
Abstract
Imprisoned persons are transported for several purposes including transfers to a different prison, legal-procedural reasons such as court hearings, and to receive medical treatments. The availability and acceptability of transportation may limit access to healthcare if health services cannot be provided within the prison grounds. The aim of this article is to examine the conditions of medical transport for older prisoners in Switzerland and to assess whether or not these practices are in line with international recommendations. Interviews with experts working in the prison context and with older prisoners were conducted. Results show that handcuffing practices and space restrictions during medical transport are not adapted to prisoners’ health condition. Older prisoners risk being exposed and humiliated by transport conditions. The reasons for delayed medical transport can be administrative constraints or erroneous medical judgement. Switzerland’s cantonal system results in a variety of regulations for transports, so that cantonal differences, administrative constraints and inappropriate conditions can delay access to necessary healthcare and increase suffering.
Introduction
Imprisonment is a radical shift in a person’s life. Not only are imprisoned persons isolated in a secured location that is difficult to access, but they are subject to various restrictions. They may be deprived not only of liberty but also of other civic or political rights (Mincke and Lemonne, 2014). Deprivation of liberty means that their movement is restricted to the prison space, except when they are moved from one prison to another prison or place upon orders of the administration. In this article we consider the current conditions for medical transport in Switzerland and the question of how they affect older prisoners, who are generally in worse health than younger inmates (Fazel et al., 2001; Wangmo et al., 2016). In this introduction, we first present the existing literature on carceral mobility, followed by some remarks on medical transportation. Thereafter, we depict the situation in Switzerland, a country where cantons (that is, federal states) have wide-ranging administrative power on transferring prisoners from one location to another. After a brief description of existing supranational recommendations or guidelines on the transport of prisoners, we go on to present the methods and the results of our study.
Carceral mobility
Carceral geography, a relatively recent subdiscipline of human geography, describes an outlook onto the practices and institutions of incarceration. It has become a topic of research since the ‘carceral turn’, that is, the increasing turn to punishment and the effect it has on the criminal justice system, education and public life (De Lissovoy, 2013). This is highlighted by Routley’s observation that carceral geography transcends the architectural, tangible institution and is more than ‘just a fancier name for the geography of prisons’ (Routley, 2016: 105). There is much exchange between carceral geography and related disciplines such as criminology or prison sociology, and the important ‘dialogues between geography and criminology’ (Moran and Schliehe, 2017) are exemplified in a growing body of literature addressing these ‘necessary interdisciplinarities’ (Shantz, 2017: 162).
According to Moran and colleagues, the terms ‘carceral’ and ‘prison’ have become synonymous. However, carceral geography not only looks at the physical and architectural spaces of confinement but goes further and considers broader conceptions such as the embodied spaces of the self (Moran, 2015) or the personalization of prison space (Moran et al., 2012; Milhaud and Moran, 2013). It also looks at institutions that go beyond ‘prison’ in the mainstream sense, for example halfway houses, detention centres for migrants (Turner and Peters, 2018), secure institutions for children and juveniles (Schliehe, 2015) or halfway houses (Allspach, 2010).
Another aspect of carceral geography is the fact that issues of confinement reach into the everyday spaces of the so-called ‘free society’ (Moran et al., 2017) where the non-carceral population comes into contact, albeit unwilling and unintentionally, with the prison population. Many of these occasions are connected with mobility issues. Scholars such as Cresswell (2010) or Merriman (2014) have underlined the importance of movement and laid the groundwork for the field of carceral mobility. Although Moran (2015: 71) noted that coerced mobility has been left underexplored and undertheorized, Mincke (2017) noted an emerging new discourse on prison that is shifting from immobilization and isolation towards certain forms of accepted and desired – or even compulsory – mobility, which constitute the ‘mobilitarian ideology’ (Mincke, 2013).
Medical transportation
When addressing mobility in carceral geography in the Russian Federation, Moran and colleagues (2012) noted the problem of the costs and inconvenience of transport for health reasons. Medical transfers of prisoners have been reported in a limited number of publications, such as Grounds (1991), Mackay and Machin (1998) or Stoller (2003).
Medical transports usually represent only a small fraction of all prisoner transports (other reasons for transport include administrative transfers between different prison settings, transfers at the prisoner’s request, and transfers to balance ethnic groups or sentence type within a prison). For Follis (2015), transports provide points of intersection and interaction possibilities between prisons and the outside. In 2010, Her Majesty’s Prison in Leeds (UK) sent 6777 prisoners to courts, received 9460 prisoners, transferred 1882 prisoners to other prisons and received 480 prisoners from other prisons, and noted 780 hospital escorts for medical treatment and specialized appointments (Follis, 2015). Such movement and mobility during the entire spatio-temporal process of incarceration are important conditions for the functioning of the penitentiary system and are associated with substantial costs for the necessary security services.
Martin and Mitchelson (2009) pointed out that, in the context of medical transports, power relations are evident in the dynamics of who can order a transfer, who decides which situation is important enough to merit a transport, and who informs whom about transport schedules and delays. Furthermore, in the case of older prisoners, power relations may be manifested in institutional thoughtlessness, which Crawley (2005: 16) described in relation to older prisoners as ‘the ways in which prison regimes (routines, rules, time-tables, etcetera) simply “roll on” with little reference to the needs and sensibilities of the old’. The notion of uniform treatment in prisons may lead to older prisoners not being able to take advantage of facilities that may be – in principle – available for them but that they perceive as – de facto – inaccessible. Although steps are being made to introduce special wards for elderly prisoners, such as the ‘60+’ ward in the Swiss prison of Lenzburg, this is the exception.
Stoller (2003) observed that prisoners’ movements through the geographical space of the prison – including extensions to other places (for example, specialized medical practices or hospitals) – are intensively controlled by custody policies and routines. These policies and routines probably consider prisoners to be a homogeneous group, making no distinction based on health or age, economic factors, and spur-of-the-moment decisions. Further, they are mostly geared towards custodial priorities and can create significant delays and obstacles to accessing care. De Souza and Peixoto (2016) noticed that transportation in general was linked to humiliation and mistreatment, long delays, and unsafe means of transport with degrading conditions. Poor conditions associated with transports may lead to prisoners delaying their need for external medical care for as long as possible, or even refusing treatments. Young and Badowski (2017) showed that access to medical care is often hindered by geographical limitations, because many prison facilities are located in rural areas and thus are far from cities with medical professionals. Moreover, Ahalt and colleagues (2013) mentioned that healthcare costs and outcomes may depend on the type of healthcare delivery sites, such as community hospitals vs. specialized prison medical facilities.
Mincke and Lemonne (2014) cautioned against the central position of medical experts such as doctors or psychologists in the context of healthcare, that is, the power that they have in arranging the modes, lengths and places where sentences are served. 1 If healthcare staff are hired by and report to prison health services only, this power is less ambiguous than if they report to the prison or justice administration but are hired by the public health administration. The most transparent solution is a separation of powers so that health personnel are hired by and report to the public health administration and can make decisions on medical grounds alone.
The empirical and ethical questions related to prisoner transportation merit increased academic attention because, to our knowledge, little has been documented on this question. The lack of information and research on the issue of medical transportation could be due to the difficulty of obtaining data on the topic and possibly low interest since transport may be deemed a minor concern considering the overall prison experience. We aim to fill this research gap by showing for the Swiss context who requests, schedules and organizes medical transportation, and the different ways prisoners can be transferred in the country. The experiences of older prisoners themselves and the viewpoint of experts in prison services need to be taken into consideration to see whether transport conditions are satisfactory, or whether some improvements are necessary. Hence, in this article, using a multidisciplinary lens, we consider current transport conditions in Switzerland and the question of how they affect older prisoners, who are generally in worse health than younger inmates (Fazel et al., 2001; Wangmo et al., 2016). The decision to define an ‘older’ prisoner as being aged 50 years or more is in line with the phenomenon of accelerated ageing that research has shown (Loeb and Abudagga, 2006; Loeb, Steffensmeier, and Lawrence, 2008; Merkt et al., 2020). Prisoners who are 50 years old often portray the health status and disease burden of someone living in the community who is 10 to 15 years older (Fazel et al., 2001; Wangmo et al., 2016).
National regulation in Switzerland for prisoner transports
Switzerland consists of 26 federal cantons (that is, states) with a high degree of independence in legal matters, and it is thus similar to other federally organized states such as the United States, Germany or Canada. Although the national penal code is valid for the whole territory, the execution of the sanctions described in the code – including the transport of prisoners – is a matter of cantonal responsibility. The federal organization of Switzerland also results in inter-cantonal and intra-cantonal prisoner transports taking place in different legal settings. The conditions for inter-cantonal transports of prisoners are stipulated in a treaty between the Conference of Cantonal Directors of Justice and Police (KKJPD) and Jail-Train-Street (Schweizerische Eidgenossenschaft, 2000). Intra-cantonal transports are managed and performed by the relevant canton.
The choice of transportation vehicle is dependent on the goal of the transport and an assessment of the individual’s dangerousness. Usually prisoners are transported in groups using road vehicles. For prisoners considered dangerous, escort vehicles may be used, or the prisoner may be asked to sit between police or security staff. Transport can also happen at least partly by train. There is a train line with a special compartment for prisoners (Schneider, 2014). The transport conditions have improved since the European Committee for the Prevention of Torture and Inhuman or Degrading Treatment or Punishment criticized transport conditions in 1996, 2 especially the fact that prisoners were transported in the goods wagon, were not monitored or accompanied by staff between stations, and were not permitted to use the toilets during transport. Conditions improved after an overarching concept was agreed in 2000 between the Department of Police, the KKJPD and a working group composed of Swiss Federal Railways (SBB) and Securitas AG, a private security firm (Altorfer, 2005). The train operates on weekdays along two connections linking Bern to the most important Swiss cities (Zurich – Basel – Bern for the German-speaking regions and Geneva – Lausanne – Fribourg – Bern for the French-speaking regions). From the railway stations, transport continues by other means. The treaty specifies that the working group uses road vehicles, often called ‘fourgons’, that are fitted out with four single cells and one ‘family cell’ and can easily access the train in order to transfer the prisoner between train and road vehicle.
As noted previously, prisoner transports are undertaken for different reasons. Whereas emergencies are usually handled by calling an ambulance, transports for medical appointments – the topic of this article – are often scheduled with prisoner transport vehicles, or more rarely with police cars. Transports between prisons and transports between prison and court are coordinated by the responsible department, which in many cantons would be the police or justice department. Here, it is probably important to consider what is easiest for the institution and best in terms of security aspects.
Supranational guidelines and regulations
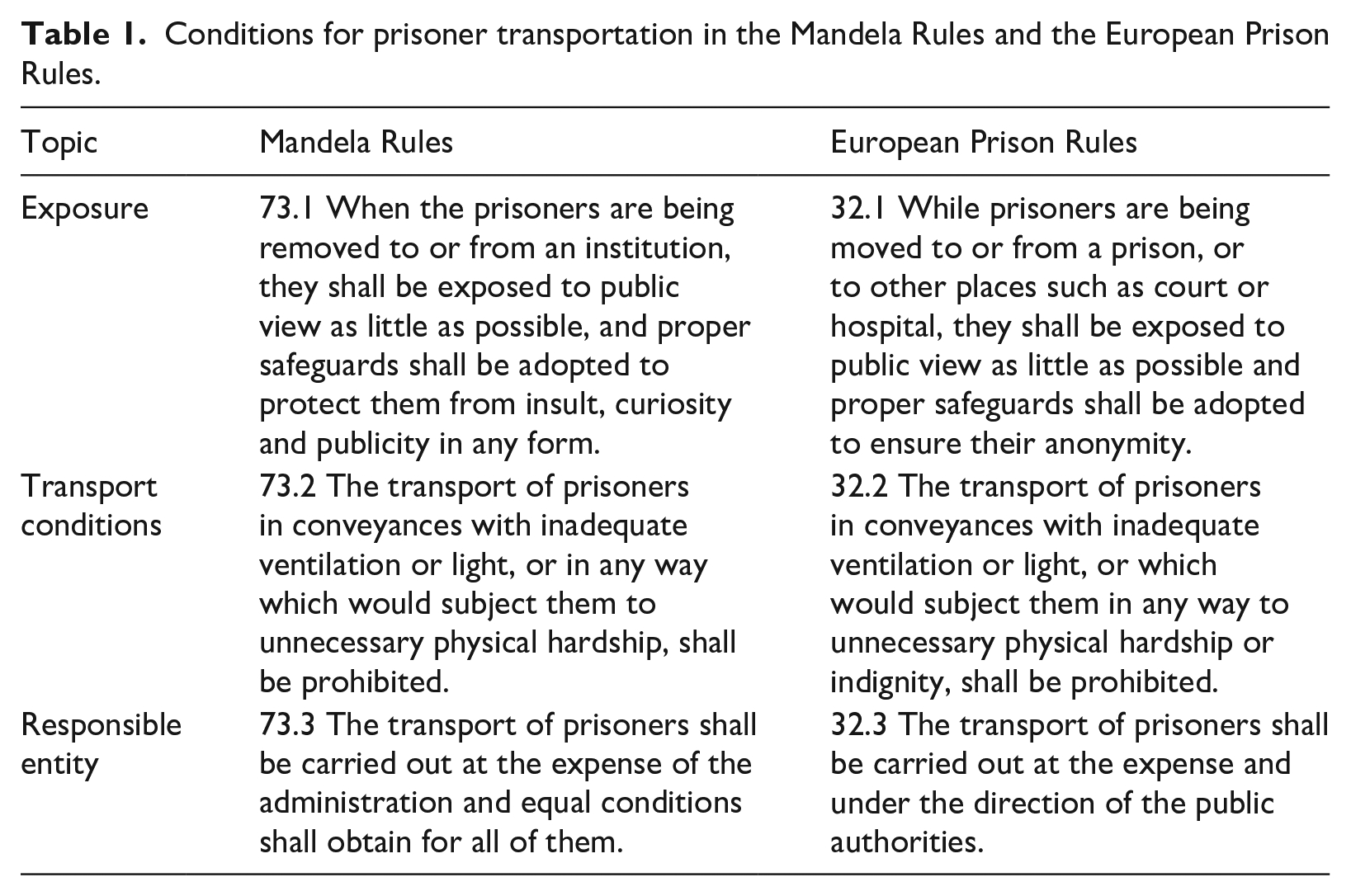
On an international level, the main guiding regulation for the conditions of imprisonment is the revised Standard Minimum Rules for the Treatment of Prisoners adopted unanimously by the UN General Assembly on 17 December 2015 (UN General Assembly, 2016). These rules became known as the Nelson Mandela Rules (hereafter, Mandela Rules) and Rule 73 describes the removal of prisoners.
For the European context, the recommendations of the Council of Europe R(98) state general principles for the ethical and organizational aspects of prison healthcare but – regarding transportation – note in paragraph 9 only that ‘in being escorted to hospital the patient should be accompanied by medical or nursing staff, as required’ (Council of Europe, 1998: 3). Another important document is the European Prison Rules – ‘Recommendation Rec(2006)2’ (Council of Europe, 2006). The European Prison Rules, like the Mandela Rules, are legally non-binding but often used as key principles by international monitoring and inspecting agencies to assess the treatment of prisoners. The European Prison Rules treat the transfer of prisoners in Articles 32.1 to 32.3. Although the two sets of rules differ in several aspects (Huber, 2016), we present their similarities regarding the conditions for prisoner transportation in Table 1.
Conditions for prisoner transportation in the Mandela Rules and the European Prison Rules.
Our study
Material and methods
The nationally funded research project of the University of Basel’s Institute for Biomedical Ethics ‘Agequake in Prisons’ on the health of older prisoners in Switzerland began in 2011 and is still ongoing. Ethics committee approval was obtained in 2011 for the first subproject on somatic health and in 2017 for the second subproject on mental health. Qualitative interviews were carried out with 92 predominantly male persons aged 50 years or older who were detained in prisons and forensic institutions all over Switzerland and participated in the research subprojects Agequake 1 (focusing on somatic health, N = 35) and Agequake 2 (focusing on mental health, N = 57).
This study focuses on older prisoners because the aim of the overall project was to study the health and ageing experiences of older prisoners. Prospective prisoner participants (those 50 years and older) were recruited through the prison health services, who contacted suitable candidates and presented the research project to them. If a prisoner was interested, the prison health services managed the administrative aspects of the interview.
In addition, 54 Swiss experts on prison healthcare and administration were interviewed. Expert participants were recruited through purposive and convenience sampling. On the one hand, study collaborators recommended potential experts. On the other hand, we asked known contact persons within prison healthcare services and prison administrations to participate in the qualitative part of the study or to recommend suitable other prospective participants.
All participants received information about the study via email or over the phone, participated voluntarily and were informed that there were no honoraria or any other incentives. Individual anonymity was assured by presenting all data in a way that would not identify specific participants or prisons.
Interviews were semi-structured and lasted from 30 to 100 minutes. Four researchers involved in the overall project conducted the interviews with prisoners and experts in Switzerland. All interviews were done face-to-face. Permission to record the interviews was obtained from all participants after information about the study aims and procedure had been provided. The interviewer or project assistants transcribed all interview recordings in the original language according to predefined transcription rules.
Transcribed documents were double-checked by independent assistants to ensure the quality of the gathered data, and all identifying information was coded to ensure anonymity. The analysis of the transcribed data involved a number of steps. First, the data were read several times by Sophie Haesen (SH), Helene Merkt (HM) and Tenzin Wangmo (TW) to gain familiarity. Second, the data were coded in the qualitative analysis software MAXQDA 12. After several introductory coding meetings of the whole research team, SH coded the data by specifically searching for sections regarding medical appointments or transport to medical institutions, as well as related words in the original language that were mentioned such as ‘handcuffs’, ‘guards’, ‘bus’, ‘transport’ or ‘ambulance’. Third, TW was included in the process of data analysis to discuss quotes and codes, respectively, that fit the purposes of this article. The draft version of the analysed data was presented to all co-authors and further improvements were made based on their analysis. This article presents the four problems that the authors agreed as being the relevant main themes on this topic. Translations of quotes from French and German to English were carried out by bilingual assistants and researchers in the corresponding two languages and checked for consistency. Where needed, information is added using [ ] to clarify the sense of the quote.
Transportation questions were part of the first study questionnaire and also came up spontaneously and repeatedly during the second research project. This shows that the issue is important not only to prisoners but also to experts and thus merits consideration.
Limitations
The main limitation of our research is that we interviewed only older prisoners and we do not know if younger prisoners would have raised the same topics and voiced the same concerns as older prisoners. Because contacts with older prisoner participants had to be facilitated by prison health services, we depended on prison health professionals to inform prisoners about the research project. Thus, not all older prisoners in all Swiss penal institutions were reached, because prison administrations decided upon participation and also the choice of interviewees. A high workload may have limited willingness to participate. Furthermore, the opinions of the professional stakeholders who agreed to participate may not be representative of all healthcare experts working in a correctional setting. Thus, the findings cannot be generalized to all older prisoners and stakeholders in the country or elsewhere. Also, we looked only at transportation in a medical context and cannot comment on other transport situations such as attending court or being transferred to another penal institution.
Results and discussion
Our findings regarding prisoner transports for health reasons can be grouped into four main categories: (1) the organization of and notification about the transport, (2) older prisoners’ views on transport conditions, (3) the use of handcuffs, and (4) exposure to the public and humiliation. These categories are discussed in detail below and are further teased into sub-themes where necessary.
Organization of and notification about the transport
Decision-making, transport organization and administration
Most interviewees – both stakeholders and prisoners – reported that the decision about the necessity of a transport was taken by the prison healthcare team, usually the doctor. A prisoner described the administrative complexity of this matter: If you get an appointment from the hospital or from the respective institution that needs to treat you, a transport order to the security service is issued, the security service informs the healthcare service, and I am also informed when I have to go to the front, to the security service. (P5, 70 years)
Similarly, two prison doctors (S6, S7) mentioned that transports needed to be scheduled quickly for the most important cases but individuals with less pressing health problems had to wait.
Some stakeholder participants mentioned well-defined procedures for transporting prisoners for health matters. A prison director stated that, in case of emergencies, transport by ambulance was organized quickly by the health team, and the necessary parties for the security escort, such as prison management and police forces, were simultaneously informed. On weekends, when health personnel was not working, the ambulance staff needed to ‘decide whether they have to go to the hospital or not’ (S5, prison director). Another stakeholder mentioned that transport vehicles other than ambulances could be used if the situation allowed it: If someone is really in very, very, very bad shape, then he is taken in by the medical ambulance team. But if we have the feeling that he can still make it to [to the hospital on his own] then it’s the simple, normal transport. . . . I think that we can already estimate whether someone can go with the normal transport or with the ambulance. . . . Nothing ever happened until now, nothing ever happened to me yet. (S4, head of prison health service)
It was not clear by which criteria the decision on whether someone could ‘still make it’ was made and if the patient always agreed with this evaluation. For example, for one prisoner with severe breathing problems the ambulance had been ordered to the building but ‘then it was said, “ah no, she can still walk down to the gate”’ (P 62, 62 years). Yet another expert described the ‘very clear agreement, a very clear structure’ to follow in his institution: For the vast majority of prisoners who are not yet entitled to leave, this is clearly an emergency with a police escort and police supervision in the cantonal hospital, emergency treatment and then immediately transfer to the guarded ward in [hospital in city a]. That is quite obvious. If this is not possible for any reason, the police must ensure that guarding and supervision is fully guaranteed. (S15, prison director)
For the director of another institution, the choice of transportation depended primarily upon the individual case, where the prisoner could be transported by ambulance but could also reach the hospital by public transport if ‘medical permission’ existed (A23, prison director). This shows the broad spectrum of solutions, which may also depend on other factors such as the institution’s security level or the type of sentence. It is possible that, for prisoners nearing the end of their sentence, accessing health institutions for regular appointments is part of the resocialization process.
Cantonal and institutional differences
This sub-theme was highlighted only by the stakeholder participants. Several prison health experts mentioned the cantonal variation in rules and regulations that results from Switzerland’s federal–state organization leaving the execution of sanctions to the canton. For example, one expert reflected upon the specific situation in Switzerland: That’s the tiresome story in every canton, how do we transport them? You would really have to settle that, you would have to come up with an instruction with the cantonal doctor and with the police. Then one would have to decide if the prisoner can be transferred using a normal vehicle and a doctor has to decide that. And if there is no doctor on site, the prisoner must be transported by ambulance, and . . . a civil servant, a police officer in an ambulance and the patrol must follow the car. There has to be . . . an institutional protocol with the emergency services; if you establish this clearly, it doesn’t cause big problems . . ., it should also be regulated that inmates can also go to the dentist or have a routine check-up with a specialist. (S22, prison administration expert)
Some experts were not at all sure who organized transportation in their canton once they had declared the need for transport. Others knew that, depending on the cantonal rules, they needed to turn to the penitentiary administration for approval, or the decision had to be jointly made by the doctor and the security services of the canton or of the institution. One health professional underlined the responsibility of prison staff: if a prisoner did not speak up about a specific health problem himself, the team alerted the medical doctor, who then organized the transport and admission to a hospital (S39, head of supported housing).
Even between institutions, there was considerable variation in resources and the management of detainees with chronic illnesses needing regular transport, for example for dialysis. For some, this did not pose any problems. One expert commented, ‘if someone’s sick, and if someone needs it, then he needs it’ (S4, head of prison health services), and another noted that transporting a prisoner to the dialysis centre twice per week was ‘an effort’ but not problematic (S1, prison director). Others stated that, for a similar situation, the transport and police escort could be organized but it was ‘a huge problem’ (S26, head of prison services). In other cases, regular transport to dialysis was refused by other actors in the administration even though the prison itself had been open to this: We have had cases where we asked the question if we could do this. . . . It’s possible to take him there two or three times per week, and then I was told that this didn’t make sense. (S23, prison director)
In other institutions, it was considered downright impossible: ‘No, that is impossible. We have just asked for one recently – but we are not able during many hours, three times per week, it’s impossible to have the staff for this, it’s impossible’ (S15, prison director). This illustrates very different reactions to the same medical condition and need for treatment.
The high level of independence of cantons in Switzerland can lead to geographical and administrative differences in the execution of sentences, including the way in which medical transports are decided and organized. Access to healthcare is further influenced by ‘spatial injustice’, which means that, the more peripherally a prison is situated, the more difficult it can be to access health services, as described, for example, by Young and Badowski (2017) for the US context. Different healthcare delivery sites may also lead to different healthcare costs and outcomes, as mentioned by Ahalt and colleagues (2013). A possible solution could be to assign one penal institution to a peripheral hospital and clearly define procedures, so that access is not that complicated, or to create regional or national prison hospitals big enough to take in acute and chronic cases from all over Switzerland, similar to the French ‘interregional secure hospital units’ (unités hospitalières sécurisées interrégionales 3 ) or the Dutch ‘judicial centres for somatic care’ (Justitieel Centrum voor Somatische Zorg 4 ).
Problems with transport organization
This sub-theme was mentioned only by prisoner participants, possibly because there was no direct exchange between prisoners and experts on this issue. Sometimes the transport to a medical institution took place only after several days of discomfort or pain, when the healthcare professional in charge was convinced that the situation was serious enough to merit a transport: Finally I could then go down to [city y] to have a stress ECG. And then after that, they did that here and they said, well, we don’t notice anything. But then the heart specialist was called in anyway, and she immediately put me up as an emergency. (P40, 63 years)
The same prisoner had had a similar experience in another prison where he had spent three days in his cell with ‘severe pain, finally I was transferred to the hospital. Well, I had pancreatitis’ (P40, 63 years).
Prisoners saw this as a general problem of prison health services because they felt that some doctors were not diligent enough in their diagnoses or made different diagnoses. A number of prisoners complained about long waiting times that they felt were unjustified: ‘maybe they’ve made an appointment, I’m still waiting – well, to go for a scan or something. But well, I’m waiting, I’m waiting. I’ve been waiting almost a month. [Imitates healthcare staff] “Yeah, but it’s coming, it’s coming”’ (P26, 56 years). In some cases where this wait was too long, prisoners stated that external physicians criticized this practice and noted that there could have been serious consequences: I haven’t been able to breathe through my nose. After a year . . . I was able to go to a specialist and he said, operate immediately, and the [prison] doctor decided that September would be early enough . . . I couldn’t breathe any more, everything was blocked. An inmate who had found me took me upstairs. And afterwards they gave me oxygen upstairs, afterwards he [someone from the prison healthcare team] said: ‘Would you like to go to the hospital? Or what do we want to do now?’ And I said ‘Please, please, to the hospital.’ I thought I was going to die. (P 62, 62 years)
Here we need to point out that we did not talk about specific cases with the health professionals or other experts from the same prison and can state only that the latter groups did not spontaneously mention organizational problems.
Some prisoners stated that they had to insist in order to be transported to external health facilities and assumed that things were easier if the hospital called and asked for a prisoner to be transported there: I think it’s more like the hospital calling, from what I understand. They follow up, and then they say ‘we’d like you on such and such a date’, that’s it. And then they arrange the transport, you see. (P23, 60 years).
Prisoners also complained that usually they were notified very late about transport to the hospital, sometimes only a couple of hours before, although the appointment itself might have been scheduled a long time ahead, as is often the case with controlled visits in hospitals. Depending on the purpose of the medical intervention, this proved to be counterproductive, for example when a prisoner needed to have an empty stomach but had already had breakfast because he had not been informed in time.
In principle, we shouldn’t know when we are going to the hospital. In fact, sometimes we receive our appointment from the hospital directly in the cell. They say ‘you will come in May’ . . . Then they change the date. Because there are always risks of escape, you understand, you have time to prepare an escape. There was a time when we were told nothing, we knew nothing. At a quarter to six you are woken up and told that you have to go to the hospital on an empty stomach. But often, at a quarter to six I’ve already had my coffee . . . As it turned out, the doctors said that something had to be done. So now we’re notified the day before. (P23, 60 years)
In light of the problems associated with medical transportation, such as waiting times, uncertainly about the appointment, and other concerns, a few participants raised their anxieties related to seeking such access to care. They found the entire process cumbersome and, in some ways, not worth the trouble.
After that . . . there are also cancellations of extractions for many reasons. There are also care services that normally have to accommodate . . . the detained person, who for reasons that are sometimes medical service reasons cannot be there on time, because they have something else to do. (P34, prison psychiatrist) On the way back I had to go on the rail transport . . . [Y]ou are locked into the waiting cell in [hospital] and then wait there for about two hours. Then the transport car leaves for the office building in [city X]. Then they wait there for three, four hours depending on the time. Then you will be taken to the loading station in [city X]. There you wait at least . . . another one and a half, two hours. Then the whole transport happens by train, inside the prisoner transport wagon, where you are locked up in a small compartment. You can’t even stretch your legs properly . . . because everything is so constricted. You can’t even stand up properly, nothing. Then this takes at least two hours by train, because the train has to avoid all other trains. . . . It took six and a half hours on the way back . . . Makes you wonder about going to hospital at all. (P29, 58 years)
Another prisoner had become reluctant to access essential healthcare services because of these obstacles, saying, ‘I don’t like going out for an appointment at all. I avoid where it is possible. Although I actually should go to a specialist, yes’ (P40, 63 years).
According to international soft law, the necessity for a medical transport must be asserted by a member of the medical staff, the prisoner’s health needs being ‘the primary concern of the doctor’ (COE, 1998). Our results indicate that such decisions can clash with administrative restrictions, as shown for transports to dialysis facilities and by the lack of alternatives to ambulances or compartmentalized vans for elderly and fragile patients. It is evident from our results that older prisoners often felt neglected or not taken seriously when stating health problems, complained about delays that they felt were unjustified, and voiced resentment and resignation. Main reasons for the underlying lack of communication were based on security issues and could have negative consequences, such as not getting a necessary examination in a timely manner because the prisoner was not informed early enough about the medical appointment, and the subsequent cost of such a cancelled appointment. We assume that this could be improved by creating clearer communication channels, by limiting the discretionary power of single prison administrations, and by developing binding guidelines at a cantonal or federal level that are in line with international guidelines and regulations. Regarding this point, we see that not all aspects of either the Mandela Rules or the European Prisoner Rules are respected in the context of transporting older prisoners in Switzerland.
Older prisoners’ views on transport conditions
Space restrictions
Although the distance between the prison and the healthcare institution is often not far (assuming that complex cases are taken to the nearest university hospital, this distance varied between 10 and 35 km), transportation sometimes took many hours owing to additional pickups on the way. In rare cases, relay stations had to be visited where the prisoner needed to spend the night. One prisoner described how picking up other prisoners on the way at various prisons considerably prolonged the time he had to spend handcuffed in the ‘fourgon’ compartment: he was ‘picked up at 6:30 downstairs, it’s around 10:00, 10:15 that we get to where I have to go’ (P28, 63 years).
The most frequent modes of transport for hospital visits were the fourgon, followed by ‘special transportation’ car and ambulance car. Many prisoners complained about the restricted space in the fourgon: You see, in about a month, I am supposed to go down to [hospital in city Y] for a cardiac examination and so on. But I dread that. Because I’m going to be in the van, the cell van. . . . We have about 65 cm wide by about 90 cm deep by 1.20 metres high. . . . Last time, two or three months ago, I had to go . . . – it’s really the ghost train. (P28, 63 years)
Several older prisoners felt that the transport conditions were designed for younger, physically active prisoners but were excessive and humiliating for older people who were no longer in good physical shape.
There can be a van for those who are known to be violent because they have already been in fights, because they have had problems and so on. And then if they’re young, okay. But for us, that’s what we’re talking about here, for those who are over 50 years old, who are a little bit – not obese but at least a bit fat to drive them around all morning and back and forth in this – I don’t see what it’s for. There’s no justification. It was just someone in an office who said, ‘Yeah, that’s how we’re going to do it.’ (P28, 63 years)
Another prisoner reported having complained about these conditions at the European Court of Human Rights in Strasbourg, stating that, ‘if I transported a cattle like that, any animal, then the animal welfare society would come and say, hey, not like that. But since we are neither animals nor human beings, these regulations do not apply’ (P35, 67 years).
The need for advocates
Both participant groups noted the need for advocates to improve the transport conditions. One health professional said that, ‘if the prisoner did not speak up about a specific health problem himself, the team alerted the medical doctor, who then organized the transport and the admission to a hospital’ (S39, head of supported housing). Prisoners reported that protesting usually did not help but that finding allies or advocates among the health staff could help them obtain more appropriate transportation. For example, one prisoner stated that the fourgon’s transport cages had no safety belt and that he felt afraid of accidents and at the driver’s mercy, without any possibility of protection. This prisoner managed to obtain a ‘special transport’ by road vehicle, because an accompanying staff member had noticed that entering and exiting the fourgon vehicle was difficult for the prisoner, and said ‘we have special vehicles, so you should get one’ (P59, 62 years).
Another interviewee commented: [Using a special vehicle] would be feasible, right, but if we apply in here for a special transport vehicle, then they say: ‘Yes, that’s not possible.’ So first somebody has to see that things are really bad. Or that you have some handicaps, for example that you can’t be tied up or anything else. Then it works from the start. But otherwise? No. (P30, 67 years)
Transport conditions could improve if medical services insisted upon a specific type of transport. A health professional described that the default mode for medical transport was the ‘cage’ in the back of the transport vehicle. When he asked for a prisoner who had been hospitalized to be transported in the front part of the van, this request was granted without problems (S4, head of prison health services).
One prisoner mentioned that, after having collapsed from severe breathing problems, the prison health services had requested an urgent ambulance transport to the hospital. However, the requested ambulance vehicle was not allowed to drive up to the building but had to wait at the perimeter. This meant that the prisoner had to walk from the prison building to the gate, which increased his discomfort and suffering. Moreover, ‘the hospital doctor said that I should already have come there two weeks earlier’ (P62, 62 years). The same prisoner had had knee surgery and asked to be allowed more time on leave days to walk down to the village bus stop in order to catch the bus, but he was told, ‘even if you had a walker you would have to respect the rules, there are no special favours’ (P62, 62 years). Medical decisions could thus be in conflict with administrative procedures that seemed to take priority.
Transports by train and fourgon were experienced by older prisoners as an additional cause of suffering, because they were supposed to comply with the transportation conditions irrespective of their health status. This is a good example of ‘institutional thoughtlessness’, where prison regimes do not take into account individual prisoners’ situations but tend to treat everybody in the same way (Crawley, 2005). It sometimes took the advocacy of an observant person noticing a problem – like a staff member saying ‘we have special vehicles exactly for these cases’ – but if such a person was not there, the institutional insensitivity was not counterbalanced. Considering that both the Mandela Rules and the European Prison Rules state that unnecessary hardships must be avoided, we propose that medically oriented conditions for and decisions about medical transports need to be established and widely publicized either for every individual penitentiary institution or at a cantonal, concordat or national level, instead of depending on random factors such as the presence or absence of a well-meaning individual. Prison healthcare professionals can play an important part in these matters.
The use of handcuffs
Interviewees reported that they had to wear handcuffs, ankle cuffs or other means of movement control, such as anklets equipped with GPS for electronic surveillance,
5
before entering the van/car, during the ride, after exiting the vehicle, while being transported in hospital, sitting in a wheelchair, and prisoners felt that their use was excessive. Many older prisoners criticized this practice and described their poor state of health due to age and illnesses: ‘What do you think, I could run away being overweight and out of breath?’ (P40, 63 years). For some prisoners who had on other occasions been allowed to take leave for several hours or even days, the unequivocal use of handcuffs was perceived as a ‘lack of trust’ (P38, 51 years). Prisoners who suffered from conditions reducing their mobility, such as a ‘bad leg’, felt ridiculed: It’s horrible. And always with the cuffs on, and all that. Like we were some . . . we were going to for example I have . . . I’m not going to take off running especially since I had a leg like that! You see, I found it ridiculous. (P 67, 74 years)
The use of handcuffs was felt by some prisoners to reduce them to the status of cattle, which seems to be a recurring theme in recent literature (see Hanna, 2016; Morin, 2015, 2016; Sim, 1991; or Struthers Montford, 2016). This feeling resulted in some of them not wanting to go to important medical appointments at all, which were sometimes seen as a necessary evil: [S]ome of them [authors’ note: younger prisoners] here are very happy . . . not to have to work for one day and all that. But it would make me mad. That’s something that I hate, I’d rather work an entire day than go to the hospital. So that would be my – let’s say my fear, I don’t think about it otherwise. (P67, 74 years)
We can only hypothesize why none of the stakeholders mentioned this issue. It is possible that the use of mobility controls is so normalized for prison professionals, even in the health sector, that mentioning them in relation to transportation seems redundant. Another reason might be that prisoners refrained from sharing their perceptions and feelings with professionals.
Older prisoners complained about the excessive use of handcuffing and mentioned differences in severity between state officers and members of private security companies. They felt that handcuffing happened not based on their dangerousness but out of routine, which leads back to the ‘institutional thoughtlessness’ linked to the traditional prison principle that elderly men are subjected ‘to regimes designed for much younger, fitter men’ (Crawley, 2005: 2). However, Crawley (2005) points out in detail that treating everyone the same may serve as a survival technique for prison officers but cannot be equated with fairness. Prisoners cited their respective illnesses or reduced mobility as an obvious contradiction to the appropriateness of these security-based routines and fears, which appeared to them as overrated. Furthermore, they noted that being cuffed led to their prisoner status being unnecessarily visible to members of the general public, which can be seen as a kind of humiliation.
Exposure to the public and humiliation
Sometimes, after being transported to the hospital, prisoners had to wait together with other patients. They complained about having to wear prison clothes and sitting in a wheelchair handcuffed, because they felt exposed and presented as someone who deserves to be singled out – ‘people should just see what kind of person you are’ (P59, 62 years). Another prisoner described the circumstances of his entry to hospital: There were at least a hundred people because, in this hospital, the corridors are the waiting room. Everywhere there are people waiting. There I was, without glasses, without lenses, without anything, I saw a lot of people from this region where people may know me a little. I have no idea who I saw, but I know that, because we are human, all those people who saw me said ‘Ah, he must be a horrible criminal, he’s tied up, two policemen. . .’ (P28. 63 years)
It is easy to imagine how the deprivation of visual aids can lead to an experience of loss of control, vulnerability and humiliation. Not unlike older prisoner participants, one prison director underlined the undignified situation that cuffed prisoners could experience when seeking care at a hospital. Changes in the admission procedures were possible but apparently depended on the institution or canton: ‘So that has changed now. I don’t know about the other cantons’ (S23, prison director).
Some prisoners resented accessing a hospital through the basement, where the prisoners were put in wheelchairs and wheeled through the corridors, which could make them feel uneasy and helpless, especially when their mobility was further limited by cuffs: You always go through . . . the entire basement, but it’s very big, very long. So they put us in wheelchairs. And then I sometimes saw people coming, I said: ‘But I hope she can steer’. Yeah with the cuffs on and all you feel powerless. You feel diminished anyway. (P 67, 74 years)
Humiliation was also felt through being ignored: You can tell the doctors and the staff of [hospital X] all this: when we go, we are with guards, and the doctors . . . they talk to the guards, they don’t talk to us. It’s like being a child, and them talking to the mother. Because we’re in prison. (P1, 56 years)
The way this situation is described, it is perceived by the prisoner as an infantilizing diminution. It is unclear whether the healthcare professionals did not notice the unequal exchange or they preferred to communicate with associates they perceived as professionals. Although prisoners in Switzerland are not deprived of their civil rights, as in the US, they may well feel deprived of the feeling of being a citizen, or even being an adult who can speak for themselves and can be addressed directly.
The topic of transportation does not just involve the transport itself but is also tied to the surrounding circumstances. Prisoners resented the fact that their status of being deprived of liberty was obvious, for example when they were wearing prison clothes, were handcuffed or accompanied by security staff, and they perceived this exposure as discriminatory and humiliating. Here, too, the Mandela Rules and European Prison Rules prohibit any unnecessary physical hardship and exposure to situations that could result in humiliations. This should lead to well-documented individual decisions on the use of restraining devices so that decision-makers are aware of the importance and consequences of their decisions. Just as prisoners wear ‘normal’ clothes when on leave, it should be possible to avoid prison clothing that may be ‘obvious’ to local residents who may work in prison themselves.
For all these reasons, access to healthcare outside the prison that required transport was difficult for prisoners because they felt that they had to unduly justify and insist on their need to see an external healthcare service. Sometimes their complaints were not taken seriously, treatment was delayed or did not happen, and prisoners found themselves in an unequal power situation with few possibilities to voice a different opinion or to access the desired service, as would typically be the case in free society. This constitutes a first-order obstacle to healthcare access. Interviewees suffered not only from the somatic problem but also from powerlessness and invisibility. Feelings of frustration sometimes provoked a loathing of procedures and an unwillingness to go through these procedures again, which constitutes a second-order obstacle to healthcare access.
Humans are inherently vulnerable (Hoffmaster, 2006; Rendtorff, 2002), and heightened awareness of this vulnerability led to the recognition of universal human rights (Masferrer and Garcia-Sanchez, 2016). Human rights, in turn, influenced the development of the principle of equivalence of care (Lines, 2006). This principle means that health services in prison should be of the same standard and quality as those for patients in the community (Niveau, 2007; United Nations, 1982). In both contexts, older people may constitute a specifically vulnerable population (Harris et al., 2006; Waisel, 2013), and imprisonment adds an additional layer of vulnerability and powerlessness (Luna, 2009). Similar feelings of powerlessness when confronted with hierarchy and subsequent frustration may also arise for older people in free society who are living in institutions such as hospitals or nursing homes that might qualify as ‘total’ owing to their barriers to social interaction with the outside, following Goffman’s definition (Goffman, 1957). The difference from a prison is that contacting family members, friends or other advocates such as lawyers or the media, and the ability of these people to access the institution, is less difficult than in a prison context, where access is extremely limited and controlled.
The mobile prison
When a prisoner on leave gets out of the prison building, he is not ‘free’. A variety of disciplinary measures keep reminding him that he is part of the carceral universe, even if these measures may not be externally visible, or at least not immediately (such as an electronic ankle cuff).
Disciplinary measures concerning the limitation of time and space start even before the actual medical visit. The appointment is fixed by prison staff, who communicate with the health services, and the prisoner is kept in the dark about the time and date until shortly before the transport starts. Disciplinary measures during the transport and in the health facility mentioned by prisoners were transportation in a car with limited space that can be recognized as a prison vehicle, being accompanied by police or security personnel, using a separate entrance, being transported in a wheelchair while wearing handcuffs or ankle cuffs, having to wear prison clothing, and communicating through a third person instead of talking to medical personnel directly. In this way, the social and spatial boundaries of prison mentioned by Mincke (2017) remain intact even while the prisoner is moving in a space that is accessible to the general public.
Conclusions
Medical transportation of prisoners is an aspect of carceral mobility that is not regularly covered in the literature. In a theoretical context, an important question is how the ‘mobile’ prison accompanies a prisoner by means of disciplinary measures even if he is brought into a setting that is open to the general public, such as a hospital or a specialized medical clinic.
Our study is novel because questions around medical transportation either for older prisoners or for prisoners in general have not been researched for the Swiss context. Thus the findings are important, first on a policy level because they illustrate the practical consequences of structural problems for this prisoner group. We studied medical transports and found that the principle of equivalence of care (Harris et al., 2006; Niveau, 2007; United Nations, 1982; Waisel, 2013) is not upheld. Thus, there is a need to apply this principle in the case of medical transports too, in addition to the general provision of medical treatments. The problems that older prisoners encounter regarding medical transports exemplify the questionable attitude of correctional facilities of applying the same principles to different groups, which leads to more inequality and can have harmful consequences for individual prisoners. Practical solutions for the concrete problems mentioned need to be found. It might be a good first step to look at possibly problematic cases involving transportation from one of the bigger Swiss prisons housing older prisoners, and establish together with prisoners and healthcare staff which problems arose and how they might be avoided in the future.
Local pilot projects using teleconsultations have started in Switzerland, and this might reduce the need for medical transport to access specialists. Other practical improvements could include proposals such as streamlining and clearly defining procedures at a concordat or nationwide level, and increasing transparency by documenting decisions regarding prisoner transport. The question of whether a central prison hospital, or one for each concordat, might solve some of these issues deserves to be discussed. The ‘medical surveillance ward’ (‘Bewachungsstation’ in German) in Bern may have been devised with such a goal in mind but it does not have sufficient beds and resources to care for more than a few acute cases overnight; there are 16 beds, 13 of which are occupied on average (Amt für Justizvollzug, 2018, 2019). To avoid dual loyalty, such an institution should be placed under a health jurisdiction, not justice(see UNODC/WHO, 2013). Furthermore, its status and administrative responsibilities and regulations on who decides on what must be well defined within the Swiss federal context. It would also be necessary to establish mobility patterns for older and younger prisoners to identify details about the frequency of and in-depth information on medical transports to better understand the dynamics and limitations of the system. This is outside the framework of our research project. We hope that this will at some point be included in a broader research project on drivers of health in detention.
Although our research was focused on older prisoners, we assume that our results might be applicable to all prisoners, younger and older alike, because the suffering that is often related to medical transports does not depend on age. Further research on this topic is necessary not only by means of interviews, but maybe by establishing a specific register of correctional health issues, including transportation and other surrounding factors. Because data on prison healthcare are scarce not only nationwide but also for the various Swiss cantons, this step could improve our knowledge about the situation. With information available, data could be appropriately interpreted, and experts from different fields – such as medicine, ethics, criminology and economics – could devise a truly interdisciplinary approach that would also guide possible interventions.
Our research complements the interdisciplinary academic work that has been done on this topic and we hope to spark a new debate about medical transportation within the framework of carceral mobility. The paucity of literature on the specific issue of medical transportation, especially in a non-American context, is striking, and we have hypothesized above some of the reasons. Given the lack of alternatives to imprisonment and a very limited number of prison hospitals able to care for prisoners, the increase in a prison population that suffers from chronic illness or is approaching the end of life justifies delving into this issue. A truly interdisciplinary approach using criminological, sociological and geographical lenses needs to be constructed in order to develop a solid scientific foundation. To our knowledge, there is no analytical framework for identifying regional and global overarching factors that influence infrastructure and decision-making by professionals as well as the motivations of detained individuals to use external health infrastructures or not. Research around these issues could advance our knowledge and is needed to help address this growing challenge.