakeholders? Previous studies have already identified as a value, in SDM between doctor and patient, the process of classifying what is important for a patient in a given health decision.14,15 As most rare diseases cannot be prevented or cured 12 and the symptoms can be different even among patients with the same disease, 13 and patient relationships permeate the clinical office and extend to other environments such as family ties, friends, social media, health professionals, the present authors conclude that the value co-created by the patient with his stakeholders is the quality of life, despite the experiences with the disease and the changes it can cause in his life. Therefore, the value that the patient seeks to co-create in their relationships is their quality of life.
The need for interactions, as well as the peculiarities of each patient and their treatments, is one of the main characteristics observed in service marketing, also highlighted in the VC: heterogeneity. In this scenario, the perceived value is subjective, as it not only varies from individual to individual but also within the same individual, in the context of their experiences in space and time.7,16
Therefore, the active participation of the patient in his own treatment is a sine qua non for this study that intends to observe multiple perspectives. On one hand, there is a doctor, a highly skilled professional who has dedicated his studies and career to treat patients of various diseases. On the other hand, there is a patient, with his own characteristics, affected by a disease that has caused a rupture in his life, with symptoms that may be the similar to or different from other patients. In addition to this main relationship of a health treatment, there is the need for bilateral relationships, both the patient and the physician, with other stakeholders and multiple perspectives, such as the patient’s relatives, health organizations, other patients, the pharmaceutical market, consumer law, other health professionals, governments, and public policies.
One of the main points in common between the VC and the SDM theories is the presence of what is represented by the concept of “stakeholder,” understood as any group or individual who can affect or be affected by the achievements and results of an organization.10,17–19 Value is co-created in relationships and interactions with and among stakeholders, and also health decisions are made based on the sharing among stakeholders.
Thus, this introduction is followed by the theoretical framework based on the two theories for which the interaction is intended, the VC and the SDM, along with the ST, which will serve as the basis for this link. Right after that, the result of the interaction is presented: the proposal of the theory of co-created decision-making (CDM).
Theoretical framework
Understanding VC has become a major recent theme in the management literature, particularly in the field of stakeholder research, 20 that intends to understand what happens in the relationships in which they are involved and how to create value with and for them. Organizations are just the vehicles by which stakeholders are engaged in a joint and co-operative enterprise of creating value for each other. 19 Stakeholders generally need to deal with issues that are similar to those of organizations, such as technological innovations, risks, limitations and challenges, and new forms of interactions between them have been explored when engaging in VC. 10
With this multi-perspective view that the VC and the stakeholder theories provide, multiple stakeholders can create value when they converge different perspectives toward the same end.10,19 And that is what this study proposes, with a multi-paradigmatic theoretical construct in the interaction between the VC and the stakeholder theories with SDM. Although the VC and the stakeholder theories are study approaches predominantly from the fields of strategy and marketing of for-profit organizations, their evolution has already been targeted in other non-economic segments.21,22 Therefore, the interaction with a specific health care theory can bring new dimensions to both theories.
Thus, this theoretical reference will address the three theories separately and the interaction between them will be seen in the next topic.
VC
The term co-creation of value began to be used in 2002 by authors Prahalad and Ramaswamy, 7 who disseminated the concept worldwide, causing a major debate on the relationships of companies with their stakeholders, such as customers, suppliers, and partners, adding innovation and value. McColl-Kennedy and others 23 conceptualized the co-creation of customer value as “benefit realized from integration of resources through activities and interactions with collaborators in the customer’s service network.” (p. 375)
Similar to Prahalad and Ramaswamy 7 who discussed the importance of VC a few years earlier, Vargo and Lusch 24 observed the evolution of marketing to a “new dominant logic,” named by them as the service-dominant logic, with emphasis on intangible aspects and the interactivity of relationships. In the intangible aspects, skills, information, and knowledge stand out. As for the interactivity and connectivity of relationships, there is a greater focus on the interactivity between company and customer, and on the experiences generated in this relationship, which may represent value to the customer, including the co-creation of the product/service.24,25
VC incrementally adds value with and for multiple stakeholders through regular and continuous interactions that lead to innovation, increased productivity, and jointly created value outcomes for all parties. 8 Stakeholders’ experiences come from interactions in their environments. 26
The co-creation paradigm is also part of a concept of interactivities that has mobilized scholars to reflect what organizations actually offer to the market and potential clients. 26 For them, it was becoming increasingly clear, both in academia and in practice, that units of production such as “goods and services” did not capture the full dimension of an economic and social exchange; moreover, it was becoming clear that the relationship between companies, customers, and markets was about VC based on a logic dominated by service, not product. And that value was co-created, rather than created by one actor and delivered to another.24,26
This view of the importance of co-production in services with VC within a service-dominated logic has also been seen as important in health care, valuing the integration between physicians, health care providers along with patients and their families.2,27,28 The view that value is not created by one actor and delivered to another, but co-produced among physicians, health care providers, and patients is seen as inherent in the concept of SDM, which is much broader than improving administrative or quality processes that have emerged from a product-dominant logic.27,28
While the concept of value for organizations tends to be linked to profit for their survival, in a systematic review of the value perceived by patients in health care, more than 100 scientific papers were identified that highlighted value as the process of separating that matters to an individual in a given decision-making of his own treatment. 14 To that end, Roque and colleagues identified five categories of what matters to patients and families in health care decision-making: preferences, concerns, life goals or philosophies, treatment-specific values, and broader contextual or sociocultural values. 15
The co-production between physicians and patients is initiated in meetings in clinics and offices, focusing on the respect for the patient’s autonomy, promoting the patient’s engagement, encouraging them to think about the treatment options and the probable benefits and harms of each option.2,3,5 Thus, a logic dominated by service, with the co-creation of values between physicians and patients, emerges as a way to go beyond patient-centered care, which some believed to be the apex of the SDM, but there is “a long journey ahead; there’s more work to be done.” 2 (p. 7)
In accordance with Elwin 2 proposed, this study aims at the conceptual interaction of VC and the service-dominant logic beyond marketing, as a contribution to the health area, integrating them to the SDM theory, not in search of wealth and prosperity for companies/organizations, but aiming at the patient’s health and well-being, through the engagement of the patient and his stakeholders.
SDM
SDM has become a widely used term in health communication. 2 It can be defined as a formal process or tool that helps physicians and patients work together to make decisions about diagnosis, treatment, or follow-up that best reflects the medical evidence and the patient’s individual priorities and goals for his care.2–5 Although the discussion about the importance of physician and patient sharing the medical decision-making has been addressed for some decades, clinical acceptance of the concept is more recent and, currently, stakeholders such as patient representatives, policymakers, hospitals and health insurance companies around the world advocate the principles of SDM as the ideal for decision-making. 4
Analyzing the characteristics and the barriers of the relationship between physicians and patients in adopting SDM in routine clinical practice, Légaré and Witteman 1 described three essential elements of SDM: recognizing and admitting that a decision is necessary; knowing and understanding the best available evidence; and incorporating the patient’s values and preferences into the decision.
Many models of SDM in health care focus on the relationship between the patient and the physician,1,2 because of the importance of this primary relationship between them. However, advances in this patient–doctor relationship are already found in the literature on this topic with the sharing of other stakeholders, such as family members and interprofessional and interdisciplinary groups.3,28
One of the main supporters of the new model is the Society for Medical Decision-Making (SMDM), a non-profit organization founded in 1979, which has among its more than a 1000 members worldwide experts from various fields, including economics, psychology, sociology, education, communication, mathematics, organizational theory, clinical epidemiology, public health, and clinical medicine. 29 SMDM is the leading society for the study and advancement of health decision sciences, including the incorporation of the values and preferences of the patients, promoting health decision research with scientific and methodological rigor, with an analytical, transdisciplinary, and integrated approach to health care decision-making and its application to health policy and clinical care. 29
In addition, the SMDM reproduces on its website, as a definition for medical decision-making, a text extracted from the book “Medical Decision Making: A Physician’s Guide”:
Medical decision science is a field that encompasses several related pursuits. As a normative endeavor, it proposes standards for ideal decision making. As a descriptive endeavor, it seeks to explain how physicians and patients routinely make decisions, and has identified both barriers to, and facilitators of, effective decision making. As a prescriptive endeavor, it seeks to develop tools that can guide physicians, their patients, and health care policymakers to make good decisions in practice.
30
(p. xiii)
Therefore, based on this definition of medical decision-making presented by Schwartz and Bergus 30 and adopted by the SMDM, 29 the effort of physicians and patients to make decisions together is effective, identifying the barriers and facilitators to do so. In other words, the importance of the SDM was already predicted in the very definition of medical decision-making. And it includes, in the prescriptive effort, a new stakeholder in SDM, the health policymakers. Thus, it also predicts that decision-making goes beyond the clinical relationship between the physician and the patient.
The variety of human, technological, and organizational resources are relevant when considering the broad adoption of SDM because “all care team members, not just physicians but also nurses, dietitians, pharmacists, occupational therapists, and others, can help make SDM a reality in all clinical settings.” 1 (p. 281)
ST
ST researchers have adopted the definition of “Stakeholder” as any group or individual who can affect or be affected by the accomplishments and results of an organization.17–19,31 As the initial focus of this theory was on analyzing companies, the main stakeholders for most of them are customers, employees, suppliers, and shareholders, classified as primary stakeholders.19,31 However, there are other stakeholders that need to be considered and vary in importance depending on the nature of the organization, classified as secondary.19,31
Although this basic classification emphasizes the importance of identifying an organization’s stakeholders, the essential problem addressed by the ST is not related to the identification of groups, but to the concept of “relationships” and networks of actors. 17 There is substantial literature on stakeholder management, which focuses on two main questions: who are the stakeholders of a company and what are the interactions between the company and its stakeholders? 10
It is noteworthy that ST has been applied in other types of organizations17,31 and also to other experiences, besides the economic, considering the dynamism of objectives, expectations, and needs of the networks with whom they maintain interfaces, acting in distinct networks simultaneously.32,33
Beyond a theory, the study of relationships with stakeholders form a new paradigm and a strategic vision to achieve mutual value creation in society, here called VC, 10 and seek a view from multiple perspectives. However, one of the problems that stand out in the search for the multiplicity of perspectives, both for the stakeholder paradigm and the VC paradigm, is how some of these can have a “voice” in interactions with organizations.16,18
In addition to mobilization, stakeholders’ collaboration is often mentioned as an important condition for the interaction between stakeholders.10,16 These interactions have gained importance in recent decades, given the speed with which information is propagated and connections are made between individuals and groups. 33 Several practical applications of the ST have been broadening the view of the scope and potential of the theory in understanding organizations and their relationships and interactions with stakeholders, with multi-stakeholder collaborations.10,20,32
Therefore, the inclusion of the ST in this theoretical proposition will not only enrich the debate but also provide the potential and qualities of the theory to be an alternative also for the well-being of chronic disease patients and, consequently, for society. Thus, the next step is to propose the theoretical interaction between VC and SDM, having the ST as an instrument to enable this interaction toward the proposition of a new theory.
CDM
The proposal of this theoretical interaction, which is now called CDM, is to study which and how stakeholders (physicians, health providers, family members and others) influence the decision-making about the patient’s health. Two points emerge initially from this theoretical dialogue, aiming at the co-creation of value in SDM among stakeholders: (a) the engagement of stakeholders in patient-centered care and (b) the patient’s self-care and their engagement in their own treatment and in the practice of pleasurable activities.
Stakeholder engagement in patient-centered care
The very definition of stakeholder17,18,19 brings the two-dimensional idea of affecting and being affected, that is, being interested and interesting. Just as the ST is characterized by a kind of heliocentrism, having an organization at the center of a model that exhibits direct dyadic relationships between the organization and its stakeholders, 17 the proposal of the CDM is to have the patient at the center of a model of studies that analyze their dyadic relationships with the stakeholders engaged in their care. In other words, they are interested and interesting to the patient’s treatment, which is the center of care.
Having the patient at the center also meets what Cyrino 34 highlighted as limitations of biomedicine, which become more evident when faced with the need to learn the complexity of getting sick and living with a chronic disease. And it is in this sense that the focus of studies on CDM is in the relationships that emerge from “living with the disease,” from treatments of a CNCD, for example, which can extend throughout life. The focus of studies on CDM, therefore, is on the patient’s relationships with several stakeholders such as physicians, family members, health providers, professionals of other activities, and friends that will be studied as primary and secondary stakeholders to enable the analysis of these relationships.
Primary stakeholders
Among the primary stakeholders in CDM, those who relate directly to the patient, are the physician(s) and the patient’s family members, already highlighted in previous SDM studies.4,30 Other studies also show that reciprocally shared support among friends and others in the patient’s circle of relationships, in addition to family members, plays a positive role, whether through emotional, instrumental, or counseling support, 34 and, thus, are also considered primary stakeholders.
Primary stakeholders need a special type of attention, being necessary to understand the values and purposes of the relationships and interactions with the central axis, 19 the patient. Therefore, it is possible to identify other important stakeholders for CDM, also already highlighted in the SDM literature, which are health care organizations and other health care professionals, besides the physicians, with the focus on generating value for the patient.1,2,3,23,27 From this perspective, the co-production of learning among the professionals deserves to be observed as a strategy for the co-creation of value with a focus on the generation of health care solutions.2,27,28
Other patients with the same disease also deserve to have their influence analyzed in the CDM due to their experiences with the disease. A great interest has been given to the possibility of those who experience a disease to share this experience with those who suffer the same problem. 34
Going back to marketing concepts, today there is more trust in horizontal relationships than in vertical ones. 35 Consumers believe in each other more than in organizations. The rise of social media is also a reflection of the migration of trust that consumers had in companies to other consumers. When making decisions, they pay more attention to their social circle, seeking advice and evaluations both online and offline. 35 Thus, it is adopted as a premise for the proposition of the CDM that this marketing concept, focused on the shift of power from vertical (exclusive and individual) to horizontal (inclusive and social), also applies to the relationships between patients who interact with each other in search of answers.
The knowledge gained through the experience with an illness takes into account emotional and practical aspects, usually excluded from the medical repertoire. 36 Such knowledge is the driving force behind mutual aid groups, patient associations, and social movements in health.
Secondary stakeholders
In addition to the primary stakeholders, the literature on ST addresses the so-called secondary stakeholders. To understand who these stakeholders are for CDM, other relationships must be considered relevant to patient care. One example is the influence of governments on patient health. The importance of the relationships between physicians, patients, and health policymakers has been predicted in the definition of medical decision-making.26,27 Currently, NCDs have been considered as an invisible epidemic and as an under-appreciated cause of poverty that hinders the economic development of many countries. 11 Governments are therefore “interesting” to the patient but also “interested” in their results, because the better patient’s health is, the lower he will cost to the health system.
Starting from public policies, a new secondary stakeholder emerges: the actors related to Consumer Law, such as lawyers and courts. Many treatments, both public and private, may require the need to go to court to grant access to special treatments and/or high-cost medications.
Because of the medications patients have to use, often for their entire lives, the pharmaceutical market also emerges as another secondary stakeholder. Pharmaceutical companies, health insurance companies, and patients’ organizations have different and sometimes opposing perspectives on what is useful to improve patients’ health. 10 However, the interaction of patients with these stakeholders can result in mutually beneficial advances.
Patient organizations stand out as special interest groups, which are another type of secondary stakeholder. These groups (formal and informal) are also configured by those linked to issues or activities related to the patient’s welfare, regardless of the biomedical area.
As a last consideration in this initial classification of secondary stakeholders in the CDM view, social media has become a major influence in health care. Broad access to the Internet has allowed patients and families to use social media to form a network of mutual support, in which they share information about diseases, about available treatments and new therapeutic options. 37 However, in addition to this mobilization potential, social media can offer a risk. For example, patients can fall victims to treatments not yet scientifically proven or with fraudulent features, clinical trials, or compassionate use of drugs. 37
Therefore, based on the Basic Map of the Stakeholders Theory, 31 a summary is presented below with the stakeholders identified in a preliminary scheme of the CDM, which are distributed in two layers, having the patient in the center, thus formatting the Basic Map of Stakeholders in the CDM, as shown in Figure 1.
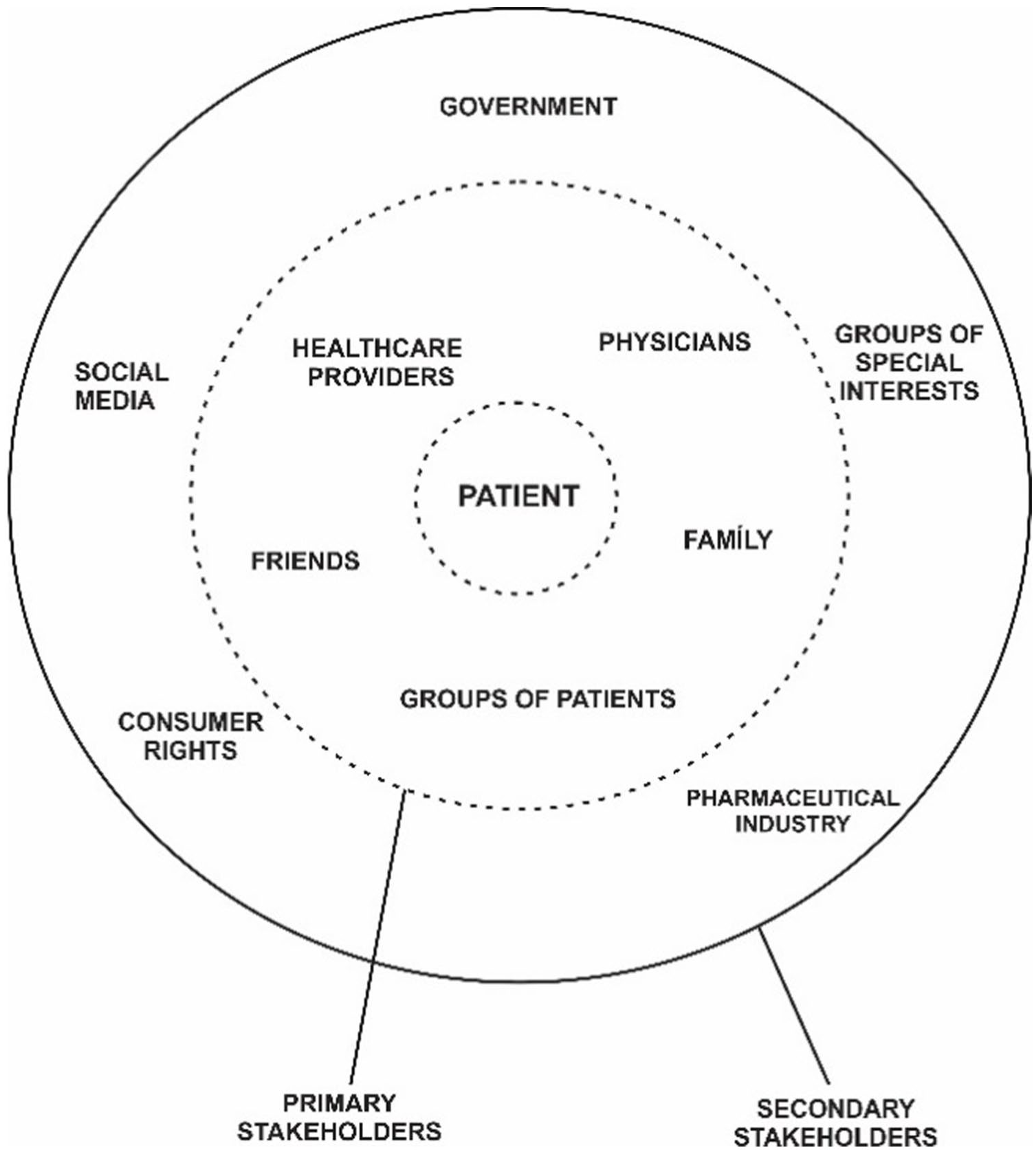
Basic map of stakeholders in CDM.
Figure 1 consolidates a proposal of a basic stakeholder map specific for CDM. The patient is the central axis. The first layer is composed of the primary stakeholders, who interact most with the patient. The second layer contains the secondary stakeholders. It is also noteworthy in Figure 1 that the lines between primary and secondary stakeholders are dotted because they symbolize the semi-permeability between them and that there are no clear boundaries between primary and secondary stakeholders.
Patient self-care and engagement in pleasant activities
CDM argues that the patient, in addition to being the center of care, is (and should increasingly be) an active participant in treatment. This active participation of the patient in his own treatment is what previous studies have called self-care. 34
A study with patients with diabetes, a chronic disease, identified “required competencies” and “effective competencies” for patient self-care. 34 The former are the competencies that health professionals expect patients to develop and the latter regards to the knowledge and skills developed by patients.
In addition to the required and effective competencies, it is also important to emphasize that active patient participation should take a holistic view, targeting not only the body, with traditional treatments based on medical sciences but also the mind and spirit. The practices of holistic medicine help people to develop behaviors, willingness, habits, and practices that provide integral well-being. 38 Previous studies already demonstrate and prove the importance of associating to conventional treatments activities that provide different motivations to patients.39–44
Therefore, as rare diseases vary in symptoms not only from disease to disease but also from person to person affected by the same condition, 6 and how studies with CDM go beyond health care settings and doctor–patient relationships and take a holistic view and propose to study the relationships that are built in the patient’s engagement in the practice of pleasant activities (PPAs), as a complement to the patient’s self-care, and how these relationships and activities influence decision-making for a better quality of life for the patient. PPAs have already been the subject of studies on how they positively influence patients of various diseases in different countries and cultures, such as creative music therapy with elderly patients with delirium and dementia; 39 leisure with chronic kidney disease patients; 43 physical activity practice with chronic obstructive pulmonary disease patients;42,44 benefits of physical activity practice concomitant with medical treatment in cancer patients; 40 and dance therapy for improving the physical and psychological health and quality of life of breast cancer patients. 41
Therefore, studies that will have CDM as a theoretical basis it is suggested evaluate patients’ participation and interactions in PPAs, not only the influence and outcomes of the activity itself on the patient’s health, but mainly the relationships and interactions arising from these practices and how they influence the patient’s health decision-making.
Bilateral relations with and between stakeholders
From these two initial points presented, the central point of interaction between the VC, ST, and SDM theories emerges: bilateral relationships with and between stakeholders. The conceptual basis of CDM is in the relationships that are created and co-created between the patient and the parties interested and interesting for their treatment. The focus of the theory is neither on the patient nor on the disease, but on the bilateral relationships of the patient with his stakeholders as well as between the stakeholders themselves. In patient-centered care, relationships are directed from the stakeholders to the patient; in self-care, from the patient to the stakeholders. The CDM proposal, as outlined in Figure 2, is that studies should be done on bilateral relationships, that is, in both directions (patients/stakeholders/patients) and also on the interactions between stakeholders.
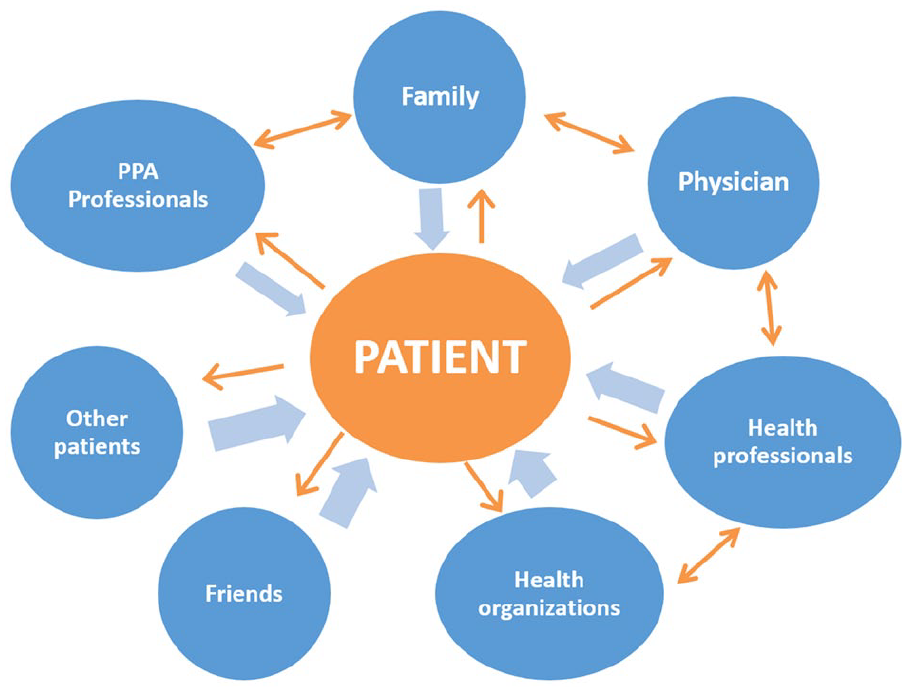
Patient relationships with and between stakeholders.
The right side of Figure 2 shows the interaction also between the stakeholders. These relationships have already been the focus of previous studies on SDM.20,23,25,28 What stands out in the CDM proposal is that, in addition to the relevance of these relationships between the patient and his or her family and health care stakeholders, as well as the relationships between them, there are other important interactions. Although the stakeholders represented on the left side of Figure 2 (friends, other patients with the same disease, and PPA professionals) do not interact among themselves and are not specifically from the health area, they are of great importance for the improvement of the patient’s quality of life and health, in a holistic view of the patient.
Figure 3 shows the theoretical evolution provided by the CDM. Medical decision-making, which used to be done exclusively by the physicians (information), started to be shared with the patients and then also with the patients’ relatives (co-production), as already presented in SDM studies. However, with the theoretical evolution reached in the CDM, by analyzing the interactions themselves, it will be possible to identify how each one of the stakeholders contributes to the patient.
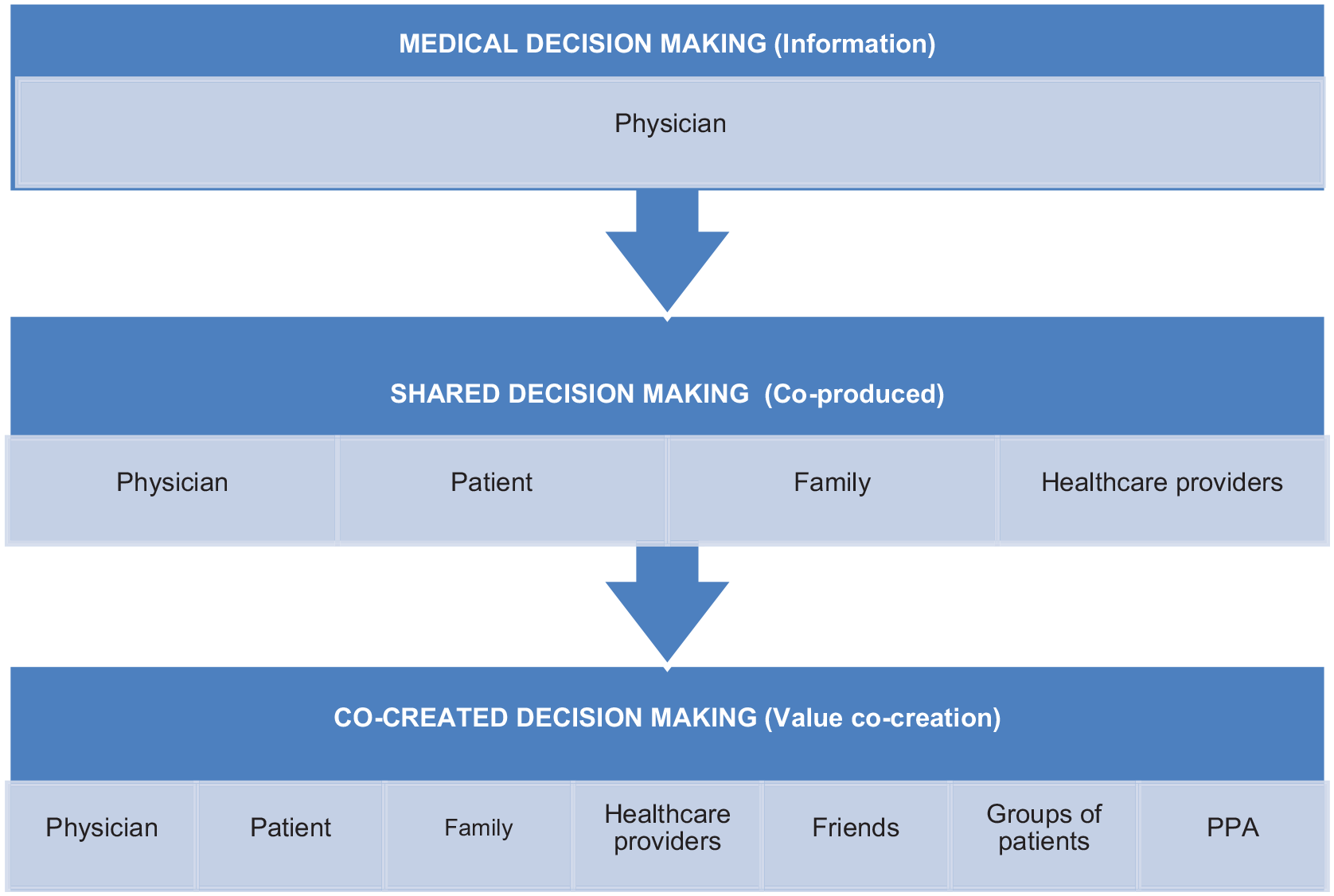
CDM theoretical evolution.
In the theoretical evolution presented in Figure 3, the difference between the co-production observed in the SDM studies and the co-creation of value proposed for the CDM studies is also highlighted. Although there are conceptual similarities between co-production and VC, differences were identified between the concepts of co-production, co-creation, and VC in an analysis of the scientific production on this theme. 6 Co-production is understood as the participation of the consumer (the patient, as seen in SDM) in operational activities, while co-creation refers to the active participation of the client with relevant stakeholders of the experience network, resulting from interactions that produce solutions perceived as superior to those produced by isolated parties.6,7
In the proposal presented here, VC in decision-making happens in the interactions between the patient and his stakeholders. There is neither a “scientific knowledge owner” nor a “life experience owner.” They go beyond the clinical office and the doctor–patient relationships, as studied in SDM,2,4,5 extending to all environments and interactions that add value to the patient’s treatment. It is not just sharing but also relationships and interactions that promote VC among people and groups, interested and interesting, who affect and are affected by the patient’s well-being.
And the value, which previous studies with SDM have already identified as the process of classifying what is important for a patient in a given health decision,14,15 is now perceived in studies with CDM as quality of life of the patient.
Conclusion
CDM emerged from the theoretical interaction of VC and ST with SDM and is defined as a process that emerges from the relationships between the patient and their stakeholders, which go beyond the clinical office and doctor–patient relationships, extending to all environments and interactions that add value to patient treatment. Its focus is on co-creating diagnosis and treatment decisions that best reflect the health conditions, well-being, and specific priorities of each patient.
The central position of the “patient,” as presented in Figure 2, represents that he is the center of care and also takes care of himself in a continuous process of interactivity with all stakeholders. Thus, studies on CDM focus on the relationships that take place between the patient and his stakeholders, as well as among the stakeholders themselves, in practical experiences, aiming to analyze its effectiveness in improving the patient’s well-being, having the patient as an active participant in the whole health/illness/care process.
Rare diseases are characterized by a wide diversity of signs and symptoms and vary not only from disease to disease but also from person to person, and living with a chronic disease leads patients to peculiar experiences and treatments, without limits of time and space, as they extend to several environments and relationships of their lives. This is the importance of value in health care relationships being co-created, rather than created by one actor and delivered to another. It is much broader than improving administrative processes or quality in physicians’ offices, clinics, and hospitals, as it starts with the active participation of the patient in his own treatment and extends to all interested parties in his quality of life.
Therefore, the impact expected with the application of CDM is to enable the analysis of the importance of greater engagement of patients of various diseases in their own treatments, as well as engagement and interactions with various stakeholders, without restricting it to health care environments, and understanding how the co-creation of value in these relationships benefits the patient. And that the dissemination of the results of these analyses can motivate other patients to engage in their own treatments and to co-create relationships with their stakeholders and in decision-making for their quality of life and, as a consequence, provide health and well-being to a significant portion of world society.
For future studies, it is also expected the application of the CDM in studies with patients and groups of patients from several diseases, as well as theoretical contributions for its development. Among the limitations of this study are the lack of practical applications, the absence of tests and analysis models, and the fact that its basis is still purely theoretical.