
Abstract
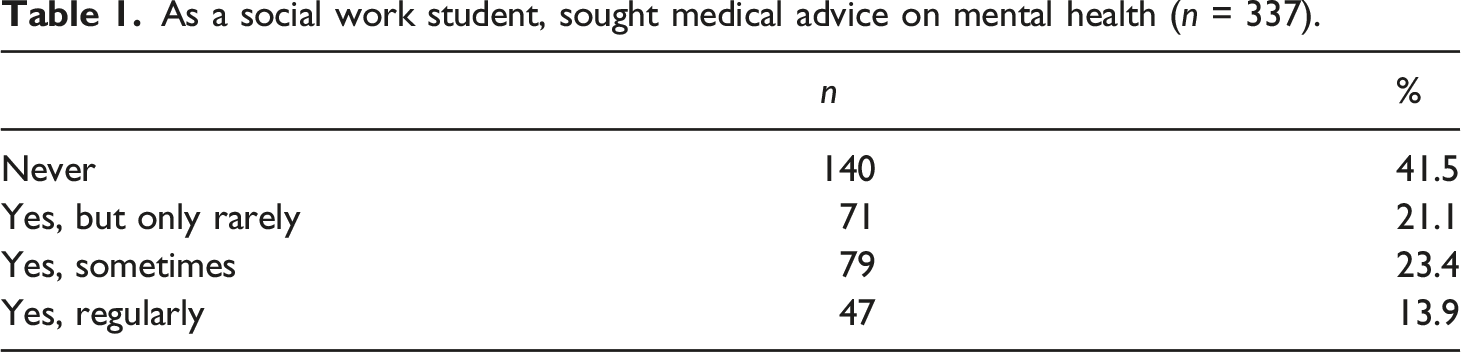
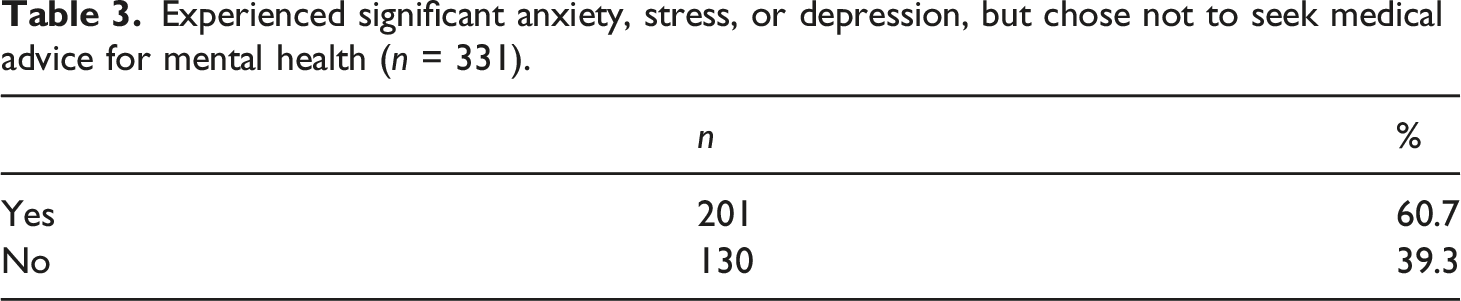
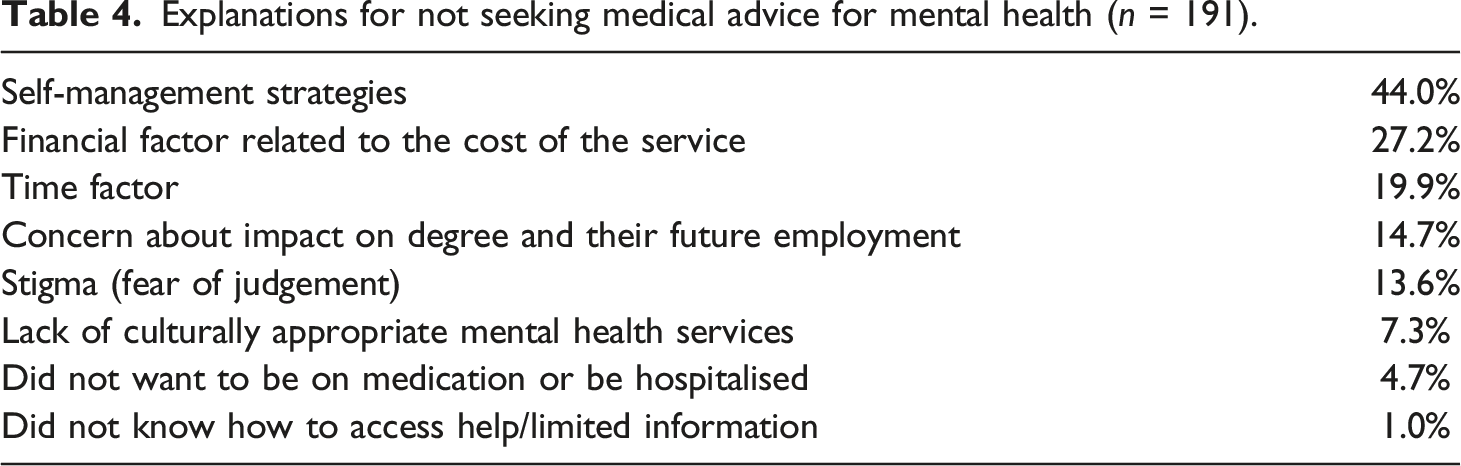
Growing evidence reports that social work students experience financial hardship and negative impacts on their health and wellbeing as they juggle study, paid work, and family commitments. Social work qualifying programmes require extended compulsory field placements, which increase students’ financial stress and potentially exacerbate mental health vulnerabilities. A national survey of social work students and recent graduates in Aotearoa New Zealand, was conducted in 2019, gaining 353 responses, augmented by 31 semi-structured interviews. We report the analysis of both open-question survey and interview data related to students’ experience of mental distress. The survey revealed that 58.4% of respondents had sought medical advice on mental health while a social work student. At the same time, 60% of participants who experienced significant anxiety, stress, or depression chose not to seek medical advice for their mental health. Cost and access were among the main reasons for not seeking help. However, more than one in four (28%) identified stigma and fear of career consequences as reasons for not seeking help. This finding has implications for social work education and needs further research and policy development.
Keywords
Following many anecdotal reports of student hardship, researchers from two different tertiary institutions offering social work degree programmes in Aotearoa New Zealand collaborated in 2019 to undertake an exploratory study of student hardship and wellbeing amongst a national sample of current social work students and recent graduates. The study aimed to gain a broad view of student perceptions of the impact of social work study on their financial, social, and mental wellbeing.
Literature review
Health, wellbeing, and hardship
Many social work students today face multiple challenges in managing their studies. Typically, they must pay education fees, borrow from student loan schemes, undertake paid work and manage family and other responsibilities while enrolled in social work education programmes. This situation is exacerbated by the demands of extended, unpaid fieldwork placements (Crutchfield et al., 2020; Morley et al., 2023; Oke et al., 2022). It is well established that the ongoing tensions of managing these different facets of student life can have a detrimental effect on health and wellbeing (Collins and Morris, 2010; Cox et al., 2022; Gair and Baglow, 2018a, 2018b; Landstedt et al., 2017; McAuliffe et al., 2013; Martin, 2010). Australian research reports that accumulating stressors from years of financial hardship, with some students forgoing even the most basic necessities, can cause or exacerbate mental distress (Gair and Baglow, 2018a, 2018b; Landstedt et al., 2017).
In New Zealand, over 1984 to 1999 governments implemented a comprehensive redesign of the tertiary education system as part of a neoliberal policy regime, including a shift towards targeted student allowances and by funding of tertiary education with ‘historically and comparatively high student tuition fees and student loans’ (Roper, 2018: p. 10). Rising tuition costs reflect the perception that higher education is a private, rather than public, good (Roper, 2018; Thornton, 2016). Tuition costs and barriers to accessing income support drive many students to borrow from student loan schemes and undertake paid work to meet their financial needs (Gharibi, 2018) raising their workloads and contributing to stress. This problem is not confined to Australasia. An earlier systematic review of the literature examining the relationship between debt and mental health found mixed results; however, there was some evidence to suggest that debt may contribute to mental distress (Fitch et al., 2011). A later two-year longitudinal study of 454 British undergraduate students found that more significant financial stress was linked to higher rates of stress, depression, anxiety, and alcohol dependence at baseline (Richardson et al., 2016). Thornton argues that neoliberalist policy ‘sloughs off responsibility for stress’ (2016, p. 48) by not acknowledging the impacts of labour market competition and rising living and education costs on student financial security and related personal hardship.
Students do not enter higher education on the mythical ‘level playing field’. Many struggle with illness, disability, and extant mental distress (Martin, 2010) or have significant caring responsibilities (Hulme-Moir, 2021; Hulme-Moir et al.2022), especially mature students (Heagney and Benson, 2017). A survey of student mental health in Aotearoa, New Zealand, with 1762 respondents from the university sector, found that the mean level of psychological distress according to the Kessler Psychological Distress Scale was 28.1, indicating a moderate level of distress (Gharibi, 2018). Unsurprisingly the burden was distributed unevenly: gender-diverse people, non-heterosexual people, and disabled people were significantly more distressed than their peers. In identifying the causes of their distress, 51.3% identified academic anxiety as a trigger for depression, stress, or anxiety ‘to a great extent’, with 36.1% reporting it triggered them ‘somewhat’. Another 28.5% were significantly distressed by financial hardship (Gharibi, 2018). Adjustments to student life, managing family responsibilities, and meeting tuition costs were also highly cited as reasons for distress.
Stigma and unwillingness to disclose mental distress
Student perceptions of the role of lecturers in higher education were significant in making students feel unsafe or uncomfortable when deciding whether to disclose illness, disability, or mental distress (Martin, 2010). One study found that social work students perceived academics as having significant power over their studies and future careers. Australian study reported on the stigma experienced by social work students who had experience of accessing services for mental distress: ‘students assumed peers and academics would judge their use of services and declare them unfit for practice’. Furthermore ‘[students] conceptualised service users as ‘others’, disconnected from their emerging professional identity … and were to be studied and attended upon rather than members of the study body’ (p. 686).
These student assumptions were borne out in a study of postgraduate social work students’ attitudes towards people with serious mental distress. Corravubias and Han (2011) found that most students would not support restricting service users’ social liberties like voting or driving. However, more than half would not want someone with a serious mental illness to babysit their children or marry into their family. Such stigmatising attitudes were less when students had connections to people who had experienced serious mental illness. Rubio-Valera et al. (2016) reported that when educational content included opportunities to talk to people with lived experience of mental distress, the stigmatising attitudes of social work students were diminished.
Recognition of the negative attitudes held by others towards people experiencing mental distress is probably a critical reason behind the reluctance of social work students to disclose and seek professional help (Martin, 2010). Reid and Poole (2013) in a Canadian study reported that a student participant who disclosed their mental health on the first day of placement was told by their field educator that they should find a different career. Institutional support services in education have also often been experienced as unhelpful to students’ mental wellbeing (Martin, 2010; Reid and Poole, 2013) or unavailable when needed (Tones et al., 2009). In the Aotearoa New Zealand student survey, more than a third of respondents reported waiting two weeks or longer for an appointment with university mental health support (Gharibi, 2018), and this is in a context where most students cannot afford private healthcare (Gair and Baglow, 2018a).
A note on stigma
As noted above, social work students can hold stigmatising views towards people experiencing mental distress. They may need to learn from those with lived experience to develop their understanding of what stigma is and how it can impact help-seeking behaviours (Corravubias and Han, 2011; Rubio-Valera et al., 2016). It is helpful at this point to define stigma. Stigma refers to a negatively perceived attribute or characteristic that sets an individual or group apart from others in society (Goffman,1968). Stigma is frequently associated with negative stereotypes, derogatory terms, discrimination, devaluation, and interactions that may increase the likelihood of social exclusion or withdrawal of people with a stigmatised identity. While stigma can manifest in various forms, UK sociologist Scambler discusses two separate but connected dimensions concerning stigmatised health statuses: felt stigma and enacted stigma (Scambler, 2009). Felt stigma refers to the internalised experiences and emotions of individuals with a stigmatised attribute. It encompasses the negative self-perceptions, shame, and guilt that result from societal prejudice. Felt stigma can lead to profound feelings of worthlessness, low self-esteem, and a compromised sense of identity (Scambler, 2018). Scambler emphasised that while felt by individuals, stigma is shaped by societal structures, power dynamics, and culture ‘weaponised’ as ‘norms marking a moral deficit, non-compliance or blame’ (Scambler, 2018: p. 777).
Enacted stigma refers to the external behaviours, attitudes, and practices perpetuating discrimination and exclusion against those with stigmatised identities (Scambler, 2009). Enacted stigma involves the policies, institutional practices and social interactions that systematically disadvantage individuals based on their stigmatised attributes and may be experienced as microaggressions, verbal or other abuse, unequal treatment, and structural barriers restricting access to opportunities and resources (Byrd and Austin, 2020). Enacted stigma amplifies the negative impact of felt stigma, creating a cycle of disadvantage and social exclusion.
In the context of this study, felt and enacted stigma manifested in several different ways. We will demonstrate from our analysis how fear of enacted stigma – that students who disclose mental distress might meet prejudice and active exclusion through institutional practices (such as being ‘safe’ to go on field placement and needing to be proved to be a ‘fit and proper person’ to be ‘suitable’ for the profession) – can lead to diminished uptake or even rejection of help-seeking.
Study design and methods
A national survey was conducted in 2019 designed to be undertaken by current students and recent graduates (i.e. within the previous five years) of all qualifying social work programmes in Aotearoa New Zealand. When the survey was administered, there were seventeen different providers of social work education. To reach current students, we enlisted the support of the Council for Social Work Education (CSWEANZ), who forwarded the survey invitation to all the schools of social work [from here on abbreviated to SSW] to advertise the survey to their students. We also advertised via the Aotearoa New Zealand Association of Social Workers (ANZASW) to attract members of the Association who were recent graduates. While membership is voluntary, the ANZASW had a membership of around 3,800 social workers at the time of data collection (ANZASW personal communication).
The Qualtrics survey was available online for three months of the 2019 academic year 2019 and completed by 353 social work students or recent graduates. Given that just over 90% of the participants identified as female, gender has not been incorporated into our analysis of the statistical results. However, this does not mean that gender is unimportant. An analysis of the experiences of women students with caring responsibilities revealed that studying social work required considerable sacrifice as study, paid work, and caring work consumed all their time, with little resource left for social and community life (reported in Hulme-Moir et al., 2022).
The survey contained 33 questions, which were a mixture of closed and open-ended questions that addressed a range of topics, including: • demographic variables; • non-paid caring responsibilities (reported elsewhere); • details of the social work qualification undertaken but not including the educational institution, to preserve anonymity; • financial matters, including employment while studying, financial support, student loan debt and the impact of financial hardship (to be reported elsewhere); • aspects of social wellbeing, including the impact of study pressures on relationships with partners, family members, friends, community and hapū/iwi, and on other cultural pursuits (to be reported elsewhere); • aspects of mental wellbeing, including whether participants had sought professional help and whether they had ever experienced significant mental health challenges but chose not to seek medical advice; and • positive strategies employed to cope with the impact of studying.
From an estimated population of 3,000 social work students, 353 participants completed the survey. Nine survey questions sought participants’ further elaboration, soliciting 48,000 words in response. Survey participants were invited to participate in a semi-structured interview. The 31 interviews explored similar themes in greater depth. Both sets of data provided rich information for analysis. This article analyses both interview and survey textual data relating to mental health.
Of the 31 interview participants, 28 identified as female and three identified as male. Twenty-five identified primarily as Pākehā, four as Māori, one as Cook Island Māori, one as Samoan/Pākehā. Eleven were aged 45–54, six were 35–44, seven were 25–34, and seven were aged 24 and under. Interview participants came from 12 different tertiary institutions. Fourteen attended university SSW, and 17 studied in other programmes. Most students (n = 25) were or had been, engaged in full-time study, and the other six were part-time students.
Ethics
Approval for the study was granted by the University of Auckland Human Participants Ethics Committee. Given that students who participated were currently enrolled in SSW, including our own, to avoid any possible sense of coercion from staff in their own programmes, the University of Auckland researchers interviewed the Open Polytechnic students and vice versa.
Researcher positionality
This article tells a compelling story of social work students’ struggles with their mental health throughout their studies. We have developed an understanding of participants’ conflicted attitudes to mental health. As a snapshot of a particular time, this can never be a complete picture, but it is our reading of the shared experience of those students who took the time in their busy academic year or early years of practice to tell us their stories. As qualitative researchers, we did not come to these narratives as neutral readers – the authors include two social work educators, a social work student, and a mental health social work practitioner. One author is the parent of a young woman with a serious and ongoing mental health condition. In this research, our positionality is a source of strength as we have been able to share our responses from different standpoints as we engaged with literature and data.
Brief mental health-related information from the survey
As a social work student, sought medical advice on mental health (n = 337).
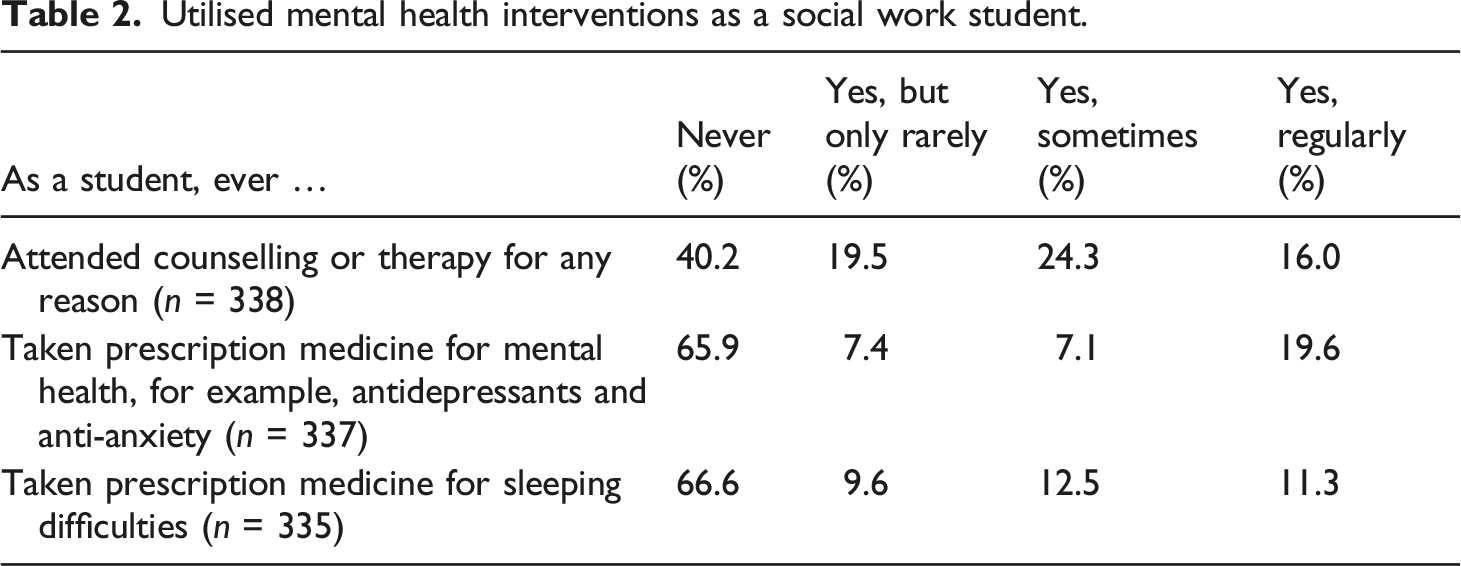
Utilised mental health interventions as a social work student.
Experienced significant anxiety, stress, or depression, but chose not to seek medical advice for mental health (n = 331).
Explanations for not seeking medical advice for mental health (n = 191).
Analysis
Two data sets were explored in the analysis, the textual data from the semi-structured interviews and an open-response survey question, which asked why support was not sought for mental distress experienced during the degree. Following transcription, the interviews and survey open-question responses were uploaded to NVivo for data-management, where all data were read carefully to build initial observations, insights and to explore new understandings. The analysis process was guided by Braun and Clarke’s (2013) method of thematic analysis. Our analysis aimed to ascertain commonalities (and possible differences) in student experiences during their social work study. The analysis process sought to provide a rich understanding of the intersections of the student experience, financial hardship and challenges to mental health, and access to support services. Once familiarisation with the data was achieved, semantic and latent codes were developed and used to identify broad themes, connecting themes and unique perspectives. Significant connections and themes relating to mental health and student hardship were identified and refined by researcher review and selective coding.
Our analysis identified themes related to the manifestation of mental distress, sleep problems, stigma awareness, and help-seeking behaviours. Interview participants are identified by a pseudonym and individual survey responses (SR) by a code.
Findings
‘It nearly killed me’: Striving to do it all and to do it well
A common narrative was shared about problems in achieving an optimal academic study–life balance, and how frequently competing commitments led to vulnerability and decreased wellbeing: For me it's more the pace of life; the financial pressures/constraints and striving to do very well (and learn as much as possible) means I didn't have much time to relax. Being on placement and working towards assignments at the same time nearly killed me… I have to work part-time (late nights), go to unpaid placement full-time, sleep and eat properly. Combined with the high stress of last year, I decided to drop to part-time and complete study a year later than planned. Although I am still not 100%, I feel am coping far better than I would have [SR – Help]
Often, overwhelming anxiety, influenced by course content, study workload, and a lack of support during their study characterised many student experiences. I had the most debilitating period I've experienced during this time; I was written off for three days because of that. I attribute that to stress. [SR – Help]
Some participants with lived experienced of mental distress told of ‘relapses’ during their study, including recurring challenges with anxiety and depression, stress: There are times when I’m procrastinating, and I know that I should be doing my work right through to the time things are due that I just get so beyond anxious [Sandra] My anxiety went through the roof. I reached a point where I couldn’t focus… I was so overwhelmed with the sheer amount of things that I was meant to be getting done [Saria]
‘Peak’ anxiety was associated with exam and assignment due dates, exposure to triggering topics and when undertaking placements – especially during the 3rd and 4th years of the undergraduate degree. Definite anxiety and stress due to workload, and the sensitive content of topics that we write about/research/learn [SR -MH]
Some interview participants described increased uptake of prescribed medications at these trigger points and many accessed doctors’ clinics to discuss medical intervention for mental health related issues. When Saria felt that her anxiety was ‘through the roof’, she reached a point where she sought help: I went to the doctor, and I did an anxiety test and one for depression, so I went on medication for anxiety and depression. [Saria]
While it was not the case for all interview participants, pharmaceutical approaches to mental distress were discussed openly. Not all participants chose to use medication, but many were open to considering this as an option. Some reported being able to engage in discussion with peers about the challenges surrounding mental health. I went on antidepressants …. they work, well they work for me and we actually had a conversation about this in class the other day with a group of us [Lucy]
While not widely named as such by participants, burnout significantly impacted those it did affect. Kahill (1988) described burnout as including three components: depersonalisation; emotional exhaustion; and low personal accomplishment. Some participants discussed how the expectations of study, placement, and balancing other responsibilities left them struggling to achieve their goals and to feelings of losing motivation and passion for social work as a profession. Joce and Maria described their experiences with burnout and how its impacts could have lingering effects on their careers as practitioners. I was completely burnt out afterwards and it took me a long time to really genuinely feel myself again…. I ended up having a complete lack of motivation to do anything social work related” [Joce] [I was] still so burnt out from study and ended up having to leave work in six months of starting and haven’t gone back since” [Maria].
Some students recounted many barriers to accessing support, even when feeling significantly unwell. The cost of accessing service, limited time availability due to employment, caring responsibilities, placements, and the burden of accessing help were also stated reasons why help was not sought by participants: I’ve never felt so bombarded with having to log my struggles-emailing lecturers, explaining how I felt, going to different doctors, and filling out different forms. Although I may have been able to have the (very little) energy to do so, someone who might be in a slightly more intense episode would definitely not have the momentum to do what is required to seek help. I understand that the option for help is there, but it’s somewhat unhelpful when it just causes more stress on someone already in a time of crisis. (SR-MH).
Finances were a contributing barrier to accessing healthcare and other basic needs, often leaving students to prioritise their needs based on immediate demands. This strain creates further pressure when considering the accumulation of study obligations and commitments, especially in the last two years of the degree.
Trouble with sleep
Of the 31 interview participants, 23 mentioned difficulties with sleeping, sheer exhaustion, or lingering tiredness throughout their social work studies. Despite this, only three had medical intervention in the form of medication. Participants identified three factors associated with disturbances to their normal patterns of sleep: study workload, especially when big assignments were due; the ‘exam season’ and field placements. There was also an accumulation of stress from balancing study with other responsibilities, like childcare, household and family obligations and paid work. Existing mental health challenges, specifically anxiety and depression, also featured. I am now in a situation where insomnia has come back quite significantly, and I think it is to do with the stress. [Bella] So that is four years of lack of sleep really… I was just tired all the time [Jane] I mean I was extremely tired and exhausted, but I had no choice because if I didn’t work then I didn’t have food to eat [Karen]
Unlike the other mental health challenges experienced, participants described the challenges of sleep deprivation. Many discussed ongoing feelings of exhaustion and historical experiences with insomnia and other sleep conditions: I have had trouble with sleep my whole degree … a busy mind and some late nights on assignments. It actually got to the stage a couple of years ago where I couldn’t work late at night, I would get migraines and so I have kind of cut that out a bit and take melatonin as a natural thing to help me sleep and I do meditation to help me sleep. [Millie]
Relief from sleep disturbances, for some participants, only came after finishing exams or submitting final assignments and when significant milestones of the degree had been completed, such as placement.
It would go on my record: Stigma, disclosure, and help-seeking
I don't like the labels and stigma attached to services; despite work being done in this area, it is still very much present. [SR – Help]
As noted above, while interview participants were open about their experiences and help-seeking related to mental distress, only three of the 31 interview participants got medical support for significant mental health challenges. Those who offered to be interviewed were more comfortable openly sharing personal stories of distress with the researchers. Many survey responses, however, reported reticence about disclosure to academic staff and recounted compelling concerns about the stigma associated with mental distress, accessing services, and the negative connotations associated with help-seeking. The most robust theme that developed in our analysis of why students did not seek help was their own expectations of themselves as aspiring social workers and the fear that disclosing their distress might jeopardise their studies or careers: Because of the stigma that I perceived amongst peers and staff about mental health, having to be stable to practice as a social worker. I believed that if I spoke to someone it would impact me graduating. I was worried that if I sought professional help it would go on my record, and I would not be able to practice as a social worker.” [SR – Help]
There were many contributing circumstances as to why students chose not to disclose their mental distress: feelings of shame and embarrassment, avoiding gaining a reputation and avoiding confronting the issues they were facing: I lied to my [senior] and said I was taking time off work to complete my placement. I lied to my job and said I was taking time off my placement. I lied to my doctor (even when I burst into tears in the office) and to my friends and family, blaming my low mood on tiredness from glandular fever “[SR – MH] When I first saw signs of poor mental health, I was too scared to seek help due to the judgement of people and people in my degree (tutors, students, other professionals) thinking that I was an unfit social worker or that I couldn’t do it. [SR –Help]
There was a prevalent theme of students’ belief that the intersection of being a social worker and experiencing challenges with mental health was a very uncomfortable place to be: Social work studies generally don’t stigmatise [mental distress]. However, many still are afraid that their job or other people will, and so it is still hard to talk to people about it. Supervisors have been great to go to, however, it is important to see an affordable counsellor. [Counselling] should be available to all students. [SR –MH] [I] did not want my SSW to find out. Hate going to the doctor. Already know what the outcome would be [and] doctors are expensive. [SR –Help]
Many responses to the survey question ‘Why You Didn’t Seek Help’ alluded to feeling their mental distress was not ‘severe enough’ [SR – Help] or that others should be prioritised in support services over them. Furthermore, many felt they could endure mental distress because it would pass once the stressful periods – exams, assignment deadlines, placement, and the final two years of the undergraduate degree – subsided.
Some described feeling they were not unwell enough to get support: I’m just dealing with it [PTSD]myself at this stage. There is nothing else I can do really. I’m just telling myself it is temporary, it will lift soon, fingers crossed. It has never gone on this long before; I have had bouts of it where it comes and lasts for a bit, but this time it is hanging around, so yeah. [Bella]
One survey participant felt that the stress and distress was a consequence of success: I wish I had taken better care of myself, but my academic results were fantastic, so I thought I was doing the right thing [SR-MH]
Some identified gaps between talking about self-care in social work education and actually doing it: … we come into a profession where we want to help others and we don’t put ourselves first and so in that study environment we still do that with our families, with our friends but then we kind of neglect our own wellbeing even though we are taught self-care… we are taught to look after ourselves first but it is generally the case where we look after everybody else and then us at the end. [Angi]
There was an overwhelming sense of embarrassment about help-seeking for mental distress, specifically due to societal expectations of what it is to be a student and the role of social work. Upon further reflection, participants were able to acknowledge their need for help during study: At the time I was embarrassed and felt that I should be able to handle the stress (as other students had). I also had a lot of other psychosocial stressors that impacted my mental health and was unsure how to address this myself. It was also my first experience of a mental health challenge, and I did not seek support from anyone as I was not aware of what might have been helpful.” [SR –Help]
Another survey participant who didn’t seek help wanted to pursue a career in mental health: I refused to go to specialist mental health services because I aspired to work there once I got my degree and felt that I might be less welcome if I had.
For some students a lack of security about confidentiality impacted on help-seeking: I chose not to [seek help] because I felt that if I saw a counsellor while studying social work it might jeopardise my studies, like my lecturers might hear about it and try to tell me to take time off or like tell me that because I'm so depressed or not feeling okay mentally, that I might get dropped from the course [SR – Help].
These beliefs further emphasise the stigma felt by students and related unwillingness to disclose mental distress, even to professionals, for fear this information could get back to the SSW and jeopardise their futures – students are choosing to struggle in the moment, to fulfil outcomes but at considerable cost.
Having trust in strong relationships with the SSW faculty meant that some students felt more able to communicate openly about mental health, their needs and their ability to adapt to commitments, like assignment deadlines, to enable them to cope. However, Bella reported that some faculty de-humanised students, and this left her feeling alienated: We have lost a few really good tutors that treated us like people and the tutors we are left with, I don’t know, they feel separate from us. They don’t feel like they are on a level with us [Bella]
When considering the content of the social work degree, it is interesting to consider whether what is taught might also drive stigma about how student mental health is viewed and whether accessing care is appropriate for them. Is seeking help what ‘other people’ do, not social workers?
The individualising discourses of neoliberalism, where ‘self-help’ and personal resilience are valorised, were also sometimes visible, for example, where this respondent feels they should not be a burden, calling on the trope of personal responsibility: That is not how I deal with my problems, and it makes me uncomfortable going to other people about my problems. It makes me uncomfortable asking for help when the SSW has taught me so much about how mental health problems develop and are fixed that I feel as if I can and should handle it myself; because I am also aware of the stress that mental health practitioners are under and I feel I do not wish to burden them with something I understand and can solve myself. [SR – Help]
Bella echoed this idea of being self-managing: “I am just dealing with it myself at this stage. There is nothing else I can do really….I work hard to try and keep the stress down”.
Addressing the challenges - coping and support
Trusting peer relationships within the SSW cohort seemed to encourage openness about their struggles in a space of commonality and support: I think because we are a really supportive group, I don’t know if every degree is like that, but social work tends to be that way. If we were to get together for a study group or something and someone had an issue, we would stop what we were doing, and it would become about supporting that person. [Doreen] Don’t shut yourself off; make sure that you’re reaching out where you can, even if it’s just one person. And keep your tutors in the know; it doesn’t have to be detailed, but them having some awareness of what’s going on went a long way.” [Maria]
Participants reflected those strong alliances, trust in their peers and strength in numbers helped to unpack challenges being experienced, where honesty and openness are highly valued. The link to reducing stigma is very clear for this participant: We need to set a good example to others by addressing our own mental health challenges and being honest about them to do our bit to reduce the associated stigma. I think social work students should be encouraged to take ownership of their mental health, and SW education would do well to have more discussion around this. [SR – MH]
Students who had experienced earlier mental distress often had beneficial coping mechanisms. Two students who reported a history of addiction in the open-response question about mental health mentioned they were coping ‘extremely well’ and knew to ‘reach out to support when needed’ [SR – MH &Addiction].
While only mentioned a few times, Te Ao Māori and Pasifika approaches to support were identified. Participants explained that they valued to the holistic approach of models like Mason Durie’s Te Whare Tapa Wha (Durie, 1998), guidance from elders as well as wanting access to services aligning to Rongoā Māori (Māori healing). One participant from the surveys also discussed wanting to see greater funding and support for Māori mental health to make them more accessible.
Non-pharmaceutical, natural approaches to mental health support were also recognised as offering alternatives to mainstream medical interventions: I know at this point some people would be choosing to take more medication for it, because it’s just going on and on and on, but I’m not - I choose not to. I don’t want that destructive stuff in me anymore. [Bella]
Our analysis suggests participants opted for alternative approaches to medical intervention for myriad reasons, including the cost of services, distrust, or the desire to avoid unwanted medical, pharmaceutical, and pathologised treatment. Some of the alternative treatment methods include: ‘natural remedies’ such as oils and herbal treatments, Rongoa Māori, mindfulness, counselling with professionals, life coaches and mentors (church and community) and seeking increased social support.
Perseverance
I just figure you just got to get on and get it done. [Esme]
Finally, our analysis revealed how passionate our participants were about social work and how driven they were to complete their degrees. Those who were caregivers also clearly desired to be good role models to their families (Hulme-Moir et al., 2022). Hulme-Moir’s (2021) exploration of interviews with caregiving students found that the word ‘struggle’ appeared 35 times and was employed by 12 participants to denote the effort required to complete their education. However, although the going was tough, and as previous research has shown (Heagney and Benson, 2017), students, particularly mature-age students, persevered in their efforts to achieve their goals. The language used evokes the spirit of struggle and determination: ‘pushing through’, ‘keeping the end in sight’ or ‘doing what it takes’. In referring to the demands of her placements, Saria was adamant, ‘I have got to get through it – I need to get through it’. Jill admitted it was sheer ‘bloody-mindedness’ that kept her going. Delia had to ‘grit my teeth and get on with it’.
Discussion
Completing this qualification has almost broken me. It has been challenging on so many levels. [SR – MH]
The findings of this study resonate with prior research regarding the mental distress experienced by social work students. Our analysis of decisions made not to disclose and not seek treatment for significant mental distress has revealed a complex set of factors linked to stigma and shame. Some students decided not to disclose mental distress, even to professionals, because of underlying anxiety that this information could get back to their university and jeopardise their future. Students are choosing to struggle without professional help, pushing through, so they can undertake placement and complete their studies. Our participants additionally clearly experienced felt stigma which influenced their help-seeking decisions.
While these findings are of concern, it is important that social work educators avoid a neoliberal emphasis on problematising individuals and their choices, or promote only individualised solutions (Lawrence, 2021). Reifying ‘survival’ is also risking the isolation of ‘individual characteristics such as resilience … without considering wider social, cultural, political, or contextual factors, or “questioning the policies and institutions which scaffold these”’ (Lawrence, 2021: p. 139). In Australia, Gair and Baglow (2018a) reasoned that focusing on student financial hardship should not shift attention away from the systemic institutional and structural reforms needed to address the root causes. While the structural elements of this distress must be addressed, particularly student poverty and indebtedness, student mental distress raises complex issues because of the gatekeeping role of social work educators (Todd et al., 2019).
The regulator (in New Zealand the Social Workers Registration Board, SWRB) influences curriculum and placement expectations but does not direct how fitness to practice might be managed while students are studying, and students do not have to register while studying. Schools of social work are however expected to attest at the end of studies that students are fit to practice (SWRB, 2018). Educators must grapple with balancing the rights of students in mental distress against clients’ rights to receive competent and safe care, as well as satisfying professional regulations. Todd et al. (2019, p. 791) warn that given so much of our focus on mental health focuses on biomedical labels, ‘the drift to further exclusion’ must be avoided, while balancing the safety of all parties.
In our own context of Aotearoa New Zealand, we must take an intersectional approach to wrestling with these challenges, considering fitness to practice alongside an analysis cognisant of the bumpy and uneven playing field our diverse students enter. Structural solutions cannot be achieved till there is the political will to offer better financial support for students, the overwhelming majority of whom are women, who will become key professionals in our social service sector. In the meantime, students will continue to experience mental distress, and educators seek new ways to support them. ‘He Arawhata’ is a programme that allows students to enhance their emotional intelligence and self-care skills alongside the academic curriculum (Meadows et al., 2020). This programme integrates tutorials ‘Nga Roopu Awhi’, which refers to ‘shelter in quiet water’ where students have time to think reflectively in a safe environment (Giles and Stanfield, 2017) where students can negotiate their academic and social work professional worlds.
While SSW can develop innovative responses to students’ needs, as described in the He Arawhata programme (Giles and Stanfield, 2017; Meadows et al., 2020), mental health services on campus require improved institutional responses (Gair and Baglow, 2018a; Gharibi, 2018; McAuliffe et al., 2012). Aligned with Todd et al.’s point about avoiding overreliance on labelling, Martin (2010) urges universities to adopt a wellness rather than a deficit-based approach. McAuliffe et al. (2012) argued that a ‘whole-of-university’ approach requires clear guidelines for responses to mental distress, with training for academic staff to recognise and respond to mental distress (Martin, 2010). Reid and Poole (2013) assert that educators should create the conditions for the safe disclosure of mental distress.
Conclusions
My advice would be that you have to expect the unexpected, you have to be prepared to be adaptable, and your tenacity and your focus to get this degree …you’re constantly reminding yourself the reasons that you’re doing it and that it’s your passion to do it that keeps you going. Sometimes that is the only thing that keeps you going [Doreen]
Our findings reflect students' struggles and their determination to persevere, which should not go unnoticed. Nor should we accept that this is how things ‘have to be’. It is important to critically interrogate the reliance on education about self-care as a solution. In a recent systematic review of self-care literature in social work, Barks et al. (2023) reported the inaccessibility of self-care and questioned its relevance to all social workers. None of the articles in their review focused on structural or institutional factors in social workers’ professional lives. They note that ‘investigated without the sociopolitical and historical context, [self-care practices] have been used to blame people who are experiencing the consequences of centuries of sociostructural oppression for distress and psychosocial challenges’ (p. 15). This argument applies equally to social work students. Educators and professional bodies must be willing to put a range of options on the table to address these challenges, not relying on self-care training that renders invisible the structural inequalities that are present for some students throughout their studies and may as a consequence produce stigma. We must strive to avoid the casualties – the silent group who do not struggle on, who fall away, left with debt, disappointment, and unmet aspirations. To do nothing is to fall short on our ethical obligations.
We echo the thoughts of Gair and Baglow (2018c), ‘Do we practice what we preach?’ which highlights the disconnect between our focus on advocacy and social justice and the lived realities of student participants in their research and who wryly observe: While universities maintain their self-congratulatory stance on enabled tertiary access for working class, mature-aged and minority student groups, the realities may be that entrenched inequalities remain largely unchallenged (Gair and Baglow, 2018c: p.214).
To maximize success, increased support for students must consider the intersections between study and life circumstances, acknowledging the structural underpinnings of the stress that students experience, particularly those already in poverty.
Footnotes
Acknowledgements
Moya Baker (Ngāpuhi, Mangaia (Cook Islands) was supported by a University of Auckland Summer Scholarship and Kendra Cox (Te Ure o Uenukukōpako, Te Whakatōhea, Tūhoe, Ngāti Porou) was supported by a research grant in the Faculty of Education and Social Work, University of Auckland. We also acknowledge the many students who shared their struggles and strategies by participating in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.