
Abstract
Objective
Renin-angiotensin-aldosterone system inhibitors (RAASi) and beta-blockers decrease cardiovascular (CV) mortality in patients with heart failure and reduced left ventricular ejection fraction (HFrEF) as the dose increases. Mineralocorticoid receptor antagonists (MRA) can also minimize CV mortality. This study aimed to investigate the potential of early administration of additional MRA to insufficient doses of RAASi and beta-blockers.
Methods
Among 609 hospitalized patients with HFrEF, we analyzed 401 patients who received either or both <50% target dose of RAASi and beta-blockers at discharge. They were divided into two groups based on the prescription of MRA: MRA (n = 287) and non-MRA (n = 114). We performed propensity score (PS) matching using diverse parameters at discharge.CV death was the primary endpoint.
Results
Among 401 unmatched patients with HFrEF, Kaplan–Meier analysis for the unmatched population did not show a statistical difference between the MRA and non-MRA groups (log-rank, p = 0.34). However, in the 160 PS-matched population, patients in the MRA group had a significantly lower CV mortality rate than those in the non-MRA group (hazard ratio: 0.29 [95% confidence interval: 0.10–0.79]).
Conclusions
Early administration of additional MRA in patients with HFrEF, even those who received insufficient target doses of RAASi and beta-blockers, may be a therapeutic option.
Keywords
Introduction
Heart failure (HF) is a major public health problem associated with high mortality and prolonged and recurrent hospitalization. Numerous clinical trials have revealed that renin-angiotensin-aldosterone system inhibitors (RAASi), including angiotensin-converting enzyme inhibitors (ACEi) or angiotensin II receptor blockers (ARB), and beta-blockers improve cardiovascular (CV) mortality in patients with HF and reduced left ventricular ejection fraction (LVEF) (HFrEF).1–6 The optimization of RAASi and beta-blockers was associated with lower long-term mortality in HFrEF patients.7,8 Additionally, prior trials have revealed that the prognosis of patients with HFrEF improves as the doses of RAASi and beta-blockers increase.9–12 However, the dose of these medication do not necessarily reach the target dose in real clinical practice. 13 The reasons for this are assumed to be patients’ blood pressure, heart rate, renal function, heart failure status and physician's clinical inertia.
The use of mineralocorticoid receptor antagonists (MRA) has been shown to be effective in reducing CV mortality in patients with HFrEF.14–16 While previous guidelines recommended initiating RAASi and beta-blockers, then considering MRA addition for persistent symptoms/reduced ejection fraction, 17 current recommendations advocate using four medication classes (RAASi/angiotensin receptor-neprilysin inhibitors (ARNI), beta-blockers, MRAs, sodium-glucose co-transporter-2 inhibitors (SGLT2i)) as first-line HFrEF therapy.18–20 Although dosing remains important, the variety of medication types is also recognized as crucial. However, few reports have evaluated the prognostic effect of additional MRA in patients treated with underdosing of RAASi and beta-blockers. Therefore, this study aimed to investigate whether an additional dose of MRA in patients with HFrEF who receive insufficient doses of RAASi and beta-blockers affects CV mortality.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Study population and endpoints
This observational study initially included 1350 consecutive patients who were hospitalized for HF at Tokyo Women's Medical University Hospital between June 2013 and April 2017. Patients were diagnosed with HF using the Framingham Heart Failure diagnostic criteria. 21 We excluded patients with preserved LVEF (≥50%) and mildly reduced LVEF (40%–49%), those who underwent regular hemodialysis, died during the index hospitalization, were lost to follow-up after discharge, and remained in the hospital at the time of the investigation. In the next step, we excluded patients (i) who received either or none of RAASi and beta-blockers at discharge and (ii) who received both RAASi and beta-blockers and the doses of both medications were ≥50% of the target doses at the time of discharge. We ultimately analyzed patients who received both RAASi and beta-blockers at discharge, but the dose of either or both medications was <50% of the target dose. The definitions of the target doses of each medication in this study are shown in the Supplemental Table 1. Patients were divided into two groups based on the prescription of MRA at discharge: the MRA and non-MRA groups. As this was a non-randomized study, propensity score (PS) matching was used to balance distributions of covariates (age, sex, BMI, diabetes, history of percutaneous coronary intervention, LVEF, systolic blood pressure, levels of hemoglobin, albumin, eGFR, sodium, CRP, and BNP at discharge) between the MRA and non-MRA groups (details below). The primary endpoint of this study was CV death, which included death resulting from acute myocardial infarction, sudden cardiac death, death due to HF, stroke, CV procedures, CV hemorrhage, and other CV causes. The study protocol was approved by the University Hospital's Ethics Committee (No. 2020-0028), and patient enrollment was carried out according to the principles of the Declaration of Helsinki. Written informed consent was waived because of the retrospective design of the study.
Data collection and follow-up
For each patient, we collected data on the medical history along with medication use and the following parameters at discharge: (1) vital signs; (2) body weight, height, and body mass index (BMI); (3) oral medications; and (4) laboratory values including hemoglobin, albumin, total bilirubin, C-reactive protein (CRP), renal functions (blood urea nitrogen, creatinine, and estimated glomerular filtration rate [eGFR]), serum sodium concentration, serum potassium concentration and brain natriuretic peptide (BNP). LVEF was evaluated by echocardiography during the index hospitalization. The parameters listed above were compared among subgroups. After discharge, outpatient visits were scheduled once at least every two months, as well as according to their medical needs, and patients were contacted by telephone if they missed a scheduled hospital visit.
Statistical analysis
Continuous values were presented as mean ± standard deviation (SD), and categorical data were presented as numbers and percentages. The independent Student's t-test and the non-parametric equivalent Mann–Whitney U test were used to compare the data of the two groups. The chi-squared test and Fischer's exact test were used to compare the categorical variables between the groups. CV mortality was evaluated using the Kaplan–Meier method, and event-free survival curves were compared between the MRA and non-MRA groups using the log-rank test. PS matching was applied to compare CV mortality after discharge between the MRA and non-MRA groups. We used a logistic model to calculate the PS as the individual probability of receiveng the MRA for each individual, based on the following variables: age, sex, BMI, diabetes, history of percutaneous coronary intervention, LVEF, systolic blood pressure, levels of hemoglobin, albumin, eGFR, sodium, CRP, and BNP at discharge. The c-statistic was calculated to assess the discrimination capability of the PS model. PS matching was performed in a 1-to-1 fashion between the MRA and non-MRA groups using calipers of width equal to 0.2 × SD of the logit of PS. 22 The quality of PS matching was evaluated by checking the covariate balance regarding the standardized difference. PS matching was generally considered successful if the standardized differences for all covariates were <0.1. Statistical significance was set at a two-sided p-value of <0.05. Statistical analyses were performed using R software, version 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
We initially included 609 consecutive patients with HFrEF who were hospitalized for decompensation of HF and were discharged alive (Figure 1). Finally, 401 patients who received either or both <50% target doses of RAASi and beta-blockers at discharge were analyzed. Of these 401 patients, 287 patients received MRA at discharge (MRA group), and 114 patients did not receive MRA at discharge (non-MRA group). After performing PS matching, we extracted the data of 80 patients who were adjusted for the clinical background of each group.

Flow chart of participant recruitment and categorization. Abbreviations: HF, heart failure; LVEF, left ventricular ejection fraction; HD, hemodialysis; HFrEF, heart failure with reduced left ventricular ejection fraction; RAASi, renin-angiotensin-aldosterone system inhibitors; MRA, mineralocorticoid receptor antagonist
Baseline characteristics
Table 1 displays the baseline characteristics of the patients in each group before and after PS-matching. After PS matching, a total of 80 pairs was formed, and the baseline covariates, including patients’ clinical profile, medical history, echocardiographic data, and laboratory data, were well balanced between the groups. The average age was 68.0 and 67.2 years for the MRA and non-MRA groups, respectively (p = 0.75). The average systolic blood pressure was 113.5 and 112.9 mmHg (p = 0.83), and the average LVEF was 30.3% and 30.6% (p = 0.82) for the MRA and non-MRA groups, respectively. The average potassium level was within the normal limit of 4.3 mEq/L in the MRA group. Of the 80 patients in the MRA group, 69 patients (86.25%) received spironolactone (the average dose was 30.8 mg/day) and 11 patients (13.75%) received eplerenone (the average dose was 44.3 mg/day) as MRA.
Patient characteristics.

BMI: body mass index; BNP: brain natriuretic peptide; BP: blood pressure; BUN: blood urea nitrogen; CABG: coronary artery bypass grafting; CRP: C-reactive protein; CRT: cardiac resynchronized therapy; eGFR: estimated glomerular filtration rate; ICD: implantable cardioverter-defibrillator; LVEF: left ventricular ejection fraction; PCI: percutaneous coronary intervention; Std diff: standardized difference.
Follow-up data
In the MRA group, 66 of 80 patients could be followed up to two years after the discharge. Of these 66 patients, 58 (88%) patients were prescribed MRA: 45 patients received spironolactone (average dose: 31.3 ± 12.6 mg/day), and 13 patients received eplerenone (average dose: 39.4 ± 13.7 mg/day). Two patients had their prescription switched from spironolactone to eplerenone. The mean follow-up LVEF at two years after discharge was 37.6 ± 10.9% among 66 patients could be followed up (30.3 ± 6.0% at discharge).
In the non-MRA group, 56 of 80 patients could be followed up to two years after the discharge, and 10 (18%) of them received MRA. Of these ten patients, eight received spironolactone (average dose: 31.3 ± 10.8 mg/day), and two received eplerenone (one patient received 25 mg/day and the other 50 mg/day). The mean follow-up LVEF at two years after discharge was 38.2 ± 11.2% among 56 patients could be followed up (30.6 ± 6.1% at discharge).
Prognoses
In 401 unmatched patients with HFrEF, the primary endpoint occurred in 53 patients (13.2%) during the observation period (median follow-up, 735 days). Kaplan–Meier analysis did not show a statistical difference in the CV mortality between the MRA and non-MRA groups (log-rank, p = 0.34, Figure 2(a)). However, in 80 pairs of PS-matched patients with HFrEF, patients in the MRA group had significantly lower CV mortality than those in the non-MRA group (hazard ratio: 0.29 [95% confidence interval: 0.10–0.79], log-rank test, p = 0.026, Figure 2(b)). Combined Kaplan–Meier curves for CV death of the MRA and non-MRA groups in both the pre-matched and post-matched populations are shown in Supplemental Figure 1. There was no statistically significant difference among the four groups (log-rank for trend: P = 0.11).

Cardiovascular mortality of HFrEF patients with or without administration of additional MRA to patients treated with an insufficient dose of RAASi and beta-blockers. Kaplan–Meier event curves for cardiovascular death of (A) before propensity score-matched groups and (B) after propensity score-matched groups. Abbreviations: MRA, mineralocorticoid receptor antagonist
Subgroup analyses were conducted to evaluate sex differences. In the pre-matched cohort, the hazard ratio for MRA receipt versus non-receipt was 0.62 (95% CI: 0.33–1.17, p = 0.14) in male patients. In contrast, the hazard ratio for female patients was 2.75 (95% CI: 0.35–21.71, p = 0.34). There was no significant interaction between MRA use and sex, with a p-value of 0.19, as depicted in Kaplan–Meier curves in Supplemental Figure 2.
In the post-matched cohort, male patients showed a hazard ratio of 0.34 (95% CI: 0.11–1.09) for MRA use. Among female patients, a single event was recorded in the non-MRA group during the study period. Kaplan–Meier curves for this cohort are provided in Supplemental Figure 3. The interaction between MRA prescription and sex demonstrated no significance, with a p-value exceeding 0.99.
Discussion
The principal finding of this study was that the additional MRA administration to patients who received insufficient doses of RAASi and beta-blockers at discharge was associated with a better CV prognosis after discharge in PS-matched population.
In the pre-matched population, patients in the MRA group were significantly younger but had lower systolic and diastolic blood pressure, lower LVEF, and lower creatinine levels at discharge compared to those in the non-MRA group. The overall clinical background tended to be worse in the MRA group than in the non-MRA group. Given the retrospective nature of our study, there was an inherent selection bias regarding the use of MRA, making it challenging to assess the true prognostic impact of additional MRA in patients underdosed with beta-blockers and ACEi/ARB. To mitigate this bias, we employed PS matching to elucidate the potential effects of MRA.
Previously, guidelines recommended initiating RAASi and beta-blockers first, followed by MRA for persistent symptoms or reduced ejection fraction. 17 Consequently, MRA prescription rates were lower than those for RAASi and beta-blockers, despite evidence linking MRAs to improved long-term outcomes in HFrEF. 13 However, current guidelines advocate the use of four medication classes—RAASi/ARNI, beta-blockers, MRAs, and SGLT2i—as first-line therapy for HFrEF, reflecting an evolved role for MRAs in guideline-directed medical therapy (GDMT).18–20
The STRONG-HF trial investigated the efficacy and tolerance of an intensive treatment strategy involving rapid up-titration of GDMT and close follow-up after an acute heart failure admission. The study included patients prescribed ≤1/2 the optimal dose of RAASi/ARNI, no beta-blocker, and ≤1/2 the optimal dose of MRA, or no RAASi/ARNI, ≤1/2 the optimal dose of beta-blocker, and ≤1/2 the optimal dose of MRA. 23 The trial demonstrated that this intensive treatment strategy reduced symptoms, improved quality of life, and lowered the risk of mid-term all-cause mortality or HF readmission compared to usual care. Our study's results align with this new concept. Specifically, we focused on HFrEF patients discharged on less than 50% of the target doses for RAASi and/or beta-blockers, representing insufficient GDMT. Adding MRA was associated with lower CV mortality, underscoring its importance as part of an intensive treatment strategy post-discharge. This supports the current positioning of MRA as first-line therapy under the latest guidelines, as opposed to its previous second-line status.
The main challenges in increasing the doses of RAASi and beta-blockers in these patients include symptomatic hypotension, worsening renal function, hyperkalemia, and bradycardia. The addition of MRA can also induce hypotension24–26 and hyperkalemia. 27 Consequently, patients intolerant to up-titration of RAASi or beta-blockers may face difficulties in receiving additional MRA. However, in our study, within the PS-unmatched population, patients in the non-MRA group had higher blood pressure than those in the MRA group. Heart rate and serum potassium levels were not significantly different between the MRA and non-MRA groups. Furthermore, 82.5% of patients in the MRA group were followed up for two years post-discharge, with 88% continuing MRA therapy during this period. These findings suggest that some patients may be receiving insufficient doses of RAASi and beta-blockers without MRA due to clinical inertia, despite being eligible for MRA treatment.
We conducted subgroup analyses to assess sex differences in MRA effectiveness. There were no statistically significant interactions between MRA use and sex in both pre-matched and post-matched cohorts. In the male cohort, patients in the MRA group tended to exhibit a better prognosis compared to those in the non-MRA group. Conversely, in the female cohort, the trend was the opposite. Although the number of post-matched female patients was particularly limited in this study, it underscores the importance of further analyzing this potential difference with a larger cohort of female patients.
The other important point of this study was that it included “hospitalized” patients due to decompensation of HF. Previous large randomized trials which clarified the effectiveness of medication for HF included “outpatients” with “chronic” HF. This study highlighted the important concept of considering hospitalization for decompensation of HF as an opportunity to initiate medications for HF. Our findings align with the STRONG-HF trial's novel GDMT concept, supporting early MRA initiation in eligible HFrEF patients, even before achieving target doses of other medications. While limited by its retrospective, single-center design, this study provides a rationale for prospective evaluation of early intensive GDMT strategies, potentially improving outcomes for HFrEF patients.
Study limitations and strengths
The study has several limitations. First, its retrospective, single-center nature with a small patient sample over a limited period restricts the generalizability of findings and impedes long-term outcome assessment and evaluation of sustained benefits of early MRA administration. Our final analysis included 80 matched pairs from an initial cohort of 1350 heart failure patients. This reduction was due to lower MRA prescription rates under previous guidelines and significant differences in patient backgrounds between MRA and non-MRA groups. While these factors may limit statistical power and generalizability, our study's strength lies in its focused approach on patients receiving underdosed beta-blockers and ACEi/ARB. This narrow focus, while constraining broad applicability, provides valuable insights into a common clinical scenario in HFrEF management. Our findings offer practical guidance for medication optimization following heart failure hospitalization, addressing frequently encountered situations in HFrEF treatment. Second, although covariates for propensity score matching were selected based on clinical relevance and previous literature, the possibility of unmeasured and unknown variables influencing the results must be acknowledged. Third, we did not consider whether patients were naïve to medications at the time of the index hospitalization or had previously received the medications. Fourth, although we analyzed patients with <50% of either or both RAASi and beta-blockers, we did not analyze why the doses of RAASi and beta-blockers did not increase. Fifth, target doses of RAASi and beta-blockers in the current study are relatively low compared to those in prior trials. Target doses of RAASi and beta-blockers according to the guidelines of the Japan Circulation Society are lower than those recommended by the guidelines of ACC/AHA,18,28 which could be attributed to the petite physique of Asian patients than that of Western patients. Therefore, the findings of the present study may not be realized for Western patients. The average doses of RAASi and beta-blockers received by the patients in each group are shown in Table 2. Sixth, This study did not include Angiotensin receptor neprilysin inhibitors (ARNI) as a RAASi because ARNI was not approved for HF patients during the study period. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) were not also investigated for the same reason. In the latest guidelines of ACC/AHA and the European Society of Cardiology for HF, ARNI and SGLT2i are recommended as the first-line medications to treat patients with HFrEF. However, the effects of these medications on the results of this study are not known.
Details in beta-blockers and renin-angiotensin-aldosterone system inhibitors.
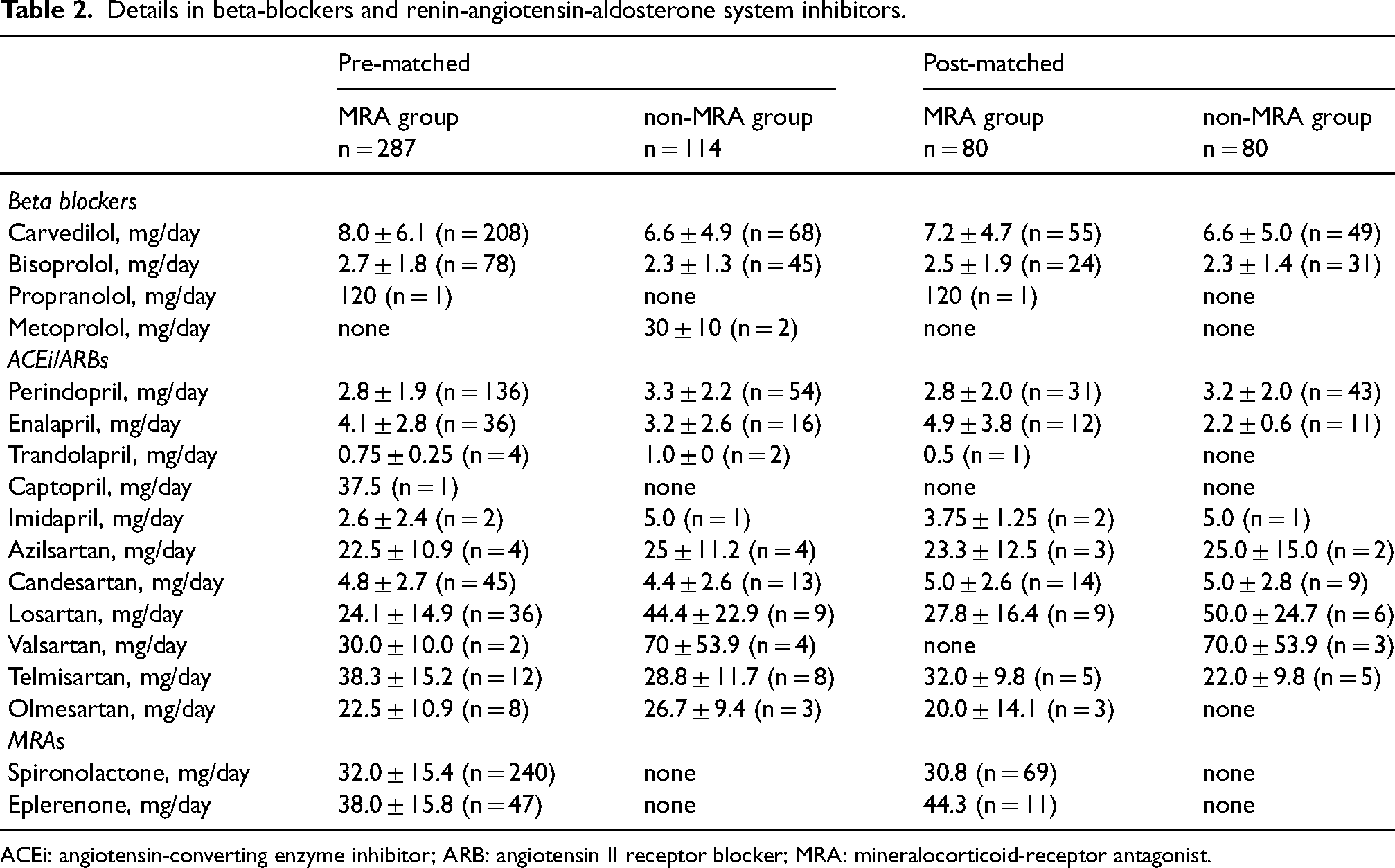
ACEi: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; MRA: mineralocorticoid-receptor antagonist.
Despite its limitations, this study is pioneering in reporting the administration of additional MRA, a crucial member of the ‘fantastic four’, to patients treated with suboptimal doses of RAASi and beta-blockers. Current guidelines advocate for the strategy of initiating and rapidly up-titrating RAASi (including ARNI), beta-blocker, SGLT2i, and MRA prior to discharge for heart failure patients.18–20 Therefore, our research offers valuable evidence bolstering these recommendations.
Seventh, eleven and three patients received Olmesartan as RAASi in the pre-PS and post-PS matching populations, respectively. However, despite the limited data on the beneficial effects and known limitations for its selection in patients with HFrEF, Olmesartan might have been administered to the patients due to its antihypertensive effects. Despite these limitations, the results of this study provide important information that may assist in developing clinical strategies for the management of patients with HFrEF. Prospective studies with larger sample sizes are warranted to confirm these findings and determine an optimal treatment strategy for HFrEF patients not achieving target doses of RAASi and beta-blockers.
Conclusions
According to this observational study, in patients with HFrEF who were treated with insufficient doses of RAASi and beta-blockers, receiving additional MRA at discharge was associated with lower CV mortality. These results indicated that early administration of MRA before reaching the target dose of RAASi and beta-blockers should be considered.
Supplemental Material
sj-docx-1-jra-10.1177_14703203241306037 - Supplemental material for Additional mineralocorticoid receptor antagonists in heart failure underdosed with guideline-directed medication
Supplemental material, sj-docx-1-jra-10.1177_14703203241306037 for Additional mineralocorticoid receptor antagonists in heart failure underdosed with guideline-directed medication by Takuro Abe, Shota Shirotani, Takuma Takada, Ayano Yoshida, Shun Hasegawa, Makoto Kishihara, Noritoshi Fukushima, Katsumi Saito, Junichi Yamaguchi and Kentaro Jujo in Journal of the Renin-Angiotensin-Aldosterone System
Footnotes
Abbreviations and Acronyms
Author contributions
Takuro Abe: Acquisition of data, analysis and interpretation of the data, Drafting of the manuscript. Shota Shirotani: Acquisition of data. Takuma Takada: Acquisition of data. Ayano Yoshida: Acquisition of data. Shun Hasegawa: Acquisition of data. Makoto Kishihara: Acquisition of data. Junichi Yamaguchi: Funding, Supervision. Noritoshi Fukushima: Statistical analysis. Katsumi Saito, Acquisition of data, Funding. Kentaro Jujo: Conception and design of the research, Acquisition of data, analysis and interpretation of the data, Drafting of the manuscript. 1. English proofing: We thank Editage (![]() ) for English language editing. 2. Author agreement: List of all Authors: Takuro Abe, MD; Shota Shirotani, MD; Takuma Takada, MD; Ayano Yoshida, MD; Shun Hasegawa, MD; Makoto Kishihara, MD; Noritoshi Fukushima, MD, PhD; Katsumi Saito, MD, PhD; Junichi Yamaguchi, MD, PhD; Kentaro Jujo, MD, PhD. All authors have seen and approved the manuscript being submitted, have contributed significantly to the work, attest to the validity and legitimacy of the data and its interpretation, and agree to its submission to the Journal of the Renin-Angiotensin-Aldosterone System. We attest that the article is the Authors’ original work, has not received prior publication and is not under consideration for publication elsewhere.
) for English language editing. 2. Author agreement: List of all Authors: Takuro Abe, MD; Shota Shirotani, MD; Takuma Takada, MD; Ayano Yoshida, MD; Shun Hasegawa, MD; Makoto Kishihara, MD; Noritoshi Fukushima, MD, PhD; Katsumi Saito, MD, PhD; Junichi Yamaguchi, MD, PhD; Kentaro Jujo, MD, PhD. All authors have seen and approved the manuscript being submitted, have contributed significantly to the work, attest to the validity and legitimacy of the data and its interpretation, and agree to its submission to the Journal of the Renin-Angiotensin-Aldosterone System. We attest that the article is the Authors’ original work, has not received prior publication and is not under consideration for publication elsewhere.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.