
Abstract
Introduction
Despite abundant literature on the diagnosis of dementia, limited research has explored the lived experiences of radiography practitioners when providing care to people living with dementia in the department.
Objectives
This qualitative study explored the perceptions and compatibility of current professional guidance by both diagnostic imaging and radiotherapeutic radiography practitioners as well as the key stakeholders involved with developing the Society and College of Radiographers clinical practice guidelines for caring for people with dementia.
Methods
This was a two-phase multi-method study. Fifteen diagnostic imaging and two therapeutic radiography practitioners from across the UK participated with online focus group discussions. Four key stakeholders involved with the development of the Society and College of Radiographers guidelines took part with individual semi-structured interviews. Data analysis included narrative and thematic analysis.
Results
Participants from both phases identified enablers and barriers to providing person-centred dementia care. Three superordinate themes were identified linked to (1) Working with care partners, (2) Departmental environmental design, and (3) Communication and interprofessional infrastructure.
Discussion
Many radiography practitioners still feel unprepared when caring for people living with dementia despite the clinical practice guidelines. Care partners were identified as having the potential to help alleviate some of the challenges radiographers faced. Participants were also aware of the impact of the departmental environment and recognised that poor way finding designs could lead to frustration. Radiography practitioners were not always aware that a patient was living with dementia prior to their attendance in the department making it difficult for practitioners to make appropriate accommodations such as additional time at appointments or the departmental environment. Our findings suggest there is a need for profession specific education and training for radiography practitioners to support the provision of person-centred dementia care. There is also a need to support the design of dementia friendly diagnostic imaging and radiotherapy departments.
Introduction
People living with dementia may attend radiography service providers for a variety of reasons including diagnostic imaging for differential diagnosis as well as for injuries and pathologic conditions. They may also attend radiotherapy departments for co-morbid cancer treatment (Chang et al., 2016; Griffiths et al., 2015). It is estimated that approximately 850,000 people are currently living in the United Kingdom (UK) with dementia and given this number is projected to increase this will likely place a further strain on radiography services across the UK (Alzheimer’s Research UK, 2021; The Society and College of Radiographers (SCoR), 2020). Regulation in the UK requires that all healthcare professionals, including radiography practitioners, provide person-centred care (Care Quality Commission (CQC), 2014).
The philosophy of person-centred care is essential for good dementia care and is built around the needs of the individual and contingent upon knowing the person through an interpersonal relationship. It challenges the traditional medical model of care that tends to focus on processes, schedules, staff and organisational needs (Fazio et al., 2018). Brooker (2004) outlined four key components that are integral to a person-centred care approach for people living with dementia which include (a) valuing and respecting persons with dementia and those who care for them; (b) treating people living with dementia as individuals with unique needs; (c) seeing the world from the perspective of the person living with dementia, so as to understand the person’s behaviour and what is being communicated; and (d) creating a positive social environment in which the person living with dementia can experience relative well-being through care that promotes the building of relationships. Brooker (2006) expanded upon these components and identified key indicators or practices for each of the four components which included communicating effectively, treating individuals with respect and supportive and inclusive physical and social environments.
There are two branches of radiography: Diagnostic and Therapeutic. Although there are similarities between diagnostic and therapeutic radiography practitioners such as the use of specialist technology and the delivery of person centred care, there are some notable differences. For example, diagnostic radiographers produce medical images using a range of modalities and may typically have limited contact time with patients, whilst therapeutic radiographers treat patients with cancer using radiation and are involved with the patient from planning to treatment stages (College of Radiographers, 2022). However, clinical protocols used to treat and care for people living with dementia vary, resulting in inconsistent training or guidelines for health professionals which may potentially compromise the quality of care provided to people living with dementia when attending diagnostic imaging or radiotherapy service providers (Chang et al., 2016). This may have implications for radiographic practice and the delivery of person-centred dementia care. Diagnostic and therapeutic radiography practitioners have distinct different roles - diagnostic radiographers produce and process images of body structures to support a diagnosis or guide direct interventional treatments, procedures and therapies, whilst therapeutic radiographers treat patients with cancer using radiation and will be planning process, treatment and eventually post-treatment review (follow-up) stages – there are similarities in that both use specialist technology and are patient-focused.
For example, when arriving in a diagnostic imaging department, people living with dementia may exhibit behaviours that radiography practitioners find to be unpredictable (Chang et al., 2016). Frustration, along with an inability to comply with or understand instructions when undertaking diagnostic imaging procedures, can manifest as aggressive behaviour, making it difficult for the radiographer to provide adequate care or establish and sustain rapport, especially as diagnostic imaging can last between 15 and 30 min (Chang et al., 2016; SCoR, 2020). Although policy and research in this area is growing there is still a gap in the evidence base reaching practice where it is needed with many radiography practitioners reporting feel grossly underprepared when caring for people living with dementia (Miller et al., 2019; SCoR, 2020; Smith et al., 2019).
Key findings from the existing literature have focused on professional attitudes towards dementia and identified that people living with dementia can receive poor patient care or negative experiences when attending radiography services (Booth et al., 2017; Challen et al., 2018; Chang et al., 2016; Kada, 2009; Miller et al., 2019; SCoR, 2015; SCoR, 2020; Wolf & Gunderman, 2020). Despite the current clinical practice guidance produced by the SCoR and the recognition of the importance of the patient experience of people living with dementia and their care partners when undergoing diagnostic imaging and/or radiotherapy procedures little research has explored the lived experiences by radiography practitioners when caring for people living with dementia and their interactions with care partners.
The aim of this study was therefore to explore the recounted experiences of both diagnostic and therapeutic radiography practitioners in the UK when providing care for people living with dementia. It also sought to investigate the compatibility of these findings with the perspectives of key stakeholders involved in developing the SCoR ‘Caring for people with dementia’ guidelines (SCoR, 2020).
Methods
Design
This was a multi-method, two phase (online focus groups followed by individual semi-structured interviews) qualitative research study. An inductive qualitative approach was taken as the study sought to explore the recounted experiences and perspectives by participants.
Sampling and recruitment
Phase 1 used purposive sampling to recruit Health and Care Professions Council (HCPC) registered qualified diagnostic and therapeutic radiography practitioners of any professional background/role based on the College of Radiographers (CoR) Career Framework for diagnostic and therapeutic radiographers (assistant practitioner, diagnostic or therapeutic radiographer, advanced practitioner, and consultant radiographer) and years of experience from across the UK. Pre-qualification student radiography practitioners were excluded from this study. Recruitment of participants was conducted via social media and by word of mouth. Phase 2 used convenience sampling to recruit participants identified as members of the core group involved with the development of the SCoR ‘Caring for people with dementia’ guidelines (SCoR, 2020). Pre-qualification student radiography practitioners were excluded from this study.
Consent
Two versions of Participant Information Sheets (PIS) were used. The same core information about the study was included but as the methods used to gather data were different, we were required to use different versions by our ethics committee. Each PIS explained issues relating to anonymity, confidentiality, withdrawal from study and a debriefing process should the online focus group or interview cause any anxiety. For the online focus groups anonymity was preserved by ensuring that no real names or other directly identifying information were used (Sim & Waterfield, 2019). Only on actively consenting with each phase were participants able to access the online focus groups or take part with the individual semi-structured interviews. This included agreeing to maintain the confidentiality of the other participants and to not repeat opinions outside of the online focus group.
Ethics
Ethical approval for the study was granted by the University of Salford Ethics Committee (23/11/2020).
Data collection and management
Phase 1
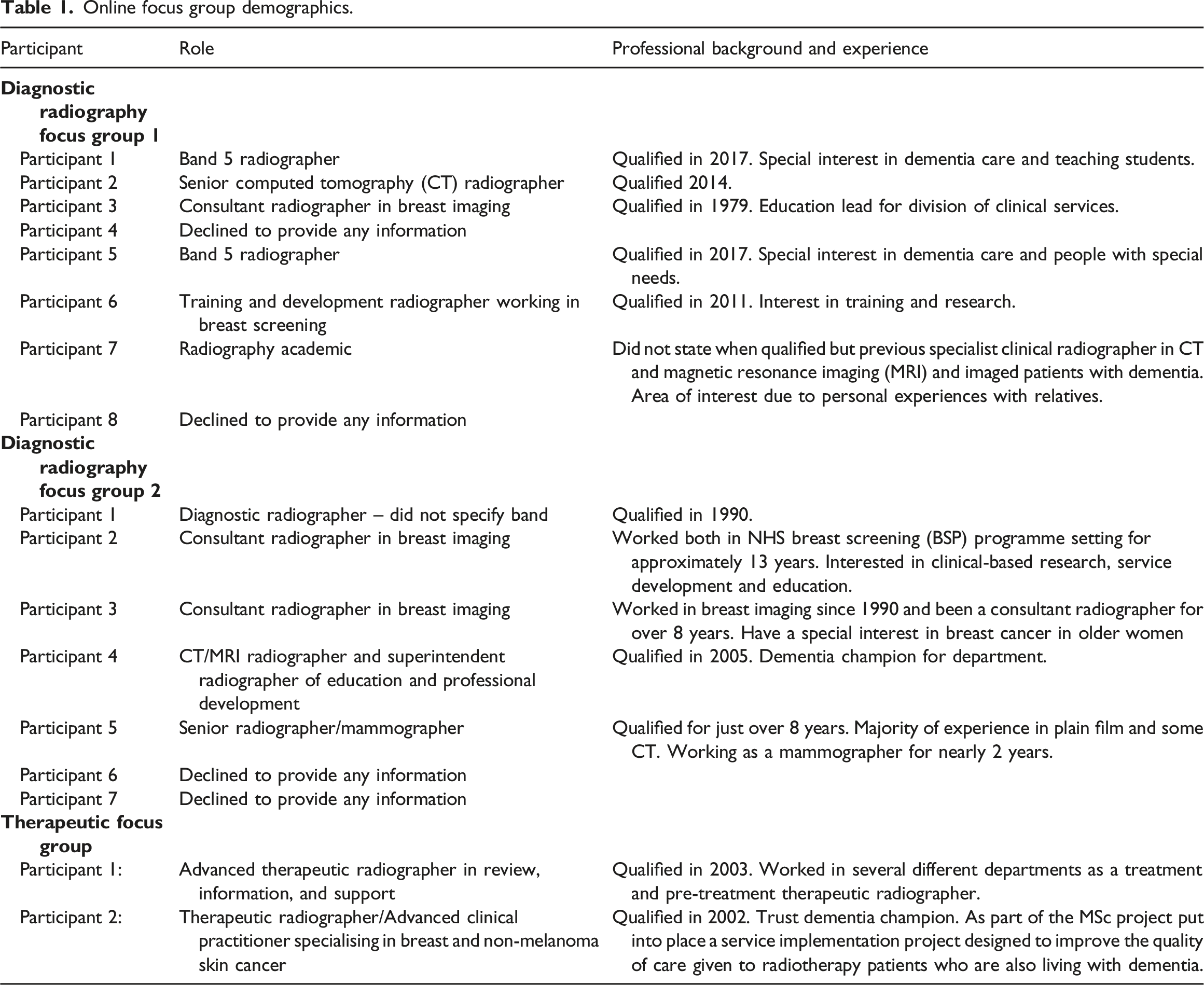
Online focus group demographics.
Phase 1 online focus group questions.
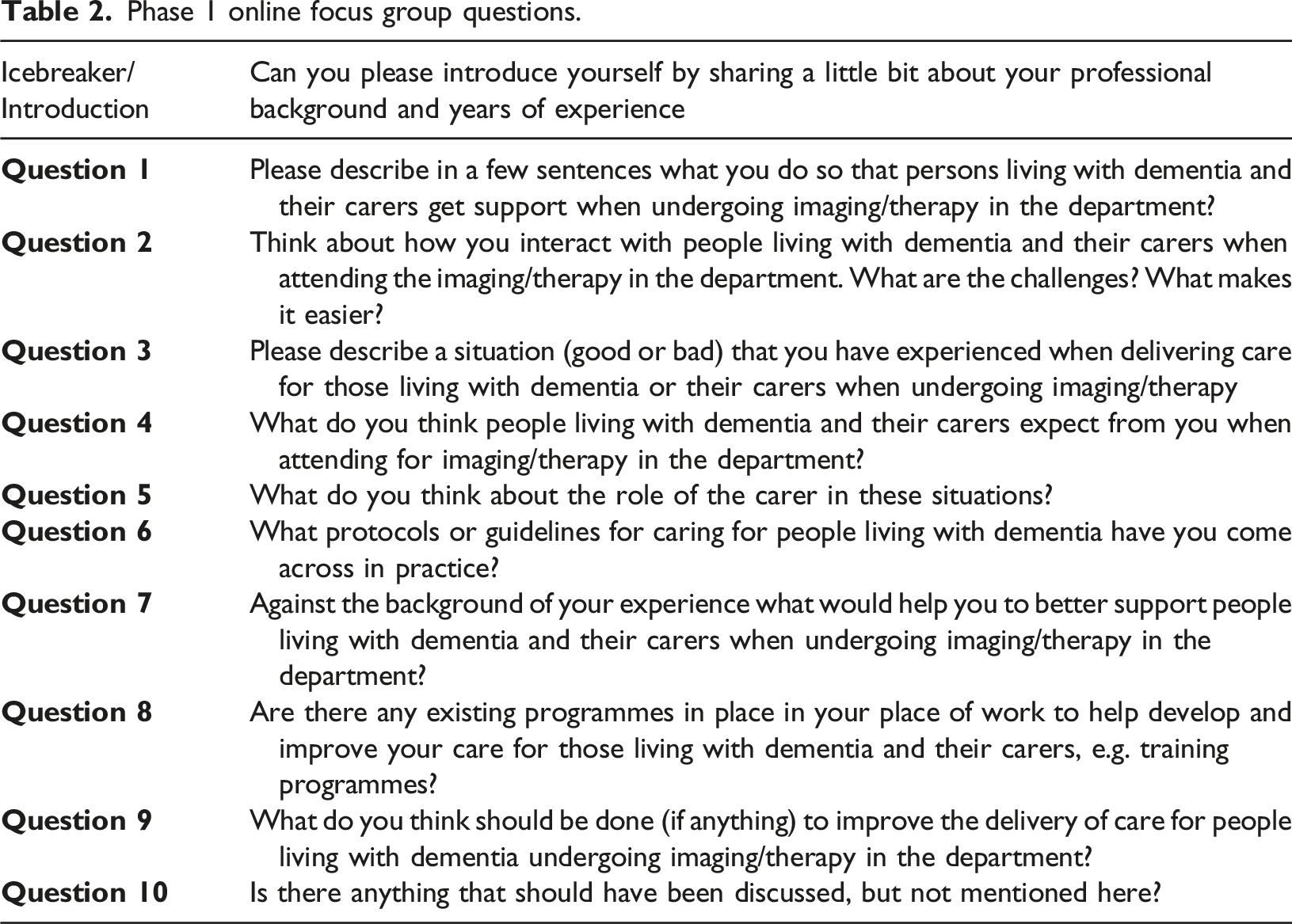
Fifteen diagnostic radiographers were recruited and divided into 2 homogenous focus groups (8 and 7 participants respectively). This was to reflect the contextual differences between therapeutic and diagnostic radiography practitioners and allow common experiences to be shared and built upon. Only 2 therapeutic radiographers took part. However, the data gained from this focus group was found to be in-depth and sufficient for the objectives of this study. Author 1 acted as moderator and monitored each online focus group as well prompting any further discussions. Each online focus group ran for 4 weeks and closed at the point of data saturation (Saunders et al., 2018).
Phase 2
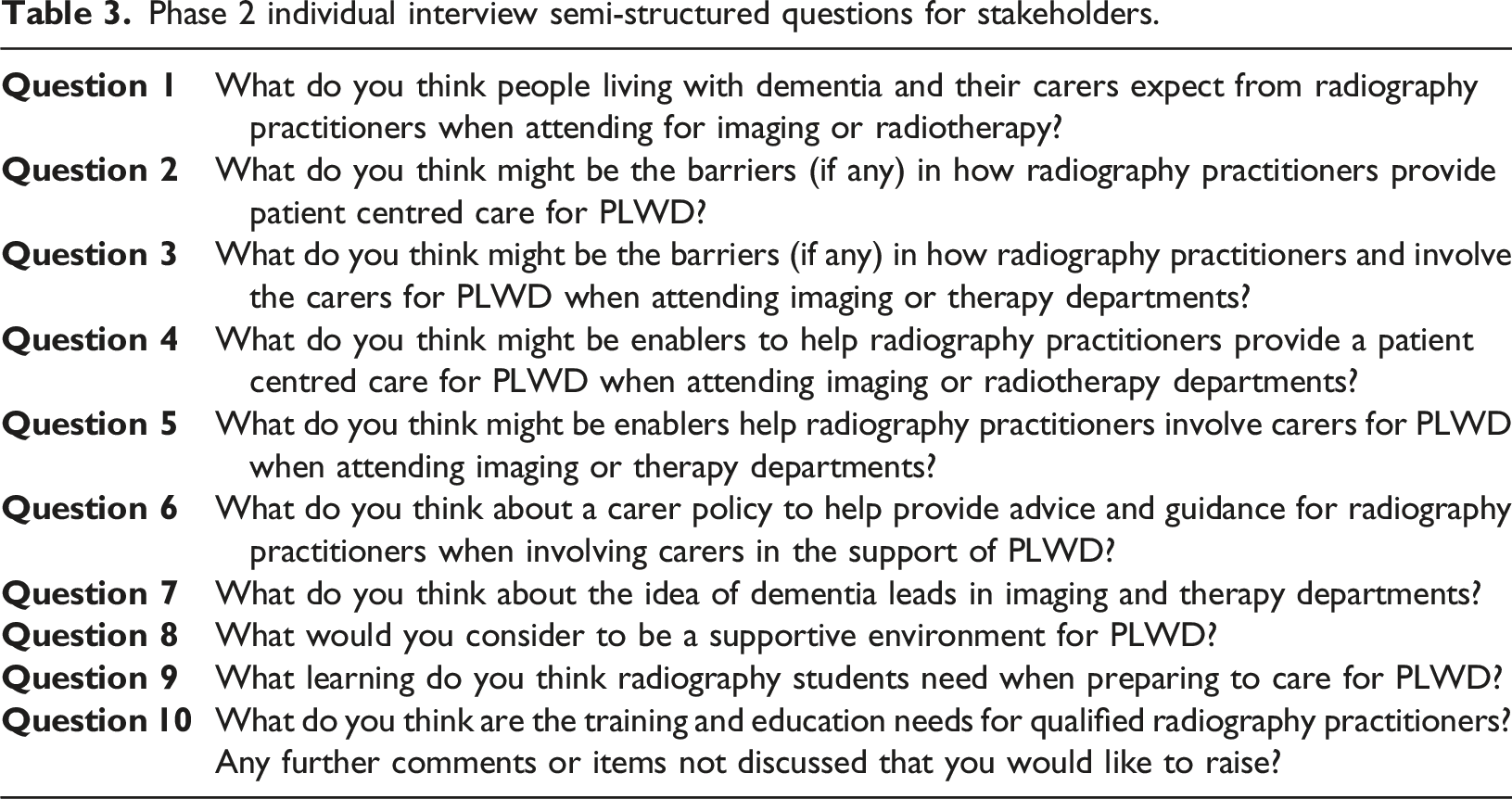
Phase 2 individual interview semi-structured questions for stakeholders.
Analysis
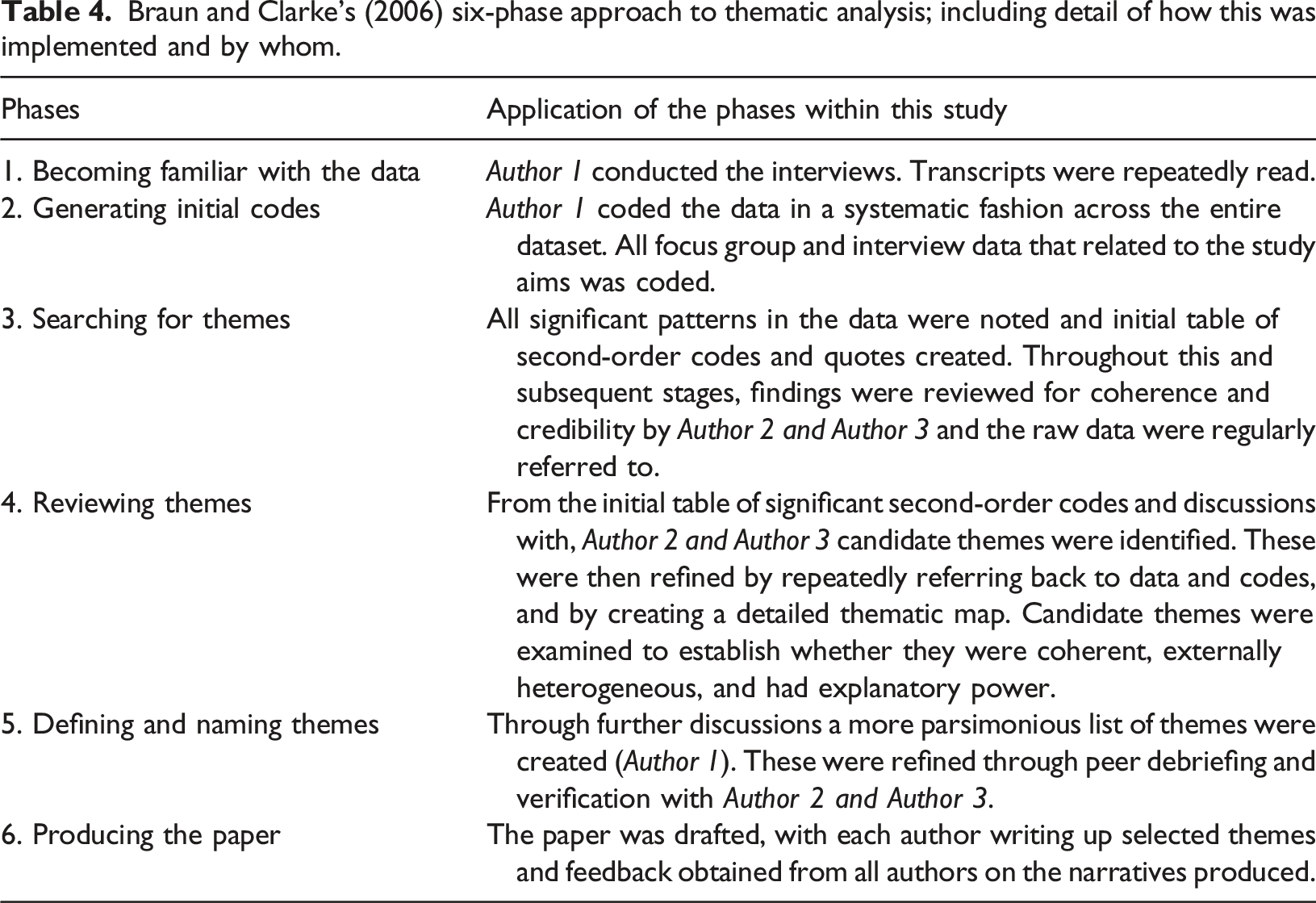
Braun and Clarke’s (2006) six-phase approach to thematic analysis; including detail of how this was implemented and by whom.
Findings
Findings identified both enablers and barriers to optimising radiographic care to people living with dementia across both phases. Three superordinate themes (1) Working with care partners, (2) Departmental environmental design, and (3) Communication and interprofessional infrastructure were identified that overarched six subordinate themes: care partners as an asset, delimiters to partnership working with carers, physical space, patient wayfinding, interprofessional communication and lack of knowledge about the patient. These themes were identified across both data sets/phases and are referred to within the SCoR caring for people with dementia guidelines (SCoR, 2020). Within the presentation of findings below, the following codes have been used to denote the focus group (Phase 1) and semi-structured interview participants (Phase 2):
Phase 1: • DR = Diagnostic Radiographer Focus Group • TR = Therapeutic Radiographer Focus Group
Phase 2: • Interview Participant
Theme 1: Working with care partners
Working with care partners was commonly recognised by all participants as being central to delivering person-centred dementia care when performing diagnostic imaging or treating people living with dementia. For the purpose of this study the term care partner is a holistic term used to denote someone who provides help and support to a person living with dementia and includes, partner, relative, friend or healthcare professionals such as nursing staff or care home assistants. Most participants recognised and valued the role care partners provided by highlighting how they involved the care partner:
Participants felt it was important to recognise that people living with dementia should be the main focus during diagnostic imaging or radiotherapy procedures, whilst supporting the care partner’s needs:
Several benefits of care partner inclusion were evident throughout the data analysis. For example, participants recognised that often care partners have in depth knowledge of the people living with dementia and can therefore support the radiography practitioner:
Despite these benefits, several challenges to care partner inclusion were identified by the participants, including the ability to recognise when or when not to include a care partner during diagnostic imaging or radiotherapy treatment. Specifically, participants noted that care partners could either be an asset or a hindrance depending on their relationship with the person living with dementia. For example, one participant highlighted that a care partner that has a poor relationship or had only just met the person living with dementia could hinder the provision of person-centred dementia care:
Despite this, our findings suggests that participants felt that by including care partners who have a good relationship with people living with dementia, they can assist radiographers in obtaining images or help to provide reassurance during setting up for radiotherapy to support the delivery of person-centred dementia care:
Participants noted a lack of guidance and policy regarding care partner inclusion explaining how and why carers can be included in diagnostic imaging examinations or radiotherapy treatments. Our findings suggests that the absence of any policy and procedures in this area left some participants feeling unsure of their current practice with involving care partners despite the SCoR guidelines advocating carer inclusion. This may suggest a lack of awareness, familiarity or agreement with the SCoR dementia guidelines:
Moreover, given the potential impact on care partners themselves, it was expressed by participants that care partners should also have an active role in the development of policy and guidelines. It was also highlighted by participants that the guidance should include a safeguarding element to support the minority of cases where care partners could potentially have a negative effect on people living with dementia when attending for diagnostic imaging or radiotherapy:
Theme 2: Departmental environmental design
Participants discussed the physical environment and how it was not always conductive to people living with dementia and the notion of dementia friendly environments generally. Specifically, this was linked to hospitals and the lack of adequate sign posting for people living with dementia when trying to find the diagnostic imaging or radiotherapy department and getting confused and agitated as they struggled to navigate their way to the department or got lost on the way. In response to identifying way-finding difficulties one focus group participant described solutions they had found such as:
This same participant felt more needed to be done to improve signage throughout the hospital and argued that:
One of the interview participants also raised issues with making departments dementia friendly:
Participants also discussed changes made to the environment such as a quiet room for people living with dementia:
However, participants also noted that further improvement was still needed linked to the environmental design of the department such as a dementia clock and appropriate signage to help people living with dementia orientate themselves and help with telling the time:
Furthermore, participants stated that resources required to make the required adaptations to improve the physical environment for people living with dementia might be limited due to cost:
Despite Participants acknowledging the importance of dementia friendly waiting areas, they did not provide any detail of their understanding of this and what that this might entail in practice. Participants discussed the importance of other calming measures in the environment that did not require new resources, rather the adoption of careful planning and attention to the individual needs of the person living with dementia, such as music playing and adjusting the lights to provide a sense of safety and comfort. One of the diagnostic radiographer focus group participants argued that their hospital needed to go further:
This demonstrated an understanding of the tokenism by the participants that may be present when using the buzz words of ‘dementia friendly environments’ in the hospital setting. Promoting safety in the environment was also discussed with risks of absconding and falls mentioned most frequently by participants:
Participants raised the need to monitor people living with dementia when attending for diagnostic imaging or radiotherapy to help prevent this happening if family members were not present. Once people living with dementia reached the waiting room, and in the absence of safe, enclosed spaces one participant described measures they took to support the people living with dementia to stay in the waiting room until their appointment:
Theme 3: Communication and interprofessional infrastructure
Good communication with people living with dementia was seen as central to person-centred dementia care along with providing privacy, dignity and respect by the participants. This was to ensure not only patient compliance with procedures but also to provide reassurance and aid patient understanding of the procedure leading to a positive outcome:
Communication with family members or care partners was also seen as being important by participants:
People living with dementia may have problems expressing language which can prove frustrating for both the person living with dementia and the radiography practitioner. This is an important consideration as dementia affects the areas of the brain that enables people to verbalise or identify the right words and to understand what is being said (Hobson, 2019). This was emphasised by participants linked to compliance or obtaining consent:
Other factors thought by participants to impact on communication with people living with dementia included restrictions in hospitals due to the recent COVID-19 pandemic resulting in patients attending departments without carers which posed difficulties with communication:
Interestingly, participants seemed to focus on verbal communication rather than body language when interacting with people living with dementia. As verbal skills deteriorate, other forms of communication become more significant as body language may expresses unmet needs, resulting in challenging behaviours (Social Care Institute for Excellence (SCIE), 2020) and this particularly highlighted by the focus group participant:
Participants also identified concerns linked to whether people living with dementia could consent to their diagnostic imaging or radiotherapy treatment:
Issues around the lack of interprofessional communication linked to forewarning of people living with dementia when attending diagnostic imaging or radiotherapy departments were also noted by participants:
Discussion
Findings from our study identified three key themes linked to both facilitators and barriers for radiography practitioners delivering person-centred dementia care which were identified across both phases of the study. These included working with care partners, departmental environmental design, and communication and interprofessional infrastructure, which have also been highlighted in the SCoR caring for people with dementia guidelines (SCoR, 2020). When discussing working with care partners participants were able to recognise and use the knowledge of care partner during diagnostic imaging or radiotherapy treatments. This was found to support the delivery of person-centred dementia care leading to better outcomes for all involved. However, there was also a perception by some participants that there could be issues based on the care partners relationship to the person living with dementia. For example, a family member may know the person living with dementia better and provide more support, as opposed to a ward nurse who may have met them only a few hours beforehand. Issues around poor care partner inclusion by radiography practitioners when caring for people living with dementia have been highlighted before, (Challen et al., 2018) but our findings would seem to indicate a positive shift in radiographers’ attitudes and understanding of care partner inclusion since 2018. Nonetheless, it was evident from our data analysis that there is need for further guidance to be implemented in relation to care partnership working to help sustain a more consistent and evidenced based practice by diagnostic imaging and therapeutic service providers.
Participants were also aware of the impact of the hospital environment on their ability to deliver person-centred dementia care and the difficulties of providing care to people living with dementia in the hospital setting is well documented (Waller & Masterson, 2015). Participants also recognised the impact of the lack of dementia friendly spaces or signage on people living with dementia wellbeing. For example, the potential for people living with dementia to become agitated before they even entered the examination room due to difficulties locating the diagnostic imaging or radiotherapy department. Although, some participants identified the term ‘dementia friendly’ and what this might mean, any improvements seemed to be curtailed by a lack of resource or spending by departments to make these changes. Information exists on how to improve acute wards for people living with dementia (e.g., Brooke & Semlyen, 2019) but the challenge lies with applying this to diagnostic imaging and radiotherapy departments with participants recognising the need to create an environment that avoided unnecessary stress and confusion for people living with dementia but felt constrained in their ability to action these ideas to improve the physical environment.
Participants suggested a way to improve person-centred dementia care would be to have more forewarning in place to identify the need for longer appointment times or time spent communicating with people living with dementia and their care partners. Several barriers were identified by participants linked to the lack of communication that occurred between people living with dementia and the radiography practitioner. However, it was recognised that this was a key element of person-centred dementia care and importance of involving care partners to support radiography practitioners when undertaking imaging or radiotherapy procedures on people living with dementia. Nonetheless, there was a focus by the participants on verbal communication rather than identifying the role of non-verbal cues when caring for people living with dementia. Whilst unusual behaviours might reflect attempts to actively express discomfort by people living with dementia, radiography practitioners may perceive these behaviours as signs of dementia (Veselova, 2013; Desai et al., 2012; Miller et al., 2019) and choose to ignore them. Interestingly, as previously noted by Miller et al., (2017) participants described generic characteristics linked to dementia when recounting their experiences, rather than noting any differences in ‘early’ and ‘later’ stages of dementia during their discussions.
Another challenge identified by the participants concerned the lack of any forewarning linked to cognitive impairment given in advance to help them prepare or make any adjustments for people living with dementia when attending for imaging or radiotherapy service providers. For example, referral requests made by general practitioners (GPs) or medical professionals tended to focus on the reason for referral but excluded information such as making them aware if the patient was known to be living with dementia which restricted any flexibility with providing person-centred dementia care such as longer appointment times or times to avoid sundowning to prevent people living with dementia feeling confused or agitated when attending for imaging or radiotherapy (Dementia UK., 2021). The SCoR caring for people with dementia guidelines (SCoR, 2020) recommend that there should be a question on diagnostic imaging and radiotherapy referral forms that includes a request for information about a person’s type of dementia and cognition, but our findings may suggest that this is not happening in practice.
Radiography practitioners clearly recognised the importance of adapting and providing person-centred dementia care, but our study would seem to suggest there is still a gap in knowledge or training in how to deliver this despite radiography professional guidelines. However, sustaining this type of dementia training may be difficult in a busy department and currently there no role specific tailored training for radiography practitioners linked to delivering person-centred dementia care in the workplace, rather there is currently a reliance on generic materials which may not link theory with radiography practice or workplace experiences (Higgins et al., 2022, 2023).
Limitations
Despite this being a UK nationwide study, recruitment to phase 1 was lower than expected. However, the wide geographical spread of participants supports the representativeness of experience and practice. Participants for phase 1 may have self-selected already having an interest in dementia. However, the study did include perspectives from a range of professional experience and backgrounds. For phase 2 wide recruitment from members of the core stakeholder group was not achieved but nonetheless the data acquired can still be considered relevant in relation to the study aims. It is also important to recognise that social desirability bias may have affected the findings by participants trying to present a positive self by not disclosing certain thoughts or perceptions to avoid embarrassment and repercussions from others (Latkin et al., 2017).
Further work
Future work is suggested to help identify what are areas of a dementia friendly environmental design have the potential to reduce the incidence of agitation by people living with dementia. By identifying what relatively straightforward or inexpensive changes to the design of diagnostic imaging or therapeutic departments can be made to meet the needs of people living with dementia and their carer partners may help to reduce the scepticism that making departments more dementia friendly may be an expensive, time-consuming activity. Further work is also needed to develop role specific tailored training linked to bridge the gap with radiography practitioner workplace learning rather than reliance on generic materials that are currently available to support person-centred dementia care delivery in both diagnostic imaging and radiotherapy departments.
Conclusions
Enablers to delivering person-centred dementia care identified the inclusion of care partners, appropriate communication, and prior identification of people living with dementia as part of the referral process. Dementia friendly environments within departments that not only supported wellbeing but also allowed easy access and way finding were identified as being important in delivering person-centred dementia care. Despite the development of the SCoR caring for people with dementia guidelines (SCoR, 2020) which have been designed to support diagnostic imaging and radiotherapy service providers when caring for people living with dementia our findings suggest that many radiography practitioners may lack knowledge or feel unprepared when providing person-centred dementia care. This may in part be due to a lack of profession linked education and training in this area and recommendations include the development of role specific tailored training to bridge the gap in workplace learning rather than a reliance on the generic materials that are currently available. Other recommendations include more robust referral systems that would help to radiography practitioners make appropriate accommodations when people living with dementia attend diagnostic imaging or radiotherapy service providers and support the delivery of person-centred dementia care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a College of Radiographers Industry Partnership Scheme Research Grant [CoRIPS Research Grant 181].
Ethics statement
Ethical approval for the study was granted by University of Salford Ethics Committee (23/11/2020).