
Abstract
Background:
Advances in paediatric care have contributed to an increasing survival of children with complex heart disease. Yet, life-saving management demands prolonged inpatient admissions, which contribute to emotional and psychological distress for parents and other caregivers in a role of main custody.
Aim:
The purpose of this study was to identify, appraise and synthesise qualitative studies exploring caregivers’ experiences of paediatric inpatient cardiac services, generating an understanding of their needs in hospital and informing priorities for change in healthcare delivery.
Methods:
Searches were conducted in Medline, Allied and Complimentary Medicine Database, Cumulative Index of Nursing and Allied Health Literature, EMCARE, Scopus, PsychINFO, Proquest, OpenGrey and ETHOs from 2008–2019, reflecting recent advances in cardiac healthcare. Articles were selected using predetermined eligibility criteria dictating qualitative inquiry into caregiver perspectives whilst their child received hospital-based interventions for heart disease. All eligible studies underwent quality appraisal. Framework synthesis was used to analyse and summarise findings.
Results:
Twenty-seven studies involving 689 caregivers from 11 countries were included. Three overarching themes were identified: ‘emotional capacity to care’, ‘practicalities of caring’, and ‘the bigger picture of caring’.
Conclusions:
Through analysis and summary of qualitative primary research, this review captures the emotional challenges that caregivers face and practicalities of undertaking a caregiver role, whilst looking after their child with heart disease in hospital. The results widen the context of the caregiver role, encompassing the whole family unit beyond the hospital environment. This review exposes the impact of these challenges on caregiver competence, wellbeing and attachment to their unwell child, informing priorities for development of family-centred paediatric inpatient cardiac services.
Introduction
Congenital heart disease (CHD) is the most common birth defect, affecting up to nine out of every 1000 births each year, with an additional 500–1000 children affected by acquired heart disease (AHD) in the United Kingdom (UK) annually. 1 The population and complexity of heart disease is increasing with rising birth rates and improved survival due to advancing healthcare technology and expertise.2,3 This has transformed childhood heart disease from a palliative or terminal illness to a chronic life-long condition. 4
However, the life-sustaining interventions necessary to manage complex heart disease have resulted in recurrent hospital admissions, recording 19,221 inpatient episodes for CHD in children (aged 0–14 years) within the UK in 2011/2012. 1 Furthermore, admissions are prolonged, particularly in younger children and those requiring complex cardiac surgery and/or use of machinery in advanced heart failure.5–7 This increasingly common scenario requires children and their families to continue their lives in hospital, focusing attention on their inpatient experiences.
Hospital admissions have been associated with increased risk of mental health morbidity in caregivers of children with heart disease. A systematic review of 30 studies revealed elevated symptoms of trauma (>80%), depression and/or anxiety (25–50%) and psychological distress (30–80%) compared to norm reference groups. 8 Reporting of symptoms was elevated in mothers, during the period following cardiac surgery and positively correlated with diagnosis severity, concurring with previous studies.9,10 However, these findings were derived from quantitative data, which lacked an in-depth understanding of this distressing period.
National Health Service England emphasises the importance of service-user insight to develop quality healthcare, demonstrating a positive association between their experiences and outcomes of clinical effectiveness and patient safety. 11 This has redirected attention to qualitative research, prompting two recent systematic reviews that explore the experiences of parents looking after a child with heart disease.12,13 Although both reviews contributed partial understanding of caregiver inpatient experiences, Lumsden et al. 12 encompassed narratives across a broader context, failing to highlight unique challenges in hospital, whilst McMahon et al. 13 focused on hospital experiences in the first year of life, excluding a significant proportion of existing primary studies.
A scoping exercise revealed a number of primary research studies from the last decade, exploring caregiver experiences whilst looking after a child undergoing inpatient cardiac care.14–24 However, individual study findings were limited by small samples and/or a single hospital context.
The aim of this systematic review was to identify, appraise and synthesise existing qualitative research exploring the experiences of caregivers in paediatric in-patient cardiac services (PICS) over the past decade. 25 The study aimed to (a) generate a deeper understanding of caregiver needs during hospital admissions, and (b) to inform caregiver priorities for future development of child and family-centred PICS.
Methods
Research design
This design follows the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P)26,27 and was registered on PROSPERO in April 2018 (CRD42019128696).
Search Strategy
All primary searches were conducted between April–May 2019 in Medline, Allied and Complimentary Medicine Database, Cumulative Index of Nursing and Allied Health Literature, EMCARE, PsychINFO and Scopus. Supplementary grey literature searches were undertaken in Proquest, OpenGrey and ETHOs, and hand searching of citations and reference lists was undertaken in included studies.
Search concepts were extracted from the research question using the modified Setting, Perspective, Intervention, Comparison and Evaluation (SPI(C)E framework 28 (see Supplementary Material Table 1). Synonyms for each concept were collectively developed by the authors, then individually applied to the ‘title’ and ‘abstract’ domain of each database. Medical Subject Headings (MeSH) terms were utilised and ‘sibling terms’ cross-referenced to exhaust search terms. All terms were systematically combined to retrieve relevant articles. An example search strategy is presented in Supplementary Material Table 2.
Eligibility criteria
The following eligibility criteria were applied:
Original studies employing qualitative research design, including mixed-method designs where qualitative results were presented.
Reporting on experiences of caregivers, defined as an adult aged 18 years and older, in a position of main custody of a child (0–18 years old), receiving hospital-based interventions for CHD or AHD.
Published between 2008 and May 2019 to reflect the last decade of advances in healthcare technology within cardiac services.6,7
Non-English language studies were considered only where a fully translated English version was available.
Studies exploring the child’s perspective were excluded due to their critically unwell status in hospital, and age, with the majority of surgeries for CHD occurring in infancy. 3
Screening
All retrieved references were screened for removal of duplicates, then screened by ‘title’ and ‘abstract’. Potentially eligible studies underwent full text review using the eligibility criteria before final inclusion was determined.
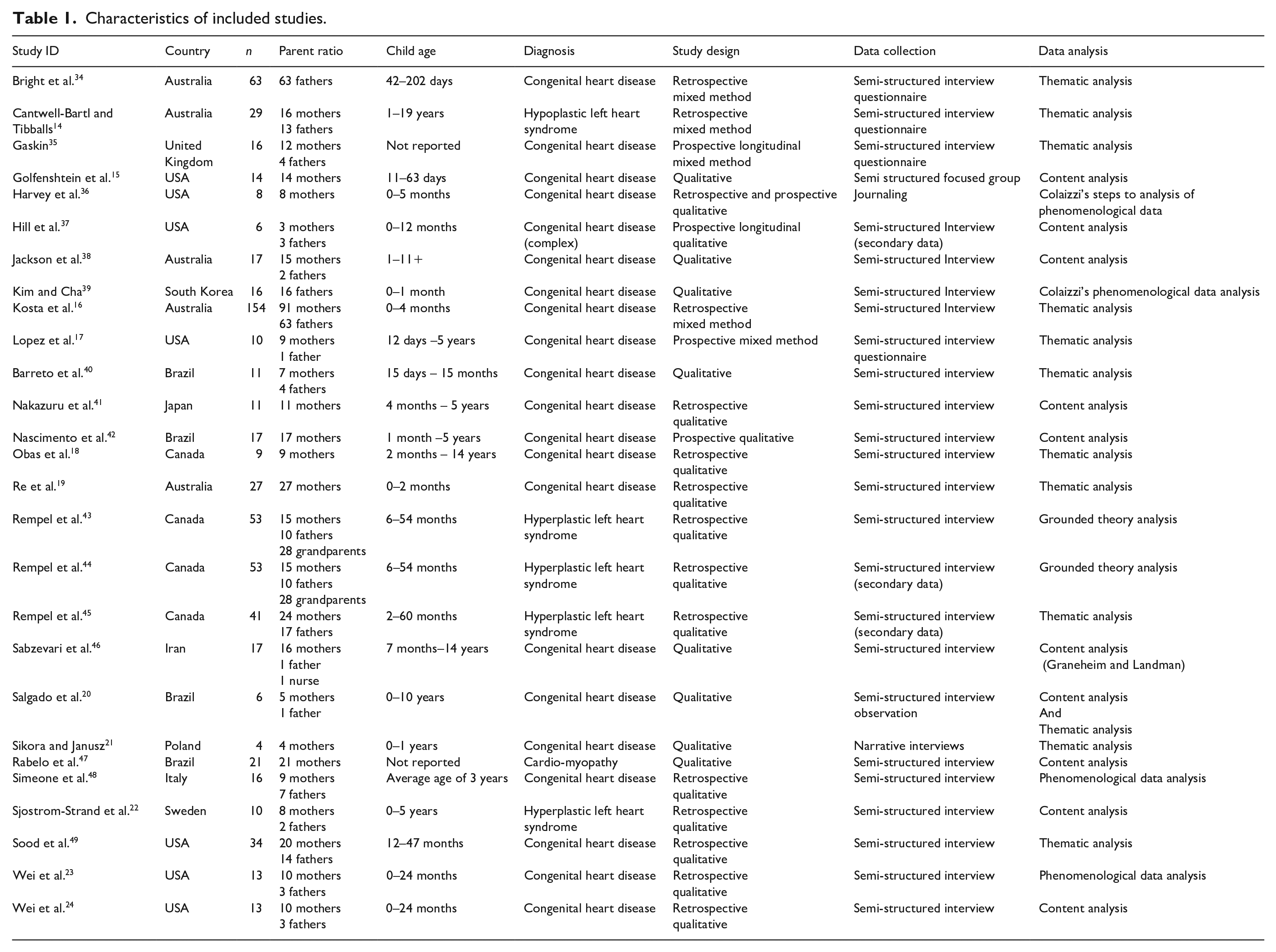
The screening process was undertaken by two authors (RKL/RS) independently. Conflicting eligibility of a study was resolved through discussion or by a third member of the research team (CC). Final articles meeting the eligibility criteria were subjected to reference list and citation screening by hand (RKL/RS), retrieving a further seven studies. The full screening process is presented in a Preferred reporting items for systematic review and meta-analysis (PRISMA) diagram 27 (Figure 1) and study characteristics were extracted into a standardised format table (Table 1). 25
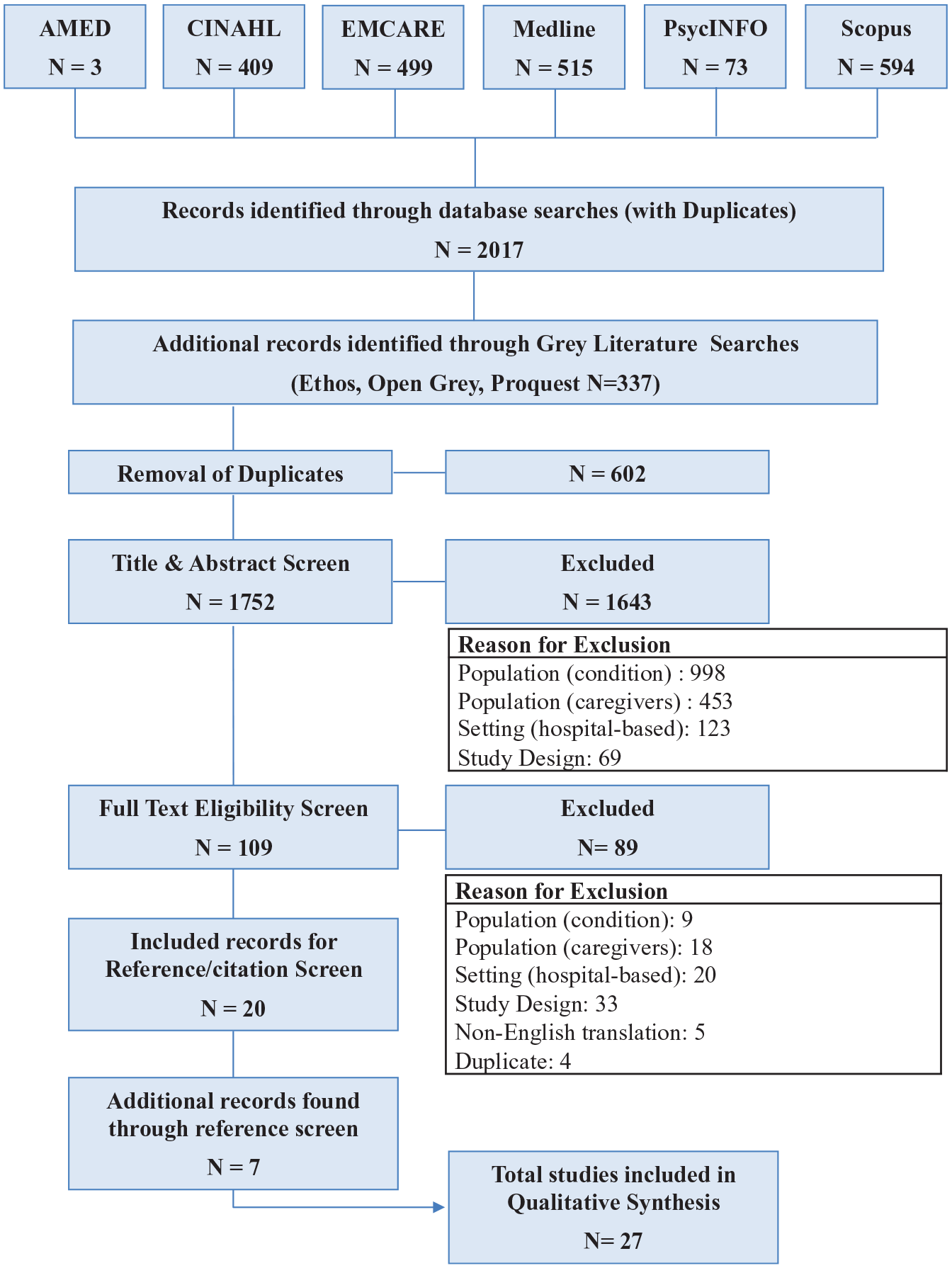
Preferred reporting items for systematic review and meta-analysis (PRISMA) diagram. 27
Characteristics of included studies.
Quality analysis
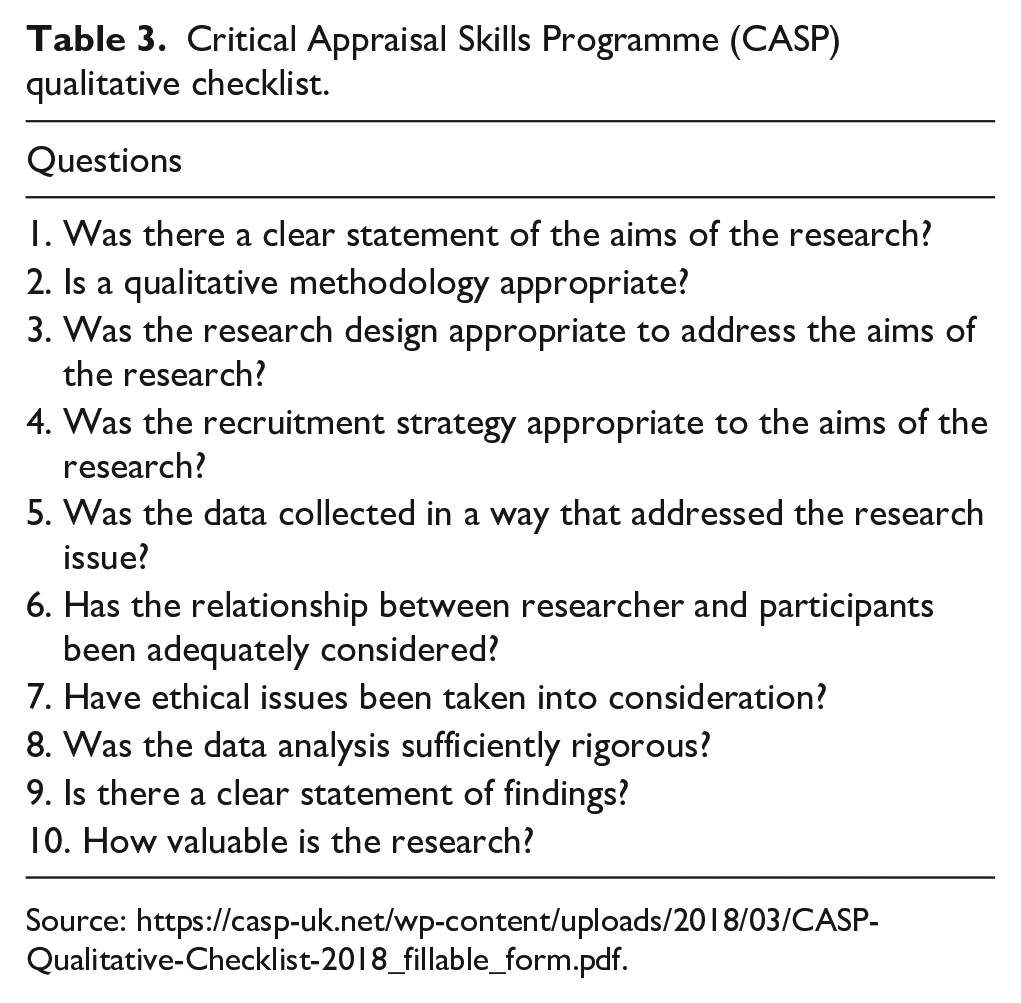
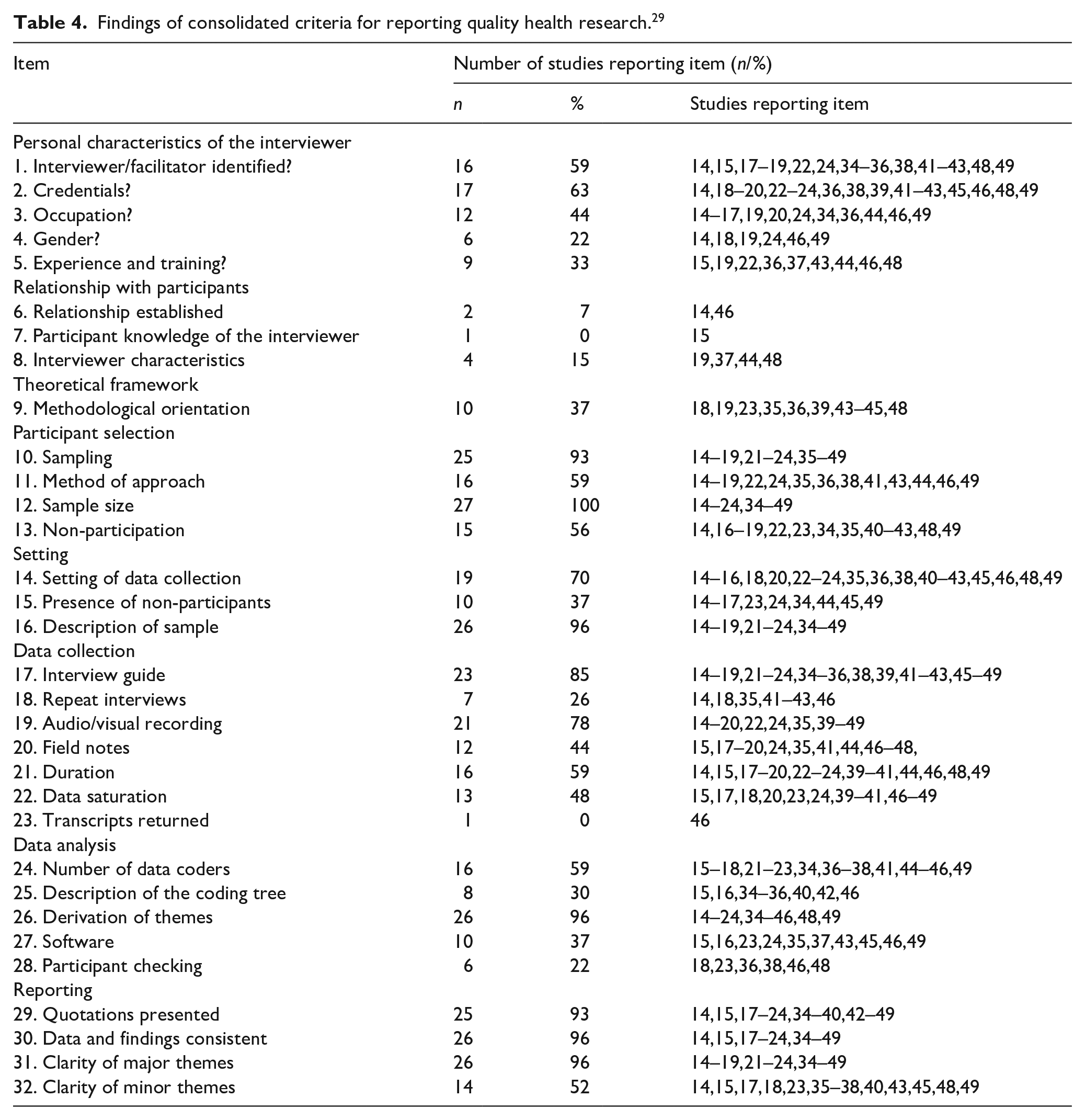
Quality analysis of eligible studies were assessed using the Critical Appraisal Skills Programme (CASP). The tool was selected based on its high utility and adaptability to assess multiple and relevant methodologies. 26 The Consolidated Criteria for Reporting Quality Health Research (COREQ) 29 were used alongside the CASP to assess comprehensiveness of items reported in individual studies.
The quality analysis process was undertaken by two authors (RKL/RS) independently and any conflicting judgments were resolved through discussion or by a third member of the research team (CC). Findings are presented in Tables 2–4. Quality analysis did not inform the exclusion of articles as there is no existing evidence-based consensus of threshold for exclusion. 30 However, quality of individual studies was considered in the Confidence in the Evidence for Reviews of Qualitative Research (CERQual) assessment of review findings. 31
Findings of Critical Appraisal Skills Programme (CASP).
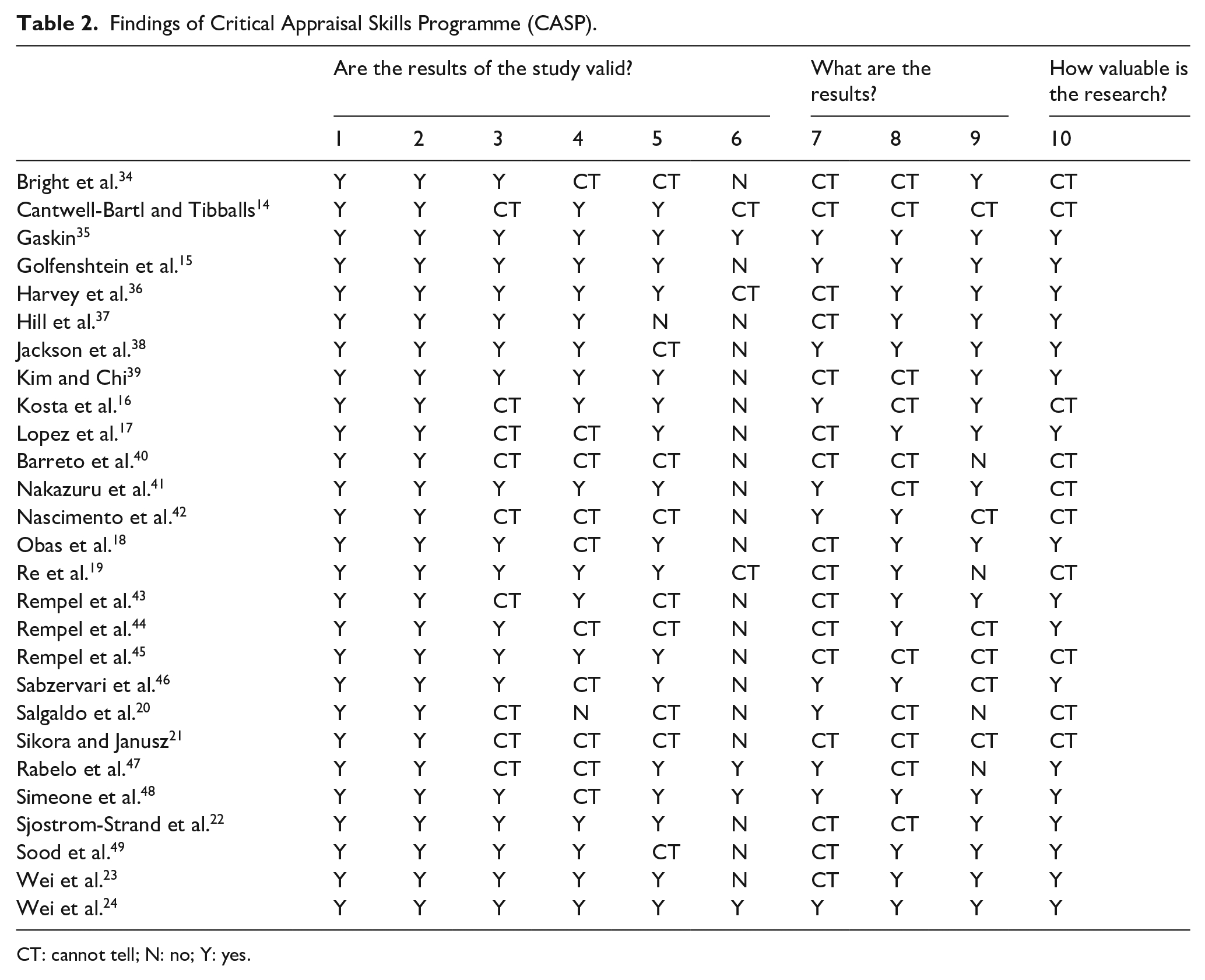
CT: cannot tell; N: no; Y: yes.
Critical Appraisal Skills Programme (CASP) qualitative checklist.
Findings of consolidated criteria for reporting quality health research. 29
Data analysis
Framework synthesis employs predetermined themes whilst simultaneously building new themes, supporting the inductive ethos of qualitative data analysis whilst maintaining a transparent, structured process of a systematic review design in a five-staged approach:32,33
Familiarisation with the included studies: eligible studies were repeatedly read until key ideas and recurrent themes became evident.
Development of the ‘a priori’ framework of themes: all reported themes were extracted from eligible studies, collectively combined and reconfigured based on commonalities to generate an ‘a priori’ framework of themes.
Application of the ‘a priori’ framework of themes: primary and secondary data was extracted line-by-line from ‘results’ and ‘discussion’ of each study and then indexed under the ‘a priori’ framework. Data failing to conform was coded to build new concepts.
Arrangement of data in a systematic matrix: all identified themes were charted against the indexed data from eligible studies, allowing clear comparison and contrast across the collective body of evidence.
Mapping and interpretation: the matrix facilitated identification of associations between themes, reconceptualising data into a final framework that represent evidence across all 27 studies.
All stages of data analysis were undertaken by two authors (RKL/RS) independently, and then collectively through in-depth discussion. Findings underwent peer review by the remaining authors before final conceptualising of themes. NVivo 12 software was used to organise and support data analysis.
Results
Twenty-seven studies met the criteria for inclusion (Figure 1), representing the views of 396 mothers, 237 fathers, 34 grandmothers and 22 grandfathers across 11 countries. Seventeen papers included mixed caregiver cohorts, whilst 10 papers focused on single cohorts of fathers (n=2) or mothers (n=8). The review represented a diverse severity level of CHD and one cohort with AHD. Two studies did not document the child’s diagnosis.20,42 All participants were caregivers of surviving children, with the exception of one mother. 19 Time of data collection varied, consisting of 15 retrospective studies, four prospective, one combined and a further seven studies failing to clarify. Study characteristics are outlined in Table 1.
Quality analysis identified 10 out of 27 studies to have significant risk of bias, whilst still contributing to review findings (Tables 2 and 3). Of these, five studies presented methodological limitations in recruitment strategy, data collection and data analysis.20,21,34,40,42 Five studies contributed mostly secondary data due to limited verbatim quotes, introducing researcher bias within individual studies.14,16,19,21,41 One study offered limited data during the inpatient period 45 reducing its relevance to this review. Inadequate reporting was noted in seven of these 10 studies, in which <50% of COREQ items were reported (Table 4), limiting author judgement within CASP analysis.
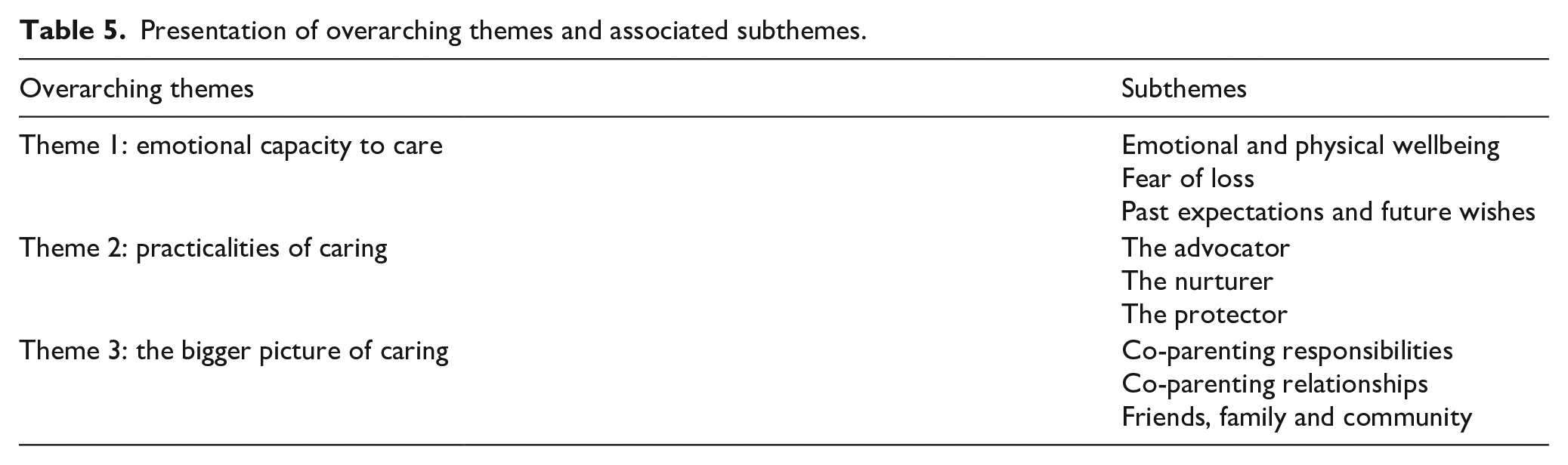
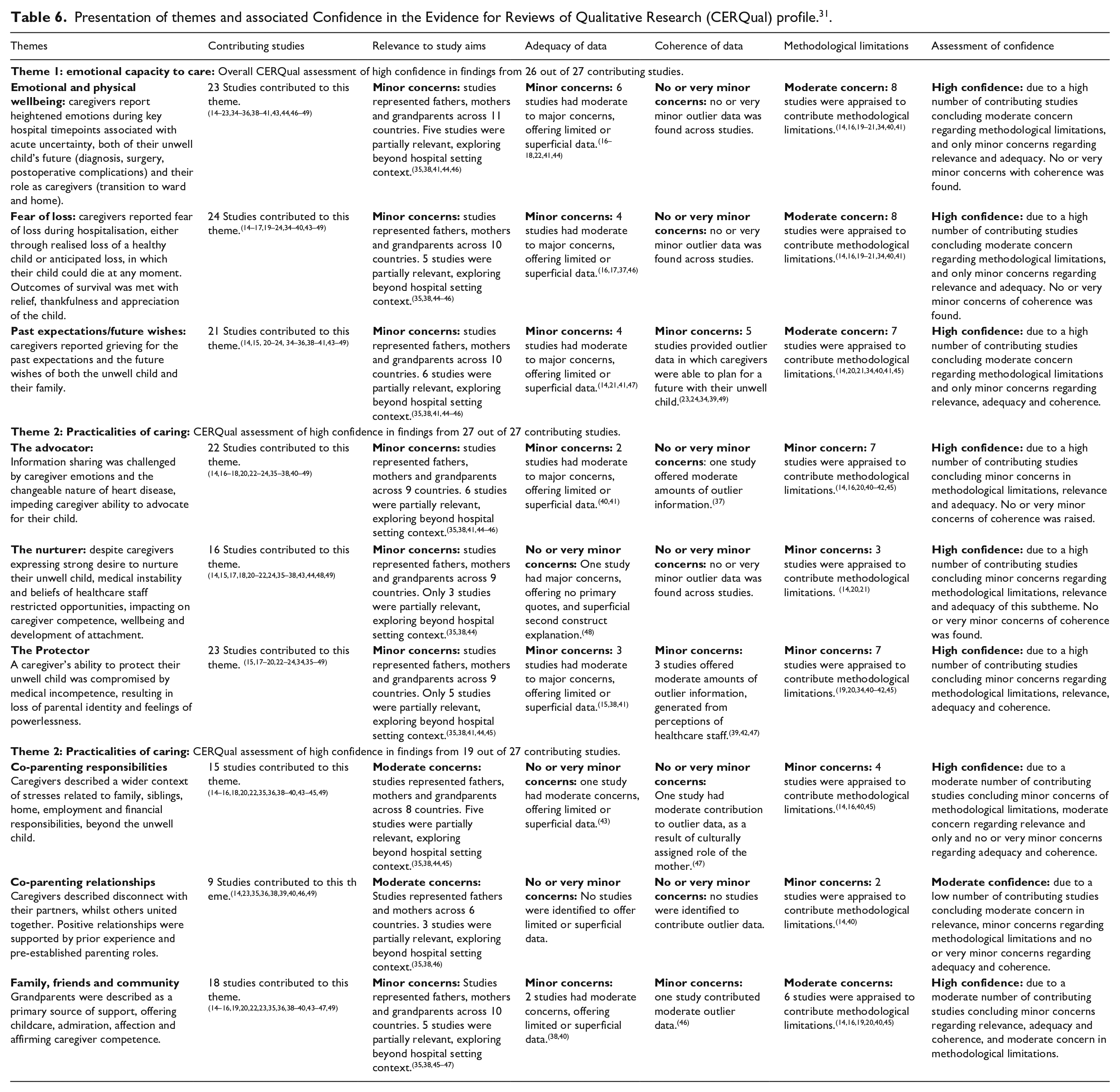
Framework synthesis revealed three overarching themes: ‘Emotional capacity to care’, ‘Practicalities of caring’, ‘The bigger picture of caring’, all of which contained three subthemes (Table 5). Illustrative quotations are provided for each theme; further detailed participant quotations are presented in Supplementary Material. All themes underwent CERQual assessment, concluding relevance, adequacy, coherence and methodological limitations across contributing studies. 31 A CERQual qualitative evidence profile is presented for each theme in Table 6.
Presentation of overarching themes and associated subthemes.
Presentation of themes and associated Confidence in the Evidence for Reviews of Qualitative Research (CERQual) profile. 31 .
Theme 1: emotional capacity to care
Caregivers were highly aware of emotional instability endured during their hospital stay. Heightened emotions were reported when receiving the heart disease diagnosis, during surgery and post-operative care, particularly when seeing a distorted image of their child. ‘The fear of my son’s death was constant and remained until I saw the tubes, all those wires around him, disappear’ [Mother]. 48 There was an overwhelming uncertainty about their child’s immediate and long-term future, accompanied by fear of their child’s death, impacting on the caregiver’s ability to form secure parental attachments.
We didn’t know if she would make it through the first surgery or anything. . . . not to say you’re detached but you’re a bit guarded. . . I loved her and I knew that we wanted to keep her but you don’t connect [Mother].
44
Outlier reports of positive attachment were noted following success of surgery, or by caregivers who had experienced bonding opportunities at home prior to admission.
Caregivers reported various approaches to manage profound uncertainty; fathers described self-protective behaviours, distancing themselves from the unwell child; whereas mothers desired proximity, expressing anxiety when separated from their unwell child at night-time. This resulted in lack of sleep and neglect of self-care. The few mothers that reserved time for themselves did so reluctantly, accompanied by emotions of fear and guilt.
At first I didn’t want to be with him but now I can’t get enough of him [Father].
34
I am not hungry anymore, I feel dizzy eventually, I do not want to dress up, and if I could, I would be by his side all the time [Mother].
47
Caregivers were compelled to live in the present, expressing grief for past expectations of a healthy child and anticipated fear of loss for a future together. Some caregivers made efforts to find positivity on a daily basis, describing a sense of thankfulness and appreciation for the time they had. Some caregivers looking to the future did so with a mixture of hope for normalcy and fear of their child’s vulnerability. A minority reported acceptance of an uncertain future with support from their religion, faith or spirituality. ‘I would pray that if it was my child’s time to go to heaven, then let him go quickly and without pain’ [Mother]. 36
CERQual assessment concluded high confidence in findings from 26 contributing studies.
Theme 2: practicalities of caring
Caregivers expressed strong desires to advocate, nurture and protect their unwell child. Limited opportunities to fulfil such roles impacted on their emotional wellbeing, competence and ability to develop secure attachments, whilst more ‘experienced’ caregivers felt a loss of normality and identity as an established primary caregiver. ‘Deep down, I’m really looking forward to going home because then we can bond properly’ [Father]. 35
Caregiver advocacy was challenged by the unpredictable nature of heart disease, generating narratives of changeable care planning, vague prognoses and urgent decision-making without preparation. Reports of shock and denial hindered caregiver’s ability to process information and advocate competently. In one study of Iranian women, advocacy was further challenged by cultural beliefs: ‘When my child needed an operation, I thought to myself, what can I do when his father doesn’t give the permission’ [Mother]. 47
Caregiver’s desire to nurture their unwell child was widely reported following surgical intervention, associated with fear of loss. Yet these moments were characterised by restricted intimacy, proximity and privacy due to their child’s medical instability. Caregivers were predominantly accepting of this, for fear of harming their child. However, opportunities to nurture were also determined by healthcare professional beliefs. Nurses were referred to as ‘gatekeepers’, generating conflicting experiences, in which some caregivers received support in rebuilding their competence whilst others felt restricted in caregiver-child interaction, giving rise to frustration, helplessness and distrust. This was exacerbated by inconsistency across professionals: ‘It depends on the nurse working as to how involved I can be with daily cares’ [Parent]. 37
A caregiver’s ability to protect their unwell child was primarily compromised by their medical incompetence, generating feelings of powerlessness and loss of parental identity, particularly during intensive care stays: ‘What is a parent who cannot help his child?’ [Father]. 48
This gave rise to contrasting behaviours: some caregivers reported reassurance and dependence from hospital staff and monitoring equipment, although this led to uncertainty of their capabilities when caregiver responsibilities increased on the ward: I just wanted to make sure I was . . . not going places I shouldn’t [because] I know she has a huge scar on her chest now [and] I don’t want to . . . rub it at all or even get it wet [Parent].
18
Others described vigilant behaviours in an effort to build medical competence, accommodate uncertainty and safeguard against perceived inadequacies in healthcare practice. These behaviours continued on the ward due to a perceived lack of nursing attention and safety: ‘I couldn’t leave him there and go rest . . . because the nurse has too many patients to watch’ [Parent]. 18
CERQual assessment concluded high confidence in findings from all 27 contributing studies.
Theme 3: the bigger picture of caring
Caregivers reported multiple disruptions to family life, identifying gender-specific stresses that were shaped by different residential environments. The majority of mothers stayed in the hospital, describing their surroundings as hostile and without comfort or privacy. Disconnect from their former lives, their partner and other children generated feelings of guilt, resentment and isolation.
My husband had to go back to work. I was resentful at times. There were dramas and horrible things that happened and he wasn’t there, women don’t have the opportunity to leave the PICU, collect their thoughts, and then return [Mother].
14
Mothers primarily sourced hospital-based supports from chaplaincy, healthcare staff and other mothers within the unit and social media groups. ‘I relax having a conversation with the other girls. Everybody here is very united. We help each other very much’ [Mother]. 47
Father’s narratives exposed a wider context of stresses, including employment, travel and family. Financial stability generated significant disparity across father’s narratives; a few families accessed paid help and medical insurance, others expressed difficulty managing transport and medical care costs. ‘Financial support from the church for paying the hospital bill. . . I was thankful for it. What could we do? We couldn’t turn it down because we needed it’ [Father]. 49
Fathers who could not afford the privilege of transport and time in hospital, expressed similar emotions of guilt and resentment, isolated from their partner and unwell child. Sources of support were limited to flexible employment and family members. ‘While mom was here and baby was here they got support and they got help, but I was pretty much fending for myself’ [Father]. 49
The co-parenting relationship was variable, as some caregivers described disconnect with their partner, whilst others came together in times of emotional distress. One determining factor in positive co-parenting relationships was the pre-established roles and responsibilities reported by caregivers with previous hospital experience. Father’s narratives expressed concern for their partner, although this was not reciprocated across mother’s narratives.
Siblings presented a shared challenge for mothers and fathers, reporting concern for their wellbeing, managing difficult behaviour and balancing childcare. Grandparents were widely identified as a source of childcare for siblings; yet they also provided emotional support to caregivers through admiration, affection and affirming competence, although a minority reported grandparents intensified their emotions of self-blame and incompetence. Caregivers expressed the importance of re-establishing the family unit prior to discharge. ‘A relief is that we could all be in the room together and he could see his brothers’ [Mother]. 23
CERQual assessment concluded high confidence in overall findings from 19 contributing studies.
Discussion
This systematic review included 27 studies, exploring inpatient experiences of 689 caregivers of children with heart disease, across 11 countries. Three overarching themes within this review generate understanding of the caregiver’s emotional wellbeing and its impact on the parent-child relationship, their identity as a caregiver and the caregiving role beyond the unwell child. CERQual assessment concluded high confidence in all three overarching themes, with moderate confidence in one subtheme: ‘co-parenting relationships’, due to fewer contributing studies and concern over partial relevance to the hospital context.
Findings from theme 1 contribute understanding and context to caregiver emotional distress evident in existing quantitative research. 8 Emotions were characterised by uncertainty and loss. Previous literature has identified key time-points of heightened stress throughout the hospital journey. 4 This review links these time-points through profound uncertainty about the child’s future (diagnosis, surgery, post-operative care) and of the caregiver responsibilities and capabilities (transition to ward care and discharge home), which is a largely overlooked finding limited to literature exploring the home setting. 50 These findings inform priorities to develop caregiver identity in the earliest stages of hospital care and establish consistency in their responsibilities to reduce uncertainty surrounding their role.
This review also highlights the caregiver’s perception of loss throughout the hospital journey, from grieving the loss of a healthy child to anticipated loss of a future together. These reports are associated with self-protective behaviours, reflecting recent review findings exploring coping strategies in parents of children with CHD, both in hospital and at home. 12 However, these behaviours are likely to be heightened in hospital, where perception of loss is more acute. Findings inform priorities for early emotional support to manage ‘loss’, in an aim to develop positive secure attachments and improve wellbeing and quality of life for both caregiver and child.4,52
Existing literature debates impacting factors of gender,4,8,51 severity8,52,53 and timing of diagnosis54–56 on caregiver distress. Our findings revealed comparative narratives across such factors. However, emotional and psychological support were variably sourced across genders. Mothers primarily relied on peer support from other mothers in the hospital, of which the benefits have been established in few existing studies.57–59 Fathers made no reference to institutional-based emotional or psychological support, despite experiencing similar emotional distress to mothers. These findings raise concerns about a lack of assessment, availability and accessibility of support for fathers in hospital, informing a priority for further research. Spirituality as support was also variably referenced, predominantly in North American and Brazil-based studies, highlighting its importance as part of a comprehensive and inclusive assessment of emotional and psychological wellbeing in future services.
Findings from theme 2 distinguish three components of the caregiver’s role: to advocate, nurture and protect their unwell child, informing meaningful involvement in family-centred hospital care. However, significant disparity existed between caregiver desire and ability to implement their role in practice, highlighting barriers of organisational policy and cultural healthcare beliefs, particularly within intensive care settings. Loss of the caregiver role impacted on caregiver-child attachment, identity, competence and emotional wellbeing. These findings are reflected in comparative paediatric60–62 and neonatal63–65 non-cardiac intensive care settings, in which the child is acutely unwell, prohibiting safe caregiver involvement. However, review findings highlight the importance of supporting the caregiver’s role as a ‘vigilant observer’ to build competence, manage uncertainty and prepare for the cultural shift between intensive care, ward and home settings. 66
This theme also revealed distinct challenges specific to caregivers looking after a child with heart disease. The unpredictable nature of this condition hindered decision-making, care planning and information exchange, leaving caregivers feeling unsupported, helpless and unable to advocate competently, with some looking to their religion for guidance. These findings validate the importance of spiritual, 67 palliative 68 and emotional care to support caregiver advocacy during crucial information exchange associated with a life-threatening heart condition.
Findings from theme 3 relate to the wider context of the caregiver role, revealing disparity in factors of gender and socioeconomic status. Very few mothers described life outside the ward, whilst fathers juggled responsibilities beyond hospital. Yet, both roles shared a myriad of painful separations, depicted by isolation, guilt, resentment and a loss of support from each other, reflecting marital strain concluded across existing literature. 69 Socioeconomic status influenced the father’s role, as finances determined their time in hospital, impacting on feelings of isolation and uncertainty, reflecting existing links between socioeconomic status and emotional wellbeing. 70
Strategies of joint decision-making, communication and teamwork were evident in families with prior experience in parenting and hospital admissions for their unwell child.71,72 These findings inform priority of resources to support first-time families that are yet to establish roles and routines outside of hospital. However, families with existing children demanded further division of their roles. Grandparents were noted to offer emotional and practical support to caregivers, whilst caring for siblings. These findings align with previous literature 73 and highlight the importance of the grandparent role as an extended caregiver within the family unit.
Transition from hospital to home is recognised as period of heightened emotional stress with support focusing on acquiring medical and nursing competencies needed to care for the unwell child. 50 This review generates an additional challenge of discharge, as caregivers depicted struggles to reconnect with their partners and faced disparities in attention given to their unwell child compared to siblings, informing priorities for further research into early family integration within the hospital setting.
Strengths and limitations
This systematic review was strengthened by a pre-agreed and transparent protocol, quality analysis of individual studies (CASP and COREQ) and findings (CERQual) and the participation of two independent reviewers during screening, data extraction and quality appraisal processes. However, lack of direct contact with participants limits the researchers’ ability to fully comprehend and interpret primary data. Furthermore, data extraction from published studies introduced a reporting bias to analysis and interpretation. The quality analysis of this review did not inform inclusion of studies, however, efforts to present quality analysis findings offer the reader transparency and an opportunity to make their own judgments about the quality and contribution of included studies.
This review highlights underrepresented views from single mothers, grandparents, caregivers of children with AHD and fathers, although recent efforts have been made to engage fathers in paediatric care research with intent on bridging the evidence gap within this field. 74 Demographics of interest including age, socioeconomic status, hospital admission duration and cardiac interventions were underreported, restricting subgroup analysis of these variables and subsequent implications. However, within the available demographic data, diverse spiritual, cultural and social characteristics were represented.
Conclusion
Caregivers looking after children with heart disease in hospital experience significant challenges, highlighting poor mental health and wellbeing, barriers to practice caregiving tasks and balancing responsibilities beyond the unwell child. These challenges impact on the caregiver’s ability to form early attachment, develop competence and prepare for primary caregiving in the home. Caregivers highlight support from their spiritual beliefs, peer groups in hospital and wider family, including grandparents. These findings further healthcare practitioner understanding of the hospital experience and highlight priorities for family-centred service development in PICS.
Supplemental Material
10.1177_1474515120951974_Supplement_Material – Supplemental material for Caregiver experiences of paediatric inpatient cardiac services: A qualitative systematic review
Supplemental material, 10.1177_1474515120951974_Supplement_Material for Caregiver experiences of paediatric inpatient cardiac services: A qualitative systematic review by Rachel Knight Lozano, Stephen May, Carl Clarkson and Rebecca Sarjeant in European Journal of Cardiovascular Nursing
Footnotes
Acknowledgements
The authors would like to thank the parents of the Freeman Parent Support Group who have contributed to the design of this study. They would also like to thank the Children’s Heart Unit Foundation, who have supported the author’s research development in this study.
Implications for practice
Assessment and support of emotional and psychological wellbeing beyond the mother, to encompass fathers, grandparents and other members within the wider co-parenting unit. Emotional, psychological, spiritual and palliative resources should focus on critical time points, including diagnosis, surgery, post-operative care, transition to ward care and discharge home, in an aim to support feelings of loss and uncertainty. Hospital cultures require further change to build ‘truly’ equal partnership with families. Opportunities for caregivers to advocate, nurture and protect their unwell child should be embedded early and remain consistent where possible, to maintain their identity, wellbeing and competence transitioning between hospital and home. Consideration of responsibilities and support networks beyond the unwell child should be established on admission, as part of a comprehensive assessment of needs to promote stability, wellbeing and quality of life for the wider family.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chartered Society of Physiotherapy Charitable Trust (PRF/18/B12).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.