
Abstract
Since the initial discovery of Angiotensin converting enzyme inhibitors (ACEI) in the 1960s and the launch of Captopril as the first available for clinical use in the 1970s, there now exist three other classes of drugs that block the renin angiotensin aldosterone system (RAAS): the angiotensin II receptor blockers (ARB), aldosterone antagonists (AA) and direct renin inhibitors (DRI). With the proven efficacy of RAAS blockers as monotherapy in many arenas there has been considerable interest in the use of dual therapy combinations of these medications that target different points in the pathway. By potentially offering a more complete RAAS blockade with a commensurate enhanced clinical effect, the strong biological rationale for dual therapy has led to it being embraced by clinicians as a treatment option, for hypertension and nephroprotection in particular. However, the initial enthusiasm for this treatment has been tempered by the recent results from several large trials such as ONTARGET and ALTITUDE, which do not support a specific dual therapy approach. In contrast, there is supportive evidence for dual blockade of specific combinations in selected patient groups and data are lacking for others. In the wake of this complex contemporary evidence, the conundrum now faced by clinicians committed to individualised care is, for which patients dual therapy could still be of benefit. This review examines for the practising clinician the current ‘state of play’ for dual blockade of various combinations and a perspective on its use in cardio-renal disease and diabetic complications.
Introduction
The complexity of the renin–angiotensin–aldosterone system (RAAS) is matched only by the myriad recommendations for the use of the blockers of RAAS under various conditions and in combination. Currently available pharmacological agents that block RAAS are the angiotensin converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), the direct renin inhibitors (DRIs) and the aldosterone antagonists (AAs). In a single patient, it is now possible to inhibit renin directly, block the conversion of angiotensin I (AI) to angiotensin II (AII) and to block the major downstream targets of AII. Until recently, the biological rationale for the use of dual RAAS blockade had been so compelling that despite a lack of robust evidence for long-term efficacy and safety, guidelines had recommended its use. 1 However, lately, in the wake of the now questionable veracity of a landmark study in support of dual RAAS blockade, the COOPERATE (Combination Treatment of Angiotensin-II Receptor Blocker and Angiotensin-Converting-Enzyme Inhibitor in Non-Diabetic Renal Disease) trial, 2 and the lack of benefit associated with combination RAAS blockade reported by the ONTARGET (ONgoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial) trialists, expert recommendations have taken an about face. ‘Dual RAAS blockade is dead until further notice’ has been a proclamation. 3 Nevertheless, updated congestive heart failure (CHF) treatment guidelines still recommend dual therapy as a viable option, 4 and at the coalface, many endocrinologists continue to observe their nephrologist and cardiologist colleagues’ ongoing use of combination therapy with impunity. Furthermore, as combination of ACEI and ARB has gained popularity in the primary care setting, the question of which patients now require withdrawal of combination therapy arises commonly. Add to this the complexity provided by the recent early termination of the ALTITUDE (Aliskiren Trial in Type 2 Diabetes Using Cardiovascular and Renal Disease Endpoints) study, which examined the DRI/angiotensin converting enzyme (ACE) or ARB combination, and that not all combination RAAS blockade can be considered equal, considerable confusion is inevitable. This review is an attempt to disaggregate the data and to examine the current status for the use of combination RAAS blockade, if any, for the practising clinician. A contemporary guide for the perplexed if you will.
Overview of dual RAAS blockade by treatment and medical indication. Some relevant trial support is mentioned.
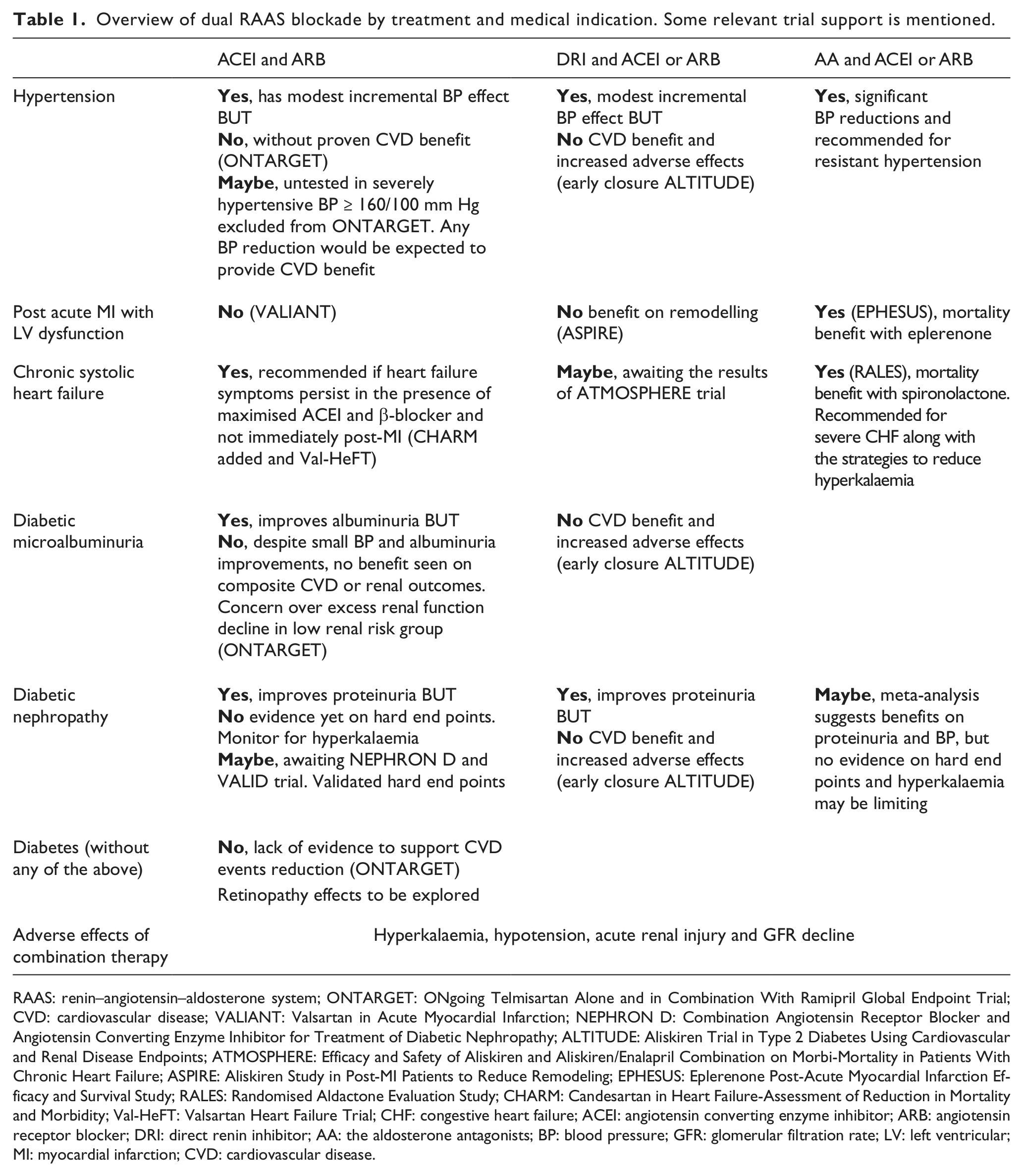
RAAS: renin–angiotensin–aldosterone system; ONTARGET: ONgoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial; CVD: cardiovascular disease; VALIANT: Valsartan in Acute Myocardial Infarction; NEPHRON D: Combination Angiotensin Receptor Blocker and Angiotensin Converting Enzyme Inhibitor for Treatment of Diabetic Nephropathy; ALTITUDE: Aliskiren Trial in Type 2 Diabetes Using Cardiovascular and Renal Disease Endpoints; ATMOSPHERE: Efficacy and Safety of Aliskiren and Aliskiren/Enalapril Combination on Morbi-Mortality in Patients With Chronic Heart Failure; ASPIRE: Aliskiren Study in Post-MI Patients to Reduce Remodeling; EPHESUS: Eplerenone Post-Acute Myocardial Infarction Efficacy and Survival Study; RALES: Randomised Aldactone Evaluation Study; CHARM: Candesartan in Heart Failure-Assessment of Reduction in Mortality and Morbidity; Val-HeFT: Valsartan Heart Failure Trial; CHF: congestive heart failure; ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker; DRI: direct renin inhibitor; AA: the aldosterone antagonists; BP: blood pressure; GFR: glomerular filtration rate; LV: left ventricular; MI: myocardial infarction; CVD: cardiovascular disease.
The RAAS: an overview
The RAAS plays a central role in the regulation of blood pressure (BP), plasma volume and sympathetic nervous system activity to maintain organ perfusion. The traditional view of the renin–angiotensin hormonal cascade begins with the hormone renin, a protease produced by the juxtaglomerular cells and its substrate angiotensinogen produced by the liver. Renin stimulation is via a number of inputs, such as sodium concentration in the distal tubule, intravascular pressure at the glomerulus afferent arteriole, angiotensin levels and sympathetic activity. The action of renin on angiotensinogen is to produce the largely inert AI. Subsequent activation of AI to the vasoactive AII is by the action of ACE produced by the lungs. AII via its actions on the AII receptor(s) results in increased aldosterone production from the adrenal cortex, direct renal vasopressor effects, increased myocardial contractility and sodium and water retention, all leading to increased circulating volume with the net effect being the maintenance of systemic BP. Negative feedback on renin is provided via the increased perfusion of the juxtaglomerular cells, and this completes the classical pathway (Figure 1).
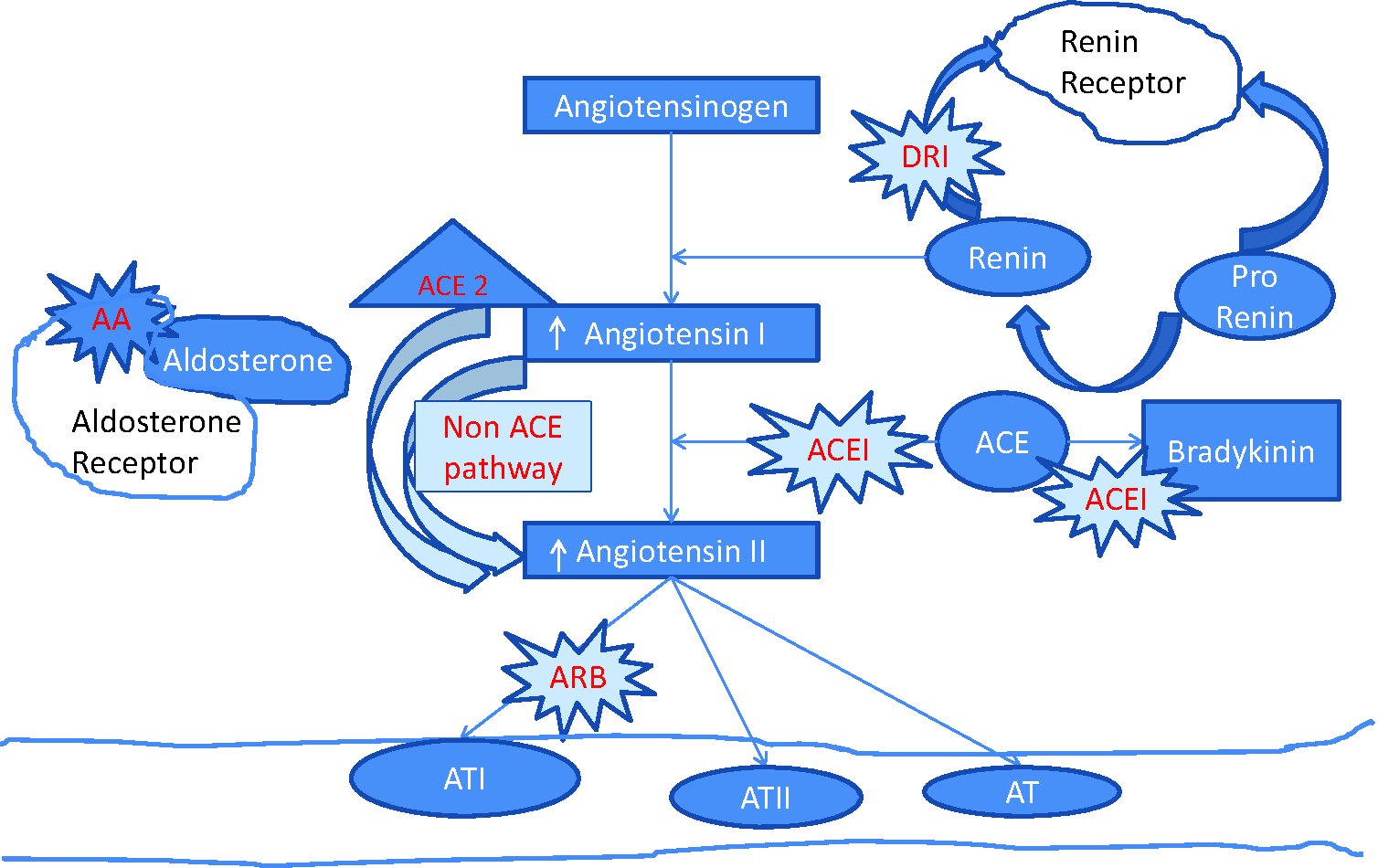
The RAAS and blockers of RAAS.
A contemporary view of the RAAS adds alternative pathways of RAAS activation into the picture with the recognition that AII, in addition to being a circulating hormone, can be produced locally in various organs with local tissue effects via autocrine and paracrine pathways. 6 Aldosterone has also been implicated in the development of fibrosis and arterial and tissue remodelling. More recently recognised are the pro-inflammatory and oxidative effects of RAAS activation resulting in endothelial dysfunction, microalbuminuria and ultimately resulting in cardiac, vascular and renal damage. The existence of these non-ACE-dependent pathways is the proposed explanation of the ‘AII escape phenomenon’ and provides the rationale for the use of combination RAAS blockade as a therapeutic intervention discussed below.
The biologic rationale for dual RAAS blockade
Maladaptive regulation of RAAS has been implicated in the pathophysiology of hypertension, cardiovascular disorders and diabetic complications. Thus, the pharmacological blockade of RAAS remains an important therapeutic target for many of these conditions. It is accepted that monotherapy using RAAS blockade has significant vascular, renal and mortality benefits, which will not be reviewed here. However, if RAAS blockade monotherapy is good, the logical next question is, would combination therapy by acting on different points in the RAAS system be better? The rationale behind dual RAAS blockade was initially based on data showing that ACEI monotherapy resulted in incomplete blockade with AI and renin accumulation and the subsequent ‘escape’ production of AII by non-ACE pathways. 7 Ménard et al. 8 first reported a synergistic effect between ACE and ARB, albeit in a mouse model, and suggested that these two drug classes would overcome the escape phenomenon resulting from incomplete blockade. It was hoped that the addition of an ARB, by attenuating the ‘AII escape’, would provide a more complete blockade of the RAAS and that a complete blockade would translate into better BP control as well as incremental nephroprotective and cardioprotective effects. Since that time, various combinations of dual agent RAAS blockade have been examined and are presented separately hereafter.
RAAS blockade with ACEI and ARB
ACEI/ARB in combination: there is a modest additive effect on BP
BP effects of combination therapy have been examined in essential hypertension, in the setting of isolated systolic hypertension, in diabetic and non-diabetic populations and in the setting of chronic kidney disease (CKD). The combination of ACEI/ARB has been shown in a number of studies to have an additive effect on BP lowering, over and above what can be achieved by monotherapy alone. The caveat here is that many of the studies have been short term and have used sub-maximal dosing of ACE and ARB, and the durability of these effects and outcomes is uncertain. In a meta-analysis, this combination reduced 24-h ambulatory BP monitoring by 4.7/3 mm Hg, compared with ACE monotherapy and by 3.8/2.9 mm Hg compared to ARB monotherapy. 9 In the CALM (Candesartan and Lisinopril Microalbuminuria) trial involving hypertensive, diabetic and proteinuric patients, the combination of candesartan and lisinopril resulted in ~9–11 mm Hg and 5–6 mm Hg reduction in systolic and diastolic BPs, in favour of dual therapy over monotherapy. 10 Thus, there is evidence that dual therapy has an overall additive but modest effect on BP over and above monotherapy, and this had been expected to translate into a significant cardiovascular benefit.
ACEI/ARB in combination: no added benefit on mortality or cardiovascular disease outcomes and increased adverse events
The current landscape has been shaped by the results of the ONTARGET study, a robust non-inferiority randomised control trial involving 25,620 patients at high risk for vascular disease, including over 9000 patients with diabetes. 11 This trial has provided the largest evidence base from which to examine the question whether ACEI/ARB combinations can improve cardiovascular disease (CVD) and mortality outcomes in high-risk patients, including diabetic patients. The study participants were randomised to receive 10 mg of ramipril daily, 80 mg of telmisartan or a combination of both for a median follow-up duration of 56 months. This study showed unequivocally that an ARB, telmisartan, was non-inferior to the ACEI, ramipril, with >90% of the benefit of ramipril preserved. With respect to BP effects and combination therapy, among the whole group, 69% had hypertension, and the reduction of BP was greater in dual RAAS blockade compared to ramipril alone.
Notably, this BP differential did not translate into a CVD or mortality benefit. Dual RAAS blockade with ramipril and telmisartan did not afford a mortality or cardiovascular benefit over and above ramipril monotherapy. In a pre-specified subgroup analysis, there was no benefit seen in the diabetic group nor in hypertensive patients. Furthermore, safety concerns reported in the ONTARGET were primarily hyperkalaemia, symptomatic hypotension and an excess decline in estimated glomerular filtration rate (eGFR), all greater in the combination group. 12 Such data have led expert guidelines to advise that the ‘combination of an ACEI with an ARB is specifically not recommended’ for patients with hypertension. 13 On face value that would seem a reasonable conclusion in the post-ONTARGET landscape, given that combination ACEI/ARB therapy showed no therapeutic benefit and a concerning safety profile. However, the devil is in the detail as they say, and there are a number of caveats and clinical scenarios where the conclusion may not be valid and to assume so may be to the detriment of the patient. These will be discussed below.
ACEI/ARB in combination: possible benefit in the very hypertensive or in those with untreated high residual CVD risk
The ONTARGET trialists included only those with BP ≤ 160/100 mm Hg. For those of us in clinical practice, there are a significant number of patients who present with resistant hypertension with BP values over and above this level. 14 Such patients require and often have already been treated with multi-agent therapy, including ACEI/ARB in combination given their additive effects on BP. In this group, where CVD risk is directly correlated with BP, any BP lowering would be expected to translate to a significant reduction in CVD-related morbidity and mortality; however, the efficacy of dual RAAS blockade in this regard, as part of a strategy to attenuate significant hypertension, has not been studied. It may be reassuring to physicians who so chose to continue combination therapy that in a case control study of 600 patients, it has been found that there is no excess decline in renal function in the very hypertensive patient (BP > 160/100 mm Hg) treated with combination of ACEI and ARB in comparison to monotherapy. 15 This suggests the primacy of BP control in preserving renal function over any potential decline afforded by combination therapy in this very hypertensive at-risk group.
The second caveat to note is that some of the ONTARGET patients had already received ACEI or ARB monotherapy for some time prior to entering the trial and that many were using therapies proven to have beneficial effects on vascular risk, such as β-blockers, statin and anti-platelet treatment. Conceivably, for these patients, their residual risk would have already been lowered, attenuating any additional benefit from combination therapy. However, in clinical practice, many patients do not or cannot take statin treatment and cannot use β-blockers or anti-platelet agents. It is theoretically possible that a greater RAAS blockade would be beneficial in this subgroup of patients who cannot have risk attenuated by other pharmacological means. Benefits to this subgroup which is not uncommonly seen in our clinics may be worth exploring.
The third qualification is that the ONTARGET study excluded those with CHF without New York Heart Association (NYHA) class specification and had only a very low prevalence of diabetic patients with proteinuria. The evidence for dual RAAS blockade in these subgroups is discussed below.
ACEI/ARB in combination: most studies point to a further reduction in albuminuria but no evidence yet on hard end points in proteinuric renal disease
ACEI or ARB monotherapy has been shown to reduce the progression of renal disease, both in terms of reducing albuminuria and loss of glomerular filtration rate (GFR). 16 Thus, ACEI or ARB monotherapy remains the mainstay of treatment for hypertension, microalbuminuria and established nephropathy in diabetic patients. Several early studies suggest that the ACE and ARB combination has a proven additive effect on albuminuria although many of these studies were small in number and with a short duration of follow-up. The meta-analyses of Jennings et al. 17 and then by Kunz et al. 18 suggest that combination therapy could reduce proteinuria by 20% more than monotherapy. In the ONTARGET population with a low prevalence of proteinuric renal disease, although no reduction in the degree of albuminuria was seen with combination therapy, the lowest progression was seen in the combination therapy groups. 12 On balance, it does seem that combination RAAS blockade has an additive effect on albuminuria. Given the close association between albuminuria with loss of renal function and CVD, the benefits of dual therapy on albuminuria could be expected to translate into a commensurate reduction in the loss of GFR and CVD benefit. However, recently, there has been considerable discussion about the suitability of albuminuria as a surrogate for harder end points, such as death, doubling of creatinine or need for dialysis. 19 This debate has been further fuelled by the surprising results of a study by Mauer et al., 20 which failed to show any benefit of early RAAS blockade on the progression of renal morphological changes, a finding discordant with other shorter term studies showing benefit of RAAS blockade on albuminuria. It is therefore important to consider the effects of dual blockade on the loss of GFR, separate from its effects on proteinuria.
In ONTARGET, despite a more favourable effect seen on albuminuria with combined RAAS blockade, there was an excess decline in renal function. The combined primary end point of death, doubling of creatinine and dialysis was reached more frequently in patients using this treatment. With 25,620 participants, this trial was, however, considered underpowered to show any renal end points 21 reflecting the low renal risk of the study population, which only had a relatively small proportion of patients with albuminuria. As the time interval to manifest the renal benefits of an intervention such as BP treatment is dependent on baseline albuminuria, 22 it has been argued that there may not have been sufficient time to show a benefit from dual therapy in this relatively low-risk renal group. 21 Nevertheless, the answer from the ONTARGET trial would have to be that there is no evidence to support the use of combined RAAS blockade in non-proteinuric diabetic patients at low renal risk, at least in the time frame studied (mean 56 months). It is unlikely for commercial reasons that a further trial using ACE and ARB combinations of this magnitude will be undertaken in a low-risk group.
The uncertainty surrounding the use of surrogate markers for hard end points should not detract from the strong evidence that albuminuria remains an important marker of renal risk and CVD. The relationship between higher levels of albuminuria and hard end points of death, doubling of creatinine and dialysis is robust. In this context, one should not extrapolate the lack of benefit of dual therapy seen in ONTARGET to patients with high-risk, proteinuric renal disease. The definitive trial to answer the question of whether combination ACEI and ARB is of benefit in diabetic nephropathy is being examined by two studies: the VA NEPHRON D trial (Combination Angiotensin Receptor Blocker and Angiotensin Converting Enzyme Inhibitor for Treatment of Diabetic Nephropathy) 23 and the VALID trial (Preventing ESRD in Overt Nephropathy of Type 2 Diabetes). NEPHRON D is powered for CKD progression to validated end points, and both trials are ongoing.
ACEI/ARB in combination: no evidence for additional benefit post acute myocardial infarction
Following acute myocardial infarction (MI), RAAS is activated in a compensatory response to maintain BP and systemic perfusion. The sustained activation of RAAS has potentially damaging effects as AII has inotropic and vasoconstrictive effects, thereby increasing myocardial oxygen demand in the critical coronary vasculature. In addition, RAAS stimulates smooth muscle hypertrophy and fibrosis leading to progressive ventricular dysfunction. Thus, continued sustained activation of RAAS is considered maladaptive, and ACEI or ARB monotherapy post-MI has been proven useful, provided BP is maintained. The VALIANT (Valsartan in Acute Myocardial Infarction) study examined the combination of captopril and valsartan in a cohort within 10 days of acute MI in those with left ventricular (LV) dysfunction. 24 No additional survival benefit was seen, and the dual therapy group experienced the greatest side effects, mainly hypotension and renal impairment. The ONTARGET study also examined patients with a history of prior MI. Although this trial did not look at combined treatment in the immediate post-MI time period, this study failed to demonstrate any survival benefit in post-MI patients. There is therefore little evidence to suggest that combination RAAS blockade is beneficial in the post-MI setting and that potentially the additive effects of ACE and ARB on BP are detrimental in the setting of potential acute reduction in cardiac output.
ACEI/ARB in combination: additional benefit on symptoms, admissions and quality of life in chronic systolic heart failure
Both ACE and ARB monotherapy increase survival and reduce symptoms and hospitalisations in those with heart failure, a condition where persistent activation of the sympathetic nervous system is correlated with severity of LV dysfunction and outcomes. Major neurohormonal systems are activated involving atrial natriuretic peptide (ANP), AII and secondary hyperaldosteronism and NO. Local cardiac and renal activation of RAAS may also be involved in neurohormonal adaptation. Notably, aldosterone may be the primary mediator of cardiac fibrosis, which also contributes further to cardiac systolic dysfunction. 25 There is more positive news for the use of combination of RAAS blockade in the setting of systolic heart failure. Several large trials have examined the combination noting positive findings from both the Val-HeFT and CHARM-added studies.26,27 Patients with NYHA classes II–IV were randomised to receive valsartan (Val-HeFT) or candesartan (CHARM) or placebo in addition to ACEI treatment. Both studies showed reductions in the composite primary outcome of CVD death or hospitalisations, driven largely by hospitalisations. The finding of an adverse effect on mortality with valsartan in combination with a β-blocker and ACEI in a subgroup analysis of Val-HeFT has not been borne out by further analysis of the data. Subsequent caveats are that in Val-HeFT, no benefit was seen with the addition of ARB if maximal dose of ACE was used. However, current guidelines suggest that combination therapy should be considered in the heart failure patient who continues to be symptomatic despite maximal ACEI and β-blockade, not in the acute MI setting. As usual, there is also the issue of additive complications such as hyperkalaemia and hypotension to contend with.
Diastolic heart failure is a subtype of diabetic heart disease. Although there is some evidence of benefit from candesartan in those with diastolic heart failure, combination use of ACEI and ARB has not been explored in this patient population.
RAAS blockade with DRI and ACEI or ARB
DRI and ACEI or ARB combination: there is an additive effect on BP
Aliskiren, the first DRI, has been available for clinical use since 2007, and most large-scale clinical trials have tested the single agent. Aliskiren directly lowers plasma renin activity, the most proximal site of the RAAS cascade. Like ACEI and ARB treatment, aliskiren has shown efficacy in the management of hypertension, proteinuria and congestive cardiac failure. Studies looking at the combination treatment of aliskiren and ACE or ARB have shown efficacy only in surrogate end points. With regard to BP, 150 mg of aliskiren along with 160 mg of valsartan was found to be more effective in lowering BP as dual therapy than monotherapy. 28 The combination therapy of aliskiren and losartan has been available in a single tablet form; however, this will be discontinued on the basis of the information described below.
DRI and ACEI or ARB combination: there is no benefit on cardiac parameters post-acute MI
The ASPIRE study (Aliskiren Study in Post-MI Patients to Reduce Remodeling) examined the addition of aliskiren to patients with left ventricular ejection fraction (LVEF) < 45%, within 2–6 weeks post-MI, with the majority already receiving an ACEI or ARB. No differences were found in echo parameters of LV function or infarct size. 29
DRI and ACEI or ARB combination: there is an additional benefit on albuminuria but no benefit on hard outcomes, and there is additional associated risk
The combination therapy of aliskiren and losartan in patients with hypertension, type 2 diabetes and nephropathy in the AVOID (Aliskiren in the Evaluation of Proteinuria in Diabetes) study showed a 20% reduction in ACR after 6 months of therapy with a slight BP advantage also seen in the combination group. 30 The harder end points of doubling of creatinine, end-stage renal failure (ESRF), CVD and death were not examined in that study, and the two studies set up to do so are the ALTITUDE (Aliskiren Trial in Type 2 Diabetes Using Cardio-Renal Endpoints) 31 and the ATMOSPHERE (Efficacy and Safety of Aliskiren and Aliskiren/Enalapril Combination on Morbi-Mortality in Patients With Chronic Heart Failure) trials. 32 The ALTITUDE study population were high-risk type 2 diabetic subjects, the majority of whom had albuminuria, and the intervention being the addition of aliskiren to ACEI or ARB. In December 2011, a prescient meta-analysis of combination treatment with aliskiren and ACEI or ARB by Harel et al., 31 highlighted the increased risk for hyperkalaemia with this combination. About the same time came the news that ALTITUDE trial had been discontinued prematurely with the Data Monitoring Board citing ‘an increased incidence of non-fatal stroke, renal complications, hyperkalaemia and hypertension over 18–24 months follow up’. 32 The committee concluded that on the grounds of therapeutic futility also, the study should be discontinued and that patients were unlikely to benefit from the addition of aliskiren in addition to standard anti-hypertensive treatment. In April 2012, the Food and Drug Administration (FDA) issued a safety warning and noted that the risks of stroke (2.7% aliskiren vs 2.0% placebo) and death (6.9% aliskiren vs 6.4% placebo) were numerically higher in aliskiren-treated patients but noted that they have not reached a conclusion regarding a link between aliskiren treatment and events. The FDA recommended a new contraindication against the use of aliskiren with ARBs or ACEIs in patients with diabetes because of the risk of renal impairment, hypotension and hyperkalaemia and a warning to avoid the use of aliskiren with ARBs or ACEIs in patients with moderate to severe renal impairment (i.e. where GFR < 60 mL/min). Aliskiren has been marketed in combination with a valsartan, which will be discontinued. The European Medicines Agency has issued similar warnings. This unexpected and salutary result has implication for diabetic patients in the ATMOSPHERE trial, which remains ongoing. The executive committee had argued that the patient populations are different between ALTITUDE and ATMOSPHERE and that an active open-label run-in phase is designed to exclude those with renal function decline, hyperkalaemia or hypotension. An independent Data Monitoring Board has agreed that the study should continue and patients have been informed. This trial includes ~5500 patients with diabetes. At this point, dual therapy with DRI is not advocated in diabetes for any indication, and we await the results of ATMOSPHERE to clarify the situation in heart failure. 32 The ALTITUDE news, however, does not bode well for the NEPHRON D trial examining ACEI/ARB combination in similar patients.
RAAS blockade with AA and ACEI or ARB
AA and ACEI or ARB combination: there is an additive effect on BP
Similar to the escape phenomena described for ACEI and ARB, aldosterone levels rise with chronic RAAS blockade treatment. There is demonstrated additional efficacy of aldosterone blockers and ACE or ARB in hypertension with significant BP reductions, 35 but with more profound relative hypoaldosteronism, hyperkalaemia is a significant adverse effect.
AA and ACEI or ARB combination: there is probable additional benefit on proteinuria
A meta-analysis of 15 studies showed benefit on proteinuria with the addition of eplerenone or spironolactone to ACEI or ARB in patients with proteinuria. 36 As above, hard end points are missing, and hyperkalaemia is a concern particularly as renal function deteriorates; currently treatment with this combination is not being recommended.
AA and ACEI or ARB combination: there is benefit in acute MI with LV dysfunction and systolic heart failure
The most robust evidence here comes from two studies. The EPHESUS (Eplerenone Post-Acute Myocardial Infarction Efficacy and Survival Study) 37 involved patients with symptomatic LV dysfunction (EF < 40%) 3–14 days post-MI, the majority of whom were already taking ACEI or ARB. The addition of eplerenone resulted in a significant cardiovascular mortality reduction of 17%, a reduction in sudden death and heart failure hospitalisations. Similarly, in the RALES (Randomised Aldactone Evaluation Study), 38 the addition of aldactone combination in chronic systolic heart failure translated into a 30% morbidity and mortality benefit. Patient selection and monitoring of renal function and for hyperkalaemia is advised with published strategies for the prevention of hyperkalaemia recommended. Triple RAAS blockade in this context is not recommended for this reason as well.
Dual RAAS blockade: areas for further study
Relevant to the endocrinologist are further areas where there is potential benefit from more complete RAAS blockade. The first is in the area of diabetic retinopathy. The retinal tissue renin–angiotensin system has been found to be upregulated in retinopathy. The DIRECT programme examined the use of candesartan in diabetes. 39 Although the trial did not meet its primary end point, there was an overall trend to less severe retinopathy. The RASS (Renin Angiotensin System Study) in type 1 diabetes similarly found benefit on retinopathy progression of both enalapril and losartan as monotherapy over placebo. 20 The question of whether more complete RAS blockade offered by combination therapy would be of benefit here is an intriguing one.
Most recently, there has been interest in RAAS blockade for the prevention of non-valvular atrial fibrillation. RAAS blockers are hypothesised to have properties that alter atrial and mechanical remodelling. A recent review has examined the question of RAAS blockade in the prevention of new atrial fibrillation, a common co-morbidity in diabetes associated with poorer prognosis. 40 The authors found a beneficial effect with ARB with less of a benefit seen with ACEI and no effect of AA. Dual therapy was not examined. The comment is made that data was considered of low quality and again further research is warranted.
Perspectives
Since the initial discovery of ACEIs as a by-product of snake venom research in the 1960s, there now exist four classes of RAAS blockers, each with multiple members and proven arenas for monotherapy. Despite a strong biological rationale, the evolving story of combination therapy has been largely disappointing with initial benefits seen on albuminuria and BP not being translated to meaningful superior clinical benefit. For most dual therapies, benefits are confined to symptomatic heart failure and arguably in severe hypertension while balancing the potential adverse effects. For the ACEI/ARB combination, while continued use for diabetic nephropathy is reasonable, we await the hopefully definitive results from the NEPHRON D trial. Remaining questions arise whether higher doses of monotherapy or lower doses of dual, triple or even quadruple therapy would be of benefit. Furthermore, given the pivotal role that RAAS activation has on the development of CVD and diabetic complications, multi-agent, low-level intervention earlier in the disease process has yet to be explored. The modern catchcry of clinical medicine is individualisation of therapy, but we are hamstrung by the inability to measure completeness of RAAS blockade in an individual. This is important as there may be an optimum degree. Other than perhaps the AII/AI ratio, a sufficiently accurate measure of the intensity of activation of the RAAS system by which to measure the efficacy of pharmacological interventions is not available for clinical use. Until then, we are dependent on well-designed robust clinical trials in representative patient groups. Given that we have not yet fully explored individual variances in RAAS blockade and more subtle combinations for intervention, it would still be premature to sound the death knell for dual blockade.
Footnotes
Conflict of interest
The author has received speaking honoraria form Astra Zeneca, MSD and Boehringer-Ingelheim.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.