
Abstract
Introduction:
Several studies have definitively shown the benefit of mineralocorticoid receptor antagonists (MRAs) in patients with heart failure (HF). However, very few prior studies examined the relationship between the timing of initiation of MRAs and prognosis. In addition, on this topic, there is no information regarding the specific population of patients suffering a first episode of decompensated congestive HF.
Methods:
We studied a homogenous cohort of patients discharged alive from our hospital after a first episode of decompensated congestive HF, in order to clarify the association between time of aldosterone receptor antagonist (ARA) initiation (within the first 90 days after hospital discharge) and mortality. Our population was composed of a series of consecutive patients. All-cause mortality was compared between patients who initiated MRAs at discharge (early group) and those who initiated MRAs one month later and up to 90 days after discharge (delayed group). We used prescription time distribution matching to control for survival difference between groups.
Results:
The early and delayed groups consisted of 365 and 320 patients, respectively. During the one-year follow-up, a significant difference in mortality was demonstrated between groups. Adjusted hazard ratios (HRs) for early versus delayed initiation were 1.72 (95% confidence interval (CI) 0.96 to 2.84) at six months, and 1.93 (95% CI 1.18 to 3.14) at one year.
Conclusions:
Delay of MRA initiation up to 30 to 90 days after discharge implies a significant increase in mortality compared with MRA initiation at discharge, after a first episode of decompensate congestive HF.
Keywords
Introduction
The renin−angiotensin−aldosterone system (RAAS) plays a pivotal role in maintaining a neurohormonal imbalance that promotes heart failure (HF).1–5 Neurohormonal activation acts to modify cardiac structure and function, inducing both left ventricular (LV) hypertrophy and collagen network remodeling, 6 changes that increase cardiovascular morbidity and mortality. 7
It is well known that drugs interfering with the RAAS attenuate or even reverse LV remodeling and improve prognosis;8–10 aldosterone levels often remain elevated or even increase in these patients because of the well-known ‘escape’ phenomenon.11,12 In addition to the other components of the RAAS, aldosterone directly promotes LV overload, hypertrophy, tissue-mediated responses (increase in cytokines, adhesion molecules, and endothelial dysfunction), and myocardial fibrosis.13,14
The pathophysiological rationale for aldosterone blockade in the treatment of HF is supported by large-scale randomized clinical trials demonstrating that anti-aldosterone agents, when added to optimal therapy, consistently reduce cardiovascular morbidity and mortality in patients with advanced HF (New York Heart Association (NYHA) class III and IV), 15 in patients with systolic HF and mild symptoms (NYHA class II), 16 and in those with systolic dysfunction and HF following acute myocardial infarction (AMI). 17 Current guidelines recommend, in fact, using mineralocorticoid receptor antagonists (MRAs) for all symptomatic patients (NYHA class II–IV) on top of optimal therapy, including β-blockers and angiotensin-converting enzyme inhibitors (ACE-Is) or angiotensin receptor antagonists (ARBs).18,19
Only two studies examined the relationship between the timing of initiation of MRAs and prognosis. The first of these is the study by Adamopoulos et al., 20 who performed a preliminary exploratory analysis of the Eplerenone Post-AMI Heart Failure Efficacy and Survival (EPHESUS) trial. This study demonstrated that an earlier aldosterone blockade improved outcome in patients with HF, and this benefit was not observed when the aldosterone receptor antagonist (ARA) was initiated later. The other study is by Hayashi et al., 21 who found that the treatment with MRAs within 24 hours after an AMI may prevent post-infarct LV remodeling. However, there is no information concerning how the beneficial effect of aldosterone inhibition relates to the timing of MRA initiation in the specific population of patients suffering a first episode of decompensated congestive HF.
Using the database of our hospital, we selected a homogenous cohort of consecutive patients in order to study the association between time of MRA initiation (within the first 90 days after hospital discharge) and mortality in patients with HF discharged alive after a first episode of decompensated congestive HF. Risk of mortality was computed comparing patients who initiated MRAs at discharge (early group), who we postulate to be advantaged, and those who initiated MRAs one months later, up to 90 days after discharge (delayed group).
Subjects and methods
Study cohort
Eligible patients were residents of the Province of Modena, who were discharged alive from the Modena Policlinico Hospital after a first episode of decompensated congestive HF between January 2007 and March 2010. Follow-up data were available for these patients until April 2011.
“MRA users” (see definition below) who were discharged alive from their first hospitalization for decompensated congestive HF were included. Patients were excluded if they met ≥ one of the following conditions: (1) presence of severe comorbidities (significant renal impairment (defined as reduction of the glomerular filtration rate, calculated by the Modification of Diet in Renal Disease equation, < 60 ml/min/1.73 m2), dementia, or malignancy); (2) age ≥ 85 years. These two groups of patients were frail and likely to have a short life expectancy, which may have obscured the effect of treatments; and (3) a total length of hospital stay ≤ three days.
Patients who filled a prescription of an MRA ≤ 90 days after discharge were identified as “MRA users.” Those who had a prescription dispensed at discharge formed the “early group,” and those who filled a prescription 30 to 90 days after discharge formed the “delayed group.”
The study outcome was defined as mortality due to any cause. All patients were followed for the earliest occurrence of death or one year after discharge.
Data source
Data were obtained from the general database of our hospital, which contains information concerning hospital admissions, discharge reports, inpatient physician encounters, and dispensed medications. Prescription information includes type of medication and dispensed dose.
Death information was obtained from the Modena provincial registry office.
Detailed information on patients’ baseline characteristics, including medication and doses, was recorded at discharge (baseline).
Baseline characteristics
General information, including patients’ age, gender, and co-morbidity, was noted at discharge. Concurrent use of major cardiac medications was recorded for beta blockers, nitrates, diuretics, warfarin, digoxin, ACE-Is, ARBs, and MRAs. In addition, data included: date of cardiac procedures after the index hospital admission (catheterization, percutaneous coronary intervention, or coronary artery bypass grafting), and length of hospital stay.
Prescription time distribution matching
By definition, patients in the delayed group survived at least the first month and up to 90 days, whereas patients in the early group may have had an event any time after discharge. Although the risk of death is higher after discharge, an excessive amount of early events is expected to occur in the early group. This systematic difference in time to treatment initiation may result in biased estimates if not corrected for either at the design or analysis level. To address this between-group survival difference, we used the method of prescription time distribution matching to define time of study entry (T0). The method considered the dispensing date of the first MRA prescription (the date of post- discharge visit) was considered to be the time of study entry of the delayed users. Early users were assigned a T0 that was selected at random from the observed prescription time distribution of the delayed users. Those who died before the assigned T0 were excluded. The two groups were then followed from their respective T0 values, and onward.
Statistical analyses
Descriptive statistics were used to compare baseline patient characteristics between groups.
To exclude the possibility that the delayed users were late to fill the prescription because they underwent more post-discharge procedures or hospital readmissions, we examined the period between discharge and matched prescription time for rates of cardiac procedures (percutaneous coronary intervention, coronary artery bypass grafting, and catheterization) and hospital admissions for congestive HF.
Survival in the two groups was displayed by a Kaplan–Meier curve. A multivariate Cox’s regression model was used to obtain the hazard ratio (HR) of mortality between the delayed (reference) and early groups after adjusting for baseline characteristics. Mortality hazards were evaluated at six months and at one year after discharge.
A p < 0.05 was considered statistically significant.
Results
Cohort and baseline characteristics
In our cohort, 689 consecutive patients filled an MRA prescription during the first 90 days after discharge. Of these, 365 patients (52.6% of the entire population) filled an MRA prescription at discharge (early group), and 320 patients (47.4%) initiated an MRA 30 to 90 days after discharge (delayed group).
After matching on study entry between the early and delayed users, the early group had an assigned T0 distribution identical to that of the delayed users (median: 55 days; interquartile range: 40 to 72 years). There were four subjects who were excluded from the early group because they died before their assigned T0.
A comparison between early and delayed users after prescription time distribution matching showed similar demographic and clinical characteristics (Table 1). Also, as regards the type and dose of the prescribed drugs, we did not note any significant difference. Specifically, types and dose of prescribed MRAs are summarized in Table 2. Patients did not significantly differ in terms of types and dose of prescribed MRAs.
Baseline (at discharge) characteristics of mineralocorticoid receptor antagonists users, discharged alive from a first episode of decompensated congestive heart failure.

Users who initiated mineralocorticoid receptor antagonists at discharge; busers who filled an mineralocorticoid receptor antagonists prescription 30 to 90 days after discharge; crates of cardiac medication use up to the matched time of first mineralocorticoid receptor antagonists prescription. BMI: body mass index; HF: heart failure; EF: ejection fraction; EDD: end-diastolic diameter; ACE-I: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor antagonist.
Type and dose of mineralocorticoid receptor antagonists prescribed to our patients, divided according to “early” (at discharge) or “late” (30 to 90 days after discharge) utilization of a mineralocorticoid receptor blocker.
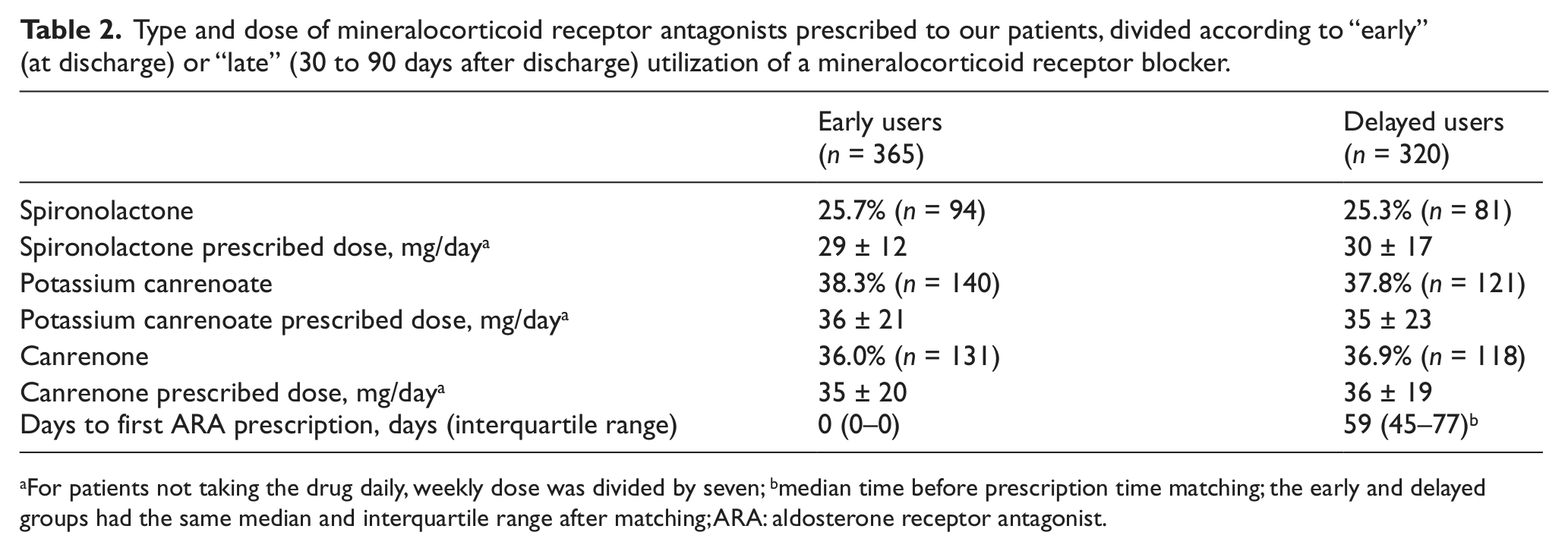
For patients not taking the drug daily, weekly dose was divided by seven; bmedian time before prescription time matching; the early and delayed groups had the same median and interquartile range after matching; ARA: aldosterone receptor antagonist.
Treatment rates after discharge and up to matched prescription time
There was no difference in the rates of post-discharge cardiac procedures and hospital admissions up to matched T0 between the early and delayed groups. For post-discharge cardiac procedures, rates in the early and delayed groups were 9% and 10%, respectively (p = 0.32). For post-discharge hospital admissions, rates were 6% and 7% (p = 0.26).
Effect associated with difference in timing of MRA initiation
Twenty-six patients in the early group (7.1%) and 43 in the delayed group (13.4%) died in the first year after first hospital admission. Kaplan–Meier curve (Figure 1) and multivariate Cox’s regression analysis showed a significant difference in mortality due to delay of MRA initiation.

Cumulative one-year mortality in patients with a first episode of decompensated heart failure among “early” and “delayed” users of mineralocorticoid receptor antagonists.
Adjusted HRs for mortality for delayed versus early initiation were 1.72 (95% confidence interval: 0.96 to 2.84) at six months, and 1.93 (95% confidence interval: 1.18 to 3.14) at one year after discharge (comparison was controlled for survival bias by prescription time distribution matching).
Discussion
The present study evaluated the effectiveness of early MRA use compared with delayed initiation in a population of patients hospitalized for a first episode of decompensated HF. Compared with a delay in MRA initiation, early users show a significant difference in mortality compared with delayed users during the first year after discharge. Based on the survival curve, a delay of only one month in the administration of an MRA implies approximately a doubling of mortality risk after one year. This aspect may be important from a practical point of view, because even the most recent guidelines do not provide guidance regarding how early to start MRA treatment after hospitalization for congestive HF. The present study provides a clear indication for use of MRAs as early as possible, on top of the treatment (including ACE-I or ARB and beta-blocker), preferably at discharge after an episode of decompensate HF.
The reason to define delayed use as one month to 90 days in the present study is threefold. First, this is determined by the actual prescription pattern. The first 90-day period captured practically all the first MRA prescriptions in the year after discharge. 22 Second, the highest risk of readmission and death occurs during the first month after discharge.23,24 Third, the EPHESUS trial suggests that earlier eplerenone administration improved outcomes in patients with HF, that this benefit was not demonstrated when eplerenone was initiated later, 20 and that the reduction in mortality from any cause was apparent within the first 30 days of randomization. 25 Therefore, it is important, in our opinion, to examine the effect on mortality as a result of an initiation delay ≥ one month compared with initiation at discharge.
Pathophysiological effects of aldosterone and “aldosterone escape” in congestive heart failure
Mineralocorticoid antagonism attenuates cardiovascular damage by mechanisms that involve direct blockade of aldosterone’s cardiovascular pro-inflammatory and pro-fibrotic effects. 26 Aldosterone induces fibrosis in the heart, blood vessels, and kidney, 25 and the antagonism of mineralocorticoid receptors has been associated with reduced fibrosis in human myocardium, limited ventricular remodeling, and improved survival in patients with ventricular dysfunction and heart failure.14,25–28 Our results suggest a greater benefit in terms of survival if MRA treatment is started as early as possible.
However, with ACE-I therapy now given routinely for congestive HF, the clinical importance of aldosterone had previously been overlooked because ACE-I therapy was widely believed to suppress aldosterone production effectively by ‘upstream’ RAAS blockade. Increasingly, it is becoming evident that following an acute fall in aldosterone in response to administration of an ACE-I, the level of aldosterone rises again, and indeed returns to baseline in almost all patients, a phenomenon known as “aldosterone escape.”11,12,29–33 Even when an ACE-I is given in combination with an ARB, aldosterone levels remain uncontrolled.34,35 Additionally, there is evidence that aldosterone escape, in turn, might promote release of angiotensin II via a positive feedback loop that stimulates ACE in the vasculature. 36 This, and the progressive escape of aldosterone, are thought to contribute to “ACE-I resistance,” whereby the effect of ACE-I becomes blunted, and beneficial effects on mortality decrease over time.37,38 The results of our study allow us to postulate that the escape phenomenon occurs rapidly in patients who have had an episode of decompensated congestive HF. MRAs, in turn, are able to antagonize the deleterious effects of aldosterone, resulting in a beneficial effect, ultimately, on patient mortality.
ARAs utilized in the present study
While in the United States the most widely used MRA is represented by spironolactone, in Italy canrenone and potassium canrenoate are also used.
Potassium canrenoate is a competitive non-selective inhibitor of aldosterone receptor; its pharmacologic activity is due to a rapid conversion to canrenone, which is the active metabolite of potassium canrenoate and spironolactone. 39 Potassium canrenoate is rapidly and completely absorbed from the gastrointestinal tract and bypasses the liver unchanged. Canrenone and canrenoate are in enzymatic equilibrium in vivo, in which canrenoate represents the derived γ-hydroxycarboxylic acid. 40 The bioavailability and water solubility of potassium canrenoate and canrenone are greater than those of spironolactone; therefore the number of active metabolites of the latter is considerably greater. 40
In Italy eplerenone, a selective aldosterone receptor blocker, is not commercially available. All of the aldosterone inhibitors used in the present study are, in consequence, not selective.
In Italy, overall, MRAs are little used: In 2011 the mean number of doses of MRAs consumed daily by 1000 inhabitants was 3.5, a very small quantity compared with 88.5 doses of ACE-Is, 56.3 of calcium channel blockers, 53.2 of ARBs, 38.5 of beta adrenergic blockers, 24.3 of loop diuretics, and 6.0 of thiazide diuretics. 41 However, the present study is indicative of current clinical practices in a large Italian referral center. Our group, together with other referral Italian centers, is part of the AREA-in-CHF network, a research group that demonstrated in patients with HF positive effects of canrenone in preventing LV remodeling 28 and in improving myocardial mechano-energetic efficiency. 42
Strengths and limitations of the study
The strengths of the present study are: first, the homogeneous cohort of patients; and second, the primary end-point of the study, represented by mortality from any cause. This is universally accepted as the strongest end-point in prognostic studies.
Despite appropriate design and analyses, this study has several limitations. First, the study is prone to biases because of its observational nature. Although the bias that results from confounding by indication is minor, because all patients are MRA users, there are likely uncharacterized factors that may confound the timing of initiation. Some of them could be related to clinical practice and patient disease severity, which could obscure the possible benefit associated with early MRA initiation. Despite adjustment for a wide spectrum of characteristics, it is possible to have residual confounding in the comparisons. Second, survival bias in the comparison of early versus delayed MRA initiation may affect the validity of the results. We controlled for this bias by matching the time of study entry between the two groups using prescription time distribution matching. However, due to matching, we could not study the effect in the first month. Third, our study is limited by the data and clinical practice during the study period, although patients were similar with regard to types of prescribed MRA and used dosages.
Conclusions
In patients suffering from HF, a delay of MRA initiation up to 30 days after discharge implies a significant increase in mortality compared with MRA initiation at discharge after a first episode of decompensated congestive HF. Subsequent studies, preferably randomized, should confirm these findings. However, on the basis of the results of our study, it seems reasonable to suggest from a clinical point of view that patients with HF in whom there is a clear indication to use an MRA, should have the possibility of starting this treatment as soon as possible.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.